
Abstract
Individuals with hearing loss, even when using hearing aids, often perceive pleasant environmental sounds as less pleasant than do those with normal hearing. This bias in emotional response may negatively impact well-being, leading to decreased social participation and increased loneliness. The present study examined whether the Positive Focus intervention—encouraging hearing aid users to focus on positive listening experiences—could influence emotional response to environmental sounds. Thirty participants were randomly assigned to either a Positive Focus or a Control group. At the initial laboratory visit, all participants were fitted with study hearing aids and performed affective ratings of 120 environmental sounds. Over 3 weeks, both groups wore the hearing aids; the Positive Focus group additionally reported daily positive listening experiences via a text message. At the end of the three-week period, participants completed questionnaires on hearing aid outcomes and repeated the affective ratings. The Positive Focus intervention did not alter emotional responses to environmental sounds in a laboratory setting. However, regression analyses revealed that valence ratings of typically pleasant sounds moderated the effectiveness of Positive Focus on hearing aid benefit; the intervention was more effective for individuals less naturally inclined to respond positively to such sounds. These findings suggest that valence screening may help identify individuals most likely to benefit from Positive Focus, supporting more personalized hearing care strategies.
Introduction
Hearing loss is a prevalent sensory impairment that affects not only speech perception but also the emotional experience of sound. Increasing attention is being given to how people with hearing loss perceive everyday environmental sounds—such as birdsong, rainfall, or music—which often feel less emotionally engaging, even when hearing aids are used (Marcrum et al., 2025; Picou, 2016; Picou et al., 2021; Tawdrous et al., 2022). For instance, Picou and Buono (2018) demonstrated a link between the severity of hearing loss and emotional reactivity to sound, with greater degrees of hearing loss associated with lower valence (i.e., pleasantness) ratings for non-speech auditory stimuli expected to evoke pleasant responses. Additionally, individuals with hearing loss tend to exhibit a narrower range of emotional responses to environmental sounds, showing less sensitivity to both pleasant and unpleasant stimuli compared to their peers with normal hearing (Tawdrous et al., 2022). Building on these findings, Lelic and Marmel (2026a) observed that both hearing aid users and individuals with hearing difficulties who do not use hearing aids tend to find everyday listening situations as less pleasant compared to those without hearing difficulties.
These changes in emotional responses to sound carry clinical significance, as emotional responses to auditory stimuli have been tied to psychological well-being and social functioning. Higher valence ratings have been linked to lower levels of both objective social isolation (i.e., reduced social network size) and subjective isolation (i.e., loneliness) (Picou & Buono, 2018). This connection is especially pertinent for individuals with hearing loss, who frequently report negative social experiences such as fatigue, exclusion, and a sense of loss (Bennett et al., 2022). Communication difficulties often lead to avoidance of social interactions, driven by feelings of embarrassment or shame (Bennett et al., 2022; Heffernan et al., 2016), which over time can result in deeper social isolation. Social isolation, in turn, poses a chronic threat to both physical and mental health. It has been associated with increased risks of cardiovascular disease, cognitive decline, depression, and mortality (Bassuk et al., 1999; Gopinath et al., 2013; Perissinotto et al., 2012; Tomaka et al., 2006; Uchino et al., 1996; Wang et al., 2002; Wilson et al., 2007; Zhang et al., 2007). These findings point to the importance of understanding and enhancing emotional response to sound as a potential pathway to improving quality of life for individuals with hearing loss.
Recent work by Lelic and Marmel (2026a) has further highlighted the nuanced role of emotional sensitivity to sound in shaping auditory social experiences. Their findings suggest that heightened sensitivity to both positive and negative emotional sounds may complicate emotional communication, potentially making it more difficult for individuals to interpret or express affective cues in auditory contexts. Notably, perceiving typically negative sounds more positively was associated with more enjoyable everyday listening experiences and better mental well-being. This aligns with broader psychological literature indicating that emotional resilience and adaptive affective processing can buffer against stress and promote psychological health (Feng & Wang, 2025; Saskovets et al., 2025).
Taken together, these findings suggest that interventions aimed at enhancing emotional responses to sound may offer a promising avenue for improving both social and psychological outcomes in people with hearing loss. One such intervention is the Positive Focus approach, which directly targets emotional engagement with sound by encouraging a shift in attention toward positive auditory experiences. Designed to enhance hearing aid outcomes by counteracting negativity bias—a cognitive tendency to prioritize negative over positive experiences (Rozin & Royzman, 2001)—the Positive Focus intervention encourages hearing aid users to actively attend to and report positive listening experiences in daily life.
Randomized controlled trials have shown that Positive Focus significantly improves hearing aid satisfaction and perceived benefit (Lelic et al., 2023, 2024a), as well as speech-in-noise performance (Lelic et al., 2024b). While Positive Focus has demonstrated benefits for both subjective and objective hearing aid outcomes, its potential to shape affective auditory experiences remains underexplored. Hence, the primary aim of the present study was to investigate whether the Positive Focus intervention can also affect the perceived pleasantness of environmental sounds in hearing aid users. A secondary aim was to further investigate whether the Positive Focus intervention improves hearing aid satisfaction and self-reported benefit, with the broader goal of providing additional evidence for its effectiveness. Additionally, we explored how individual differences in emotional response to sound may influence the outcomes of the Positive Focus intervention, emphasizing the potential role of affective auditory experiences in shaping self-reported hearing aid benefit.
Methods
An ethical waiver for conducting the study was obtained from the Research Ethics Committee of the Capital Region of Denmark (case no. H-18056647).
Study Design
Figure 1 illustrates the study flow. A randomized, single-blind, parallel-arm design was employed. Participants were unaware of the study's true purpose and that they were assigned to one of the two groups—either the Control group or the Positive Focus group. All participants were informed that the study aimed to explore how individuals with hearing impairment emotionally respond to sound, both with and without hearing aids. The study included two laboratory visits separated by a three-week field trial.
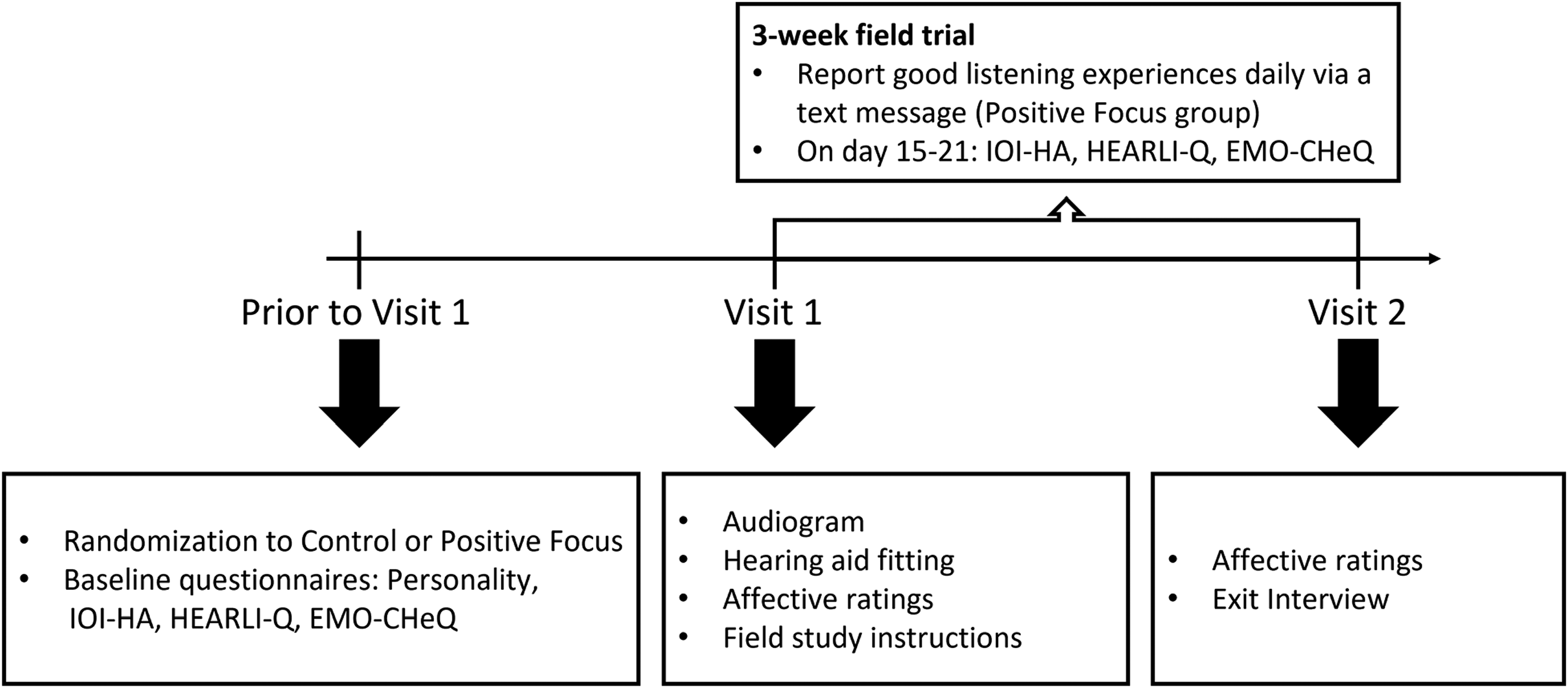
The study flow. Abbreviations: IOI-HA = international outcome inventory for hearing aids; HEARLI-Q = hearing-related lifestyle questionnaire; EMO-CHeQ = emotional communication in hearing questionnaire.
Participants
Thirty participants were randomized into a Control (N = 15; age: 72.5 ± 7.0 years; 10 males, 5 females) or Positive Focus (N = 15; age: 74.3 ± 8.8 years; 10 males, 5 females) group. Audiograms of the two groups are shown in Figure 2. All participants were bilateral hearing aid users. Inclusion criteria included having a bilateral sensorineural hearing loss within the fitting range of the study hearing aids (approximately mild-to-severe hearing loss, corresponding to audiometric thresholds up to ∼95–110 dB HL across 125 Hz–8 kHz, depending on receiver configuration), 40–85 years of age, and fluency in Danish. Exclusion criteria included: fluctuating hearing loss; severe cognitive impairment—identified through the research audiologist's clinical judgement during the initial visit—that could hinder task performance; complex auditory conditions such as Ménière's disease; and prior participation in studies involving the Positive Focus intervention (Lelic et al., 2023, 2024b). Participants were informed about the study procedures, associated risks, and compensation both orally and in writing. Before the trial commenced, the participants gave written informed consent.

Audiograms by group. Right ear audiograms are shown in the left panel, and left ear audiograms are shown in the right panel. Thick lines indicate group averages, while thin lines show individual audiograms.
Baseline Questionnaires
Before attending their first laboratory visit, all participants received an email containing links to baseline questionnaires hosted on Enalyzer (www.enalyzer.com). These questionnaires were administered to compare the two groups at baseline and to ensure they were balanced across various characteristics that could influence the study's outcomes. Participants were instructed to complete the questionnaires prior to their initial visit. If they had not done so beforehand, they were given the opportunity to complete them at the laboratory during their first visit.
The baseline questionnaires included:
Big Five Inventory (BFI): A 44-item measure of personality traits—extraversion, agreeableness, conscientiousness, neuroticism, and openness. Each trait score is calculated as the mean of its items, ranging from 1 to 5, where higher scores indicate stronger expression of the respective trait. The English version is highly reliable and externally valid (Rammstedt & John, 2007). The questionnaire has been translated into Danish using a forward–backward method (Lelic et al., 2023). International Outcome Inventory for Hearing Aids (IOI-HA): A 7-item tool widely used to assess hearing aid effectiveness. The Danish version is psychometrically comparable to other validated translations (Jespersen et al., 2014). A total score (range: 7–35) reflects overall hearing aid benefit (Cox et al., 2000), with higher scores indicating more benefit. Hearing-Related Lifestyle Questionnaire (HEARLI-Q): Assesses hearing experiences across 23 everyday listening situations using four dimensions: lifestyle richness and hearing demand (both ranging from 0 to 100), hearing difficulty (0–4), and satisfaction (1–5). Higher scores indicate greater richness, demand, difficulty, and satisfaction. Scores are based on Likert-scale ratings, and the four dimensions have demonstrated strong test-retest reliability (Lelic et al., 2022). For the present study, a fifth dimension, pleasantness, was added, with participants rating how pleasant each of the 23 listening situations typically feels on a 9-point scale (1 = extremely unpleasant to 9 = extremely pleasant, with 5 as neutral); an overall pleasantness score was calculated as the average across all situations. Emotional Communication in Hearing (EMO-CHeQ): A 16-item questionnaire assessing hearing-related handicap in emotional vocal contexts. Respondents rate each item on a 5-point Likert scale, and the overall score is calculated as the average of all items, ranging from 1 to 5. Higher scores reflect greater perceived handicap. The English version is reliable and ecologically valid (Singh et al., 2019). For this study, the EMO-CHeQ was translated into Danish using a forward–backward method involving four bilingual translators and consensus meetings to ensure linguistic and conceptual equivalence.
Visit 1
During the initial laboratory visit, hearing was tested using pure-tone, air conduction threshold testing. Following this, participants were fitted bilaterally with Widex MOMENT MRB2D 440 receiver-in-canal hearing aids. To minimize variability related to hearing aid brand, model, and fitting procedure, all participants received the same device model fitted by the same audiologist. The devices were programmed to match the participant's hearing loss using Compass GPS fitting software (version 4.8), in accordance with Widex's fitting protocol. This process included a feedback test and measurement of in-situ hearing thresholds (Sensogram) to account for the unique acoustic characteristics of each ear canal (Kuk, 2012). Receiver types and ear tips were selected based on recommendations from the fitting software or the research audiologist's clinical judgment. After the fitting, participants performed the affective rating task under both aided and unaided conditions. The order of the aided and unaided conditions was pseudorandomized and counterbalanced. A break was taken between the two conditions. Finally, participants were introduced to the field task.
Affective Rating Task
Participants were informed that they would be evaluating a series of sounds based on their emotional reactions, specifically along two dimensions: valence (the degree of pleasantness or unpleasantness) and arousal (the level of calmness or excitement). To support these evaluations, the Self-Assessment Manikin (SAM) scale (Bradley & Lang, 1994) was employed. This scale uses five pictorial figures per dimension to visually represent a spectrum of emotional states. The valence scale and the arousal scale were displayed together, with all SAM figures visible at the same time. The valence scale was displayed at the top of the screen (ranging from very unhappy to very happy), and the arousal scale below it (ranging from very calm to very excited). Each dimension was rated using a 9-point Likert scale. The scale shown to participants was labeled between −1 and 1 (see Figure 3), with the endpoints corresponding to the most extreme figures. Higher scores reflected more positive valence or greater arousal.
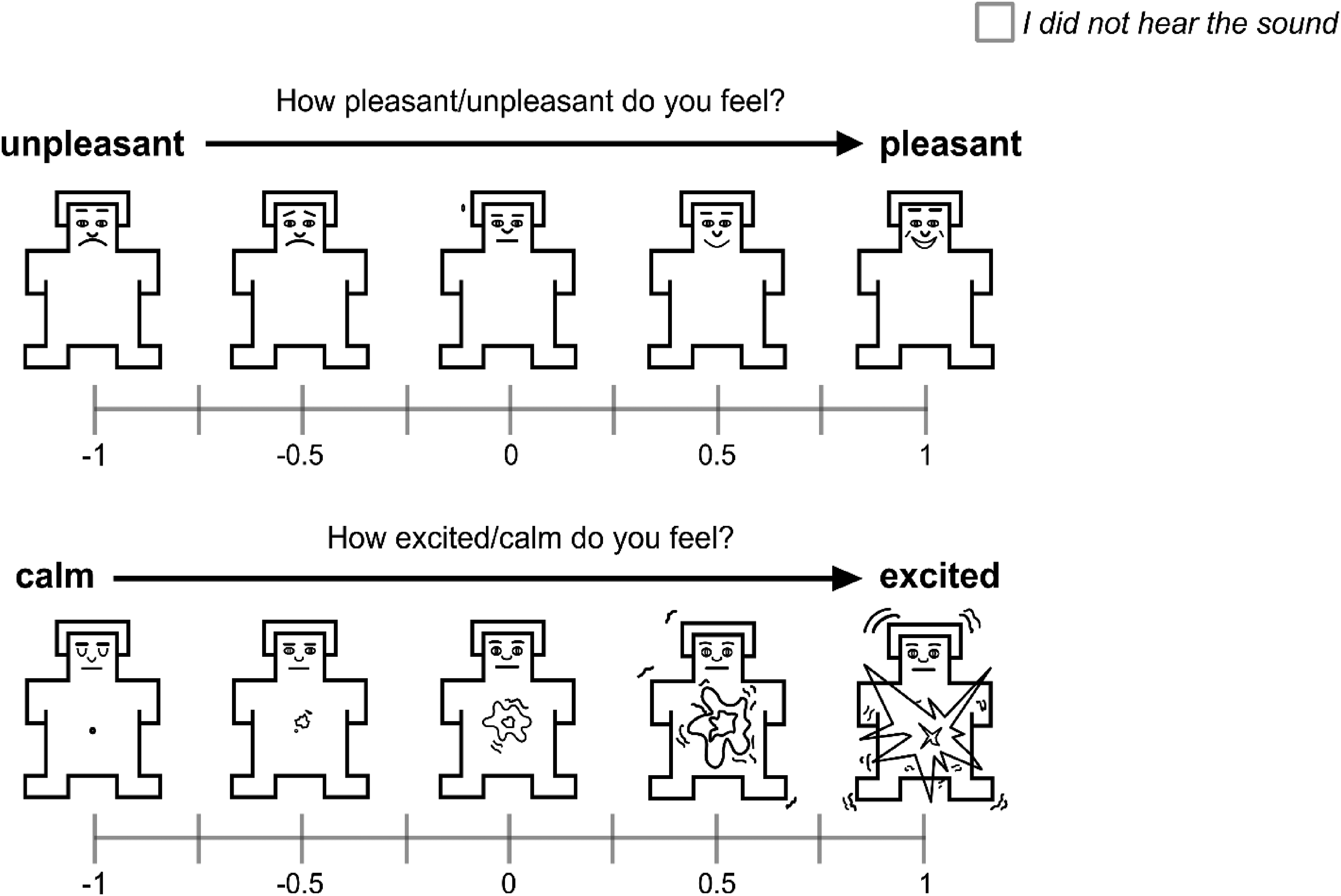
This figure depicts how valence (top) and arousal (bottom) scales were presented on the screen. Each time participants listened to a sound, both scales were displayed for them to provide their ratings. Participants could indicate that they did not hear the sound in the top right corner of the screen.
To ensure understanding, the concepts of valence and arousal were explained with examples. For valence, participants were told that a sound such as birdsong, if perceived as very pleasant, should be rated using the figure on the far right (with a high numerical score); conversely, if a loud siren was perceived as very unpleasant, it should be rated using the figure on the far left (with a low numerical score). For arousal, a gentle breeze might be considered calming (left side), while a loud explosion might be rated as highly exciting (right side). It was emphasized that valence and arousal are independent dimensions—a sound could be high in arousal and either pleasant (e.g., laughter and upbeat music) or unpleasant (e.g., a child crying and a gunshot).
Emotional ratings were collected in response to non-speech auditory stimuli from the Marcell corpus (Marcell et al., 2000), which includes 120 sound samples such as animal vocalizations, human social sounds, bodily noises, environmental sounds, and music. These sounds vary in duration—from brief events (e.g., cork popping, 137 ms) to longer recordings (e.g., helicopter, 5.937 s)—preserving their natural temporal characteristics. We categorized each sound by expected valence (pleasant, unpleasant, and neutral) and arousal (high, low, and neutral) based on normative data from older adults with self-reported normal hearing (Lelic & Marmel, 2026b).
Before beginning the main task, participants completed a short familiarization phase, rating three practice sounds (from an internal environmental sound database not used in subsequent data collection) on both emotional dimensions. They then proceeded to rate all 120 experimental sounds, which were presented in a randomized order without replacement. A mandatory one-minute break was provided after every 30 sounds. If a participant was unable to hear a sound, they could select the option “I did not hear the sound” to skip it.
The individual stimuli were allowed to vary in volume to retain their unique characteristics, with the overall presentation level across stimuli set to 65 dB SPL. The standard deviation of levels across all stimuli was 5 dB, and there was a 30-dB difference between the quietest and the loudest stimulus. The presentation level was calibrated using a steady-state broadband signal and verified using a sound level meter with no frequency weighting positioned at ear height in the test booth, without a participant present. Auditory stimuli were delivered via a loudspeaker positioned ∼1 m in front of the participant at 0° azimuth. Participants recorded their valence and arousal ratings using a laptop placed in front of them.
Field Trial
Participants were instructed to wear the study hearing aids for a three-week period following the fitting. After 2 weeks, they received an email prompting them to complete the IOI-HA, HEARLI-Q, and EMO-CHeQ questionnaires, reflecting on their experiences with the hearing aids. They were asked to submit their responses before attending Visit 2 at the laboratory. Alternatively, they had the option to complete the questionnaires upon arrival.
For the three-week field trial, only the Positive Focus group received additional instructions. They were asked to focus on positive listening experiences and to report them daily via a text message. The instructions were as follows: For the next three weeks you will be wearing these hearing aids instead of your own. During these three weeks, I am very interested to hear about the situations in which the hearing aids are helping you. Therefore, I would like to ask you to focus on the good listening experiences you encounter, and sometime throughout each day, report these to me by text. You can include as many good experiences as you want. It can be any good experience, from being able to hear sounds of nature, or environmental sounds such as water dripping from a tap, to understanding speech. It could also be situations in which you notice the hearing aids are helping you and where you notice your hearing is better than before. Don’t be afraid to repeat situations. I’d love to hear about any experience more than once, if you encounter it multiple times. After two weeks, I will send you a set of questionnaires to answer, and then you will come back and do another round of listening tests.
In contrast, the Control group received the following instructions: For the next three weeks you will be wearing these hearing aids instead of your own. Please go about your daily life as usual. After two weeks, I will send you a set of questionnaires to answer, and then you will come back and do another round of listening tests.
Participants received the instructions both verbally and in written form. If a participant in the Positive Focus group did not submit their daily text for 2 consecutive days, the research audiologist followed up to remind them of their task.
Visit 2
During the second visit, participants completed the affective rating task again, this time exclusively in the aided condition. This was followed by an exit interview, during which they were asked two questions:
Can you recall some good listening experiences you have had during the last three weeks? Can you recall some difficult listening experiences you have had during the last three weeks?
After the interview, participants returned the study equipment, and data on hearing aid usage was retrieved from the device logs.
Data Analysis
No a-priori power analysis was conducted because valence data based on the Marcell database for hearing aid users were not available at the time the study was designed. In the absence of such baseline information, the study was structured around a robust repeated-measures design, with the intention to evaluate sample-size adequacy after data collection if the resulting patterns suggested a need for further assessment of statistical power. For the questionnaire-based secondary outcomes, sample-size expectations were guided by previous Positive Focus studies using the HEARLI-Q and IOI-HA (Lelic et al., 2023, 2024a), where power analyses were done showing that cohorts of 10–20 participants provide adequate power.
Baseline characteristics of the two groups were compared using appropriate statistical tests to evaluate potential differences between groups. Additionally, hearing aid usage time during the field trial was examined, given its potential influence on hearing aid outcomes. A summary of these comparisons, including the specific statistical methods applied, is presented in Table 1.
Baseline Characteristics of the Two Groups.
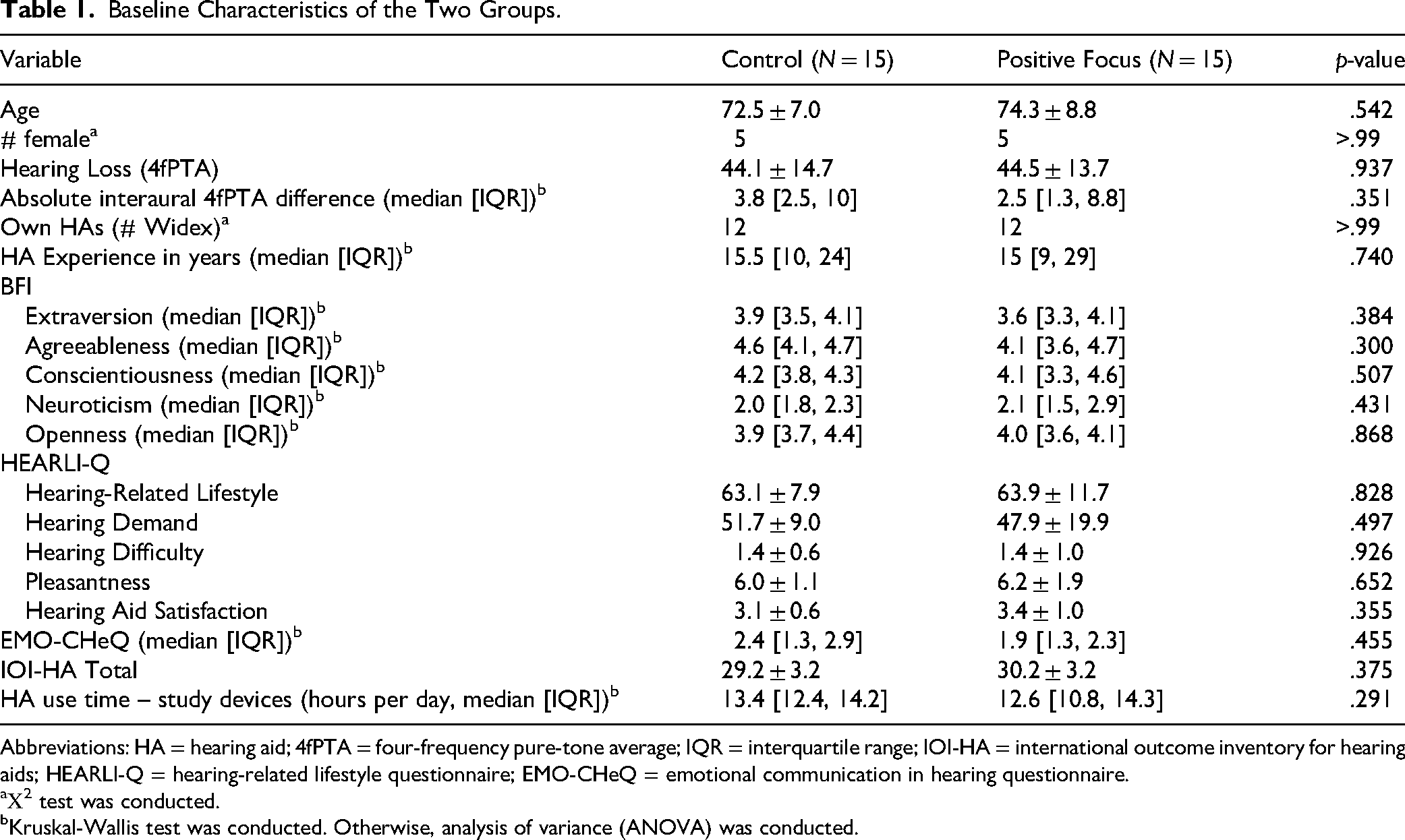
Abbreviations: HA = hearing aid; 4fPTA = four-frequency pure-tone average; IQR = interquartile range; IOI-HA = international outcome inventory for hearing aids; HEARLI-Q = hearing-related lifestyle questionnaire; EMO-CHeQ = emotional communication in hearing questionnaire.
Χ2 test was conducted.
Kruskal-Wallis test was conducted. Otherwise, analysis of variance (ANOVA) was conducted.
Although data were collected for both valence and arousal under aided and unaided conditions, the scope of this study was restricted to analyzing valence responses in the aided condition. This decision is based on previous research showing minimal effects of hearing loss and hearing aids in the arousal dimension (Picou, 2016; Picou et al., 2021; Tawdrous et al., 2022), suggesting that valence may be the more relevant target for intervention. For readers interested in the full dataset, results for arousal and unaided conditions, along with statistical details, are provided in Supplemental Figures 1 and 2 and Supplemental Tables 1 and 2.
Results From the Mixed-Effects Analyses.
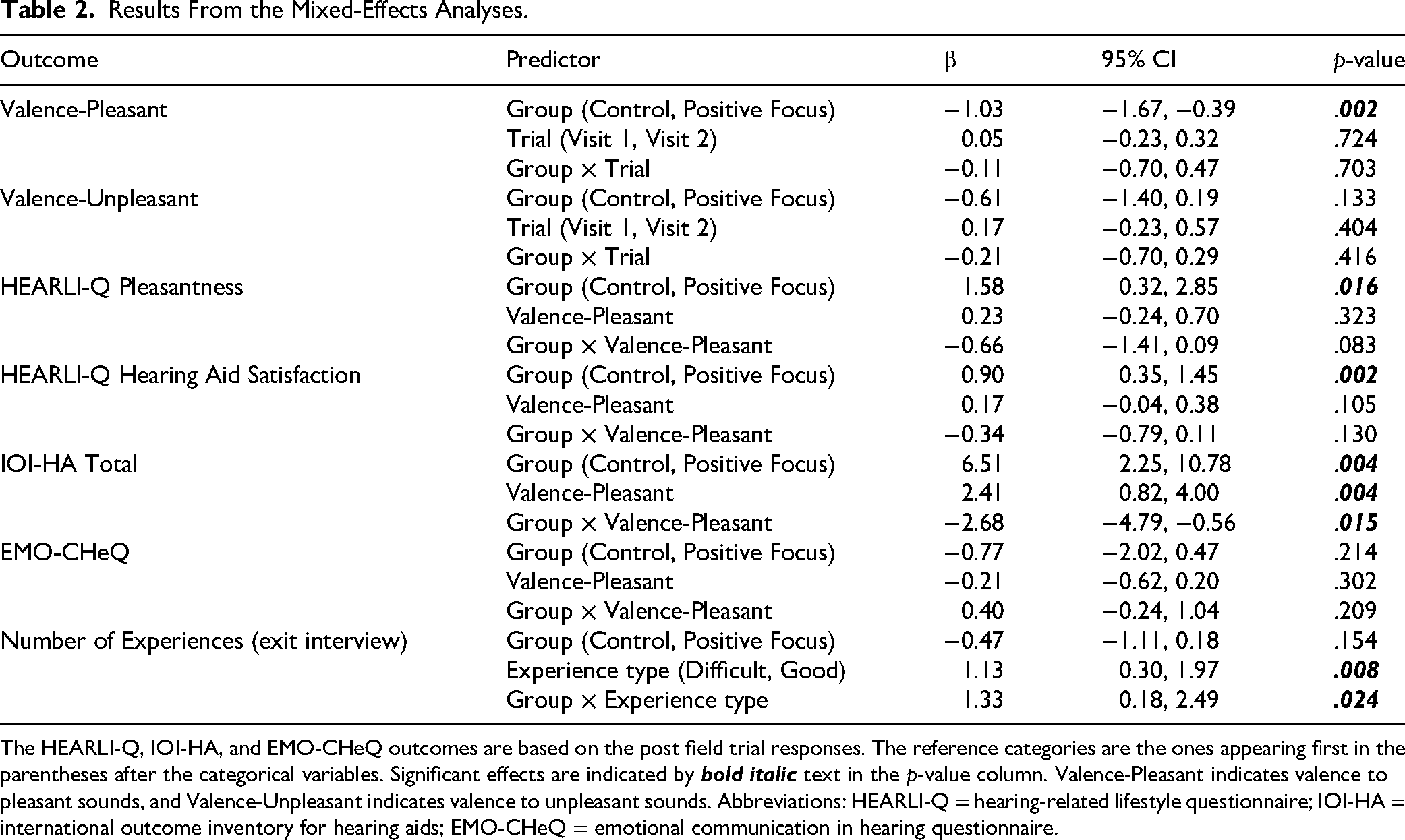
The HEARLI-Q, IOI-HA, and EMO-CHeQ outcomes are based on the post field trial responses. The reference categories are the ones appearing first in the parentheses after the categorical variables. Significant effects are indicated by
To assess the effects of group (Control vs. Positive Focus), trial (Visit 1 vs. Visit 2), and their interaction on valence ratings for pleasant and unpleasant sounds, two mixed-effects linear regression models were conducted. In these models, valence ratings for pleasant and unpleasant sounds served as the outcome variables, while group and trial were the explanatory variables.
To examine group differences in pleasantness of everyday listening situations and hearing aid satisfaction (both derived from HEARLI-Q), the IOI-HA total score, and the EMO-CHeQ score, four separate mixed-effects linear regression models were conducted. In each model, the questionnaire outcome was the outcome variable, and group was the explanatory variable. To account for potential bias from response imbalances in the affective ratings task, any affective ratings that differed by group were included as covariates in the respective models. Because these models were included to explore the robustness of the findings rather than to support formal confirmatory comparisons, they should be interpreted as exploratory analyses.
For the exit interview data, the number of good and difficult listening experiences reported by each participant was extracted. The extracted data were analyzed using a mixed-effects linear regression model, with the number of experiences as the outcome variable and group and situation type (good vs. difficult) as explanatory variables.
Descriptive statistics are presented as mean ± standard deviation (SD), unless otherwise noted. Across all mixed-effects regression analyses, participant identification number was included as a random effect. Residuals were visually inspected to confirm approximate normality and homoscedasticity. In cases where homoscedasticity was violated, models were estimated using robust standard errors. All statistical analyses were performed using Stata version 15 (StataCorp, College Station, TX, USA).
Results
Baseline Characteristics
The two groups were comparable across all baseline characteristics, as well as hearing aid use time during the field trial period (see Table 1).
Affective Ratings
All participants successfully completed the Affective Rating task, with only rare instances of participants indicating they could not hear a sound. At Visit 1, six participants (two Control and four Positive Focus) reported not hearing between one and three sounds, and at Visit 2, three participants (two Control and one Positive Focus) reported not hearing one sound. The sounds which were not heard were predominantly of neutral valence. Only one sound, not heard by one participant, was of negative expected valence.
Figure 4 presents the valence ratings for both pleasant and unpleasant sounds, with detailed statistical data provided in Table 2. Participants in the Positive Focus group rated pleasant sounds significantly less pleasant compared to those in the Control group at both Visit 1 and Visit 2. There was no significant interaction between group and trial, indicating that the Positive Focus intervention did not influence emotional responses to sounds typically associated with positive emotions. Regarding unpleasant sounds, no significant differences in ratings were observed between the groups at either visit.

Valence ratings for pleasant (left panel) and unpleasant (right panel) sounds. The data show that participants in the Positive Focus group rated pleasant sounds significantly less pleasant compared to those in the Control group across both visits. ** p < .01.
Post Field Trial Questionnaire Outcomes
Figure 5 illustrates the regression coefficients for pleasantness of everyday listening situations (from the HEARLI-Q), hearing aid satisfaction (from the HEARLI-Q), and the IOI-HA total score, with detailed statistics available in Table 2. Because there were significant group differences in valence ratings for pleasant sounds, the analyses were adjusted by incorporating valence ratings of pleasant sounds from Visit 2 into the mixed-effects regression models. The Positive Focus intervention showed a significant positive effect on all three outcomes. Pleasantness of everyday listening situations (Control: 5.9 ± 1.5 and Positive Focus: 6.8 ± 1.4), hearing aid satisfaction (Control: 3.2 ± 0.6 and Positive Focus: 3.7 ± 0.8), and IOI-HA total score (Control: 27.6 ± 5.5 and Positive Focus: 29.3 ± 3.4) were all higher for the Positive Focus group than for the Control group.
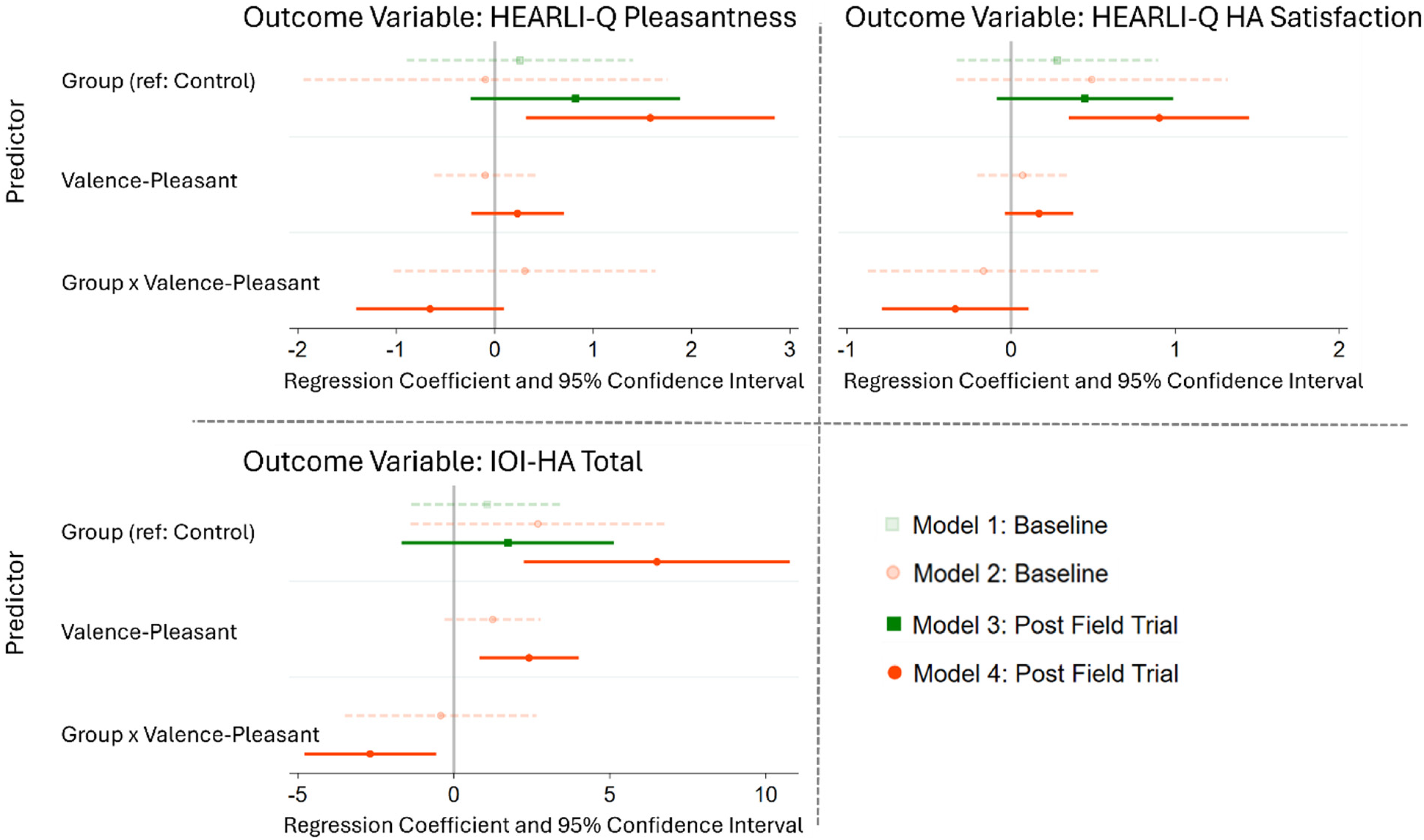
Regression coefficients for pleasantness on the HEARLI-Q scale (top left panel), hearing aid satisfaction on the HEARLI-Q scale (top right panel) and IOI-HA Total (bottom left panel) outcomes. Valence-Pleasant indicates valence to pleasant sounds. The gray vertical line indicates a regression coefficient of 0. If a confidence interval crosses this line, it indicates no significant effect. Four models are shown. Model 1: outcome at Visit 1 and group as explanatory variable; Model 2: outcome at Visit 1, and group, valence-pleasant, and group × valence-pleasant interaction as explanatory variables; Model 3: outcome at Visit 2 and group as explanatory variable; Model 4: outcome at Visit 2, and group, valence-pleasant, and group × valence-pleasant interaction. Models 3 and 4 are the ones of interest, whereas Models 1 and 2 are plotted as a reference to illustrate that the observed moderating and suppressing effects are not seen at Visit 1. Abbreviations: IOI-HA = international outcome inventory for hearing aids; HEARLI-Q = hearing-related lifestyle questionnaire; EMO-CHeQ = emotional communication in hearing questionnaire.
When valence for pleasant sounds was excluded from the models, the group effect was no longer significant for any of the outcomes (HEARLI-Q pleasantness: β = 0.13 [95% CI: −0.24, 1.88], p = .126; HEARLI-Q satisfaction: β = 0.45 [−0.09, 0.99], p = .098; IOI-HA: β = 1.73 [−0.13, 3.59], p = .068). This suggests that valence to pleasant sounds contributes to the effectiveness of the Positive Focus intervention.
The significant interaction between group and valence ratings for the IOI-HA outcome, characterized by a negative regression coefficient, indicates a moderating effect: participants who rated pleasant sounds less positively when aided experienced greater benefit from the intervention. In contrast, no interaction effects were found for pleasantness or satisfaction on the HEARLI-Q scale, implying a suppressor effect—where the Positive Focus intervention's impact was only evident when accounting for valence ratings of pleasant sounds.
Because differences in valence ratings for pleasant sounds between groups were already evident at Visit 1, we performed a reference analysis to determine whether similar group and group × valence effects were present in the baseline hearing aid assessments, prior to any exposure to the Positive Focus intervention. This analysis showed no significant differences between groups at Visit 1 (see Figure 5). Thus, the observed difference is not incidental but can be attributed to the Positive Focus intervention introduced during the field trial.
In contrast to the pleasantness of everyday listening situations, hearing aid satisfaction, and IOI-HA total scores, there was no effect of Positive Focus on the EMO-CHeQ score (Control: 2.0 ± 0.8 and Positive Focus: 1.8 ± 0.8; see Table 2 for detailed statistics).
Exit Interviews
During the exit interview, participants in the Control group reported an average of 1.6 ± 1.0 difficult listening experiences and 2.7 ± 1.6 good ones, and the Positive Focus group reported 1.1 ± 0.8 difficult listening experiences and 3.6 ± 1.5 good ones. Overall, both groups recalled more good than difficult listening experiences. However, the Positive Focus group identified a greater number of good experiences compared to the Control group, while the number of difficult experiences was similar across groups (see Table 2 for detailed statistics).
Discussion
This study investigated whether the Positive Focus intervention could enhance emotional responses to environmental sounds in hearing aid users and improve hearing aid outcomes. Contrary to our initial hypothesis, the intervention did not significantly alter valence ratings for pleasant or unpleasant sounds. However, valence ratings of typically pleasant sounds while aided influenced the effectiveness of the Positive Focus intervention on the perceived pleasantness of everyday listening situations, hearing aid satisfaction, and total IOI-HA scores.
Emotional Response to Sound
The absence of significant changes in valence ratings following the Positive Focus intervention suggests that emotional responses to environmental sounds may be relatively stable and resistant to short-term psychological or cognitive modulation, when measured using brief in-lab stimuli. This finding aligns with prior research indicating that hearing aid use alone does not fully restore emotional engagement with sound (Picou et al., 2021; Tawdrous et al., 2022). Emotional responses to sound are influenced not just by auditory perception, but also by how listeners interpret and assign meaning or relevance to specific sound sources and events (Cuadrado et al., 2020). Standardized laboratory stimuli, while useful for experimental control, may lack the personal relevance and multisensory richness necessary to evoke authentic emotional responses.
One potential explanation for the null effect is the limited mundane realism (Beechey, 2022) of the sound stimuli employed. The Marcell database sounds, although normed and diverse, are inherently decontextualized and presented in isolation, devoid of the environmental and narrative cues that typically accompany real-world auditory experiences. This reductionist approach may attenuate emotional salience, particularly in populations where emotional engagement with sound is already compromised. Supporting this, Rosenthal et al. (2016) found that personally meaningful sounds elicited stronger emotional responses than standardized stimuli in individuals with borderline personality disorder, emphasizing the role of autobiographical relevance in auditory-affective processing.
The Positive Focus intervention, by design, encourages participants to attend to and reflect on real-world listening experiences, potentially fostering deeper emotional connections through autobiographical memory and affective appraisal (Holland & Kensinger, 2010; Smalley et al., 2023). However, this reflective process was not mirrored in the laboratory-based rating task, which may explain the lack of observed change. Incorporating more immersive, ecologically valid representations of daily listening scenarios may enhance emotional resonance and better capture the intervention's effects.
Another possibility is that experienced hearing aid users may be somewhat anchored in their existing emotional appraisal patterns, making short-term interventions less likely to shift their valence ratings. Future research could include new or recent hearing aid adopters. Individuals who are still adjusting to amplified sound may exhibit greater emotional variability and openness to changes in affective appraisal and thus may be more responsive to interventions aimed at enhancing emotional engagement. Understanding how valence range evolves from early hearing aid adoption through long-term use could provide valuable clinical insight into when psychological interventions are most effective and how emotional adaptation unfolds across the rehabilitation process.
Why Hearing Aid Outcomes Improve Without Shifts in Valence
Despite no detectable change in laboratory-measured valence, the Positive Focus intervention enhanced the pleasantness of everyday listening experiences as well as hearing aid satisfaction and IOI-HA total scores after the field trial. These findings align with prior randomized Positive Focus trials showing improvements in hearing aid satisfaction and perceived benefit in both first-time and experienced users (Lelic et al., 2023, 2024a). Such outcomes appear to depend on attentional, appraisal, and behavioral processes in context rather than on immediate, stimulus-bound affective reactions, consistent with appraisal theories (Moors, 2017). In our dataset, Positive Focus effects on HEARLI-Q and IOI-HA were attenuated when valence covariates were excluded, suggesting that affective tendencies contribute to the mechanism through which Positive Focus operates.
Conceptually, Positive Focus may broaden attentional selection toward positive acoustic cues (Fredrickson, 2001; Rowe et al., 2007) and bias memory toward successful experiences through savoring and capitalization processes (Bryant & Veroff, 2007; Gable et al., 2004). These mechanisms directly counteract the negativity bias, whereby negative events exert disproportionate influence on cognition and memory (Baumeister et al., 2001). Our exit interview pattern – where participants recalled more positive than difficult experiences, with a numerically higher count of positives in the Positive Focus group—aligns with evidence that sharing and savoring positive events enhances affect and memory accessibility (Bryant & Veroff, 2007; Hanson et al., 2021; Lambert et al., 2012). Notably, the ratio of positive to negative recalled experiences in the Positive Focus group broadly approximates a 3:1 ratio, echoing the “positivity ratio,” which suggests that it takes roughly three positive experiences to offset one negative experience and counteract negativity bias (Fredrickson, 2013).
While participants reported increased satisfaction and pleasantness in everyday listening, along with greater hearing aid benefit as measured by the IOI-HA, these improvements did not extend to self-reported emotional communication in hearing, as assessed by the EMO-CHeQ. One likely reason is that the EMO-CHeQ primarily captures perceptions of vocal emotional expression in others and the individual's own expressive abilities. These aspects are unlikely to be influenced by Positive Focus, which targets listening experiences rather than interpersonal or expressive skills. Consequently, such trait-like evaluations might remain relatively stable and less responsive to short-term, context-specific interventions unless paired with targeted interpersonal or communication skills training. Overall, the findings of the current study suggest that Positive Focus improves daily listening and hearing aid outcomes, without influencing brief, decontextualized valence ratings in laboratory settings or broader perceptions of emotional communication.
Moderating and Suppressing Role of Valence
Although no direct effects on subjective emotional ratings were identified, a suppressor effect emerged in analyses of the HEARLI-Q outcomes (pleasantness and satisfaction). The effect of Positive Focus on these evaluations became significant only once the influence of emotional reactivity to pleasant sounds was statistically controlled. This result highlights the complex interplay between emotional processing and intervention efficacy and points to the necessity of accounting for individual differences in emotional sensitivity when assessing the impact of auditory rehabilitation strategies.
Regression analyses further revealed that valence sensitivity to pleasant sounds significantly moderated the effectiveness of the Positive Focus intervention on self-reported hearing aid benefit. Participants with lower valence ratings—indicating reduced positive emotional response to sounds—demonstrated greater gains on the IOI-HA. This suggests that individuals who are less naturally inclined to perceive auditory stimuli as pleasant may gain more from an intervention designed to increase attention to positive listening experiences. From a clinical standpoint, a brief valence screening tool—evaluating emotional response to pleasant sounds—could help audiologists identify candidates most likely to benefit from Positive Focus and recognize those who may require alternative or supplementary interventions. This approach aligns with broader trends in audiology and healthcare toward individualized treatment plans based on psychological and behavioral needs (Feng & Wang, 2025; Granberg & Skagerstrand, 2022; Saskovets et al., 2025; Searchfield et al., 2017). However, establishing clinically useful valence thresholds will require further research.
Study Considerations
While this study offers valuable insights into the potential impact of Positive Focus on hearing aid outcomes, several limitations should be acknowledged. First, the relatively small sample size and exclusive inclusion of older participants may restrict the generalizability of the findings. Although the inclusion criteria specified an age range of 40–85 years, participants who enrolled tended to be toward the older end of this spectrum. This was not an intentional recruitment strategy but rather reflected the characteristics of individuals who ultimately participated. Considering that aging is associated with a positivity bias (Mather & Carstensen, 2005), Positive Focus might be less effective among older individuals. Future research should examine whether the current findings extend to younger adults with hearing loss, or whether the effect is even stronger in that population.
Second, the sound stimuli used in this study consisted of brief audio-only tokens. To enhance mundane realism and external validity, future studies should incorporate richer, personally meaningful audiovisual scenes. Such stimuli may be more sensitive to the effects of Positive Focus and better reflect real-world listening experiences.
Third, the study did not include probe microphone verification of hearing aid output. This means that individual variation in hearing aid acoustics may not have been fully captured. Incorporating probe microphone verification in future studies would ensure that the stimuli are consistently audible across participants, hence strengthening confidence in the interpretation of hearing-related outcomes.
Finally, although the moderating and suppressing roles of valence are described above, the study was not originally designed to test emotional responsivity as a determinant of Positive Focus effectiveness; these effects therefore emerged as secondary, exploratory observations. Because the questionnaire outcomes and Visit 2 valence ratings were collected at a similar time point, our analysis plan prespecified Visit 2 valence as the covariate in the primary models. To evaluate robustness, we conducted sensitivity analyses using baseline (Visit 1) valence; these analyses (Supplemental Table 3) showed that Positive Focus remained associated with higher hearing aid satisfaction (HEARLI-Q) and IOI-HA scores even when controlling for pre-intervention valence. Methodologically, these results suggest that pre-existing affective tendencies can mask or magnify observed intervention effects if not modeled appropriately. Prospectively, future studies should (a) prespecify valence as a baseline moderator, (b) test a priori whether moderation replicates, and (c) examine clinically actionable thresholds to guide valence-informed tailoring of the Positive Focus intervention.
Conclusions
The findings of this study further support the value of the Positive Focus intervention in personalized hearing care. While Positive Focus did not change laboratory-based emotional ratings of environmental sounds, it significantly enhanced self-reported hearing aid benefit and satisfaction in a group of experienced hearing aid users. The evidence suggests that Positive Focus is particularly beneficial for those individuals whose valence ratings of pleasant sounds are lower, positioning valence screening as a potentially useful clinical step to identify those who could benefit from the Positive Focus intervention.
Supplemental Material
sj-docx-1-tia-10.1177_23312165261437852 - Supplemental material for Emotional Response to Pleasant Sounds Plays a Role in the Effectiveness of the Positive Focus Intervention
Supplemental material, sj-docx-1-tia-10.1177_23312165261437852 for Emotional Response to Pleasant Sounds Plays a Role in the Effectiveness of the Positive Focus Intervention by Dina Lelic, Frederic Marmel, Mads Errboe Sørensen and Erin M. Picou in Trends in Hearing
Footnotes
Acknowledgments
We thank Frederik Nielsen for his support in setting up the laboratory for the affective rating task.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
Dina Lelic, Frederic Marmel, and Mads Errboe Sørensen are employed by WSA.
Supplemental Material
Supplemental material for this article is available online.