
Abstract
Introduction
The co-occurrence of depression and chronic pain causes additive adverse effects on patients” outcomes, response to treatment, and poorer functioning. Despite this, there is a dearth of studies in developing countries. Therefore, this study aimed to provide a new insight into the understanding of the prevalence and associated factors between chronic pain and depression among patients with chronic pain in Jimma town public hospitals.
Methods
Institution-based cross-sectional study was conducted in Jimma town public hospitals. A total of 422 sampled patients with chronic pain participated in the study. Depression was assessed using the PHQ-9 scale. The coded data were entered to Epi Data version 3.1 and exported into SPSS version 23.0 for analysis. Logistic regression analysis model was used to identify factors independently associated with depression.
Result
The prevalence of depression among chronic pain patients was found to be 43.3%. The number of presenting compliant (AOR = 3.092, 95% CI: 1.684-5.678), history of depression (AOR = 0.319, CI: 0.133-0.766), pain intensity (AOR = 5.296, 95% CI: 2.018-13.901), pain location (AOR = 0.318, 95% CI: 0.158-0.638), pain persistence (AOR = 5.163, 95% CI: 2.784-9.576), the extent the pain compromised the respondent quality of life (AOR = 3.816, 95% CI: 1.685-8.643), and episodes of the pain associated with activities (AOR = 0.247, 95% CI: 0.138-0.442) were significantly associated with depression among patients with chronic pain.
Conclusion
This study has shown a high prevalence of depression among patients with chronic pain. Furthermore, depression was associated with various pain-related factors. Hence, effective screening and management of depression among chronic pain patients’ needs noteworthy attention.
Introduction
Depression is a commonly occurring neuropsychiatric condition 1 Manifested by low mood, reduced energy, loss of interest, feelings of low self-worth, trouble sleeping or eating, and poor concentration for at least two weeks. 2
350 million people are affected by depression worldwide. A survey carried out in 17 countries globally showed, on average about 1 in 20 people reported having depression. 2 The consequences of untreated psychiatric disorders especially depression can be serious, these include suicide, job, and relationship loss, loss of productivity, and deterioration in physical health. 3
Chronic pain is usually defined as any persistent or intermittent pain that lasts more than 3 months4,5 chronic pain is classified as a mixed pain syndrome that resulted from neuropathic as well as nociceptive mechanisms. 5 Chronic pain is a common condition, affecting an estimated 20% of people worldwide. 6
Chronic pain and depression are each prevalent and often co-occur, with up to 60% of chronic pain patients also presenting with depression, 7 their coexistence has been shown to incur additive adverse effects on patient outcomes, including poorer functioning and reduced response to treatment. 8 A bidirectional relationship exists between depression and chronic pain. 9 This might occur as a result of the shared neuroplasticity alterations and underlying processes between chronic pain and depression. 4
Since depression and chronic pain symptoms such as insomnia, fatigue, and change in activity can be related to both chronic pain and depression assessing depression in chronic pain has become challenging. 10
Epidemiologic studies indicate that the mean prevalence rate for depression in patients having pain was 52% in pain clinics or patient pain programs, 38% in psychiatry clinics or psychiatry consultation, 56% in orthopedics clinics, 85% in dental clinics addressing facial pains, 13% in gynecology clinics addressing chronic pelvic pain in laparoscopy patients, 27% in primary care clinics. 11
US CDC mortality and morbidity report indicate depression to be more common in females (4.0%) than males (2.7%) and in unemployed (9.8%) than employed (2.0%). Depression is also common among substance users, disrupted marital status, older age, and lower educational level. Other factors associated with depression in different studies were lack of social support, rural residence, having a chronic illness, smoking, and alcohol use.12,13
Knowledge about the prevalence of depression and its determinants is crucial for health planners but little is known about the prevalence of depression and its determinants among patients with chronic pain in Jimma town public hospitals. Hence, the finding of this study helps health planners, governmental, non-governmental organizations, and clinical practitioners working in the area to develop depression reduction management program strategies. This study will also be used as baseline information for further investigation in the area.
Material and Methods
Study Design, Setting, and Period
Institution-based cross-sectional study design was conducted at two public hospitals in Jimma town (Jimma medical center (JMC) and Shenen Gibe hospital (SGH)). Jimma town is located 352 km southwest of the capital city Addis Ababa, Ethiopia. The study was conducted from April 30 to May 30/2019.
Sample Size Determination and Sampling Technique
The sample size was determined using a single population proportion formula n = (Z α/2)2 p (1−p)/d2, considering a p-value of 50%, 95% confidence level, 5% margin of error, and 10% non-response rate, the final sample size was 422. A consecutive sampling technique was used.
Population
All sampled patients with chronic pain who were on follow-up and admitted to medical, surgical, maxillofacial, gynecology, ophthalmology, psychiatry, chronic illness follow-up, and ART clinic were the study population. Patients aged less than 18 years, who had a severe psychiatric illness that impairs communication skills, pediatrics, and critically ill patients who cannot respond to questions were excluded from the study.
Data Collection Tools and Procedures
The data were collected using pretested structured interviewer-administered questionnaire which consists of socio-demographic characteristics, a depression screening tool, and a chronic pain assessment tool. Depression was assessed by a 9-item patient health questionnaire (PHQ-9) tool. The PHQ-9 tool has proved to be reliable and valid with a sensitivity of 86% and specificity of 67% that can be used to screen for depression in Ethiopia.12–14 The Amharic and Afan Oromo version of PHQ 9 has been validated for use to screen depression in hospitals based.14,15 For the screening of depression, the cutoff point of 10 was used, given the fact that the questionnaire's had a sensitivity of 81.2% and specificity of 86.7%. 13
To assess chronic pain a tool that addresses the two parts of chronic pain including persistent baseline and breakthrough pain was used. 15 A chart review was done to identify the number of patients with chronic illnesses.
The number of sampled study participants for each hospital was identified by proportional allocation of the number of patients with chronic pain. Hence, a total of 4600 and 1135 patients in Jimma medical center and Shenen gibe hospital visits per month respectively. Accordingly, a total of 338 and 84 patients from Jimma medical center and Shenen gibe hospital were selected respectively. Then proportional allocations were done for all wards in the hospitals based on patient number visits per month. To maintain data quality, training was given to the data collectors and the supervisors.
Data Processing and Analysis
The collected data were checked for completeness, consistency, and quality of the data on daily basis. The collected data were coded and entered using Epi-data 3.1 and exported to SPSS version 23.0 for analysis. The data were analyzed using descriptive statistics and bivariate and multivariate logistic regression models were used to identify factors associated with depression. Binary logistic regression analysis was done and those variables with a P-value less than .25 were candidates for the multivariate logistic regressions model. Finally, variables with a P-value less than .05 and a 95% CI odds ratio in multivariate logistic regression were considered to have a statistically significant association with the outcome variable.
Compliance with Ethics Guidelines
Ethical clearance was approved by Jimma University institutional review board (IRB). Subsequently, an official support letter was obtained from the health research and postgraduate director office of the institute to the respective administration of Jimma town public hospitals. The participants in the study were clearly informed about the aim of the study and that participation in this study was voluntary; respondents could also withdraw at any time from the study if they feel uncomfortable. Refusal to participate didn't affect patient care.
Then after, written informed consent was obtained from a respondent who participated in the study. Confidentiality was maintained by omitting their name and personal identification. And those patients who were screened as having depression have been advised and linked to a psychiatric clinic.
This study was performed in accordance with the Helsinki Declaration of 1964, and its later amendments. All subjects provided informed consent to participate in the study.
Result
Socio-Demographic Characteristics
A total of 406 study respondents were involved in the study giving a response rate of 96.2%. More than half 226(55.7%) of the respondents were female, married 273(67.2%) and literate 227(55.9%). Similaly, most 237(58.4%) respondent's family monthly income was between 1000-4999 and the mean age (standard deviation) of respondents was 45.01 (± 14.24) (Table 1).
Socio-Demographic Characteristics of Study Participants of Jimma Town Public Hospitals, 2019.

Other occupational status: labor workers and retired respondents.
Pain-Related Factors
The majority of the study participants had moderate pain 233 (57.4%). The Head is the most common pain site or location 141 (34.7%). Most 214 (52.7%) respondents have persistent pain and138 (34%) of them have episodes of breakthrough pain (Table 2).
Distribution of Pain Factors and History of Patients with Chronic Pain in Jimma Town Public Hospitals, 2019.

Patient History-Related Factors
More than half of the respondents have one diagnosed chronic illness 213(52.5%) and 162(44.8%) of the study participants presented with one complaint, Among the 406 study participants, 37(9.1%) of them have a history of diagnosed depression (Table 2).
Clinical Factors
The majority 352(86.7%) of the study participants were presented with medical illnesses. 20(4.9%) presented with surgical illnesses while 6(1.47%) gynecological, 7(1.72%) psychiatric, 3(0.73%) ophthalmological, 6(1.47%) maxillofacial, and 12(2.95%) oncological diagnosis. Nearly half of the patients 205 (50.4%) reported the extent their life quality compromised due to the pain is in a fair amount.
50.40% of the respondents’ life had been compromised fairly due to the presence of chronic pain. While 3.40% of the respondent's life has been extremely compromised (Figure 1).

Distribution of respondents’ extent of quality of life compromised due to the pain of patients with chronic pain in Jimma town public hospitals, 2019.
Prevalence of Depression
The prevalence of depression is found to be 176(43.3%). Among those patients who were depressed, 9(4.93%), 46(26.16%), 39(22.17%), 40(22.91%) and 42(23.83%) had severe, moderately severe, moderate, mild and none-minimal depression.
Multivariate Logistic Regression
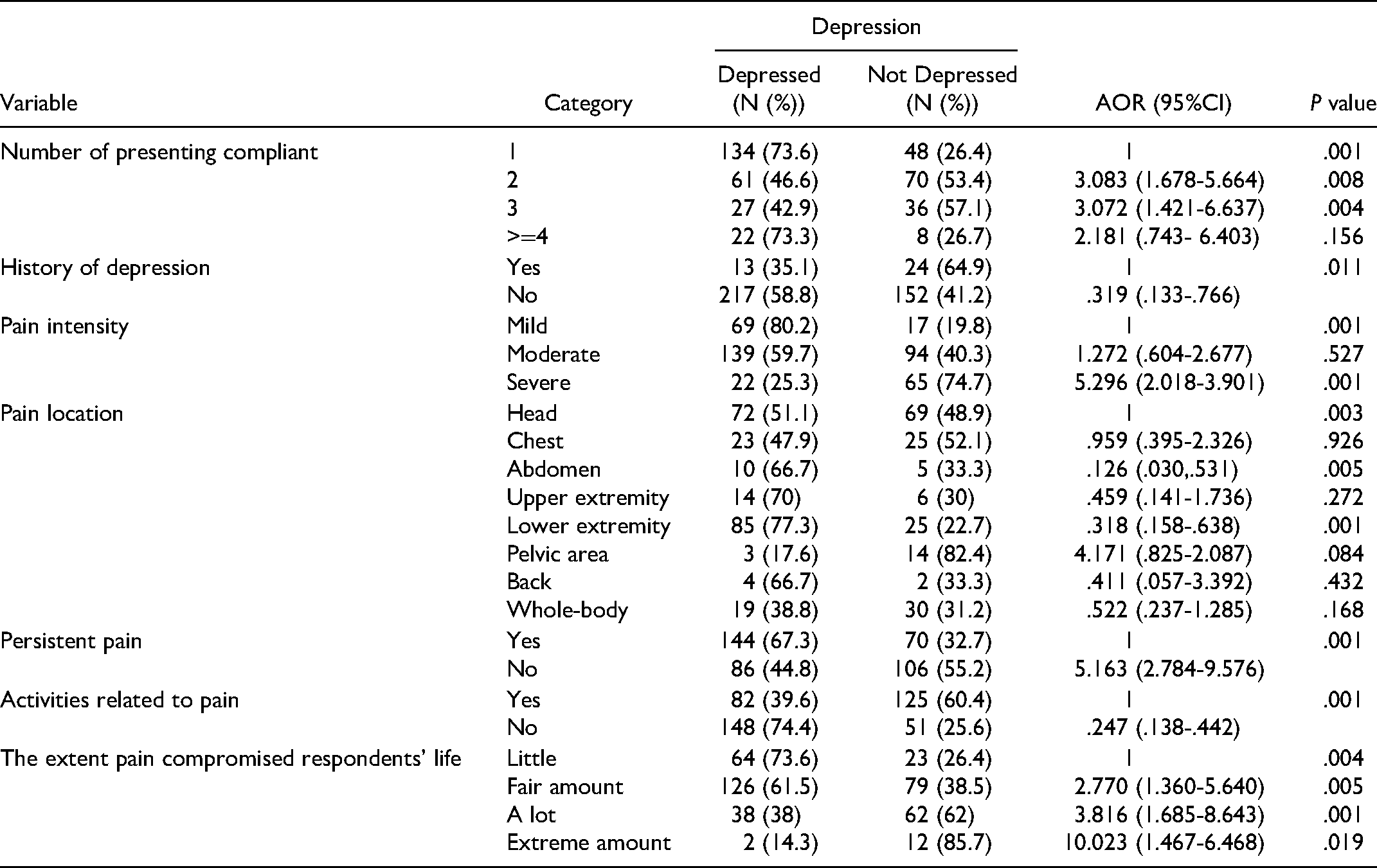
Multivariate logistic regression analysis showed patients with two (AOR = 3.092, 95% CI: 1.684-5.678, P = .008) or three (AOR = 3.082, 95% CI: 1.427-6.655, P = .004) presenting compliant were three times more likely to have depression than patients with one presenting complaint. Those patients who didn't have a history of depression were 68.1% less likely to be depressed than patients with a history of depression. (AOR: .319, 95% CI: 0.133-0.766; P = .011). Patients whose pain is not associated with certain activities were 75.3% less likely to report depression as compared to patients whose pain is associated with or aggravated by certain activities in chronic pain-matched participants (AOR = 0.247, 95% CI: 0.138-0.442). Regarding the severity of pain and its association with depression, results showed that patients who had severe pain were five times more likely to be depressed than patients with mild pain. (AOR: 5.296, 95% CI: 2.018-13.901; P = .001).
Patients whose pain location is on abdomen (AOR: 0.126, 95% CI: 0.030-0.531; P = .005) and lower extremity (AOR: 0.318, 95% CI: 0.158-0.638; P = .00) were.87.4% and 68.2% less likely to be depressed than those patients with pain location is on head.
Study respondents who do not have persistent pain are five times more likely to be depressed than those who have persistent pain (AOR = 5.163, 95% CI: 2.784-9.576) and those patients whose life quality is compromised a lot (AOR = 2.770, 95% CI: 1.685-8.643, P = .001) and in a fair amount (AOR = 3.816, 95% CI: 1.360-5.640, P = .005) are more likely to be depressed than those patients whose life quality are compromised in a little extent (Table 3).
Multivariate Logistic Regression Analysis of Factors Associated with Depression Among Patients with Chronic Pain in Jimma Town Public Hospitals, 2019.
Discussion
This study assessed the prevalence of depression and associated factors among patients with chronic pain.
The finding of this study showed that the prevalence of depression is 43.3%. This result is lower than the study done in Hong Kong (57.1%), 16 London (60.8%), 17 and Saudi Arabia (71%). 18 A literature review done using 15 studies to assess depression and pain co-morbidity among patients with chronic pain from pain clinics or inpatient pain programs indicated the prevalence of depression as 52%. 19 This may be explained by the higher PHQ cutoff of limit 10 used in our study versus a lower cutoff limit of 5 used in others.16,17 Using the lowest criteria or cutoff limit increases the number of patients screened to have depression. Additionally, population sample and patient characteristics are other factors that may have caused the difference. In the current study, the study populations include all patients with chronic pain in hospital wards and follow-up clinics. But in other studies, the participants were patients who came to attend the pain clinic, so this may be the reason for the discrepancy that may have been caused by the difference in pain severity.
However, this study finding is higher than the study done in Greece (22.5%), 13 China (25%), 20 Ethiopia (17.5%), 12 southwest Trinidad (28.3%), 21 and Saudi Arabia (36%). 4 The difference could be due to the tool used to assess depression. The current study used PHQ-9 while the study done in Saudi Arabia used the Center for Epidemiologic Studies-Depression (CESD) scale. 4 The difference could also be explained by the Chinese study being conducted only among patients with chronic low back pain unlike the current study. 20
Multivariate logistic regression analysis indicated that there was a statistically significant association between depression and the number of presenting complaints, a history of depression, pain intensity, pain location, persistent pain, activities related to pain, and the extent to which the pain compromised the respondents’ life.
The current study indicates that patients with severe pain are more likely to be depressed than those with mild or moderate pain. This is supported by the cross-sectional study done in Addis Ababa, 22 China, 20 and Saudi Arabia 4 indicates a significant association between pain intensity or severity with depression. Additionally, a comparison study done among Patients Attending Specialist Orthopedics clinics and multidisciplinary pain clinics in Hong Kong indicates present pain intensity increased the odds of comorbid depression. 16 This could be explained by when pain is moderate to severe, impairs function, and/or is refractory to treatment, it is associated with more depressive symptoms and worse depression outcomes (eg, lower quality of life, decreased work function, and increased health care utilization). Similarly, depression in patients with pain is associated with more pain complaints and greater impairment. Depression and pain share biological pathways and neurotransmitters, which have implications for the treatment of both concurrently. 23
In the current study patients whose pain is not associated with certain activities were 75.3% less likely to elicit signs of depression as compared to patients whose pain is associated with or aggravated by certain activities. This is supported by a study done among patients attending Specialist Orthopedics Clinic and Multidisciplinary Pain Clinic in Hong Kong indicates those reporting greater pain interference with daily activities had a higher odds of comorbid depression. 16 Chronic pain is at least partly attributed to a sedentary and inactive lifestyle. Physical activity/inactivity may be determined by genetic/epigenetic and neural factors encoded in our brain. 24 Evidence showed that sedentary behavior/ inactive lifestyle is associated with depression.25,26
This study indicates the number of presenting compliant had a statistically significant effect on depression, where patients with two or three presenting compliant were three times more likely to have depression than patients with one presenting complaint. This study is in line with a cross-sectional survey in Four health offices in the Southwest region of Trinidad. 21
The current study shows that those patients who didn't have a history of depression were 68.1% less likely to be depressed than patients with a history of depression. This study is in line with a cross-sectional study that is carried out in a chronic pain clinic in a tertiary care hospital in Riyadh, Saudi Arabia King Faisal Specialist Hospital and Research Centre show that medical history of depression was significantly associated with depression. 18 Depression is a highly recurrent disorder, patients who recovered from the first episode of depression will have one or more additional episodes in their lifetime.27,28
In the current study, patients that do not have persistent pain are less likely to be depressed than patients having persistent pain, A possible explanation is that impaired functioning caused by pain can lead to social isolation, which in turn can lead to a negative effect on depressive symptoms, and vice versa.29,30
This study has found those patients whose life quality is compromised a lot and in a fair amount by pain were more likely to be depressed than those patients whose life quality is compromised a little. The chronic disease disrupts an individual's life and this disruption may be interpreted in terms of its impact on well-being, or quality of life. Psychosocial well-being is compromised by two limitations: by reducing positively reinforcing outcomes of participating in valued activities and feelings of personal control and by limiting the ability to obtain positive outcomes or avoid negative ones. 31
The study is cross-sectional by nature, which does not show the cause-effect relationship between the outcome variable and explanatory variables.
Conclusion
The prevalence of depression in this study was found to be high and associated with multiple clinical and pain-related factors. This emphasizes the need for detecting those risk factors for patients coming to either the follow-up clinic or inpatient services. Moreover, the high rate of depression in this study calls for further researchers to conduct evidence about the cause-effect relationship between the predictor variables and depression.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Jimma University