
Abstract
Self-fitting hearing aids (SFHAs)—devices that enable self-directed threshold measurements leading to a prescribed hearing aid (HA) setting, and fine-tuning, without the need for professional support—are now commercially available. This study examined outcomes obtained with one commercial SFHA, the Companion (SoundWorld Solutions), when support was available from a clinical assistant during self-fitting. Participants consisted of 27 experienced and 25 new HA users who completed the self-fitting process, resulting in 38 user-driven and 14 clinician-driven fittings. Following 12 weeks’ experience with the SFHAs in the field, outcomes measured included the following: coupler gain and output, HA handling and management skills, speech recognition in noise, and self-reported benefit and satisfaction. In addition, the conventionally fitted HAs of 22 of the experienced participants who had user-driven fittings were evaluated. Irrespective of HA experience, the type of fitting (user- or clinician-driven) had no significant effect on coupler gain, speech recognition scores, or self-reported benefit and satisfaction. Users selected significantly higher low-frequency gain in the SFHAs when compared with the conventionally fitted HAs. The conventionally fitted HAs were rated significantly higher for benefit and satisfaction on some subscales due to negative issues with the physical design and implementation of the SFHAs, rather than who drove the fitting process. Poorer cognitive function was associated with poorer handling and management of the SFHAs. Findings suggest that with the right design and support, SFHAs may be a viable option to improve the accessibility of hearing health care.
Keywords
Introduction
Technological advancement during the past 40 to 50 years has led to increasing user control of acoustic hearing devices. After a long period in which hearing aids (HAs) allowed users to only manipulate overall gain via an onboard volume control, the tone control was introduced, enabling HA users to further change the slope of the gain-frequency response. In the late 1980s, digitally programmable HAs—devices equipped with analogue components for sound processing but a digital control circuit—with multiple memories were introduced, making it possible for users to select between different HA settings to suit different listening situations (Johnson, Kirby, Hodgson, & Johnson, 1988; Mangold, Eriksson-Mangold, Israelsson, Leijon, & Ringdahl, 1990; Sandlin & Andersen, 1989). More recently, after HAs had transitioned to fully digital, algorithms were introduced enabling HA users to permanently change the settings in their devices by training them to learn their preferred settings (Chalupper, Junius, & Powers, 2009; Keidser & Alamudi, 2013; Mueller, Hornsby, & Weber, 2008). At the same time, HAs were offered for sale online together with sophisticated fitting software, enabling HA users to manipulate the full range of HA parameters. The latest development is an HA that enables users to set up the aid in a prescribed manner to their individual hearing loss, a process previously managed by trained clinical personnel (Convery, Keidser, Seeto, & McLelland, 2017). Such devices, referred to as self-fitting hearing aids (SFHAs; Convery, Keidser, Dillon, & Hartley, 2011; Keidser & Convery, 2016b), are equipped with an onboard tone generator that enables the user to perform an automated in situ hearing threshold test, the result of which is used as input to an onboard prescription formula that then determines the initial prescribed settings of the HA. Further self-directed fine-tuning is possible if controls that enable manipulation of the HA settings are available, either onboard or in an accompanying software application. SFHAs could improve access to technology for people in areas where audiological services are unreliable or nonexistent and be more affordable if there is no service fee attached. It may also appeal to people who would like to take complete control of the HA fitting process.
Over the same period in which the evolution of user control has taken place, technological advancement has also resulted in changes to the form factor and processing capability of acoustic devices. Examples of recent form factor advances are multimodal earbuds (or hearables), which will amplify sounds among other functions (Johansen et al., 2017; Taylor, 2015), and hearing enhancement smartphone applications (Lesner & Klingler, 2011; Paglialonga, Tognola, & Pinciroli, 2015). Examples of recent processing capability advances are wireless connectivity via Bluetooth that enables direct streaming of audio from sound production systems to the hearing device (Hernandez & Martin, 2007; Smith & Davis, 2014) and binaural signal processing strategies aimed at further enhancing speech recognition in noise (Best, Mejia, Freeston, van Hoesel, & Dillon, 2015; Kamkar-Parsi, Fischer, & Aubreville, 2014; Picou, Aspell, & Ricketts, 2014). While such advances in form factor and processing capability have provided clinicians and consumers with more choices to meet the needs and preferences of people with hearing impairment, the advancement of user control to the level of self-fitting seems to have the greatest potential yet to disrupt the traditional clinical pathway.
Before SFHAs were commercially available, studies were undertaken to examine the feasibility of self-fitting devices. Using either conventional HA components or offline, computer-based simulations, it was demonstrated that critical components of the self-fitting process (e.g., individually customizing the physical fit of the device and obtaining reliable and valid hearing thresholds with a self-directed in situ audiometry procedure) could be successfully performed by a wide range of adults with hearing loss (Convery et al., 2013; Convery, Keidser, Hartley, et al., 2011; Convery, Keidser, Seeto, Yeend, & Freeston, 2015), provided instructions were designed in accordance with best practice health literacy principles (Caposecco, Hickson, Meyer, & Khan, 2011). While these studies support the feasibility of the concept of self-fitting, the ultimate evidence for the viability of self-fitting devices would, as pointed out by Keidser and Convery (2016b), be that the actual product can be appropriately managed by consumers and produce outcomes that are not inferior to those achieved with conventionally fitted devices. These aspects were recently investigated using one commercially available SFHA, a preproduction version of the SoundWorld Solutions (SWS) Companion. This aid provides the same processing strategies as the SWS CS50+ that has been reported to meet four electroacoustic tolerance criteria set for HAs (Reed, Betz, Lin, & Mamo, 2017). Results showed that 55% of a group of 40 adults could successfully self-fit this HA (Convery et al., 2017). During the study, participants could obtain assistance from a family member or friend. However, as the partners knew as little about the self-fitting process as the participants, their contribution to the outcome was negligible, and the study concluded that a greater self-fitting success rate was probable if the participants could instead access support from specially trained personnel, similar to the support provided by SWS and other online dispensers. For various reasons, only five participants provided outcomes data for the self-fitted HA that could be compared with outcomes obtained with their own conventionally fitted HAs. In this small population, there was no significant effect of HA type on speech recognition in noise or self-reported benefit and satisfaction (Keidser & Convery, 2016a). Significantly higher gain settings at the lowest frequencies of 250 and 500 Hz in the self-fitted HAs did result in a significantly higher rating of loudness with this aid. While these results could suggest that SFHAs are not inferior to conventionally fitted HAs, they needed to be verified in a much larger sample.
More recently, a study was completed in which a commercial version of the SWS Companion was evaluated in a group of 60 adults, comprising both new and experienced HA users. In that study, participants self-fitted the HAs following computer-based instructions, which included video clips on the more challenging steps of the self-fitting process, and support on demand by a clinical assistant (i.e., a person with no audiological qualifications who had been trained in managing the self-fitting procedure associated with the test device). Of the 60 participants, 41 obtained a user-driven fitting, meaning that they either independently set up the SFHAs by accurately following the instructions, or they correctly identified when they had a problem with the procedure and then obtained appropriate help from the clinical assistant. Three participants, who either gave up on the self-fitting procedure or could not find an acceptable setting, withdrew from the study. The remaining 16 participants obtained a clinician-driven fitting, meaning that they did not recognize that they made mistakes during the procedure and, consequently, were made to repeat the self-fitting procedure under guidance of the clinical assistant. More experienced than new users obtained user-driven fittings. The 57 participants who accomplished a user- or clinician-driven fitting subsequently participated in a 12-week field trial, at the end of which outcomes were obtained. For participants who owned conventionally fitted HAs, outcomes were also measured on these devices. The outcomes data are presented in this article to examine whether outcomes with the SFHAs were affected by who was responsible for setting up the device and whether such an effect interacted with past experience with amplification. In addition, we compared outcomes for SFHAs and conventionally fitted HAs among the experienced HA participants who obtained a user-driven fitting.
Method and Material
Participants
Participants included 57 adults with permanent, stable, bilateral hearing loss who had completed the setup procedure of a SFHA with access to support from a clinical assistant. Thirty of the participants were current bilateral HA users (EXP group), and 27 had no previous amplification experience (NEW group). The EXP participants, who had an average of 10.2 years of experience with HAs (SD = 8.6 years), were recruited from the National Acoustic Laboratories’ database of volunteers, while the NEW participants were mainly recruited through an advertisement in local newspapers and through family and friends of NAL colleagues. None of the recruits had prior experience with the test HA. The two groups of participants were well balanced in terms of gender distribution (67% and 63% males in the EXP and NEW group, respectively); age (M = 72.2 years with SD = 7.4 years, and M = 71.7 years with SD = 6.9 years for EXP and NEW participants, respectively); and cognitive status as measured by the Montreal Cognitive Assessment tool (Nasreddine et al., 2005; M = 26.3 points with SD = 2.7 points, and M = 26.4 points with SD = 2.6 points for EXP and NEW participants, respectively). The EXP participants did, however, have a significantly (t55 = 2.4; p = .02) higher mean four-frequency average (4FA) hearing loss, measured across 0.5, 1, 2, and 4 kHz, as compared with NEW participants (M = 46.2 dB HL with SD = 10.3 dB HL, and M = 39.7 dB HL with SD = 9.5 dB HL, respectively).
Test HA
The SFHA used in this study was the Companion by SWS. The Companion is a receiver-in-canal (RIC) HA with a retractable tube that can be adjusted to different lengths and connected to an instant-fit, closed dome of three different sizes. The HA features three programs, 16-channel compression, noise reduction, feedback cancellation, and a directional microphone. The HA is further equipped with integrated Bluetooth that enables it to be wirelessly connected to a mobile device. This feature means that the aid is powered from an integrated battery pack that makes the Companion a heavier and larger (twice the size) HA than conventional RIC HAs. The battery, which is rechargeable and cannot be replaced with ordinary cell batteries, lasts about 12 to 14 hr on a full charge. Users can download the SWS self-fitting app to self-administer a pure-tone hearing test, the results of which are used to determine an initial gain/frequency response for the HAs using a proprietary formula. The prescribed gain/frequency response forms the basis for three programs designed for different acoustic environments: Baseline Profile, Restaurant Mode, and Entertainment Mode. In each of these programs, users can fine-tune the overall gain as well as gain in low-, mid-, and high-frequency bands from the SWS self-fitting app. Onboard controls further enable program change and volume control adjustments. Setting of the maximum power output of the HAs is also proprietary and cannot be further adjusted by the user.
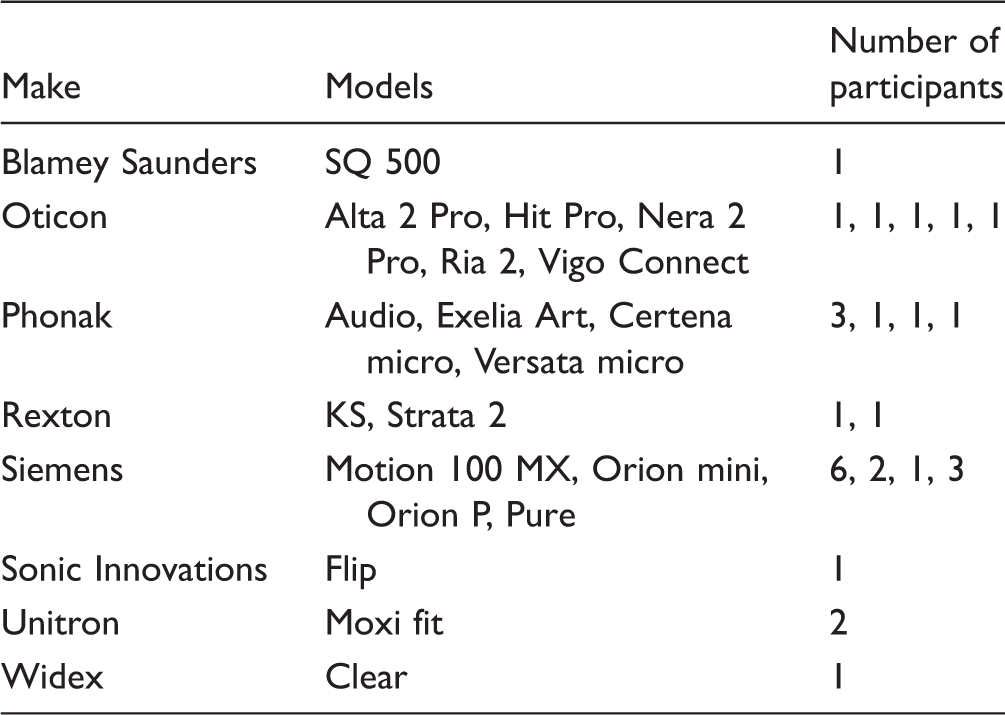
Own HA
Overview of the Make and Models (in Alphabetical Order) of Hearing Aids Worn by the 30 Participants With Hearing Aid Experience.
Outcomes
The outcomes measured in the study were 2 cc coupler measurements of gain and maximum output, HA handling and management skills, speech recognition in noise, activity limitations, participation restrictions, and self-reported HA satisfaction.
Coupler measurements
The gain/frequency responses of the HAs were measured with a standard small dome attached to an HA1 2 cc coupler with putty. Gain curves were measured for 50, 65, and 80 dB sound pressure level (SPL) inputs using the International Speech Test Signal (Holube, Fredelake, Vlaming, & Kollmeier, 2010) as the input stimulus. The OSPL90 was measured in response to a 90 dB SPL pure-tone frequency sweep.
HA handling and management skills
HA handling and management skills were evaluated using a purpose-designed test that was modeled on the Practical Hearing Aid Skills Test (Doherty & Desjardins, 2012) and the HA Management test (Caposecco et al., 2016). The evaluation was divided into observation and demonstration sections. In the observation section, the experimenter noted whether the participant was wearing the HAs upon arrival at the laboratory and whether they were correctly inserted in the participant’s ears. One point was allocated for wearing the HAs, and additional points were awarded for each correctly inserted aid. In the demonstration section, the participant was asked to remove and insert the HAs, switch the HAs on and off, change (own HAs) or recharge (SFHAs) the batteries, use the onboard volume and program controls (if applicable), and clean the HAs. During evaluation of handling skills with the SFHAs, participants were also asked to launch the SWS self-fitting app and use the app to change the volume and select a different program. For all demonstration tasks, participants were awarded two points for correct execution, one point if they demonstrated some difficulty or made a minor error, and no points if the task could not be performed. For each skills evaluation, a percentage-correct score was calculated based on the number of applicable tasks.
Speech recognition in noise
The signal-to-noise ratio at which 50% speech recognition threshold in noise (SRTn) is achieved was measured with an automated version of the Beautifully Efficient Speech Test (Best, McLelland, & Dillon, 2014) presented in a background of uncorrelated 8-talker babble noise. The noise level was fixed at 55 dB SPL, while the speech level varied adaptively throughout the test from a starting level of 65 dB SPL. Speech was presented to the participant from a loudspeaker at 0° azimuth, while the noise was presented from four loudspeakers positioned at ±45° and ±135°. The adaptive procedure continued until a minimum of 16 sentences had been presented and a test–retest standard error of 0.8 dB had been reached, or a maximum of 32 sentences had been administered (Keidser, Dillon, Mejia, & Nguyen, 2013). The Beautifully Efficient Speech Test lists were scored morphemically. Three adaptive runs were completed to obtain three independent values that were averaged to yield a single SRTn score.
Activity limitations
Activity limitations were measured with the Abbreviated Profile of Hearing Aid Benefit (APHAB) inventory (Cox & Alexander, 1995). The APHAB is a 24-item questionnaire in which participants rate the degree of difficulty they experience in everyday listening situations on a 7-point scale from always to never. Aided performance was compared with the unaided condition in the domains of ease of communication, reverberation, background noise, and aversiveness, with higher scores indicating fewer activity limitations, or greater HA benefit.
Participation restrictions
Participation restrictions were measured with the Hearing Handicap Inventory for the Elderly (HHIE; Ventry & Weinstein, 1982). The HHIE is a 25-item questionnaire in which participants are asked to indicate the extent to which their hearing impairment causes a problem in a given situation by answering yes, sometimes, or no. Aided performance was compared with the unaided condition in the domains of emotional and social handicap, with higher scores indicating fewer participation restrictions, or less hearing handicap.
Self-reported HA satisfaction
HA satisfaction was measured with the Satisfaction with Amplification in Daily Living (SADL) inventory (Cox & Alexander, 1999, 2001). The SADL is a 13-item questionnaire designed to capture information about the satisfaction that people feel with their current HAs. Excluding three items related to service and cost, which were not relevant for this study, the participants were asked to rate their opinion about each item using a 7-point scale from not at all to tremendously. Scores are calculated in the domains of positive effect, negative features, and personal image, with higher scores indicating greater satisfaction.
Procedure
Participants in the NEW group attended three appointments at our laboratory, while EXP participants attended four appointments. At the first appointment, all participants were briefed about the study and signed consent forms. Participants were then evaluated with otoscopy and tympanometry before they underwent standard audiometric testing to confirm that their hearing thresholds were within the range of threshold levels that can be measured in situ by the SFHA. A case history was further obtained for NEW participants to ensure there were no contraindications to using HAs.
At the second appointment, participants self-fit the HAs. To guide the self-fitting procedure, participants were asked to follow a set of self-paced instructions presented in Microsoft PowerPoint format. Embedded in the PowerPoint slides were six captioned video clips demonstrating key self-fitting skills: (a) pair the HAs via Bluetooth to a mobile device; (b) insert the HAs into the ear; (c) change the ear tips; (d) adjust the length of the tubing; (e) adjust the settings; and (f) clean the HAs. The videos were modeled on the C2Hear video library (Ferguson, Brandreth, Brassington, & Wharrad et al., 2015). The instructions were designed by the authors in collaboration with SWS. A telephone was available inside the test booth, which participants could use to access knowledgeable support from a trained clinical assistant. Support was provided over the phone or face-to-face at the discretion of the clinical assistant; this depended largely on the nature of the support required. At the conclusion of the self-fitting procedure, the achieved settings and maximum output were measured in a 2 cc coupler. The purpose of the coupler measurements was to ensure that the HAs were safe to wear in everyday life, rather than to confirm whether the gain/frequency response matched a particular target. No participant selected settings that were deemed unsafe or likely to cause temporary or permanent threshold shift. Participants then started a 12-week field trial.
During the field trial, participants could continue fine-tuning their settings as needed with the SWS self-fitting app on their smartphone or tablet. To assist them with the ongoing use of the SFHAs, they were provided with the manufacturer’s instruction booklet on how to use and maintain the HAs. Participants could additionally revisit the self-fitting videos, which were made available to them on a dedicated website. Personalized support from the clinical assistant was available via telephone or e-mail upon request. At the end of the field trial, participants attended a third appointment during which outcomes with the SFHAs were measured. In a separate, fourth, appointment, the EXP participants also had outcomes measured with their own HAs. For both HA types, coupler measurements were obtained for the settings that the participants were wearing upon arrival at the laboratory. To potentially control for any order effect, half of the EXP participants had the outcomes data on their own HAs collected before the SFHA trial; for the other half, data were collected 2 weeks after they had completed the trial.
The study was approved by and conducted under the oversight of the Australian Hearing Human Research Ethics Committee (AHHREC2016-4/AHHREC2016-10) and conformed in all respects to the Australian government’s National Statement on Ethical Conduct in Human Research (National Health and Medical Research Council, 2007). At the end of the study, participants were given the option of receiving a cash gratuity to offset the cost of traveling to the laboratory or purchasing the SFHAs at the wholesale price.
Results
Mean and Standard Deviation Values (in Brackets) of the Profile Data for Participants With Different Level of Experience With Amplification (EXP and NEW) and Support With Self-Fitting (User-Driven and Clinician-Driven).

Note. 4FA = four-frequency average; MoCA = Montreal Cognitive Assessment; HA = hearing aid.
Table 2 shows an overview of the profile of participants in each of four groups defined by experience with amplification (EXP or NEW) and type of fitting (user- or clinician-driven). According to factorial analyses of variance, the 4FA differed significantly between EXP and NEW participants, F(1, 48) = 7.1; p = .01, with EXP participants being more likely to have a higher degree of hearing loss. Age and cognitive function differed significantly between those who had user-driven and clinician-driven fittings, F(1, 48) = 4.7; p = .04; F(1, 48) = 7.6; p = .008, respectively. Participants who obtained a user-driven fitting were more likely to be younger and to have better cognitive function. There were no significant interactions between experience with amplification and type of fitting, F(1, 48) < 0.3; p > .61. Across all participants, older age was significantly associated with poorer cognitive function, r = − 0.32; p = .02, while there was no significant association between age and 4FA, r = .03; p = .84.
Effect of Type of Fitting
Average Outcomes Measure and Standard Error (in Brackets) Obtained for Each Subgroup.

Note. SFHA = Self-fitting hearing aid; SRTn = speech recognition threshold in noise; HA = hearing aid; HHIE = Hearing Handicap Inventory for the Elderly; APHAB = Abbreviated Profile of Hearing Aid Benefit; SADL = Satisfaction with Amplification in Daily Living.
Figure 1 shows the average frequency-specific 2 cc coupler gain levels measured for a 65 dB SPL input across those with user- and clinician-driven fittings among EXP (Figure 1(a)) and NEW (Figure 1(b)) participants. Adding frequency as a repeated measure, the GLM showed a significant effect of 4FA, F(1, 46) =20.5; p < .001, and a significant interaction between frequency and 4FA, F(5, 230) = 6.2; p < .001. Higher 4FA was associated with higher coupler gain, especially at frequencies below 4 kHz. No other main factors or interactions were significant (p > .09), meaning that when controlling for degree of hearing loss and cognitive status, type of fitting did not significantly affect the final gain settings.
Average 2cc coupler gain for a 65-dB input of user-driven (full circles) and clinician-driven (open squares) fittings for (a) experienced and (b) new hearing-aid users. The bars show ± one standard error.
Among both EXP and NEW participants, those with clinician-driven fittings required slightly higher signal-to-noise ratios on average to obtain 50% correct speech recognition in noise when compared with those with user-driven fittings (Table 3). Statistically, the effects of 4FA and cognitive function were significant, F(1, 46) = 48.1; p < .001, and F(1, 46) = 4.6; p = .04, respectively, with higher 4FA and poorer cognitive function associated with poorer speech recognition performance. Controlling for these factors, the effect of type of fitting was nonsignificant, F(1, 46) = 3.3; p = .08, as was the interaction between HA experience and type of fitting, F(1, 46) = 0.4; p = .55. This finding seems reasonable because selected gain varied as expected with 4FA and was not affected by type of fitting.
Participants with user-driven fittings obtained higher percentage-correct scores on the evaluation of handling and management skills than did participants with clinician-driven fittings (Table 3). These data revealed a significant effect of cognitive function, F(1, 46) =11.0; p = .002, and type of fitting, F(1, 46) = 4.1; p < .048; participants with poorer cognitive function and clinician-driven fittings displayed greater difficulty managing the SFHA. The interaction between type of fitting and experience was nonsignificant, F(1, 46) = 1.5; p = .23. This finding reflects the difficulty the clinician-driven group had setting up the SFHA in a self-directed manner (see Table 2) and suggests that these difficulties extended to the daily handling and management of the aids.
The HHIE, APHAB, and SADL data showed no clear patterns across participants who had user- vs. clinician-driven fittings (Table 3). Adding subscales as repeated measures, the GLMs revealed no significant effect of 4FA or cognitive function on this data, F(1, 46) < 1.2, p > .28 for HHIE; F(1, 46) < 0.2, p > .65 for APHAB; and F(1, 46) < 0.7, p > .42 for SADL. The lack of a pattern between participants who obtained user-driven and clinician-driven fittings was confirmed by the absence of a significant effect of type of fitting, F(1, 46) = 0.03, p = .87; F(1, 46) = 0.03, p = .87; F(1, 46) = 1.3, p = .26 for HHIE, APHAB, and SADL, respectively. The interaction between type of fitting and HA experience did not reach significance in any of the models, F(1, 46) < 3.12; p > .08. There was a significant interaction between subscales of the SADL, HA experience, and type of fitting, F(2, 92) = 4.9; p = .009, but Tukey honest significant difference (HSD) post hoc analyses revealed significant differences between groups only between subscales, not within subscales. Overall, whether fittings were user- or clinician-driven, it did not affect perceived benefit and satisfaction with the SFHAs.
Effect of HA Provision
For the 22 EXP participants who had user-driven fittings and who also provided outcomes data for their own conventionally fitted HA, the effect of HA provision, that is, whether the fitting was self-directed or conventional, was examined. Ten of the participants had outcomes data measured with their own devices before the SFHA trial; 12 participants had outcomes data measured after the SFHA trial. Between these two groups, there was no significant difference in age (t20 = 0.1, p = .93); 4FA HL (t20 = − 0.8, p = .46); or cognitive function (t20 = − 0.6, p = .58), nor did test order have a significant effect on any of the outcomes data (p > .39). Consequently, the average outcomes data obtained with the conventionally fitted HA are shown across groups in the first column of Table 3. These data are directly comparable with those obtained with the SFHA shown in the second column. In this cohort, the outcomes data were analyzed with GLMs using provision (conventional vs. self-directed) as repeated measure.
In Figure 2, the average frequency-specific 2 cc coupler gain levels measured for a 65 dB SPL input are compared for the two HAs. The GLM when further including frequency as the repeated measure revealed a significant effect of provision, F(1, 21) = 12.7; p = .002, and a significant interaction between provision and frequency, F(5, 105) = 11.0; p < .001. According to Tukey HSD post hoc analysis, significantly higher gain resulted from the self-directed than the conventional fitting process at all frequencies up to and including 2 kHz (p < .02). Differences in gain may be attributed to various factors that are each discussed in the discussion section. Despite this difference in gain settings, analyses of the speech recognition data showed no significant effect of provision, F(1, 21) = 2.6; p = .12. Further, the difference in SRTn values produced with the two HAs was not associated with the root-mean-square difference in gain settings between HAs (r = .004, p = .99); 4FA (r = − .28, p = .20); or cognitive function (r = .12, p = .59).
Average 2cc coupler gain for a 65-dB input of self-fitted (full circle) and conventionally fitted (open square) hearing aids for 22 experienced participants with user-driven fittings. The bars show ± one standard deviation.
There was a significant effect of provision on HA handling and management skills, F(1, 21) = 23.3; p < .001. On average, participants demonstrated poorer HA handling and management skills for the SFHAs than for their conventionally fitted HAs, for which the average score of 98% was near ceiling. Greater variability in handling and management skills was also observed for the SFHAs, with scores ranging from 44% to 100%. The difference in HA handling scores for the SFHAs was explained by differences in participants’ cognitive function (r = .68, p = .001); those with poorer cognitive function demonstrated poorer handling and management skills.
On the HHIE, there was a tendency for participants to report fewer participation restrictions in the social domain with the SFHAs than with their conventionally fitted HAs (Table 3). However, when including the HHIE subscales as repeated measures in the GLM, there was no significant effect of provision, F(1, 21) = 1.2; p = .28, or a significant interaction between provision and HHIE subscales, F(1, 21) = 2.5; p = .13, on the benefit scores.
On the APHAB, there was a tendency for the participants to report fewer activity limitations when communicating in background noise with the SFHAs than with their conventionally fitted HAs, while their conventionally fitted HAs provided more relief from aversive sounds (Table 3). Statistically, when including the APHAB subscales as repeated measures, there was no significant main effect of provision, F(1, 21) = 0.1; p = .76, but there was a significant interaction between provision and APHAB subscales, F(3, 63) = 6.0; p = .001. According to a Tukey HSD post hoc analysis, only the difference in benefit scores obtained for the aversive subscale was significant (p = .03). It is worth noting that the self-fitting procedure does not include a step for setting and fine-tuning the maximum output of the HA. Of further note is that differences in reported benefit between the SFHAs and conventionally fitted HAs when communicating in noise were significantly correlated with cognitive function (r = .60, p = .003). Participants with better cognitive function were more likely to report greater benefit from the SFHAs.
According to the SADL scores, participants reported greater satisfaction with their conventionally fitted HAs than with the SFHAs (Table 3). Specifically, participants were more satisfied with their conventionally fitted HAs when it came to communicative confidence and naturalness of sound, and they also found their conventionally fitted HAs more physically appealing and less noticeable to others compared with the SFHAs. Statistically, when including the SADL subscales as repeated measures, provision had a significant effect on HA satisfaction, F(1, 21) = 13.3; p = .002, as did the interaction between provision and SADL subscales, F(2, 42) =13.9; p < .001. Tukey HSD post hoc analysis revealed significantly higher satisfaction scores for participants’ conventionally fitted HAs on the positive effect and personal image subscales (p < .008).
Discussion
In this study, outcomes obtained with a commercially available SFHA were compared between a group of adults with hearing impairment who managed to self-direct the fitting of the aid (i.e., they either managed the process by themselves or correctly identified when assistance was needed and obtained it) and a group who failed the self-directed process and received full intervention from a clinical assistant. In addition, the effect of provision (i.e., self-directed vs. conventional fittings) was investigated in 22 of the participants with self-directed fittings by comparing outcomes with the SFHAs with their own conventionally fitted HAs.
Keeping the HAs constant and controlling for degree of hearing loss and cognitive function, there were no significant differences observed in coupler gain, speech perception, or self-reported HA benefit and satisfaction between those who achieved user-driven fittings and those who had clinician-driven fittings. This would suggest that the technical performance of the SFHAs was a stronger determinant of outcomes than who drove the fitting process.
While coupler measurements of gain for a 65 dB input demonstrated no significant effect of type of fitting within the SFHA, suggesting that a self-directed fitting was as accurate as a clinician-driven fitting, significantly higher gain levels were measured across the low frequencies in the SFHAs than for the conventionally fitted HAs. A number of factors may have contributed to this observation, such as the calibration of the automated in situ threshold test, the applied prescription formula, low-frequency leakage during threshold measurements, ambient noise, or any fine-tuning performed by participants. As the calibration of the audiometric test and prescription formula are proprietary, we are unable to comment more specifically on their implementation. However, we do know that relative to thresholds obtained manually with a calibrated audiometer, the thresholds measured by the automated procedure in the SFHAs were, on average, 10.2 dB higher at 500 Hz and 4.4 dB lower at 2000 Hz. Both of these differences were statistically significant (t81 = − 6.5, p < .001 and t64 = 2.9, p = .005, respectively). The elevated threshold at 500 Hz could be explained by low-frequency leakage during threshold measurements that is not adequately accounted for in the calibration of the audiometric test in the SFHAs (O’Brien, Keidser, Yeend, Hartley, & Dillon, 2010). Excessive leakage could also occur in cases in which the selected dome was too loose or had been inserted too shallowly in the ear canal. This hypothesis is partly supported by examining differences between manually and automatically measured thresholds at adjacent frequencies. At 250 Hz, the thresholds (N = 8 ears) measured by the SFHAs were, on average, 17.9 dB higher than those measured with a manual audiometer; at 1000 Hz, the automatic thresholds (N = 83 ears) were 3.2 dB higher than the manual thresholds. Ambient noise is unlikely to have had a significant influence as its effects are accounted for in the test HAs (Shawn Stahmer, personal communication, January 13, 2016) and the fitting process was performed in a quiet room. It also seems unlikely that the participants would have significantly increased low-frequency gain of their own volition, as several studies have demonstrated that individuals fine-tuning to their own listening preferences typically make few changes to the baseline response shape (Dreschler, Keidser, Convery, & Dillon, 2008; Keidser, Dillon, & Convery, 2008). Consequently, the differences in coupler gain between the self-fitting and conventional HAs can likely be traced to the prescriptive fitting formula that is implemented in the SWS HAs combined with some uncontrolled low-frequency leakage. Despite the difference in gain settings between self-fitted and conventionally fitted HAs, there was no significant difference in SRTn obtained with the two HAs. An earlier study in which five participants provided similar outcomes data on conventionally fitted HAs and a prototype of the test HA suggested that a greater difference in measured SRTn between HAs was associated with a greater difference in 2 cc coupler gain (Keidser & Convery, 2016a); however, such an association was not observed in this larger test sample. Consequently, the findings in this study would suggest that the calibration and prescription formulas implemented in this particular SFHA generally lead to an acceptable HA setting.
Participants in the EXP group with self-directed fittings reported significantly greater satisfaction with their conventionally fitted HAs relative to the SFHAs. The greatest difference in satisfaction was observed on the Personal Image subscale of the SADL, which probes satisfaction with the appearance of the HA. A likely contributor to this finding is the form factor of the SFHA used in the study. Because of the large battery pack required to allow a direct Bluetooth connection between the HA and a mobile device, the SFHAs are larger than conventional HAs. As a result, the SWS SFHAs are heavier and more visible to others than conventional HAs, which can be particularly challenging for those users with small ears. Significant satisfaction differences were also observed on the Positive Effect subscale of the SADL, which probes naturalness of sound. This could suggest that the closed domes of the SFHAs were too occlusive for some participants. The Positive Effect subscale further probes into the values of wearing and using the HAs, and in this context, many participants commented that the 12 to 14 hr of battery life offered by the rechargeable SFHAs were insufficient to last them throughout a full day, and some participants reported ongoing difficulties connecting to and using the app. Similarly, the narrow range of closed domes that accompanies the test HA meant that not all participants could obtain a comfortable seal, with some participants reporting sore ear canals from even the smallest dome. All these factors likely contributed to participants favoring the conventionally fitted HAs.
The same participants also reported that their conventionally fitted HAs performed significantly better than the SFHAs in the presence of aversive sounds on the Aversiveness subscale of the APHAB. This may be due to the fact that the maximum power output level of the SFHAs is set according to a proprietary prescription and cannot be fine-tuned by the user. On average, the OSPL90 measured across frequencies was 7 dB higher in the SFHAs than in the participants’ conventionally fitted HAs. Combined with the higher gain levels across the low frequencies, this discrepancy could explain the significant difference in the aversiveness rating, which favored the conventional HAs. Although not significant, greater benefit scores were assigned to the SFHAs for listening in background noise (see Table 3), and many participants, especially those with better cognitive function, reported that the directionality of the SFHAs was better than that of their conventionally fitted HAs. Taken as a whole, the factors and experiences that influenced self-reported benefit and satisfaction with the SFHAs can likely be traced to the physical design and implementation of the particular SFHA used in the study, rather than the fact that the study HA had been self-fitted. Thus, the findings suggest that there is scope for improvements around the design of the SFHA. This is further supported by the type of inquiries that were received by the clinical assistant during the field trial. According to a brief log the assistant kept, nearly half (16 of 38) related to the mobile device and affected Bluetooth connection and app navigation, and another seven related to understanding the behaviors of the particular HAs, such as why “the HAs flash green when first turned on” and “the HAs say ‘connection on’ and ‘connection off ’.” The remaining inquiries (15) concerned general audiological issues like feedback, dome discomfort, tube setting stability, HA functionality, battery life, and rehabilitation expectations.
The only area consistently affected by who drove and managed the fitting was handling of the HAs. Those who obtained user-driven fittings showed significantly better handling skills of the SFHAs than those who had clinician-driven fittings, but they had significantly poorer handling skill of the SFHAs than their conventionally fitted HAs. From the inquiries received by the clinical assistant during the field trial, it is clear that the technology involved in managing the SFHAs continued to be troublesome to participants, and data showed a significant association between poor skills and poorer cognitive function. In particular, difficulties in using the app, which was necessary to make permanent adjustments to the SFHA, contributed greatly to the lower HA handling score measured for this aid. An integral and important part of the professional hearing health-care service is counseling of clients in how to continue to use and maintain their new HAs. In the context of self-fitting, the HA users have to develop these skills independently after the initial setup of the device. Apart from the clinical assistant, participants also had access to an instruction booklet and online how to videos during the field trial. While the use of support resources was not formally investigated in this study, it would appear from conversations with the participants at the end of the study that more could probably have benefitted from accessing these resources. There are several possible reasons why not all participants took advantage of the available resources. First, some participants did not recognize that they were using the SFHAs incorrectly until it was noted by the experimenter at the end of the study. For example, if the HAs were not fully inserted into the ear canal, but they could still be worn comfortably and securely, the participant would be unlikely to conclude that there was a problem for which she or he needed to seek help. Second, among those participants who did correctly identify that they were experiencing difficulties, several reported that they did not perceive the problem as sufficiently important to necessitate a visit to the support website or a call to the clinical assistant. Third, it is possible that among those whose problems were left unaddressed, some of the participants had low HA self-efficacy for solving those problems, or a belief that any efforts they made to solve the problem would not be helpful or sufficient. The effect of self-efficacy on support-seeking after HA fitting is a topic for future investigations and would, in the case of the SFHA used in this study, require a tool that probes the skills of connecting HAs to a smartphone via Bluetooth and self-administering a hearing test with a smartphone app among other things.
Findings from this study suggest that neither self-fitting nor inexperience with amplification compromises outcomes with HAs. Therefore, with an optimized implementation, access to knowledgeable support during the self-fitting process, and accessible resources for managing the ongoing use of the device, SFHAs seem to be a viable option to improve the accessibility of hearing health care. Providing SFHAs through the traditional service model would also be an option, although the prerequisites for doing so would include unbundling prices and making technical support available on demand for clients who choose to self-fit. The benefits to clients who choose to pursue the SFHA through the traditional service model would be access to a full assessment of their hearing and advice on further treatment options while obtaining an HA at a lower cost. The benefits to clinicians who choose to offer SFHAs include the possibility of attracting a more diverse array of clients and spending more time assessing new clients and meeting the needs of complex clients than setting up HAs.
Conclusions
Participants with poorer cognitive function consistently exhibited more difficulty in handling the SFHAs. On other performance outcomes, there were no significant differences found between those who successfully self-directed the fitting of the SFHAs and those who needed a clinician-driven fitting, nor was there a significant interaction with HA experience. Significantly higher ratings for aversiveness, positive effects, and personal image in favor of conventionally fitted HAs were due to design issues rather than who had set up the HA. Consequently, with an optimized implementation, instructions, and a support infrastructure, SFHAs appear viable and could be provided as a more affordable option, either within the traditional hearing health-care model in which other audiological services would be available to the consumer, or as part of any direct-to-consumer delivery model.
Footnotes
Acknowledgments
The interpretation of data presented in this article are solely those of the authors and are not necessarily shared by the funding sources. The authors would like to thank SoundWorld Solutions (SWS) for supplying the test hearing aids, and Mr. Shawn Stahmer from SWS specifically for his ongoing support during data collection. The authors additionally thank Vivian Fabricatorian, Scott Brewer, and Pamela Jackson of the National Acoustic Laboratories and Jamie Macaulay of Macquarie University for acting in the role of clinical assistant during the study. Finally, the authors thank Professor Louise Hickson and Dr. Carly Meyer from the University of Queensland for fruitful discussions about aspects of the study design, and Professor Robert Cowan for the editorial review of an earlier draft of this article.
Authors’ Note
Preliminary results were presented at the International Hearing Aid Research Conference (IHCON), Lake Tahoe, CA, in August 2016; the 44th Annual American Auditory Society Scientific and Technology Meeting, Scottsdale, AZ, in March 2017; The Otometrics Seminars, Sydney and Melbourne, in March 2017; the 21st ENT World Congress, Paris, in June 2017; Cutting-Edge Perspectives in Service Delivery for Older Adults, American Speech-Language-Hearing Association Online Conference, October 2017; the Norwegian Audiological Society Biannual Meeting, in November 2017, and the 14th Annual British Academy of Audiology Conference, Bournemouth, UK, in November 2017.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from the HEARing CRC, established under the Cooperative Research Centres (CRC) Programme, and the Commonwealth Department of Health and Ageing. The CRC Programme supports industry-led, end-user-driven research collaborations to address the major challenges facing Australia.