
Abstract
Objectives:
The purpose of this study was to evaluate whether health-related quality of life and levels of sense of coherence among people with obesity are correlated with body mass index, age, and gender.
Methods:
A cross-sectional, descriptive research design was used. Subjects (n = 157) were selected from a sample of participants in an ongoing survey and had a body mass index >30 kg/m2. Data were collected using the Short Form-36 Health Survey and the Sense of Coherence Scale.
Results:
The mean body mass index of women was higher than that of men. Compared to men, a greater proportion of women had a low sense of coherence. There was a significant relationship between low physical health and high body mass index. Female gender and older age correlated with a low sense of coherence and showed a significant association with high body mass index.
Conclusion:
To increase the health-related quality of life, people with obesity need support to help manage their life situation based on their individual needs and personal resources.
Introduction
According to the World Health Organization (WHO), 1 obesity has been declared as a global epidemic with significant association with many chronic diseases and health conditions. There are currently approximately 400 million clinically obese adults around the world. 1 The general prevalence of obesity has increased rapidly in many regions, including the United States and many European countries such as Sweden. In Sweden, the prevalence of obesity (body mass index (BMI) > 30 kg/m2) among middle-aged people doubled over the last two decades and accounts for approximately 10% of the adult population. 2 Eriksson et al. 3 reported that the prevalence of obesity continues to increase, but with a shift in the distribution of BMI by age. Specifically, those authors found that BMI has become more stable in younger people and has decreased among older adults. Other studies2,4 have also shown an overall increase in obesity over time, especially among women.
Obesity is defined as a condition of abnormal or excessive fat accumulation in adipose tissue to such an extent that health may be impaired. A BMI exceeding 30 kg/m2 increases the risk for diseases, especially cardiovascular diseases, diabetes, and some cancers.5,6 However, obesity is not only a threat to the individual’s physical health, it is also an important factor in health impairment related to experiences of well-being and quality of life.7,8
The concept of health is broad and has been conceptualized in both positive and negative denominates over time. The most widely used definition of health was developed by the WHO 9 which describes health as “a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.” This definition considers health from a holistic perspective and does not focus solely on the physical dimension. Therefore, health cannot be defined only in terms of the absence of an illness or disease such as obesity. Aspects of quality of life are important factors in the domain of health and illness, as clinical or objective indicators used to assess health status cannot provide a complete picture.10,11 Given that health includes both subjective and objective indicators, 12 health needs should also be considered in relation to quality of life (health-related quality of life (HRQoL)) and include the individual’s perspective on health, life satisfaction, and well-being. 13
The relationship between obesity and HRQoL has been studied in a number of population-based studies.14–19 The research concluded that the HRQoL of many obese persons is low. Furthermore, it has been found that obesity has a negative impact on physical functioning, such as impaired general health perception and vitality; 7 psychological functioning; and social well-being. 20 Factors reported to be associated with severe impairments of HRQoL among people with obesity include gender21–24 and psychological variables, such as low self-esteem, negative self-image, and poor social relations. 25 Additionally, individual characteristics may influence HRQoL, such as perceptions about one’s health situation as well as attitudes and values about treatment and self-management.
To measure an individual’s resources, levels of sense of coherence (SOC) can be investigated and can provide significant knowledge about how a person may handle a potentially stressful situation, such as managing obesity. 26 Brown and Psarou 27 observed that there has been a lack of attention on the personal characteristics that people with obesity need for self-management and to make successful lifestyle changes. Elfhag and Rössner 28 suggested investigating the associations between obesity and personal resources to better understand obese people’s life situation and to develop knowledge that will improve healthcare professionals’ capacity to support health, self-management, and lifestyle changes. Therefore, the purpose of this study was to evaluate whether HRQoL and levels of SOC among people with obesity are correlated with BMI, age, and gender.
Methods
A cross-sectional, descriptive research design was performed as data were collected at one point in time. This design is appropriate for describing a phenomenon and the relationships among factors that influence it, for example, to determine whether HRQoL and SOC are correlated with BMI, age, and gender. This study was conducted according to the principles expressed in the Declaration of Helsinki. The study sample was provided with information about the aim and content of the research, and provided written consent (a returned completed questionnaire) for their participation. The study sample was assured of confidentiality regarding the information they provided. It was also made clear that their participation was voluntary and that they could withdraw from the study at any time. The study was approved by the Regional Ethical Review Board, Sweden.
Study sample
This study selected participants from the northern Sweden component of the multinational MONItoring of trends and determinants in CArdiovascular disease (MONICA) population survey. The MONICA survey began in the early 1980s to follow trends in cardiovascular risk factors globally. 29 Altogether, 41 study centers, spanning 26 countries and 4 continents, joined the MONICA survey. One of these centers was located in northern Sweden, including the two northernmost counties of Norrbotten and Västerbotten (target population 312,000). The worldwide MONICA study ended after 10 years with a total of six population-based surveys conducted between the time period of 1986 and 2009.
In 2009, 1729 subjects between 25 and 74 years of age were randomly selected from the population register of the MONICA survey. The subjects were stratified for age and gender; details of sampling, selection, and data in the MONICA survey have been presented elsewhere. 3 To perform the survey, two teams operated in each county (Norrbotten and Västerbotten), from January to April 2009. The teams traveled to approximately 40 healthcare centers, in the two counties. All individuals selected to participate in the 2009 MONICA survey were invited to visit their closest healthcare center. Of these individuals, 237 met the inclusion criteria of having a BMI >30 kg/m2. All of these individuals were specifically invited to participate in this study when they visited a healthcare center (n = 231). The research nurse on the MONICA team distributed an informational letter and the questionnaires, which included the Short Form-36 (SF-36) Health Survey and the Sense of Coherence (SOC) Scale. The informational letter informed participants about the aim of this study and the research process, and that all returned, completed questionnaires were considered to be written consent for participation. The study sample was assured of confidentiality of the information they provided and that their participation was voluntary. The participants could either answer the questionnaires at the healthcare center or at home. The estimated time required to answer each questionnaire was approximately 15 min. All returned questionnaires (n = 157) were answered at the healthcare center.
Data collection
Data were collected with two questionnaires: the SF-36 Health Survey and the SOC Scale. Demographic data such as age, gender, and BMI were gathered from the subjects by the MONICA research nurse when the informational letter and the questionnaires were distributed. In total, 231 questionnaires were distributed, and 157 completed questionnaires were returned. Each questionnaire will be presented below in more detail.
The SF-36 Health Survey
The SF-36 is a generic, standardized questionnaire based on the WHO definition of health concepts which include physical capacity, general health, vitality, and mental well-being. The questionnaire is used to measure self-rated health status and provides insight into individuals’ conditions and limitations in daily life during the prior 4 weeks.30,31 The questionnaire is validated for generic health assessment and also used in obesity research.7,32 The SF-36 contains 36 items divided into eight domains: Physical Functioning (PF), Role Physical (RP), Bodily Pain (BP), General Health (GH), Vitality (VT), Social Functioning (SF), Role Emotional (RE), and Mental Health (MH). Each of the 36 items was scored on a scale from 0 to 100, with 100 representing the most optimal state of health. Furthermore, two summary scores of the eight domains can be combined to provide an overall description of subjective health status. The Physical Component Summary (PCS), which includes PF, RP, BP, and GH, summarizes physical health status, and the Mental Component Summary (MCS), which includes VT, SF, RE, and MH, summarizes mental health status. The two summary scores, which provide a concise picture of a person’s HRQoL, can explain approximately 80%–85% of the total variance. 31 The evidence for the validity of the SF-36 is considerable, and Cronbach’s alpha calculated for the eight subscales ranges from .67 to .95. Cronbach’s alpha in this study was .82.
The SOC Scale
The SOC Scale is developed by Antonovsky 26 to reflect a person’s capacity to respond to stressful situations, such as managing obesity. The SOC Scale used in this study was the Swedish version of the questionnaire. 33 The questionnaire covers three dimensions of the SOC Scale via 29 items: comprehensibility, manageability, and meaningfulness. The three dimensions investigate the ability of the people to understand what happens around them, to what extent they were able to manage the situation on their own or through significant others in their social network, and the ability to find meaning in the situation. The 29 items are presented on a 7-point Likert scale with scores ranging from 29 to 203. A higher score suggests a stronger SOC; however, extremely high scores indicate rigidity (no cutoff point is mentioned). Antonovsky 26 recommends the use of the SOC questionnaire as a measurement of all the dimensions together and not examine the three subscales separately. The structure and properties of the SOC Scale show a face validity and content validity with Cronbach’s alpha coefficient ranging from .82 to .95. 34 Cronbach’s alpha in this study was .85.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science (version 17.0; SPSS Inc, Chicago IL, USA). In total, 231 questionnaires were distributed, and 157 completed questionnaires were obtained for analysis of the SF-36 and the SOC Scale, yielding a response rate of 68%. All data were first divided into two age groups (24–49 years and 50–74 years), according to the MONICA survey. Thereafter, a median split (high and low SOC scores) was used to create groups for comparison of associations between the SOC Scale, HRQoL, BMI, age, and gender. An initial descriptive analysis conducted on all the tested variables found that most of the variables were not normally distributed. Therefore, medians and non-parametric tests were used in most analyses. Pearson’s χ2 test was used to determine the relationships between the SOC Scale and age, gender, and BMI; HRQoL and age; and gender and BMI. The predictive value of the SOC Scale and HRQoL was assessed by logistic regression analyses. The dependent variables were high and low SOC scores, and the independent variables were demographic characteristics, such as BMI, age, and gender. The significance of each independent variable was evaluated using a t-test and one-way analysis of variance (ANOVA). Trends were analyzed using generalized linear models, and a p value <.05 was considered to be statistically significant for all tests.
Results
The distribution of the study sample (n = 157) was relatively equal according to age and gender (n = 86 women vs n = 71 men). The mean age of women was 49.8 years (standard deviation (SD) = 13.8 years) and that of men was 47.8 years (SD = 12.4 years). The mean BMI was higher for women (34.7) than for men (33.5), and no correlation between BMI and age was found.
Relationship between HRQoL, gender, age, and BMI
The comparison between women and men revealed significant differences in PF (p = .001), RP (p = .000), and RE (p = .006), all to the disadvantage of women. The results of the two health measures (PCS and MCS) showed that the scores of women were lower than those of men. Evaluation of MCS by gender further showed that women in this study had a lower value (46.9) than the reference value 30 (49.4). The same phenomenon was observed among men (49.8 vs the reference value 50.7). Significant differences were found in PCS between women and men (44.4 for women vs 48.9 for men; p = .001). Regarding MCS, no significant differences were noted between women and men (p = .099) (see Table 1).
HRQoL outcome, Physical Component Summary (PCS), and Mental Component Summary (MCS) for gender and age.

HRQoL: health-related quality of life; PF: Physical Functioning; RP: Role Physical; BP: Bodily Pain; GH: General Health; VT: Vitality; SF: Social Functioning; RE: Role Emotional; MH: Mental Health.
PCS and MCS reference values for the normal Swedish population. 30
p ≤ 0.05 (independent samples t-test).
The comparison of the age groups (24–49 years and 50–74 years) showed that older subjects had a greater prevalence of low PF (p = .002) and RP (p = .003). Older subjects also showed lower PCS (43.2 vs 49.4), but higher MCS (49.7 vs 46.9). However, no significant differences were found between PCS (p = .079) or MCS (p = .886) scores and age group (see Table 1).
The relationship between BMI and MCS and PCS scores of women and men is illustrated in Figure 1. The linear relationships showed a weak negative correlation between BMI and PCS scores of both women (R1 = −.0140, p = .205) and men (R1 = −.148, p = .220) and a weak positive correlation between BMI and MCS scores for both women (R1 = .073, p = .547) and men (R1 = .022, p = .839).
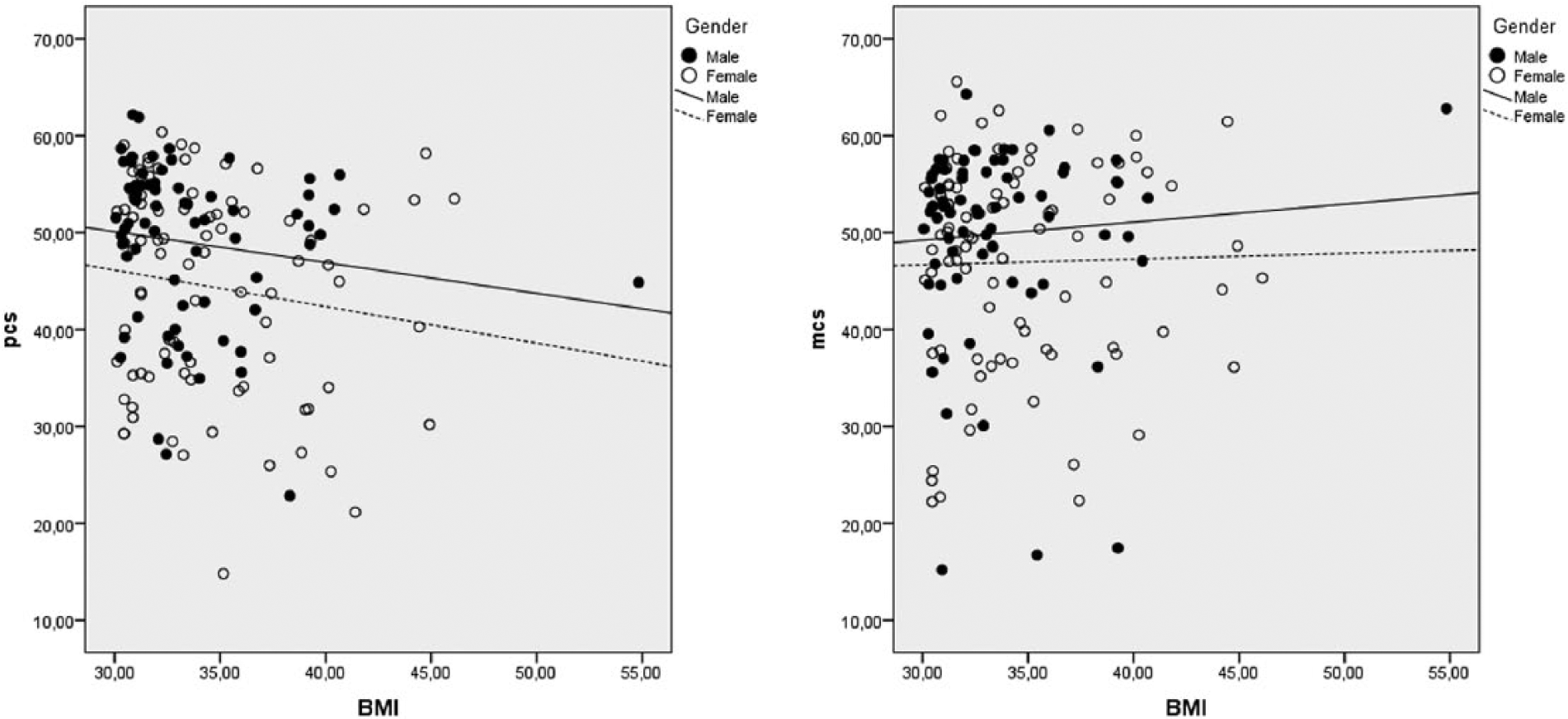
The relationship between BMI and MCS and PCS of women and men.
Relationship between SOC, BMI groups, gender, and age
The mean SOC score among women was lower (140.2) than that of men (150.1), although there was no significant difference (p = .200). In regard to the relation between SOC and BMI, women with high BMI had a higher burden of lower SOC scores (≤34.9, 58.2%, and ≥35.0, 64.5%) than men (≤34.9, 34%, and ≥35.0, 50%) (seeTable 2). The comparison between SOC and age groups showed that a low SOC score (≤146) was more common in age group II (52%) than in age group I (47.6%).
SOC and BMI of women and men.

SOC: sense of coherence; BMI: body mass index.
p ≤ 0.05 (Pearson’s χ2 test).
The relationship between BMI and the SOC score showed a negative linear relationship between women (R1 = −.186, p = .086) and men (R1 = −.031, p = .800).
Discussion
In this population-based, cross-sectional study, it was found that BMI had an impact on HRQoL. Research18,35,36 assessing BMI and HRQoL has shown that obese people feel significantly impaired in HRQoL as a result of their obesity and that this impairment increases in accordance with BMI values. In this study, the mean BMI was higher for women than for men. According to Lilja et al., 32 obesity has increased more among women (17.8%) than among men (14.7%) in northern Sweden during the time period of 1986–2004. Furthermore, as demonstrated in this study, research 37 has shown that the distribution pattern of BMI values appears to be the same irrespective of age (i.e. BMI does not appear to be age specific).
As the results in this study show, women have lower HRQoL than men. 38 The observed differences in this study can thereby be interpreted as being gender dependent. According to Singh and Dixit, 10 two important factors that can explain gender differences in HRQoL are physiological and psychosocial factors. With regard to physiological factors, women are more likely than men to have co-morbid conditions such as hypertension and diabetes related to obesity, 30 and women tend to be older at the onset of the disease. 39 However, research40,41 has concluded that these gender differences could partly be explained by etiology. Gender differences in HRQoL due to psychosocial factors encompass factors such as how people perceive their health, as well as health in relation to functional status. 10 According to Carryer, 42 thin women feel healthier than obese women. Obese women also have to struggle against attitudes related to obesity, which may in turn affect their perceptions of HRQoL. 43 For women with obesity, attitudes and social expectations of thinness according to Western standards affect their perception of HRQoL and result in an increased level of dissatisfaction with their bodies, compared to men.44–46 Women with chronic illnesses also reported lower HRQoL if they were unable to participate in social events and socialize with friends and family members. 47 Singh and Dixit 10 stated that chronic diseases, such as obesity, pose challenges for individuals and their family members. As HRQoL is dependent on effective health interventions, it can be interpreted that individual health management of obesity is very important. Health management strategies and support should therefore be based on individuals’ experiences, life situation, needs, and levels of HRQoL.
The results of this study further indicated that age and gender were affected for both the PCS and MCS. This finding is confirmed by the reference value for the general population in Sweden. 30 A marked change in physical health is observed among women over 50 years, whereas similar change occurs 5 years later among men. 31 People with obesity are often severely hindered in their ability to perform their day-to-day physical activities.7,36 When the limitations of physical health measures impede physical activity, it can be interpreted that physical health is controlled by age. 30 According to Kolotkin et al., 23 there appears to be an association between BMI and the degree of physical and mental health impairment, in that severely obese individuals report significantly greater decrements in energy to perform physical activities than those of individuals with a lower degree of obesity. Robinson et al. 48 observed that women are more prone to low physical functioning than men, which may be connected to a higher BMI value. The correlation between obesity and mental health has been discussed,11,24 and it has been shown that obesity affects physical health more than it does mental health. The conclusion that BMI appears to have little impact on mental health is consistent with our study findings.
Furthermore, the results in this study indicated that a low SOC score was more common among subjects with a high BMI value. This finding is consistent with Antonovsky’s 26 theoretical framework that describes that SOC is influenced by degree of illness. A low SOC score, therefore, suggests that obese people require more support for health management. Compared to men, women in this study had a greater proportion of low SOC scores which might mean that women need more support to cope with their health and life situation. This finding is consistent with the results of the previous clinical-based studies8,49 and population-based studies, 44 and also with previous research of patients with obesity or other chronic illnesses. 22 Conversely, people with a strong SOC are generally more resilient to stress and are better able to seek solutions by themselves to cope with a health problem. 50 A strong SOC score has also been significantly correlated with improved HRQoL and can be a protective factor for people facing stressful health situations, such as managing a disease. 51 These benefits may be related to the role SOC plays with respect to personal resources available to manage health problems, which have proven to be psychometrical with multidimensional characters rather than a uni-dimensional concept.
The results in this study also showed that a low SOC score was more common in the older age group. It is found that SOC scores tend to increase with age throughout the entire lifespan, 52 but previous research 53 has shown little differences between SOC scores and age. Langius and Antonovsky 34 reported that SOC scores often stabilize by the end of early adulthood with only minor changes observed thereafter. Liukkonen et al. 54 describe SOC as an independent psychosocial construct in a person’s evaluation of health. According to the above-described research and the results in this study, SOC scores may be an indicator of an individual’s health promotion and health management needs, regardless of age or gender. Health management can prevent a negative progression of obesity and illness, as well as increase HRQoL. Interventions designed to increase people’s willingness to change and increase motivation, confidence, and understanding of the importance of lifestyle changes must be discussed beyond future health risks. 46 Primary healthcare has been observed to be well suited to deliver obesity advice and support health management. Primary healthcare professionals can help an individual focus on personal health problems and support health engagement, thereby improving the success of health management strategies.55,56 Accordingly, it is imperative that we shift the focus from problems and obstacles to patient resources by incorporating data relevant to the SOC concept into the systematic orientation and perspective as well as the daily activities and actions of healthcare professionals. 53 HRQoL data should also be a part of care planning and health management for both the patient and clinicians involved in patient care. However, for these data to be useful, it must be in a format that patients and professionals can easily interpret and integrate with clinical information. In addition, discussions of HRQoL data in clinical practice should be based on the patient’s needs, wishes, and socio-demographic characteristics as well as clinicians’ attitudes toward HRQoL measures. 57
A limitation of this study included the use of self-reported data, which can lead to inaccurate information due to individual perceptions of the questions. The questions of HRQoL are subject to individual interpretation and are not based on obvious facts that would allow definitive conclusions to be made about the association between obesity and HRQoL. We attempted to reduce this limiting factor for each participant as well as reduce the numbers of incomplete surveys in the analysis by having a research nurse on the MONICA team available for questions. The study sample was composed entirely of obese people selected from a population survey and cannot be considered representative of the general population of obese people. The results were not compared with the normal weight group as we were not able to include the non-obese sub-samples in this study. Therefore, this study cannot make conclusions about the causes and effects or sequence of obesity, as the study measured the results at one specific time point based on one group of subjects. A further limitation was that data on other possible confounders, such as depression or complications related to obesity, were not included in the analysis, which may affect the levels of SOC and HRQoL. However, the use of the two well-validated questionnaires, the SF-36 Health Survey 31 and the SOC Scale,33,34 is considered a strength of this study’s results.
To conclude, this population-based cross-sectional study showed that women have a higher BMI than men and that BMI was significantly associated with low SOC scores. The PCS and MCS showed that women have lower scores than men. Furthermore, significant differences were found between gender and PF and between RP and RE, all to women’s disadvantages. This knowledge indicates that women are more at risk of lower HRQoL and have fewer personal resources to manage their health situation. In order to further understand which resources people with obesity, and especially women, need to manage their health, prospective and longitudinal studies are required. Further research aimed at exploring the meaning of HRQoL among people living with obesity and which emphasizes the importance of their lived experience is therefore needed.
Footnotes
Acknowledgements
The authors thank all the participants of this study for their valuable contributions. We also thank the research nurse, MONICA study, for all the help with the selection of the study sample.
Declaration of conflict of interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.