
Abstract
Background
Ultrasound scanning is an integral part of antenatal care worldwide. However, little is known about the utilization of obstetric ultrasound in Ethiopia. This study aimed to assess prenatal ultrasound utilization and its associated factors among pregnant women attending antenatal care in Jimma town public health care facilities.
Methods
An institutional-based cross-sectional study was conducted on 303 pregnant women attending antenatal care (ANC) from July to August 2021 in Jimma town public health care facilities. A systematic sampling technique was used to select study participants who attended the ANC service during the data collection period. Logistic regression analysis was performed to determine the association between the explanatory and response variables. The strength of association of dependent and independent variables was presented as crude and adjusted odds ratio (AOR) at a 95% confidence interval. The level of significance was declared at a P-value of less than .05 in multivariable logistic regression. Narratives, figures, and tables were used to obtain the results.
Findings
The proportion of prenatal ultrasound utilization in this study was 60.7% [(95% CI); (55.4%-66%)]. Residency AOR = 6.09 (95%CI: 2.35-15.78), household monthly income less than 1000 AOR = 0.159(0.035-0.73), mother's history of at least one abortion AOR = 5.78 (95% CI: 1.89– 17.64), and knowledge towards prenatal ultrasound AOR = 15.77 (95% CI: 6.39-38.92) were found statistically significant association with prenatal ultrasound utilization.
Conclusions
In the current study, the proportion of prenatal ultrasound utilization during pregnancy was lower than the world health organization (WHO) recommendation. Therefore, the author recommended that educating mothers on the purposes of obstetric ultrasound and/ or including a prenatal ultrasound screening as part of antenatal care is needed.
Introduction
The use of ultrasound has quickly gained acceptance in medicine because of it's non-invasive, cost-effective, and safe for the mother, and fetus. 1 Nowadays, antepartum ultrasound has become an essential part of antepartum care (ANC) worldwide. 2 Consistent with the recommendations of the World Health Organization (WHO); an ultrasound scan should be a part of routine prenatal care, specifically, one ultrasound scan before 24 gestational age is suggested for every pregnant woman. 3 The International Federation of Gynecology and Obstetrics (FIGO) recommends 2 ultrasound screens for all pregnant women during the first and second trimesters. 4
Ultrasound during pregnancy is mostly used to estimate fetal age, number of fetuses, placental localization, screening of vertebrate malformation, fetal growth, and fetal presentation, to diagnose obstructed labor, incomplete miscarriage, hydatidiform mole, and ectopic pregnancy.3,5,6 Additionally, it's psychological effects on the initiation of bonding, reduction of tension, depression, hostility, and corporal symptoms when USS is well established. 7 Identification of malformations and obstetric complications by routine USG provides early information and helps in creating timely selections based on physiological conditions for termination, acceptable treatment at birth, and prompt transfer to units specialized within the care of the newborn. 8
In western medicine, ultrasound has achieved nearly universal coverage in obstetrics, wherever routine screening has become an integral part of prenatal examination after each pregnant woman (. 9 However, the use of ultrasound in developing countries is limited by several factors. According to a world health organization report, women in Sub-Saharan Africa still embrace early physiological conditions due to factors that vary from individual challenges in health-seeking behaviors to health facility capacity limitations and unclear national policies. 10 In addition, in low-income countries [LICs], factors such as the high cost of ultrasound equipment, the fee to use ultrasound in a private clinic, lack of trained sonographers or physicians, and the skill required to perform the examinations have been among the barriers to its use.11,12
Ethiopia is undertaking many activities to improve the quality of maternal health care service utilization, reduce maternal and neonatal morbidity and mortality, and achieve sustainable development goals. 13 However, there's still a high share of maternal and neonatal morbidity and mortality which might result from the poor utilization of prenatal ultrasound scans to stop the complications of physiological condition. There are only a small number of published studies tha have reported the use of prenatal ultrasound in low-resource settings and no studies that assessed the utilization of prenatal ultrasound and its associated factors in Ethiopia. Therefore, this study aimed to determine the prevalence of prenatal ultrasound utilization and its associated factors among pregnant women attending ANC in Jimma town public health care facilities.
Methods
Study Design, Area, and Period
A prospective cross-sectional study was conducted at Jimma town public health institutions from July to August 2021. The town is found in the Jimma zone, southwestern Ethiopia, and is approximately 352 km away from Addis Ababa the capital city of Ethiopia. The town has five public health centers and two public hospitals (one referral and one district). The referral hospital serves as a referral site and provides specialized care for southwestern Ethiopia, with a catchment population of approximately 15 million. At the health centers, pregnant women from the nearby urban and rural communities are seen, and primary health care services (including ANC, delivery services, postpartum care, and family planning) to all population groups are provided. According to the 2007 census of Ethiopia, the total population of Jimma is 182 942 from these male accounts 91 771 and Female accounts 91 171. The main language spoken in the town is Afan Oromo and Amharic.
Study Participants
All pregnant women attending antenatal care services at Jimma town public health facilities were the source population of the study, while pregnant mothers who were available during the data collection period were considered as the study population.
Sampling Technique and Sample Size Determination
Sample size determination
The sample size was calculated based on a single population proportion formula using the following assumptions. The utilization of prenatal ultrasound was taken p = 50%.



n = initial sample size, nf = final sample size
Following the addition of a 10% non-response rate the final sample size was 303.
Sampling techniques
Five public health centers and two public hospitals (one referral and one district) were found in the town. Two public health centers and one referral hospital were randomly selected. The allocation of the sample to health facilities was performed proportionally based on the average number of clients who received antenatal care at each facility in the month preceding the data collection period. A systematic sampling technique was used to select study participants. The respondents were selected in the order by which they came to health facilities. Participants’ card numbers were used to systematically select study participants every K interval taking K = N/n = 957/303) 3.16≈3 (where N is the source population and n is the sample size for this study).
Study Variables
Dependent variable
Prenatal ultrasound utilization
Independent variables
Socio-demographic factors: age, religion, ethnicity, educational status, marital status, educational status of husband, respondent's occupation, residence
Obstetric and other factors: parity, gestational age, previous obstetrics related complication, attitude towards prenatal ultrasound, knowledge of obstetrics ultrasound.
Operational Definitions and Definition of Terms
Knowledge of obstetric ultrasound: Respondents who answered greater than 50% of questions provided for them regarding knowledge are considered as having good knowledge. While those answers below 50% are those with poor knowledge of obstetric ultrasound. 14
Attitude towards obstetric ultrasound: The respondents whose responses are ‘agree’ to >50% of questions regarding attitude provided are categorized as having a good attitude toward obstetric ultrasound; whereas those whose responses are ‘agree’ to <50% /disagree to the majority of questions are considered those with poor attitude toward obstetric ultrasound. 14
Obstetric ultrasound: It is also known as prenatal ultrasound, is the use of medical ultrasonography in pregnancy, in which sound wave is used to create a real-time visual image of the developing embryo or fetus in the uterus (womb). The procedure is a standard part of prenatal care in many countries, as it can provide a variety of information about the health of the mother, the timing and progress of pregnancy, and health and development of the embryo or fetus. 15
Data Collection Methods and Instruments
Data were collected using a semi-structured and pretested questionnaire through face-to-face interviews after the study participants received antenatal care services. The tool was first prepared in English and then translated into the local language (Afan Oromo). The tool comprises socio-demographic variables, obstetric history of mothers, Information on prenatal ultrasound utilization, mothers’ knowledge, and attitude toward Obstetric ultrasound. A one-day training session was given for both data collectors and supervisors about the methodology and questionnaire by the investigators.
Data Quality Control
The quality of data was assured before data collection, during data collection, and after data collection. Before data collection, the questionnaire was translated into the local language, a pretest was conducted on 5% (17) of the sample size other than the study area and one-day training was provided for data collectors and supervisors. During data collection, close follow-up was performed by supervisors and the principal investigator. After data collection, data were checked for completeness, and using epi data also helps to automatically detect errors made during data entry.
Data Analysis
Data were entered into Epi data version 3.3.1 software after coding and checking completeness and exported to the statistical package for social science (SPSS) version 21.0. Descriptive statistics were obtained and are presented using narratives, tables, and figures. Binary Logistic regression was used to determine the crude association between prenatal ultrasound use and explanatory variables. Explanatory variables that had a P-value of less than .25 and fulfill the assumption of logistic regression from bi-variable logistic regression were considered for the multivariable logistic regression model. The strength of association was evaluated using an odds ratio at a 95% confidence interval and P-value < .05 was considered to indicate significant associations.
Results
Socio-Demographic Characteristics of the Study Participants
A total (303) pregnant women participated in this study. The mean age of the study participant was 26.3 years with a minimum of 16 years and maximum of 43 years. One hundred-eighty-six (61.4%) were living in urban areas. The majority of the respondents (95.4%) were married in their marital status and 156 (51.5%) of the respondents were housewives. The educational level of the interviewed respondents varied from illiterate to above secondary school, and 68(22.4%) of them were illiterate. One hundred (33%) of the husbands’ have above attended secondary school. The remaining socio-demographic characteristics are listed in Table 1.
Socio-Demographic Characteristics of Pregnant Women at Jimma Town Public Health Institution, Ethiopia, 2021. (N = 303).

Obstetric History of the Study Participants
Two hundred forty-three (80.2%) of the respondents were multigravida. Eleven (4.7%) of the respondents had a history of congenital anomaly birth while fifty-seven (18.8%) mothers had a history of abortion. Twenty-five (10.7%) of the mothers had experienced illness during their previous pregnancy and delivery (Table 2).
Obstetric History of Pregnant Women at Jimma Town Public Health Institution, Ethiopia, 2021.

Knowledge of Obstetric Ultrasound
One hundred ninety (62.7%) of the respondents know about obstetric ultrasound. The sources of information for prenatal ultrasound were, Health Professional 147(76.2%), health extension worker 18(9.4%), Radio/TV 12(6.2%), Relatives 8(4.1%) & Others 8 (4.1%). Regarding the knowledge about the recommended gestational age for a routine prenatal ultrasound scan, 89 (46.6%) reported during the first three months of pregnancy (Table 3).
Knowledge on Prenatal Ultrasound among Pregnant Women at Jimma Town Public Health Institution, Ethiopia, 2021.

Attitude Towards Obstetric Ultrasound
The majority (77%) of study participants had a good attitude towards prenatal ultrasound scanning (Figure 1).

Attitude toward obstetric ultrasound among pregnant women in jimma town, Ethiopia, 2021.
Prenatal Ultrasound Utilization
One hundred eighty-four (60.7%) of respondents used prenatal ultrasound during their pregnancy, out of which 109(59.2%) were requested by clinicians. Time (GA) of first O/U utilization of 44(23.9%) of the respondents were during their third trimester (after 24weeks) (Table 4).
Utilization of Prenatal Ultrasound among Pregnant Women at Jimma Town Public Health Institution, Ethiopia, 2021.

Factors Associated with Utilization of Prenatal Ultrasound
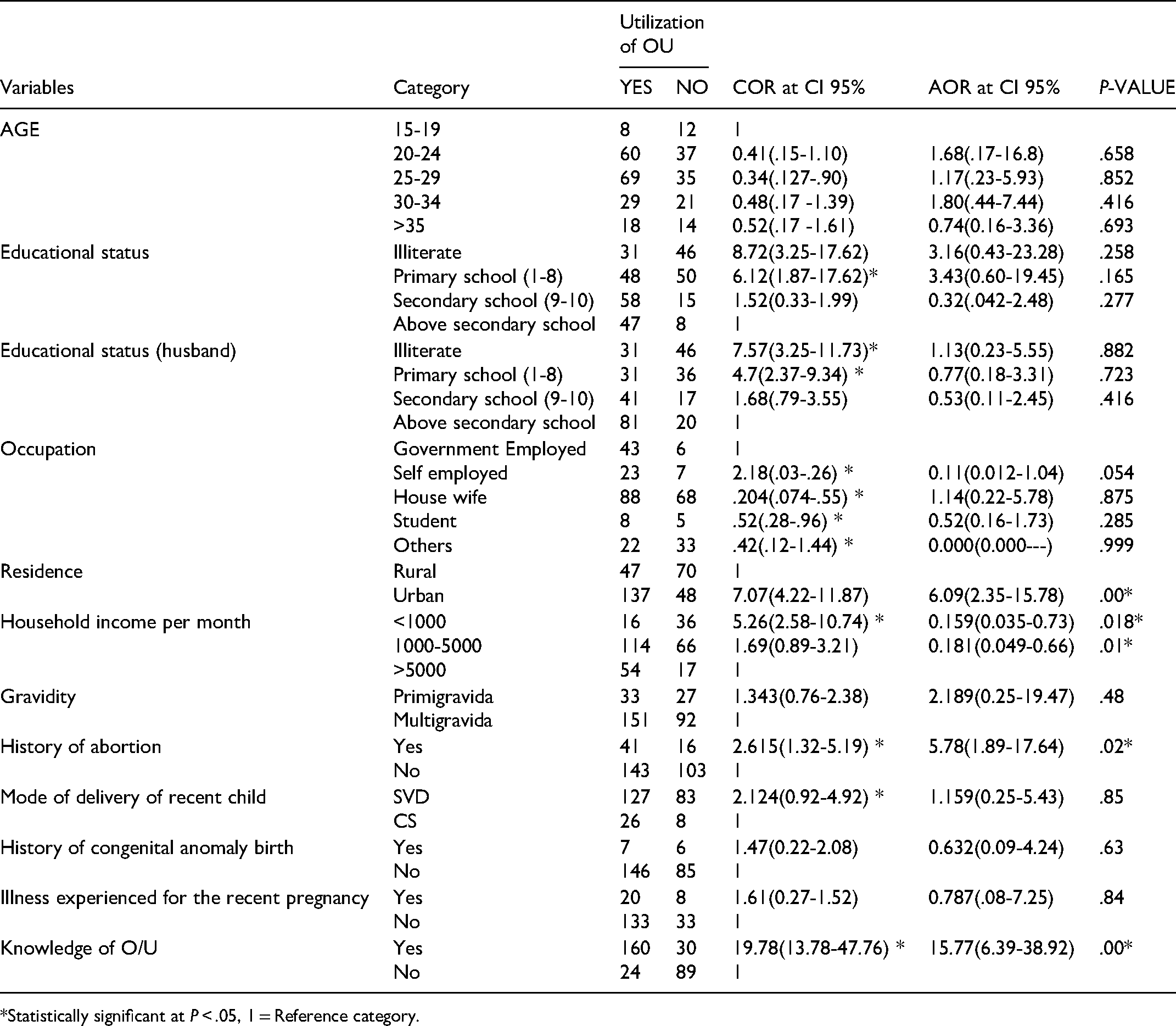
In bivariate logistic regressions, nine variables were associated with the utilization of obstetric ultrasound: women's educational status, husband's educational status, residence, occupation and household monthly income, gravidity, history of abortion, mode of delivery of previous birth, and knowledge of obstetric ultrasound.
Respondents whose educational status above secondary school were nearly eight times more likely to use prenatal ultrasound compared to those with no formal education COR = 8.72 (95%CI: 3.25 - 17.62). Similarly, pregnant women whose husbands had above secondary school education status were more likely to utilize prenatal ultrasound compared to those whose husbands were illiterate COR = 7.57(95%CI: 3.25- 11.73), However, in multivariate analysis only five variables were associated with the utilization of obstetric ultrasound; residency, household monthly income, history of at least one abortion, and knowledge of prenatal ultrasound showed significant association with utilization of obstetric ultrasound. The odds of the utilization of prenatal ultrasound among pregnant women who reside in urban areas were six times higher compared to residing in rural areas AOR = 6.09 (95%CI = 2.35-15.78). Those respondents with a history of at least one abortion were nearly six times more likely to utilize prenatal ultrasound than their counterparts AOR = 5.78 (95% CI: 1.89– 17.6). Similarly, women who had good knowledge of prenatal ultrasound were nearly sixteen times more likely to utilize prenatal ultrasound when compared with their counterparts AOR = 15.77 (95% CI: 6.39-38.92). The binary and multivariable regression outputs of the different independent variables with the utilization of prenatal ultrasound are shown in Table 5.
Bivariate and Multivariate Analysis of Utilization of Prenatal Ultrasound and Other Determinant Factors among Pregnant Women Attending ANC in Jimma Town Public Health Institution, Ethiopia, 2021.
*Statistically significant at P < .05, 1 = Reference category.
Discussion
This study aimed to assess the utilization of prenatal ultrasound and its associated factors among pregnant women attending ANC in Jimma town public health institutions. The proportion of prenatal ultrasound utilization in this study was 60.7%[(95% CI); (55.4%-66%)]. This study is consistent with the findings of prenatal ultrasound utilization recorded in the southeast of Nigeria 58%. 16 However, the finding of the current study was lower than studies conducted in Uganda, 17 Zaria Local Government, Kaduna State, Northern Nigeria (83.5%), 18 a cross-sectional study in rural Eastern China 96.1%, 19 and the United Kingdom 96% 20 This variation may probably due to socio-demographic differences between Ethiopia and the four countries. Moreover, the discrepancy may be due to variations in the sample size and the health service system. In contrast, the finding of the current study was higher than studies conducted in Kenya suggested that utilization of prenatal ultrasound was 49.7%. 21 The possible reason for this discrepancy may be due to the variation in health policy towards maternal and child health care in Kenya and Ethiopia.
The finding of this study revealed that there was a strong association between participants’ knowledge of prenatal ultrasound and the utilization of prenatal ultrasound. Mothers who had good knowledge were 15.8 times more likely to utilize prenatal ultrasound than their counterparts. This finding is consistent with the results of different studies conducted in semi-urban pregnant women in developing nations, 22 at a peri-urban health centers in Uganda, 23 and Nigeria. 24 This may be due to the fact that those with a good knowledge of prenatal ultrasound knew its purposes and they are eager and readily go for it even when their doctor has not requested it. Hence, providing information on prenatal ultrasound in rural community is paramount.
Women's residency was another explanatory variable that was significantly associated with the utilization of obstetric ultrasound. In this study, women living in urban areas were six times less likely to utilize prenatal ultrasound than those living in rural areas AOR = 6.09 (95% CI: 2.35-15.78). This is probably due to the accessibility of better information and awareness about prenatal ultrasound in urban areas than in rural areas and the variation in the distance of the health facilities. Another reason may be the low expansion of infrastructure in the rural parts of our country compared to urban areas. Therefore, the ministry of health and/or other stakeholders should focus to address health information's and infrastructures for the rural community.
Another sociodemographic variable associated with prenatal ultrasound utilization was monthly household income. Respondents’ household income below and 5000ETB were less likely to utilize prenatal ultrasound than those who had a household monthly income above 5000 ETB. A consistent finding was reported in a study conducted in Kenya on barriers and enablers that influence the utilization of ultrasound screening services. 21 This may be because high household income increases the ability of women to cover their travel expenses, pay ultrasound service fees, and easily access prenatal care services.
This study also showed that history of abortion had a statistically significant association with prenatal ultrasound utilization. Those respondents with a history of abortion were 5.78 times more likely to utilize prenatal ultrasound than their counterparts. This might be because of the perceived fear of losing their pregnancy and the complications associated with it. Furthermore, mothers with a history of abortion might feel that their abortion was related to poor utilization of ANC service.
Strength and Limitations of the Study
Being the first study to assess the situation in Ethiopia and the study area, in particular, is the major strong side of this study. In addition, the study tried to include public health facilities where most pregnant women in Ethiopia receive antenatal care. Regarding limitations, since the study design was an institutional-based cross-sectional study, the study does not represent those women who had antenatal care visits at a private clinic. Moreover, the study shares the limitations of cross-sectional study design
Conclusions
In the current study, the proportion of prenatal ultrasound utilization during pregnancy was low as compared to the world health organization (WHO) recommendation. Residency, household monthly income, mother's history of at least one abortion, and knowledge towards prenatal ultrasound Therefore, the author recommended that educating mothers on the purposes of obstetric ultrasound and including a prenatal ultrasound screening as part of antenatal care is needed.
Footnotes
Acknowledgments
First, we would like to express our heartfelt gratitude to study participants to devote their time to answer numerous and private questions and Jimma town public health institutions. Secondly, we would like to express our deepest gratitude to data collectors for their devotion and patience during the data collection period.
Author Contribution
All authors contributed to the study conception and design. Aynalem Yetwale: Software and Writing- Original draft preparation, Tola Kabeto: Data curation. Tsegaw Biyazen: Supervision. Writing- Reviewing and Editing. Belete Fenta: Supervision. Writing- Reviewing and Editing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Institution of health science, Jimma University. In this study, the funders did not have any role in the study design, data collection, analysis, or interpretation of the data, or in the writing of the manuscript.
Ethical Considerations
Ethical clearance and permission were obtained from the Ethical review committee of Jimma University, school of midwifery. Study participants were informed about the objectives, benefits, risks, and their right to the decision of participating in the study. Also, the study subjects were informed their responses will be coded and used only for only research purposes. Participants name was made anonymous to affirm confidentiality throughout the study. Moreover, informed written consent was taken before data collection started.