
Abstract
Hearing aids (HA) are a fundamental component in restoring auditory function; however, they cannot completely alleviate all problems encountered by adults with hearing impairment. The aim of this study is twofold. Firstly, we assess the health-related quality of life and coping strategies of experienced HA users. Secondly, we assess whether HA users can benefit from auditory training. To this end, 40 participants who had worn HAs for more than 6 months participated in this study. Half of the participants received auditory training, while the other half served as a passive control. The training consisted of a personalized training scheme, with outcome measures including speech in noise perception in free-field and via direct streaming to the HA, phoneme identification, cognitive control, and health-related quality of life. Results showed that experienced HA users reported a relatively good quality of life. Health-related quality of life was correlated with aided speech perception in noise, but not with aided pure tone audiometry. Coping strategies were adaptive, leading to improved communication. Participants showed improvements in trained tasks, consonant identification, and speech in noise perception. While both groups yielded improved speech in noise perception at the end, post hoc analysis following a three-way interaction showed a significantly larger pre–post difference for the trained group in the streaming condition. Although training showed some improvements, the study suggests that the training paradigm was not sufficiently challenging for HA users. To optimize daily life listening, we recommend that future training should incorporate more exercises in noise and focus on cognitive control.
Introduction
More than 25% of adults older than 60 years are affected by disabling hearing impairment (World Health Organisation, 2021). Hearing impairment is associated with increased cognitive decline (Davis et al., 2016; Lin et al., 2013; Lin & Albert, 2014; Taljaard et al., 2016), activity limitations (Solheim et al., 2011), and increased social isolation (Shukla et al., 2020).
One cornerstone of audiological rehabilitation is sensory management, such as the provision of hearing aids (HA). HAs improve the ability to hear sounds and, in turn, can improve health-related quality of life in adults with mild to moderate hearing impairment (HI) (Chisolm et al., 2007). Health-related quality of life (HRQoL) refers to the perceived burden on the physical, emotional, and social dimensions of a chronic disease. Previous research has focused on the improvement of HRQoL immediately after HA adoption, showing that the use of HAs reduces overall loneliness (Weinstein et al., 2016), improves psychosocial well-being (Tsimpida et al., 2022), and social participation (Mulrow et al., 1990; Yamada et al., 2017). In general, the use of an HA decreases the negative effects of HI (Niemensivu et al., 2015; Stark & Hickson, 2004). Nevertheless, even after HA adoption, HA users still report problems with speech understanding in noise (Humes et al., 2012; Pang et al., 2019; Tremblay et al., 2015) and communication in general (Dalton et al., 2003; Heine & Browning, 2002), indicating that HRQoL is not optimal. These problems persist even after long-term HA use (> 6 months) when HA users are used to their devices. Very few reports exist on the quality of life for long-term HA users.
Given that life with hearing impairment presents various difficulties, coping mechanisms are required to manage stress, and mental and emotional well-being. HA users can use different coping strategies to improve their communication in challenging listening situations. Coping refers to the way the individual reacts behaviorally, cognitively, and emotionally to changes in his/her environment, such as age-related HI. In a meta-synthesis of the qualitative research on coping, Barker et al. (2017) note that people with hearing impairment use several different strategies. These strategies can be adaptive and/or maladaptive. Adaptive strategies relate to accepting and attempting to adjust to situations: willingness to continue in activities regardless of limitations, denying the stigma attached to hearing impairment, and the use of effective communication strategies. Maladaptive strategies include withdrawal from social activities, blaming the lack of hearing on external factors, and denying the hearing impairment. HA users could use multiple strategies during difficult listening situations: they could actively tackle the problem (e.g., inform people about their HA) or ask their communication partner for help. They could also make use of maladaptive strategies like avoiding certain situations. To our knowledge, no prior study has explored coping strategies used by long-term HA users.
Coping, and in turn quality of life, can be partly enhanced through learning and acquiring new skills, such as those offered by auditory training programs. The goal of auditory training is to improve perceptual distinctions and speech perception in noise (SPIN) and even more, the quality of life of adults with a hearing impairment. AT has been shown to improve performance in individuals who use HAs (Dubno, 2013; Humes et al., 2019; Saunders et al., 2016), mainly on trained tasks (on-task learning). Next to improvements on trained tasks, AT also aims for improvements on novel, nontrained tasks (transfer). Some studies have demonstrated the transfer of training to untrained measures of speech perception and cognition (Anderson et al., 2013a, 2013b; Ferguson & Henshaw, 2015; Kucuk Ceyhan et al., 2022; Morais et al., 2015; Saunders et al., 2016). A few studies have shown self-reported improvements following auditory training (De Miranda et al., 2008; Ferguson et al., 2014; Henshaw et al., 2022; Sanchez et al., 2020; Stecker et al., 2006). A review by Lawrence et al. (2018) shows that auditory and/or cognitive training may improve cognition. Given that cognition plays a role in SPIN (Dryden et al., 2017), training SPIN could improve general cognitive control functions like inhibition (ignoring distractions), switching (flexibly changing tasks), and working memory updating (maintaining and updating information) Miyake et al., 2000).
Home-based auditory training has been shown to provide several benefits. One advantage is its cost-effectiveness in delivering aural rehabilitation services. Additionally, the ability to schedule training sessions at the individual's convenience can increase treatment adherence and improve outcomes. Moreover, the Covid-19 pandemic has highlighted the need for remote treatment options, making home-based AT a viable solution for individuals seeking (extra) rehabilitation (Swanepoel & Hall, 2020).
Magits et al. (2022) developed a home-based training paradigm for Dutch-speaking cochlear implant users. Training tasks include analytical and synthetic training exercises. Tasks are first presented in silence, and based on the participant's progress, exercises in noise are presented. By doing so, the optimal cognitive load during training is achieved (Sweetow & Palmer, 2005). The efficacy of the paradigm in cochlear implant users was evaluated in a randomized controlled trial (Magits et al., 2022). Results showed that half of the cochlear implant users showed better speech in noise perception and better quality of life following training. Adherence and usability were sufficient for all cochlear implant users. The question arises whether the same training paradigm yields benefits for adults with HAs.
The aim of this study is twofold. In the first part, we study the quality of life and coping strategies of experienced HA users. We expect that adults with poorer (aided) hearing thresholds and poorer SPIN report poorer HRQoL. The coping strategies of experienced HA users are compared with the reported strategies of normal-hearing adults. Given that the utilization of HAs indicates a proactive approach to managing hearing difficulties, we predict that HA users will employ more positive coping strategies, such as seeking social support, practicing assertiveness, and taking an active approach to addressing their hearing issues. Findings from Bennett et al. (2022) suggest that the implementation of these strategies can lead to improved communication outcomes.
In the second part of this study, we assess whether HA users can benefit any further from auditory training and whether auditory training can in turn improve self-reported HRQoL. To this end, the performance of HA users undergoing auditory training will be compared to participants that do not receive additional training. The evaluation will focus on SPIN, on-task learning, and time spent on training, with the expectation that participants will improve on the trained tasks and SPIN throughout training. Since adults report most difficulties with SPIN, the main outcome was the efficacy of the training paradigm in SPIN. The close relationship between SPIN and cognitive control raises the question of the transferability of training gains to cognitive measures. We will also discuss the usability of the training paradigm for HA users.
Materials and Methods
Participants
Recruiting for this study began in June 2020, and the final session took place in May 2021. Participants were recruited through the University hospitals of Leuven and audiological centers. Power analysis conducted with the G*Power software (Erdfelder et al., 2009) indicated that a total sample of 34 HA users was needed to detect differences in speech understanding in noise outcomes between the training groups with a medium effect size (F = 0.35) with 95% power using a repeated measures ANOVA (α = 0.05, 0.4 correlations among repeated measures). In total 42 participants were recruited of whom one moved abroad during the training phase, and one experienced difficulty handling the tablet during training and did not wish to continue. Both were excluded from further analysis (Figure 2). All participants were experienced HA users and did not receive any audiological rehabilitation elsewhere. None of them had to consult their audiologist to alter their HA fitting during the study. Participants’ ages ranged from 60 to 80 years old, and they all passed the cognitive screening. The demographics of the participants can be found in Table 1.
Demographics of Participants.
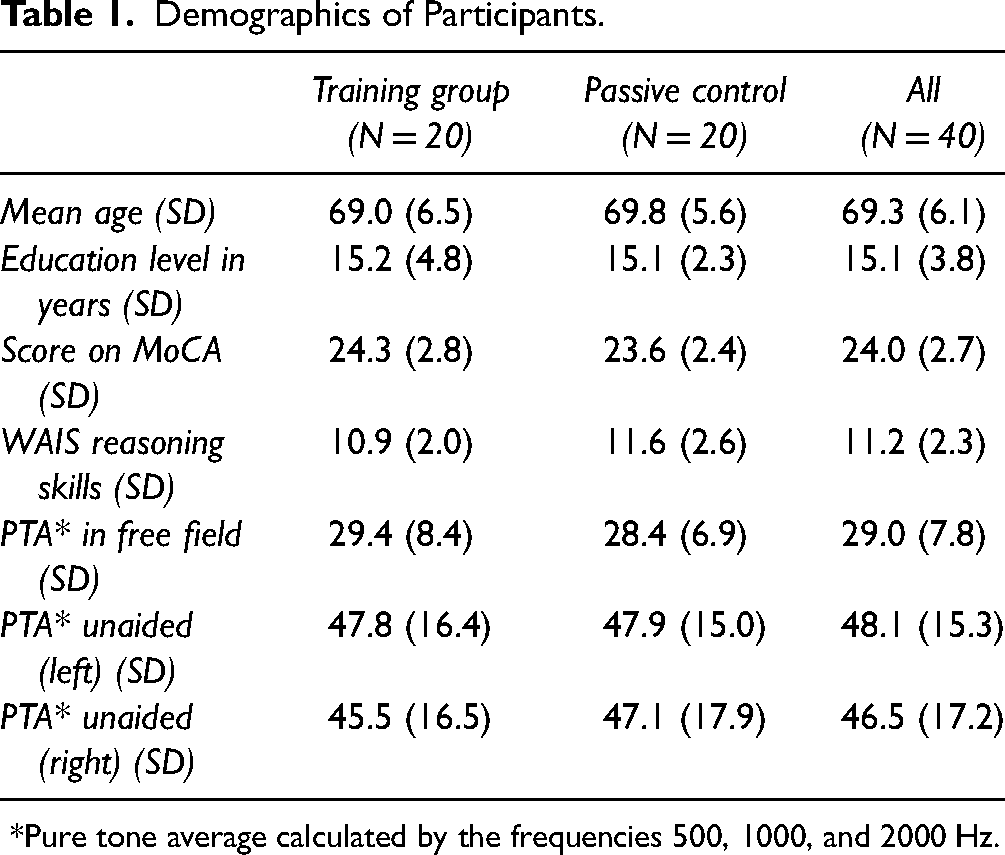
*Pure tone average calculated by the frequencies 500, 1000, and 2000 Hz.
All participants were pooled to obtain information on the HRQoL and coping strategies of experienced HA users. Afterward, participants were stratified by age and randomly assigned to the training group or the passive control. The two treatment groups did not differ significantly in chronological age (t(38) = 0.49, p = .63), education level (t(38) = 0.35, p = .75), performance on the MoCA (t(38) = 0.83, p = .41), or reasoning skills (t(38) = 0.88, p = .38). Pure tone air conduction thresholds were measured using standard clinical procedures using a Madsen Astera² (Otometrics) audiometer. Figure 1 shows the thresholds with HAs in free-field (black stars), and both left (blue crosses) and right (red circles) unaided hearing thresholds. The pure tone average (PTA) was calculated from the frequencies 500, 1000, and 2000 Hz. High PTA was defined as the average value of 1000, 2000, and 4000 Hz. Before participation participants provided written informed consent. The study was approved by the Ethics Committee of the University Hospitals Leuven (approval no. B322201731501). Participants received reimbursement for their testing sessions but were not compensated for the practice sessions at home. The study protocol is registered on ClinicalTrials.gov (ID = NCT04063748). Note that the Clinical Trials Protocol comprises two separate studies: one for CI users and another one for HA users. This approach was taken due to the simultaneous acquisition of ethical approval from the University Hospitals involving N = 90 participants. The current study did not blind the participants/test leaders, since there was only a training and a nontraining group. Also, we did not test for consolidation effects. The overall goal, namely to examine whether auditory training can improve speech in noise perception, cognitive control and/or quality of life remains the same. We added an objective to this study, to describe HRQoL and coping strategies in experienced HA users.

Hearing thresholds for each group. Error bars depict the standard deviation between participants. Black stars represent performance with hearing aids in FF. Blue crosses and red circles represent respectively left and right unaided hearing thresholds.
Procedures
The trial started with a baseline assessment. During this assessment speech understanding of noise, cognitive control, a questionnaire regarding HRQoL, and coping strategies were assessed (more details under outcome measures). After the baseline session, participants were stratified by age and divided into two groups: one active training group and one passive control group. The training group received a brief introduction about the use of the training program, the tablet, and the streaming devices (if streaming directly from the HAs was not possible). An instruction manual was also provided to work with the program on a tablet. The use of the tablet enabled data logging of the training and user characteristics (i.e., time spent on training). Due to technical issues, data could not be retrieved for one person after 6 weeks. Therefore, data from this participant was deleted from the on-task analysis.
After the baseline session, the training group trained for 12 weeks, five times a week for 15 to 20 min. Training materials were streamed from the tablet to both HAs to allow practicing at home without disturbing others. After 6 weeks, the clinician made sure that everything was going well and gave participants an overview of the participant's data logging to encourage them to continue practicing. After the second training period, participants were asked to rate the user-friendliness of the AT program using a System Usability Scale (SUS) from 0 to 100 (Brooke, 1995). The passive control group did not receive any training but returned after 12 weeks for comparison with the baseline session. After the 12 weeks, participants performed the same protocol as in the baseline to assess potential changes in speech understanding in noise, cognitive control, and HRQoL. Coping strategies were not assessed after the 12 weeks. The AT-training group was asked to give qualitative feedback on the training paradigm.
Training Stimuli and Procedures
The training paradigm consists of the LUISTER paradigm, originally developed for cochlear implant users (Magits et al., 2022). The training tasks consist of different analytical and synthetic tasks (for a detailed overview see Magits et al., 2022). Tasks included vowel/consonant discrimination, word recognition, identification of the gender of voice, emphasis recognition, clock recognition, and completion of sentences. Two additional tasks were added for HA users that include sentence recognition in noise. Each training task came with a defined set of rules that determined whether the participant needed to repeat a similar task or was referred to an easier or more difficult training task (Magits et al., 2022). Participants started training in silence, and when they performed sufficiently on these tasks, similar tasks were presented in noise, more specifically, first speech-weighted noise (SWN), then in babble noise (BN). This approach resulted in a personalized selection of tasks and difficulty levels for each participant. Participants received feedback during the practice. Training stimuli were calibrated at 65 dB SPL at the start of the training. Participants could adjust the volume during the listening training when needed.
Each week before the training tasks, participants completed the digit in noise (DiN) test twice. This task includes the identification of 17 triplets of digits in SWN. The level of the speech was fixed at 65 dB SPL and the first triplet was presented at +4 dB SNR. Triplet scoring and an adaptive step size converged to a speech reception threshold (SRT) in noise (Denys et al., 2019). The SRT was used to determine the starting level (SNR) of the training tasks in noise. Participants received feedback on the DiN. Besides the DiN, all participants also performed either a vowel or a consonant identification task in quiet (Gordon-Salant, 1985; Rødvik et al., 2018). The vowel identification task presented the Dutch vowels in a p-t context (e.g., /paat/) and included the vowels: /oe, oo, i, I, o, u, e, ee, aa, a/. While the consonant identification task presented consonants in /a/ - /a/ context (e.g., /ata/), and included the /p, t, b, d, m, n, s, f, ch, z, v, w/. Stimuli were pronounced by a female speaker (van Wieringen & Wouters, 1999). Each phoneme was presented ten times in a random order (n = 100 for vowels, n = 120 for consonants). No feedback was provided.
Outcome Measures
Testing occurred in a quiet room with their HAs. Each outcome measure was assessed pre- and posttraining, except for the Utrechtse Coping list (UCL) and the SUS. The former was only assessed before training, and the latter after training. An overview of all tests and the moment they were assessed can be found in Figure 2.

Timeline of the study design with participant flow diagram. Participants were followed up for a total of 12 weeks, preceded by the baseline session and ended with the final session. After the first 6 weeks, an intermediate appointment was scheduled for the training group.
Speech Perception in Noise
SPIN was assessed using the LIST sentences with SWN (Van Wieringen & Wouters, 2008). Stimuli were directly streamed to the HAs and presented in the sound field (S0N0). Both conditions were tested in a double-walled sound-attenuated booth. Participants were seated in front of a loudspeaker at a 1 m distance. Stimuli were played using APEX (Francart et al., 2008) from a tablet via a streaming device to both HAs or a computer via an external sound card to the loudspeaker at 65 dB SPL, measured at the location of the participant's head. Testing was performed adaptively with a one-down-one-up procedure with a step size of 2 dB SNR. Sentences were scored as correct if all keywords of the presented LIST sentence were repeated correctly. The adaptive procedure results in an SRT at which 50% of the sentences were repeated correctly. The SRT is calculated by averaging the last five SNR levels plus the SNR of the 11th imaginary sentence. In addition, the adaptive procedure's variation was calculated as the intrasubject SD of these last six SNRs. Participants completed two lists per condition, a third list was completed if the SRTs differed more than 2 dB SNR. Sentence lists with an intrasubject SD larger than 2.99 dB SNR were excluded from further analysis. In total two staircases out of 446 were excluded.
Cognitive Control
Inhibition was assessed by the Stroop Color-Word Test (Hammes, 1978). The tests consisted of three parts. In the first part, participants were asked to read aloud the written color names (in black ink). For the second part, they were asked to name the ink color of the blocks. In the last part, they were asked to name the ink in which the words are written while ignoring the written word (which is a color). This results in an incongruent pattern where participants must inhibit the implicit response of word reading. Participants were asked to perform all cards as fast and accurately as possible. Afterward, the interference score was calculated based on the difference between the time needed to complete the third task and the time needed to complete the second card. The test was presented on paper.
Task switching was assessed by the Trail Making Test (TMT, Delis et al., 2007). Which is a paper–pencil test. During the first part, participants were instructed to connect numbers from 1 to 25 in ascending order as fast and accurately as possible. For the second part, they had to alternate in ascending order between numbers and letters. Both parts were preceded by a practice to ensure participants understood the instructions. Afterward switching costs were calculated by subtracting the time needed to complete part one from the time needed to complete part two.
The Letter Memory Test (LMT, Friedman et al., 2008) assessed working memory updating. Participants must remember the last three letters on the screen. Total strings vary between 5, 7, and 9 letters consecutively. After the string presentation, participants were asked to repeat the last three digits each time a new letter was presented. Before the test, three practice strings were presented. The test includes 12 strings in pseudorandom order varying between the three string lengths. The outcome was the proportion of correctly recalled last letters of the 12 test trials. The LMT was presented on a laptop using APEX (Francart et al., 2008).
Questionnaires
The Nijmegen CI Questionnaire (Hinderink et al., 2000) was developed as a self-assessment HRQoL instrument. It was originally developed and validated to evaluate the hearing HRQoL in cochlear implant users. In this study, we extended the use of the questionnaire to HA users. We opted to use a disease-specific questionnaire to assess the additional benefit of auditory training in terms of hearing and the psychological and social domains, without questioning the satisfaction with the HA itself and the perceived handicap. The Nijmegen Cochlear Implant Questionnaire (NCIQ) includes 60 questions divided into three general domains: physical, psychological, and social functioning. Physical functioning is further divided into three subdomains: basic sound perception, advanced sound perception, and speech production. The domain of social functioning is divided into activity and social interaction. Psychosocial functioning is described as self-esteem. Participants had to indicate to what extent the statement applied to their daily life (with corresponding scores): never (1), sometimes (2), moderate (3), adequate (4), and good (5). Items with reverse phrasing were recoded by subtracting the scores from 6. For each subdomain, the sum of all item scores was divided by the number of completed items for that subdomain. The overall NCIQ scores were calculated as the mean of the six subdomain scores for each participant. Scores range from 0 to 100, where higher rates a better self-reported HRQoL.
The Utrechtse coping list (Schreurs et al., 1988) was developed to determine what coping behavior is performed when confronted with problems or adaptation-demanding events, in this case, hearing impairment. In this study, all participants wore HAs, which is a coping mechanism itself. We will focus on the coping mechanisms that adults use after HA adoption. The questionnaire distinguishes seven categories of coping mechanisms: (1) actively tackling or confronting the problem, (2) palliative reaction (ignoring the problem), (3) avoiding or awaiting a solution, (4) seek for social support, (5) a depressive reaction pattern, (6) expression of emotions or anger, and (7) having reassuring or comforting thoughts. The questionnaire consists of 47 items, and each item could be answered by four answer options indicating whether this applies to them: seldom/not (1), sometimes (2), often (3), or very often (4). Per coping category, the sum scores were calculated, where higher means that the strategy is used more often. The UCL is norm-referenced based on 1075 men and 65 women between 23 and 64 years old.
The SUS (Brooke, 1995) was performed at the end of training and aimed at rating the usability of the tablet. Systems or products that receive a score above 68 are considered to have good usability.
Statistical Analyses
Statistical analyses were performed using the R programming language and statistical environment (R Core Team, 2017). For the purpose of statistical analysis, percent correct scores were transformed into Rationalized Arcsine Unit scores (Studebaker, 1985), and TMT results were log-transformed to obtain normality. Correlations between SPIN, PTA, and HRQoL were assessed with Pearson correlations. Bonferroni corrections were added to control for multiple testing. Coping strategies of HA users were compared with those of normal-hearing adults using Welch t-tests, making it possible to control for different standard deviations between groups. Potential improvements at the start and end were assessed using linear mixed models (LMMs). Each LMM contained participant as a random factor and session (start vs. end) and treatment group (training vs. control) as fixed factors. For improvements on the DiN-test and phoneme identification tasks, we implemented a custom a priori contrast (Schad et al., 2020) where the average performance of the first two sessions was taken as a baseline for evaluation of improvements toward later performances, while also including the difference between the first and second performance. By doing so, we control for procedural learning effects. Post-hoc tests were performed by a t-test with Bonferroni corrections.
Results
The goal of this study was twofold. The first aim was to investigate the quality of life and coping strategies in experienced HA users. The second aim was to evaluate a home-based auditory training paradigm's effectiveness compared with a passive control group.
Health-Related Quality and Coping Strategies
Figure 3 shows the scores of the NCIQ in HA users. Higher scores indicate a better quality of life. To identify processes that influence self-reported HRQoL we determined correlations with aided PTA (normal and high) and aided SPIN for all subscales (Table 2). Bonferroni corrections were applied for multiple testing. The total score of the NCIQ was reliably related to aided SPIN (r = −0.45, p = .004, α = 0.007), but not to aided PTA (r = −0.21, p = .21, α = 0.007). None of the NCIQ-subscales were correlated reliably with aided PTA. The subscales advanced sound perception (r = −0.56, p < .001, α = 0.007) and speech production (r = −0.5, p = .001, α = 0.007) were significantly correlated with aided SPIN. The subscales of basic sound perception (r = −0.41, p = .01, α = 0.007) and activity limitations (r = −0.34, p = .04, α = 0.007) were not significant after Bonferroni correction.

Quality of life scores on all subdomains (left) and overall health-related quality of life.
Correlations Between Quality-of-Life Scores and Audiological Measures.

*p < .05, ** p < .01, *** p < .001.
The coping strategies of HA users are shown in Figure 4. By comparing these coping strategies to those of the normative values of 209 employees of the Dutch railways aged 55–65. Coping strategies of HA users were significantly different with regard to active approach (t(39.46) = 3.40, p = .001), comforting thoughts (t(39.11) = 4.1, p < .001), ignoring the problem (t(39.49) = 4.03, p < .001), seeking social support (t(39.20) = 2.73, p = .01), and avoidance of a situation (t(39.32) = 2.14, p = .04). The HA users in our study did not show significant differences in the coping strategy of expression of emotions or anger (t(38.97) = 1.12, p = 1.73) or a depressive reaction pattern (t(39.30) = 1.09, p = .28).

Coping strategies of HA users (black) and the reference group (red).
Evaluation of Auditory Training

Speech understanding in noise at baseline compared to the final session for the control group (left) and active training group (right). Each data point represents the median SRT of a participant, with error bars representing the IQR between lists. The area between full lines represents changes in speech understanding in noise that fall within –2 and +2 dB SNR. The dashed line represents the identity line (y = x).
To assess whether auditory training transfers to improved SPIN an LMM with the participant as a random factor, treatment group, and session (start vs. end) and condition (streaming vs. FF) as fixed factors was performed. The analysis showed a significant effect of session (β = −0.41, SE = 0.19, t = 2.18, p = .03) and a significant three-way interaction of session, treatment, and condition (β = −3.40, SE = 1.71, t = 1.99, p < .05). The main effect indicates that on average, participants improved 0.41 dB SNR after the 12-week period. Post-hoc tests following the three-way interaction with Bonferroni corrections showed that the training group in the streaming condition showed the largest improvement (t(250) = 2.39, p = .018, α = 0.0125) at the end of training. Figure 5 illustrates the performance on SPIN tests before and after auditory training for each participant seperateley, for free-field and streaming conditions. The area between full lines represents changes in speech understanding in noise that fall within -2 and +2 dB SNR, indicating a clinically relevant improvement. The dashed line represents the identity line.
Improvements on LIST in the streaming conditions were larger for those with worse baseline performance (Spearman ρ = −0.66, p = .002), which could indicate regression to the mean. Therefore, we adjusted the baseline scores by the procedure described by Rocconi and Ethington (2009). This results in a correlation of −0.40 (p = .08). No significant association was observed between time spent on training and LIST improvements (Spearman ρ = 0.03, p = .89). There was a significant correlation between performance on the LIST in the streaming condition and the FF condition (Spearman ρ = 0.60, p < .001).
Figure 6 illustrates the median scores and IQR of the cognitive control tasks for each treatment group and each testing session. Each group showed comparable results in terms of inhibition (β = −7.73, SE = 7.07, t = 1.04 p = .30), switching (β = 0.02, SE = 0.08, t = 0.27, p = .25) and updating (β = −5.69, SE = 5.74, t = 0.99, p = .32). Cognitive scores pre- versus posttraining were not significantly different (inhibition: β = −6.17, SE = 6.99, t = 0.88, p = .38, switching: β = −0.06, SE = 0.09, t = 0.64, p = .52, updating: β=3.01, SE = 5.47, t = 0.53, p = .60). Nor were improvements better for one of the two treatment groups (inhibition: β = 5.12, SE = 10.01, t = 0.51, p = .61, switching: β = −0.10, SE = 0.13, t = 0.81, p = .42, updating: β = 9.58, SE = 8.12, t = 1.18, p = .24).

Median (+IQR) scores on cognitive control tests before and after training: (A) inhibitory control, (B) task switching, and (C) working memory updating. The gray dots show the individual data of each participant.
Both treatment groups performed similarly concerning HRQoL at the start and end (β = −1.33, SE = 2.08, t = 0.64, p = .52). There were no significant improvements at the end (β = 0.35, SE = 2.11, t = 0.16, p = .87), nor was there a significant interaction effect (β = 0.32, SE = 2.96, t = 0.11, p = .91). Results are shown in Figure 7.

Median (+IQR) scores on the health-related quality of life questionnaire before and after training.
Time Spent on Training and on-Task Learning
The practice time was logged to determine adherence to the training program. Adherence is shown in Figure 8, with each bar indicating the number of hours that participants trained. Colors indicate whether they trained in silence, SWN, or BN. The black horizontal line indicates the recommended total practice time of 15 hours, showing that 80% of participants performed at least the recommended training. Participants first trained in silence (light gray bars). On average 31.5% (SD = 7.3%) of exercises were performed in silence, 45.6% (6.8%) in SWN, and 22.9% (11.8) in BN.
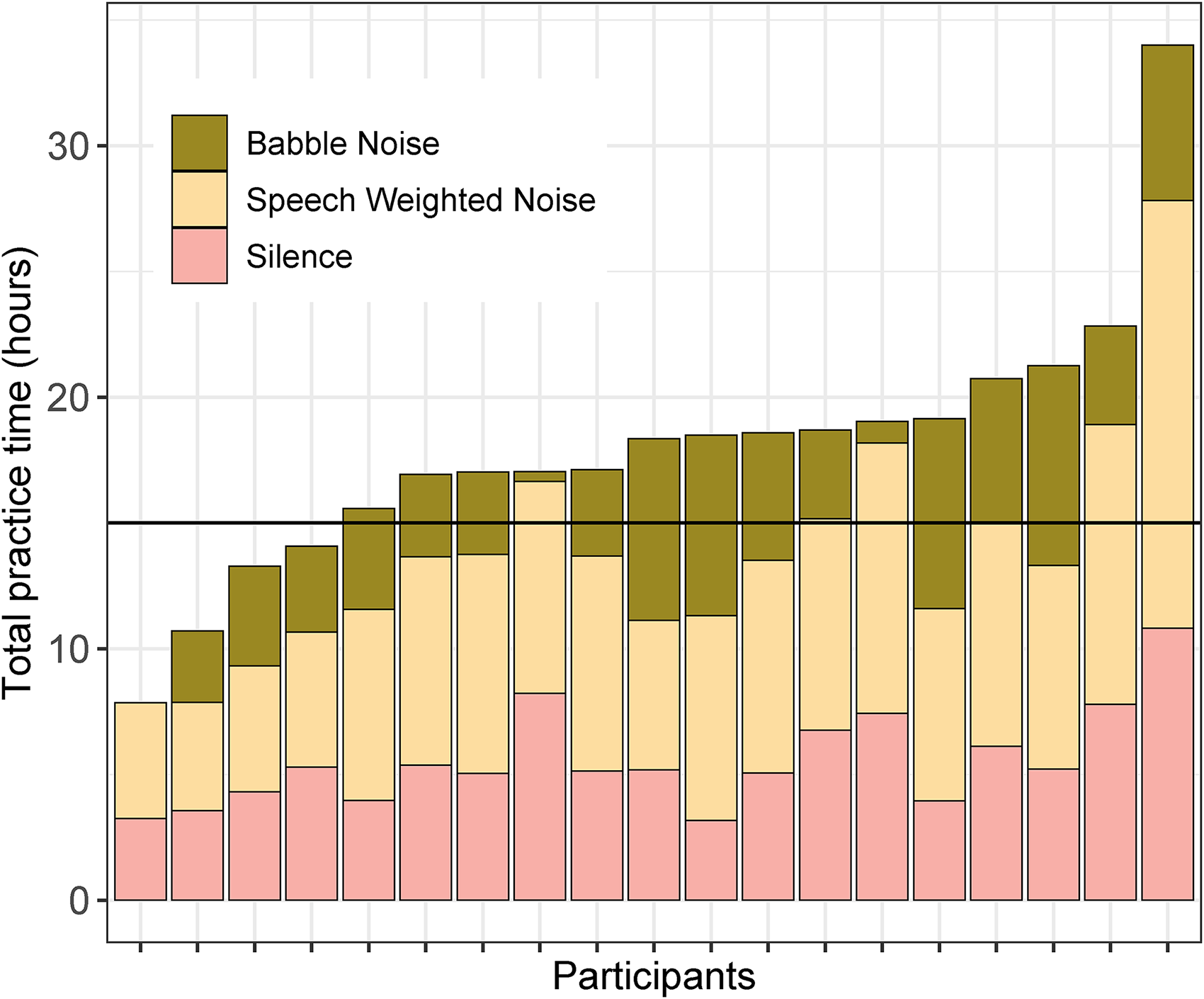
Total practice time in hours for the training group. The color indicates whether training took place in silence, speech-weighted noise, or babble noise. The horizontal line at 15 hrs indicates the recommended training time of 15 min sessions, five times a week for 12 weeks.
Regarding on-task learning (data not shown), only data from the training group were analyzed (N = 20). All participants progressed past the initial starting level (i.e., signal-to-noise ratio based on the DiN-test) by at least 6 dB SNR in SWN. All but three participants progressed past the initial starting level by 4 dB SNR in BN. Participants in the training group did not improve significantly on the DiN-test after 12 weeks (β = −2.26 dB SNR, SE = 1.16, t = 1.95, p = .052).
Improvements in Phoneme Identification
Improvements in phoneme identification were assessed using LMM with the participant as a random factor and session as a fixed factor. Custom a priori contrasts were implemented to control for procedural learning effects. Participants performed the consonant identification task six times throughout the training period (Figure 7). There is no evidence of procedural learning effects from the first to second time performing the consonant identification task (β = 5.13, SE = 3.26, t = 1.57, p = .12). Results show a significant improvement after 10 weeks of training (5th time performing the task) (β = 12.92, SE = 5.80, t = 2.23, p = .03) and 12 weeks of training (β = 21.24, SE = 5.80, t = 3.66, p < .001).
Participants performed vowel identification task 5 during the training period (Figure 9). The LMM shows improvements after the first two weeks of training (second presentation) (β = 7.99, SE = 3.55, t = 2.25, p = .03), indicating a potential procedural learning effect. Participants did not improve reliably after the third (β = 7.31, SE = 6.17, t = 1.18, p = .23), fourth (β = 11.35, SE = 6.30, t = 1.80, p = .07) and fifth (β = 10.07, SE = 6.28, t = 1.60, p = .11) presentation.

Performance in the training group over 12 weeks on the phoneme identification tasks. In red the consonant identification and in blue the vowel identification task.
Usability of the Training Paradigm
At the final test session, 50% indicated that they wished to use the program regularly (4 or 5 on the Likert scale), 30% agreed nor disagreed (3 on the Likert scale) and 20% indicated not wanting to use the program (1 or 2 on Likert scale). The mean system usability score was 84.63. Values above 68 are considered highly usable. Sixty percent of participants also indicated that training 15 min per day was considered good (not too time-consuming and not too short).
Discussion
The goals of this study were to assess HRQoL and coping strategies among individuals with long-term experience using HAs and to determine if experienced HA users can benefit from auditory training.
In comparison to the NCIQ values reported by Magits et al. (2022), adults with HAs scored better than cochlear implant users. The high scores of HA users on the “activity limitations” and “speech production” subscales indicate that our participants did not experience many limitations regarding their daily activities and speech production abilities in daily life. The latter is probably because they all gradually acquired hearing loss, meaning that their speech development was sufficient (in comparison to some CI users). The lower scores on the speech perception subscales indicate that HA users still have difficulties perceiving speech. Given the absence of correlations between aided PTA and HRQoL and the presence of an association between aided SPIN and HRQoL, our results suggest that aided SPIN is a stronger predictor than HRQoL than audibility. It is worth noting that the data demonstrate considerable variability, indicating that the participant experiences varied widely in terms of the impact of hearing-related difficulties.
Our results suggest that experienced HA users show a more active approach, make use of comfort-seeking, ignore the problem, seek social support, and might avoid some situations. It seems like HA users show no increased expressions of emotion or anger, nor a depressive reaction pattern. Our results suggest that HA users possibly use more adaptive strategies like an active approach or seeking comfort. These strategies are in line with coping strategies that have been identified to improve communication among HA users (Bennett et al., 2022; Pang et al., 2019; Sparrow et al., 2020). Coping strategies were compared to those of 209 employees of the Dutch railways aged 55–65, but it is worth noting that it is not mentioned whether any in this sample of employees had hearing loss.
The efficacy of training in HA users was evaluated by comparing an active training group to a passive control group. Eighty percent of participants performed the recommended training time, indicating good adherence to the training program. Participants spent on average 1/3 of their time training in silence, around 1/2 of their training time in SWN, and 1/5 in BN. All participants showed improvements in on-task learning (either both in SWN and BN or only in SWN).
Our results showed that all participants, irrespective of treatment group and condition (streaming or FF), improved on the second session in comparison to the first. On average, participants improved with 0.41 dB SNR at the end session. This improvement is rather small and could be due to the effects of procedural learning. However, the significant three-way interaction yields larger improvements for the training group in the streaming condition, suggesting an effect of training. Improvements in the sentences in noise were larger than 2 dB for 40% of participants when sentences were streamed to the HA. Note that some HA users scored relatively close to −7.8 dB SNR, which is the reference value in normal-hearing adults for the LIST sentences (Van Wieringen & Wouters, 2008), indicating limited room for improvement. The larger improvements for the training group in the streaming condition could be because the training was performed via streaming, resulting in a lack of generalization to the FF condition. Also, HA users with worse thresholds pretraining showed larger improvements. However, with the correction for possible regression to the mean, the correlation was not significant.
Neither the training group nor the passive control group showed improvements posttreatment in self-reported HRQoL, inhibitory control, updating skills, nor cognitive flexibility. Previous research has shown that self-reported improvements can occur following training: (Sanchez et al., 2020) showed a significant reduction in self-perceived hearing handicaps and (Ferguson et al., 2014) showed improvements in self-reports of hearing disability. Both studies measured the hearing handicap and not the hearing-related quality of life. It is worth noting that Henshaw et al. (2022) showed small improvements in self-reported hearing ability, but that these results do not transfer to self-reported hearing in daily life. Other training studies that showed transfer toward nontrained cognitive measures all included a cognitive component during training (Anderson et al., 2013; Anderson et al., 2013b; Henshaw et al., 2022; Sweetow & Sabes, 2006). Since our training includes limited exercises that include cognitive control, this could explain why there was no generalization toward cognitive control measures.
Results of the training group showed significant improvements on the vowel identification task from the first to second time performing the task, while scores for consonant identification improved toward the end of the auditory training. Improvements in the vowel identification task could be attributed to a procedural learning effect, resulting from increased familiarity with either the content or procedure of the task. It is also important to consider that the training began with more analytical tasks (in silence), such as phoneme discrimination and word identification, which may have contributed to early improvements in vowel identification. Vowel identification tasks did not improve at the end of the training, possibly due to the high scores at the start (ceiling effect). Results did improve near the end of training for the consonant identification task, showing on-task improvements for consonant identification.
Our study employed a passive control group instead of an active control. Employing active control would have provided insights into the specific benefits of the training tasks themselves. In addition, it would control for the differential participant and/or experimenter expectations between the trained group and the passive control group (Au et al., 2020; Melby-Lervåg et al., 2016). Meta-analytic reviews have shown that the use of a passive control may overestimate the true size of training effects (Melby-Lervåg et al., 2016; Sala & Gobet, 2017). However, Au et al. (2020) suggest that passive controls generally offer a more reliable and consistent means of controlling for retest effects across various studies than active controls. Ideally, a training study should include three treatment groups to be able to distinguish true training effects from placebo and test–retest effects.
Participants were hesitant but willing to perform the training paradigm regularly. Also, participants reported most difficulties with speech understanding in noise. It is likely that, especially at the start of training, exercises were too easy, and it would be better to train more SPIN. In turn, this may lead to better self-reported HRQoL.
Given the evidence, we propose incorporating more exercises in noisy environments for individuals with HAs. Complaints of HA users often comprise listening difficulties in noise. Furthermore, given the relationship between HRQoL and SPIN at baseline (and not aided PTA), improvements following auditory training could be larger when SPIN, with the inclusion of cognitive control, is trained more.
Conclusions
Adults who wear HAs for longer than 6 months report a relatively good quality of life. HRQoL was correlated with speech perception (in noise) and not with aided pure tone audiometry, suggesting that SPIN measures may be a better predictor of quality of life than the PTA. After 12 weeks, participants improved slightly on average, speech-in-noise improvements were larger for the training group in the streaming condition, but not the sound field. It is possible that the training paradigm was not sufficiently challenging for HA users. We suggest that future training should incorporate more cognitive control processes into the training paradigm, and include more exercises in noise to optimize daily life listening.
Footnotes
Acknowledgments
The authors would like to thank Sara Magits and Linus De Meyere for their technical assistance, and the ENT team of UZ Leuven, specifically Ellen Boon, and Ann Dierckx, for their help with data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Fonds Wetenschappelijk Onderzoek (Grant number T002216N) and KU Leuven (grant number C14/19/110).