
Abstract
Objectives:
Health-related quality of life of people living with epilepsy is significantly impaired. The disease causes a significant psychological and social impact on daily living conditions and usually has lifelong consequences for the patient and family. Therefore, this study aimed to investigate the health-related quality of life of people living with epilepsy and its predictors in Dessie Referral Hospital, Dessie, Ethiopia.
Methods:
A facility-based cross-sectional study was conducted from April to June 2020. Systematic random sampling was used to recruit a total of 385 study participants. Written informed consent was obtained for each participant, and data were collected using World Health Organization Quality of Life Brief Version and Hospital Anxiety and Depression Scale questionnaires. Descriptive statistics were used to summarize the data, while multivariate logistic regression analyses were used to examine factors affecting the quality of life. P value ⩽ 0.05 was considered statistically significant.
Results:
About 95.80% of the study participants had a generalized seizure, and 64.30% were on two antiepileptic drugs. Of the total, 12.20% and 37.00% suffered from depression and anxiety, respectively, based on the Hospital Anxiety and Depression Scale score. The mean total health-related quality of life score was 51.98 (standard deviation: ± 10.08; 95% confidence interval: 41.90–62.06) out of 100. Age, education level, marital status, occupation, residence, current comorbidity, family support, and recreational activities were associated with good health-related quality of life (p ⩽ 0.05)
Conclusion:
The average overall quality of life of people living with epilepsy in the Dessie Referral Hospital was low. Therefore, concerted efforts must be made to improve the quality of life of patients over the healthcare services provided.
Introduction
Epilepsy is the most common neurological disorder that affects patients’ health-related quality of life (HRQoL) and social and psychological ties. It is a global public health problem and is often associated with physical and cognitive disabilities that lead to limitations in employment, independence, and social activities.1,2 Globally, 70 million people have epilepsy, and 80% of cases occur in developing countries.3,4 About 90% of people with epilepsy in developing countries do not receive appropriate treatment. As a result, people with epilepsy have a lower HRQoL than people with other chronic diseases. 5 In Ethiopia, in a recent cross-sectional study conducted at Ambo General Hospital, the mean HRQoL score for people living with epilepsy (PLWE) was 56.43. 6
The HRQoL of PLWE may be impaired for a variety of reasons, including complications of seizures, a chronic condition, and social isolation. 7 The assessment of HRQoL should not only focus on the evaluation of seizures. However, it must also include other domains of life such as physical, environmental, cognitive, emotional, and socio-occupational functioning, perceptions of health, and overall life satisfaction.4,6,8 Epilepsy affects life in many ways and should be studied, taking into account the cultural conditions and psychosocial composition of each community. Lack of medical services, unavailability of anti-seizure medications (ASMs), lack of awareness of medical procedures, and culturally related factors are common in developing countries such as Ethiopia. 2
Unpredictable disease progression, stigma, low self-esteem, anxiety and depression, unemployment, social isolation, and cognitive problems reportedly affect HRQoL in PLWE. Physical injuries such as burns, drowning, falls, and car accidents can endanger the lives of PLWE. PLWE may isolate themselves from society and, as a result, suffer from depression, which can further decrease their HRQoL.9–11 Epilepsy has a significant impact on HRQoL in PLWE and family members. However, less is known about the impact of family support and family functioning on HRQoL for PLWE and family members and their interaction. 12
The growing population in developing countries such as Ethiopia has an impact on the healthcare system and poses a socioeconomic burden. This study area, Dessie Referral Hospital (DRH), serves as a referral hospital for most of the northeastern Amhara and Afar regions and serves more than 3.5 million people annually. It has about 749 workers. Of this, 548 are health professionals, and 201 are administrative staff serving in the hospital. In this hospital, one-third of PLWE struggled with side effects, and more than 30% of PLWE do not achieve complete seizure control even with the best available treatment regimen because they take ASMs poorly. 13
In Ethiopia, few studies have been conducted on the HRQoL of PLWE, so the disease is increasing from time to time due to unawareness.2,6,9,14,15 Hence, the purpose of this study is to determine the HRQoL and identify factors associated with HRQoL among PLWE at DRH, Amhara, Ethiopia.
Materials and methods
Study setting
The study was conducted in the adult epilepsy outpatient department (OPD) of DRH, located in Dessie, Amhara, Ethiopia. It serves as a teaching center for medical students, pharmacists, nurses, midwives, medical laboratory technicians, and radiologists. The DRH serves about 500,000 patients annually in its OPD and about 40,000 in the inpatient department and the same number in the emergency department.
Study design and period
A facility-based cross-sectional study was conducted from April to June 2020 at DRH in the epilepsy OPD using the standardized instrument World Health Organization Quality of Life Brief Version (WHOQoL-BREF) and Hospital Anxiety and Depression Scale (HADS).
Source and study population
The study population consisted of PLWE who attended the epilepsy OPD at DRH during the study period, and all PLWE who attended DRH was the source of the population.
Inclusion and exclusion criteria
All outpatients who visited the DRH epilepsy OPD with a clinically confirmed diagnosis of epilepsy and had been receiving treatment at DRH for at least 6 months and were age ⩾18 years were included in the study. Patients who had not yet started treatment, who had cognitive impairment, and individuals who were not volunteer to participate were excluded from the study.
Sample size determination and sampling technique
The sample size was determined using the single proportion formula, 16 assuming that the overall HRQoL was 56.43% 6 with a margin of error of 5% and a confidence level of 95% and adding a 10% non-response rate. Accordingly, 415 study participants were recruited. Systematic random sampling was used to recruit study participants from epilepsy OPD of DRH.
Data collection and management
Data were collected using a data collection format and the standardized tool WHOQoL-BREF. The data collection format was designed to extract information directly from the patient, such as data on sociodemographic characteristics (age, sex, marital status, education level, residence, employment status, occupation). Clinical characteristics (seizure type, seizure frequency, number of ASMs and frequency of AED use per day, current comorbidity) were collected by interviewing patients and reviewing their medical records, respectively.
The WHOQoL-BREF contains 26 items and a robust cross-cultural assessment of HRQoL, consisting of four domains: physical health (seven items), psychological health (six items), social relationships (three items), and environmental health (eight items); it also includes the first two questions on the general perceptions of life and health, and each item of the WHOQoL-BREF was assigned a score ranging from 1 (very dissatisfied/very poor) to 5 (very satisfied/very good). 17
The HADS was a 14-item questionnaire commonly used to assess anxiety and depression symptoms. The 14 items can be divided into two 7-item subscales for anxiety and depression. 18 The HADS score has been used on PLWE and has shown that it is a good screening tool. 19
Data quality assurance
The WHOQoL-BREF and HADS questionnaires were translated into Amharic and back-translated into English by a second bilingual translator to check their consistency. Subsequently, the tool was tested on 10 selected PLWEs at Boru Meda Hospital. Accordingly, all necessary changes and adjustments were made before the questionnaire was used in this study. All data were reviewed daily by the study director to ensure the quality of the data.
Outcome measurements
HRQoL scores were calculated using the tool WHOQoL-BREF. According to the instructions for use, raw scores for the ranges of WHOQoL-BREF were calculated and transformed to a scale of 0 to 100 by using the formula for mean transformation.

Where Domain x̄: domain mean transformed to 100; MAXs: maximum score; N: number of items; ∑x̄: sum of means; 100 is the highest HRQoL, and 0 is the lowest HRQoL. 17
The mean score of each domain and the total score were also calculated because HRQoL measures are often presented as mean values in studies. Therefore, categorization was based on the mean scores from WHOQoL-BREF. Subjects whose scores were greater than or equal to the mean were categorized as good HRQoL in WHOQoL-BREF, while subjects with scores below the mean were categorized as poor HRQoL. 15 In the HADS tool, participants with a total score of 0–7 were categorized as normal (non-cases, patients who have no sign of depression and anxiety), with a score of 8–10 as borderline abnormal (borderline case, patients who have borderline or have the risk of developing depression and anxiety), and with a score of 11–21 as abnormal (case, patients who had a sign or cause of depression and anxiety). 20
Statistical analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) version 21 software. Descriptive statistics such as frequency, mean, and median were used to summarize sociodemographic and clinical characteristics and to assess the distribution of responses. After testing the assumptions, a bivariate analysis was performed to obtain candidate variables for the multivariate regression models to determine possible predictors for the outcome variable (HRQoL). In the bivariate analysis, factors related to HRQoL were included with a p value of <0.2, while a p value of <0.05 was considered statistically significant.
Ethical considerations
Ethical approval (Ref. No; 321/09/2012) was obtained from the ethical review committee of Medicine and Health Sciences, Wollo University. A formal approval letter was obtained from the administration of DRH. Before data collection, the purpose and significance of the study were explained to each study participant. The participant’s name was not given at the time of data collection, all other personal information was completely obscured, and confidentiality was maintained throughout the study period.
Results
Sociodemographic characteristics of participants
The response rate for this study was 92.50%. Of the total 384 study participants, more than half were male, 215 (56.00%). The mean age of the participants was 35.50 (standard deviation (SD) ± 14.40) years, with 111 (28.90%) participants in the age group between 25 and 34 years (Table 1).
Sociodemographic characteristics of study participants, DRH, 2020.

Clinical characteristics of participants
Generalized seizures 21 occurred in the majority, 368 (95.80%) of the study participants. Regarding the frequency of seizures, 359 (93.50%) had more than one seizure episode per year, and more than half, 247 (64.30%) of the study participants were taking two ASMs. The rest of the figures are depicted in Table 2.
Clinical characteristics of study participants, DRH, Ethiopia, 2020.

ASMs: anti-seizure medications.
Personal characteristics of study participants
Of the total 384 study participants, 356 (92.70%) had perceived self-esteem. Regarding adherence to self-care, 378 (98.40%) were capable of self-care, and most study participants, 366 (95.30%), had family support (Table 3).
Personal characteristics of study participants, DRH, Ethiopia, 2020.

HADS of study participants
About half of the participants rated the depression subscale as normal, followed by borderline depression, 146 (38.00%), and 72.70% and 37.00% of patients scored normal and anxiety cases, respectively, on HADS scores (Figure 1).
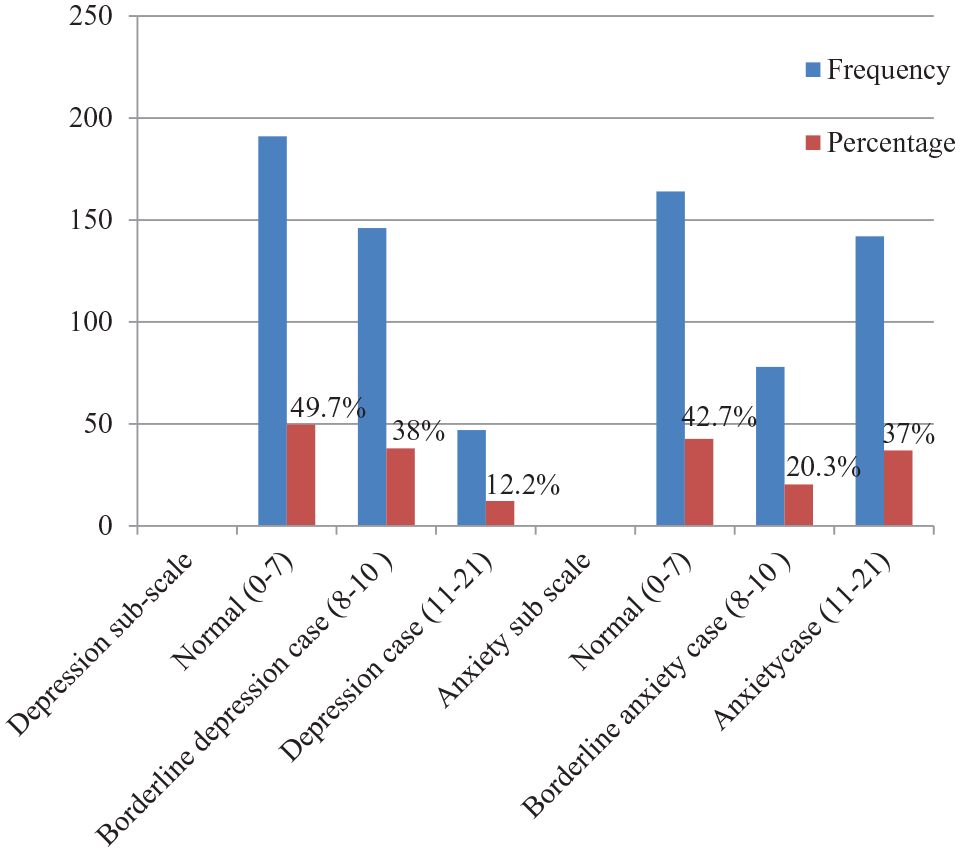
HADS of the study participant, DRH, Ethiopia, 2020.
Mean score HRQoL scale
The mean ± SD of the WHOQoL-BREF physical domain rating scales was 58.60 ± 3.30, psychological domain 50.25 ± 2.80, social domain 53.30 ± 1.50, and environmental domain 48.75 ± 3.90 with an overall HRQoL of 51.98 ± 10.08 (Table 4).
Mean scores of HRQoL scale among patients treated for Epilepsy, DRH, Ethiopia, 2020.

SD: standard deviation.
Factors associated with HRQoL
In the bivariate analysis, 16 of the 22 variables studied (p < 0.2) showed a relationship with good HRQoL, as measured by the WHOQoL-BREF scale. Then, of the 16 variables used for multivariate logistic regression analysis, eight variables (age, educational status, marital status, occupation, residence, current comorbidity, family support, and recreational activity) were identified as being associated with good HRQoL, as indicated in Table 5.
Factors associated with good HRQoL among patients treated for epilepsy at DRH, Ethiopia, 2020.
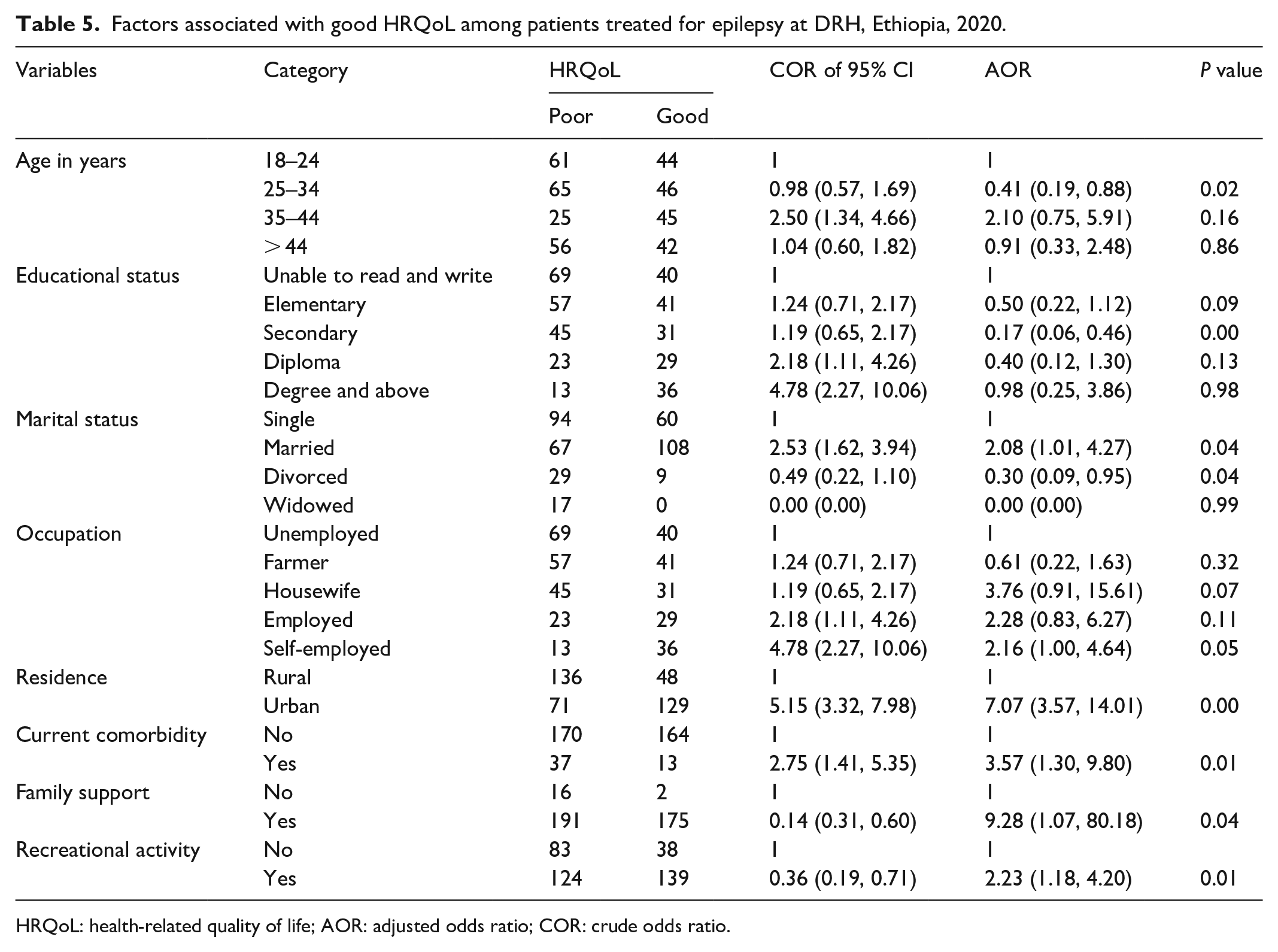
HRQoL: health-related quality of life; AOR: adjusted odds ratio; COR: crude odds ratio.
Discussion
The present study reveals that the mean score overall level of epileptic patients’ HRQoL was 51.98 ± 10.08 (95% confidence interval (CI): 41.90–62.06), which was comparable with studies done in Uganda and Kenya, 58.00 and 49.90, respectively.22,23 It was also consistent with studies conducted in Ethiopia at Jimma College Medical Center (58.80), 14 Addis Ababa Amanuel Mental Specialized Hospital (56.36), 15 Ambo General Hospital (56.43), 6 Wollega zone public hospitals (60.47), 9 Russia (48.67 ± 10.80), 24 and Japan (46.40 ± 33.20 to 60.90 ± 30.50), 25 but differed from studies conducted in Mekelle City (77.97%). 2 The consistency in the above studies’ results may be since the study in Mekelle used the Quality of Life in Epilepsy Inventory-31 (QOLIE-31) instrument, which focused on seizure worry, well-being, energy/fatigue, cognitive performance, and medication effects. This result is also lower than in studies from the United Kingdom (76.50), 26 Brazil (68.73), 27 and Malaysia (68.90). 7 This difference could be because, in these countries, the quality of health services and the socioeconomic status of the population were better than in Ethiopia. On the contrary, in Africa, which includes the population of the present study, there was low socioeconomic status, and the number and level of health facilities were lower compared with the population size, which could affect the HRQoL of PLWE 28 , 29
According to these results, the HRQoL in the physical domain ranked relatively higher (58.60) on the WHOQoL-BREF scale compared with the social (53.30), psychological (50.25), and environmental domains (48.75). However, the result of this study in the physical domain was lower than that in a study from Brazil (72.76). 30 The discrepancy could be since the treatment approach for epilepsy in this hospital does not focus on a holistic approach that includes the psychological, social, and environmental needs of the patients, rather than focusing only on seizure control.
The results show that the mean scores of the psychological domain (such as the meaningfulness of life, the ability to focus on daily activities, and the ability to accept the appearance of the body) on the WHOQoL-BREF scale were 50.25. The environmental domain (which was the healthy state of the living environment, the availability of information about daily life, and the accessibility of health services, including transportation) was 48.75; this is lower than the mean scores of the physical domain (58.60) and the social domain (53.30).
This difference could be because most of the study participants were single, illiterate, and unemployed. These factors could affect the psychological perspective of PLWE. On the contrary, 12.20% and 37.00% of the study participants suffered from depression and anxiety, respectively, which might have contributed to the psychological domain of the WHOQoL-BREF scale. Regarding the environment, almost half (47.90%) of the study participants live in a rural area, which could affect the health status of the living environment, the availability of information about their daily life, and the accessibility of health services and transportation.
Educational status (secondary) was negatively related to good HRQoL. Patients who had completed secondary school were 83.30% less likely to have a good HRQoL than patients who were not literate (adjusted odds ratio (AOR) = 0.17, 95% CI: 0.06, 0.46). However, other studies conducted in Uganda and Kenya show that a high level of education was strongly associated with a good HRQoL.22,23 Similarly, in Ethiopia, studies conducted at Amanuel Mental Specialized Hospital, Ambo General Hospital, and Mekelle City associated high educational attainment with good HRQoL in PLWE.2,6,15 The reason might be due to educated patients having a good understanding of the natural disease history of epilepsy, and they were good at adhering to the treatment. This study reveals that the age of the participant had associated with good HRQoL in the patient age group between 25 and 34 years. This could be because educated patients have a good understanding of the natural history of epilepsy and can adhere well to treatment. This study shows that the age of the participants was associated with good HRQoL. The 25- to 34-year-old age group was 59.10% less likely to have a good HRQoL than the 18- to 24-year-old age group (AOR = 0.41, 95% CI: 0.19, 0.88). This study was consistent with studies from Malaysia and Italy.7,27
Occupational status was associated with good HRQoL. Self-employed patients were 1.16 times more likely to have a good HRQoL than those who were unemployed (AOR = 2.16, 95% CI: 1.00, 4.64). This study was supported by studies in Kenya 23 and Ethiopia at Jimma University Medical Centre. 14 The consistent results could be that patients who have a job can pay for their treatment costs, transportation, and other health-related costs. Moreover, employed patients also had relatively more financially stable to meet their daily needs compared with unemployed patients.
The present study found that patients who lived in urban areas were 7.07 times more likely to have a good HRQoL than patients who lived in rural areas (AOR = 7.07, 95% CI: 3.57, 14.01). This study was consistent with a study from Kenya 23 and studies from Ethiopia at Jimma University Medical Centre. 14 The above finding could be because patients living in rural areas are not able to get complete information about their health status, reach health facilities near them, and have limited opportunities to participate in recreational activities.
Marital status was associated with good HRQoL. Married patients were 2.50 times more likely to have a good HRQoL (AOR = 2.53, 95% CI: 1.62, 3.94) than single patients. This result is consistent with a study conducted in Uganda. 22 The possible reasons for this difference could be that married patients have stable living arrangements, and they can receive psychological support from their partners and feel comfortable in their relationships.
The presence of comorbid diseases was another factor related to HRQoL. Those without a comorbid disease were 3.57 times more likely to have a good HRQoL than patients with a comorbid disease (AOR = 3.57, 95% CI: 1.30, 9.80). This study was consistent with studies from India. 1 Similarly, in Ethiopia, studies conducted at Jimma University Medical Centre, Ambo General Hospital, and public hospitals in Wollega zones suggest that the absence of comorbid conditions is a good predictor of good HRQoL.9,14,15 According to works of literature, patients who did not have comorbid conditions such as depression, anxiety, cognitive impairment, and psychosocial problems had good HRQoL compared with patients who had a comorbid condition.
Patients who had family support were 9.28 times more likely to have a good HRQoL (AOR = 9.28 95% CI: 1.07, 80.18) than patients who did not have family support in their lives. On the contrary, PLWE who participated in recreational activities were 2.23 times more likely to have a good HRQoL (AOR = 2.23, 95% CI: 1.18, 4.20). The finding may be because individuals who have good personal character can avoid negative feelings in their personal lives, focus on their daily activities, enjoy their lives, and make their lives meaningful. Unlike other studies,2,4,6 seizure type, frequency, and duration were not significantly associated with good HRQoL in our study.
Limitation of the study
The cross-sectional design of this study limited the identification of causal relationships. Moreover, this study was conducted in a governmental referral hospital. Therefore, the score may not reflect the HRQoL of patients with epilepsy in other healthcare systems. This study aimed to assess the HRQoL of PLWE and only sourced the data from the epilepsy OPD clinic of DRH. Thus, the results may not be generalized to PLWE in Ethiopia.
Conclusion
The average overall HRQoL of PLWE in the DRH was low compared with similar studies. Young adults (25–34 years), secondary education, married, divorced, self-employed, urban residence, presence of current comorbidity, family support, and recreational activities were associated with good HRQoL of PLWE. In general, concerted efforts need to be made to improve the HRQoL of PLWE at DRH in Ethiopia.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221129146 – Supplemental material for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221129146 for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study by Alebachew Sisay Stotaw, Prem Kumar, Dessale Abate Beyene, Tamrat Assefa Tadesse and Alfoalem Araba Abiye in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221129146 – Supplemental material for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study
Supplemental material, sj-docx-2-smo-10.1177_20503121221129146 for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study by Alebachew Sisay Stotaw, Prem Kumar, Dessale Abate Beyene, Tamrat Assefa Tadesse and Alfoalem Araba Abiye in SAGE Open Medicine
Supplemental Material
sj-docx-3-smo-10.1177_20503121221129146 – Supplemental material for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study
Supplemental material, sj-docx-3-smo-10.1177_20503121221129146 for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study by Alebachew Sisay Stotaw, Prem Kumar, Dessale Abate Beyene, Tamrat Assefa Tadesse and Alfoalem Araba Abiye in SAGE Open Medicine
Supplemental Material
sj-docx-4-smo-10.1177_20503121221129146 – Supplemental material for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study
Supplemental material, sj-docx-4-smo-10.1177_20503121221129146 for Health-related quality of life and its predictors among people living with epilepsy at Dessie Referral Hospital, Amhara, Ethiopia: A cross-sectional study by Alebachew Sisay Stotaw, Prem Kumar, Dessale Abate Beyene, Tamrat Assefa Tadesse and Alfoalem Araba Abiye in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank all study participants for their time and willingness to participate in the study. We would also like to express our sincere gratitude to the staff of the Epilepsy OPD at DRH and the data collectors for their support throughout the study period. We would also like to thank Wollo University, the College of Medicine and Health Sciences, the School of Nursing and Midwifery, and the Department of Adult Nursing for allowing us to conduct this research.
Authors’ contributions
ASS designed the study, participated in and supervised data collection, analyzed the data, and wrote the first draft of the article. PK, AAA, and TAT participated in the design, review, and modification of drafts of the article. DAB also participated in the writing of the first draft, review, and analysis of drafts of the article. All authors read and approved the final version of the article.
Data availability
All data supporting the findings are adequately included within the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the ethical review committee of Medicine and Health Sciences, Wollo University (Ref. No; 321/09/2012).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
A written informed consent was obtained from all subjects before the commencement of the actual data collection process, and the study subjects had the decisional capacity to participate in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.