
Abstract
In the wake of the COVID-19 pandemic, many nations around the world instituted strict social distancing measures. Although necessary to deter the spread of the virus, these measures may also have had adverse health repercussions by increasing social isolation. Using a national longitudinal study from Canada, in which respondents were surveyed in March 2020 at the beginning of stay-at-home orders and again two months later in May, we show that, at baseline, loneliness was inversely associated with perceptions of self-rated health, and there was a beneficial indirect association between respondents’ number of social network confidants and perceived health through lower levels of loneliness. Between March and May, social network confidants decreased and loneliness increased; these changes were independent of each other and contributed to declines in self-rated health. Greater loneliness at baseline was also associated with declines in self-rated health. Our observations suggest that social distancing during the COVID-19 pandemic impaired social connectedness, thereby resulting in declines in perceptions of health. We conclude by discussing several policy-related implications of our findings.
The desire for social connection is a fundamental human need that is crucial for individual well-being (Thoits 2011; Turner and Brown 2010). Yet, in the wake of the COVID-19 pandemic, many nations across the world instituted unprecedented strict social distancing measures that included advising much of the population to stay at home, as well as banning social gatherings and closing schools, places of worship, and many workplaces (Douglas et al. 2020). Although necessary to curb the transmission of COVID-19, some health scholars also voiced concern that these social distancing measures could result in prolonged isolation that would have adverse consequences for well-being (Vieira et al. 2020).
Indeed, daily social life underwent a seismic shift in routine and organization when stay-at-home issues were put into place in the early months of 2020. Work and communication with family and friends shifted almost exclusively to an online environment. Although technological tools (e.g., Zoom, FaceTime) have made it possible to remain in contact with close friends and family members at the outset of the pandemic, emerging evidence suggests that virtual connection is not as conducive as face-to-face contact for discussing personal problems. For instance, some evidence suggests that virtual screen time at this initial stage of the pandemic was associated with lower mental well-being (Ellis, Dumas, and Forbes 2020; Stieger, Lewetz, and Swami 2021). In addition, past research on support crisis situations shows that face-to-face contact, but not virtual interaction, was associated with improved well-being (Hawdon and Ryan 2012). Since remote interactions lack the richer experience of person-to-person interaction, which also encompass physical touch and the ability to read verbal and nonverbal expressions more accurately, virtual communication may not be an effective means of buffering against feelings of social isolation. Thus, many people may be left feeling disconnected and unable to discuss personal problems with close confidants during a time of intense stress when support is especially needed. Due in part to a disruption of social contacts, some have increasingly turned to unhealthy coping methods, such as greater use of substances like alcohol (Rogers et al. 2020) as well as opioids (Alexander et al. 2020). A critical question is therefore how social connection changed in the context of COVID-19 social distancing measures and the implications for well-being at the start of the pandemic as individuals struggled to adjust to the “new normal.”
Our study considers whether any relationship between social network size and perceptions of health works through reduced loneliness as a mechanism. Imposed quarantine is both an unfamiliar and unpleasant experience that involves a departure from usual everyday routines and physical separation from friends and family. Much research documents the importance of supportive others in one’s social network for individual health (Thoits 2011), and immersion in a network of supportive others has a clear tendency to deter loneliness (Rote, Hill, and Ellison 2013). Loneliness is in turn damaging to a number of health outcomes (Cacioppo and Cacioppo 2014; Ong, Uchino, and Wethington 2016), through such mechanisms as impaired health behaviors and elevated levels of stress (Cacioppo and Hawkley 2009). The sum of the breadth of these adverse health effects will tend to be reflected in one’s perceptions of their overall health (Doiron et al. 2015).
To examine these interrelationships, we use a unique panel survey of Canadians, where the first wave of data collection occurred during the early stages of the pandemic in March of 2020, shortly after stay-at-home measures were instituted across Canada, and a second wave was administered two months later in May. This study therefore contributes policy-relevant information to the study of population health during the COVID-19 pandemic by considering the extent of decreases in key markers of social connectedness, and whether these changes are in turn detrimentally associated with individual perceptions of health during this period of crisis. These social distancing measures created a context where we can witness the real-time importance of social connections and network confidants—and what happens when those are eroded or limited. Given the potentially lifesaving effects of social distancing measures and current debates regarding their continued implementation (e.g., Allcott et al. 2020), it is vital for health professionals and policymakers to recognize whether the loss of close social network members affects loneliness and health outcomes at the population level.
Background
Loneliness and Health
Figure 1 depicts our conceptual model for this study. This model locates loneliness as a key influence on health. Loneliness is an evaluative construct that reflects individual evaluations of social relationships as failing to meet individual and social needs, particularly when the individual is not satisfied by the degree of intimacy (Hughes et al. 2004). The central role of loneliness as an evaluative construct leads loneliness to serve as a primary conduit for the effects of supportive social networks on perceptions of health (Uchino 2004). We therefore begin by detailing the ramifications of loneliness for self-perceptions of health, giving special attention to the onset of social distancing measures in response to the COVID-19 pandemic. In a subsequent section, we expand on these ideas, describing how social networks of close confidants will influence perceptions of health through loneliness, as well as how changes in the number of social network confidants during the pandemic may have negatively influenced perceptions of health through increased loneliness.
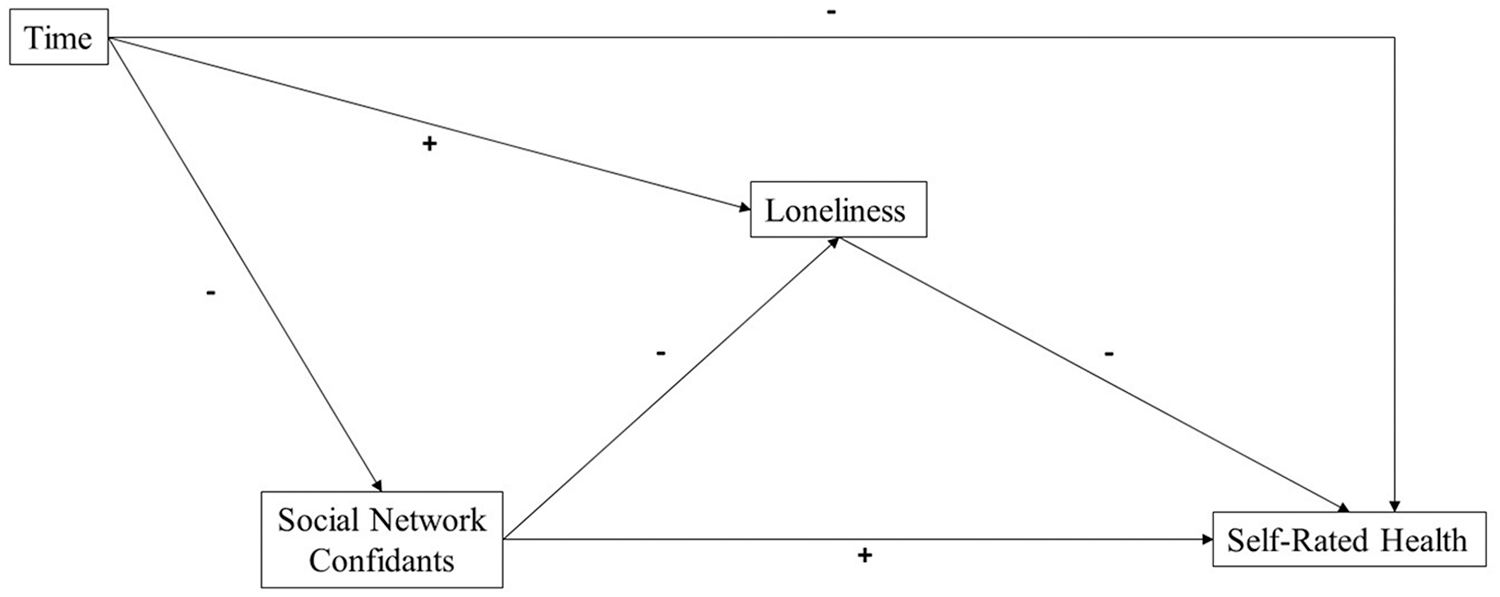
Conceptual model of the indirect associations between social network confidants, loneliness, and self-rated health.
Even prior to the COVID-19 pandemic, some scholars characterized North American and other Western nations as in the grip of an “epidemic” of loneliness (e.g., Jeste, Lee, and Cacioppo 2020). The severing of social contacts that was required in response to the pandemic led to concerns that a public that was already quite vulnerable to loneliness would be especially likely to experience increases in loneliness due to these changes. As Sharma, Maheshwari, and Bronsther (2020) noted, “forced quarantines and social distancing imposed by the COVID-19 crisis are likely to further exacerbate the loneliness epidemic” (p. 32). Indeed, comparisons of cross-sectional population surveys from 2018 and during the pandemic indicate higher rates of loneliness during the pandemic than in years prior (McGinty et al. 2020). Community samples of young adults in Canada in the United Kingdom also appear to support these concerns, showing increases in loneliness between early in 2020 and later in April and May 2020 (Folk et al. 2020; Lee, Cadigan, and Rhew 2020). Similar results were also observed in a small community sample of older adults in the United States (Krendl and Perry 2021) and in a small sample of older Swiss adults (Macdonald and Hülür 2021). Taken together, these studies from diverse samples with data coinciding with the beginning of the COVID-19 pandemic and onset of stay-at-home orders suggest that loneliness increased over this short period of time.
We focus on self-rated health as an outcome because changes in loneliness during the pandemic are likely to have had acute detrimental consequences for health that would be reflected in perceived health. Critically, self-rated health is a perceptual measure that combines active experiences of physical and mental well-being with unconscious evaluations of bodily sensations (Au and Johnston 2014; Jylhä 2009), though physical functioning is found to be more strongly associated with perceptions of self-rated health than mental functioning (Mavaddat et al. 2011). The sensitivity of self-rated health to multiple systems and unconscious experiences results in a highly dynamic measure that is responsive to bodily fluctuations (Benyamini 2011) and may be ideal to capture any health changes occurring amid the vast reorganization of social life that characterized the outset of the pandemic. Indeed, self-rated health has been lauded by health scholars for its ability to capture not only more immediate changes in physical and mental health, but also somatic concerns that may be physical manifestations of stress (e.g., stomach aches, fatigue) (Caetano, Silva, and Vettore 2013; Ferraro and Wilkinson 2015) which may not typically result in diagnosable medical ailments until years later.
Theoretical and empirical support for the proposition that changes in loneliness can have acute effects on perceptions of health can be found within the evolutionary theory of loneliness. According to this theory, transient (shorter, or intermittent) periods of loneliness may function as an alarm to motivate individuals to reconnect with others. If reconnection does not occur, these feelings might become exacerbated and lead to further disruption and feelings of distress that can interfere with multiple physically restorative health behaviors and systems (Cacioppo and Hawkley 2009; Cacioppo et al. 2006). Moreover, as an acute signal of social threat, loneliness is robustly associated with acute physiological stress responses (Brown, Creaven, and Gallagher 2019). In support of these arguments, baseline levels of loneliness have been shown to predict subsequent declines in self-rated health (Luo et al. 2012; Tsur et al. 2019), and decreases in loneliness has have be shown to be favorably associated with subsequent self-rated health (Nummela, Seppänen, and Uutela 2011). Moreover, in a longitudinal study of households in Spain, Martín-María et al. (2020) found that transient loneliness was associated with worse self-rated physical health scores relative to the never lonely, both cross-sectionally at each wave and over time.
We therefore suggest that baseline levels of loneliness at the beginning of the COVID-19 pandemic will be inversely associated with initial perceptions of self-rated health. In addition, we expect that there will be increases across the population in loneliness during the COVID-19 pandemic, as well as a decline in perceptions of self-rated health, and increases in loneliness will contribute to explaining declines in self-rated health.
Social Network Confidants during the Pandemic
As Figure 1 illustrates, the breadth of one’s social network confidants is likely to be a primary contributor to loneliness, with decreases in networks during the COVID-19 pandemic contributing to increases in loneliness. We examine social network confidants in terms of the number of people with whom a respondent can discuss “intimate” or “important” matters. This measure captures a vital component of social isolation because assessment of the number of social contacts that are available to provide supportive interactions is critical for a sense of enmeshment in a network of supportive relationships (Wellman and Gulia 1999). As demonstrated in empirical research, one’s network of social confidants will therefore act as a bulwark against loneliness by reinforcing a sense of connection and rewarding social relationships, in turn influencing self-rated health (Chen and Feeley 2014; Ong et al. 2016).
We posit that stay-at-home orders and associated social distancing measures during the COVID-19 pandemic would be critical for declines in networks of social confidants that would lead to increases in loneliness. Recent research shows that a decline in the size of one’s confidant network is linked to increases in reports of social isolation shortly following the outbreak of the COVID-19 pandemic (Bierman and Schieman 2020). As a relative comparison to another large-scale crisis, personal social networks were identified as the most important source providing psychological, financial, and social support after Hurricane Katrina (Forgette et al. 2009), suggesting that declines in social confidants would have potent consequences for loneliness during the pandemic. This argument is supported by additional research conducted during the pandemic that has shown that people with low numbers of network confidants tended to report increases in loneliness (Kovacs et al. 2021). By extension, the likely increasing importance of reliance on social support networks during the pandemic, paired with the losses of these very same support networks, could lead to notable increases in loneliness that in turn undermine self-rated health.
Methods
Data
The data analyzed in the present study are the Canadian Quality of Work and Economic Life Study (C-QWELS). The baseline C-QWELS data used in the current research are a part of a Canadian national study intended to examine social conditions and well-being among Canadians who were currently employed. Data were gathered by the study authors in cooperation with the Angus Reid Forum, a Canadian national survey research firm that maintains an ongoing national panel of Canadian respondents. The baseline data used in this survey were gathered from March 17 to March 23, 2020, using an online survey of 2,528 working Canadians. The response rate was 43 percent, and results were statistically weighted according to the most current education, age, gender, and region Census data to ensure a sample representative of working Canadians. Subsequently, 44 respondents were removed because they were not working at the time of the survey, reducing the sample size to 2,484; another 28 respondents were removed because they preferred to self-describe their own gender, and this was too small of a response size to analyze as a separate category, resulting in a final sample size of 2,456. An attempt was made to recontact these respondents using a similar online survey that was administered from May 17 to May 23, 2020, resulting in a sample of 1,854 respondents (a retention rate of 75.5 percent). The timing of the first wave of data was during the early stages of the pandemic when social distancing measures had recently been put in place. Thus, change between March and May is specific to the changing nature of experiences during the pandemic, rather than change from prior to the pandemic to during the pandemic.
Focal Measures
Self-rated health
Our dependent variable—perceptions of health as indicated by self-rated health—was measured with a frequently used survey question which asked, “Overall, how would you describe your current state of health?” with response categories of (1) “Excellent,” (2) “Very good,” (3) “Good,” (4) “Fair,” (5) “Poor,” and (6) “Very Poor.” As a low number of respondents indicated “Very Poor,” responses to “Poor” and “Very Poor” were combined, creating a five-level variable; responses were reverse-coded so that higher values indicated better perceptions of health.
Loneliness
The measure of loneliness was adapted from a validated three-item scale designed to assess loneliness in surveys (Hughes et al. 2004). Respondents were asked, “In the past month, how often did you . . . ?” (1) “feel like you lacked companionship”; (2) “feel left out”; and (3) “feel isolated from other people.” Responses were coded on a scale of 1 (“none of the time”) to 5 (“all of the time”). The mean of the three items at each wave was used as the indicator of loneliness (Cronbach’s alpha of 0.80 in March and 0.81 in May).
Social network confidants
The measure of the number of social network confidants was adapted from the European Social Survey (ESS) and has been validated as a measure of close social network size (Bearman and Parigi 2004) and as a predictor of loneliness (Swader 2019). The measure specifically asks about the extent of one’s supportive social network, thereby reflecting channels through which perceived and embedded support can flow. Respondents were asked, “How many people, if any, are there with whom you can discuss intimate and personal matters?” with responses of None, 1, 2, 3, 4–6, 7–9, and 10 or more. To create a measure with more evenly distributed categories and avoid the influence of outliers, responses to the top two categories were combined, creating a five-level measure with the top category of 7 or more.
Control Measures
Control measures focused on prominent demographic determinants of social relationships and health. Age was measured in years and coded where individuals aged 18–29 were compared to categories of 30–39, 40–49, 50–64, and 65+. Gender was coded as 0 = men, 1 = women. As is common in Canadian research (Little 2016), racial and ethnicity minority status was measured by a dichotomous variable in which the higher value indicated a “visible minority.” Education was operationalized as a set of categories, in which individuals with a university degree were compared with categories of high school degree, some college/trade school/university, and college/trade school; less than 2 percent of weighted sample had less than a high school degree, and these respondents were grouped with those with a high school degree. Income was measured as a set of categories in which $150,000 or more in household income was compared to less than $25,000, $25,000 to less than $50,000, $50,000 to less than $100,000, and $100,000 to less than $150,000. Those missing reports of income was considered as an additional analytic category. We control for the presence of additional individuals in the home with an indicator of not living with a romantic partner (0 = does not live with a partner, 1 = lives with partner), and additional measure of the number of people in household other than the respondents (with a value of 0 indicating that the respondent lives alone and a top value of 5 or more additional people). Furthermore, because baseline data focused on a working sample, we controlled for baseline work statuses with a set of dichotomous variables in which business owners or the self-employed were compared with part-time and full-time workers who were employed by others. Weighted sample descriptives are provided in Table 1.
Weighted Sample Means (N = 2,456).
Methods of Analysis
Our primary means of analysis in the current research is sequential latent change score (LCS) analysis (Grimm, Ram, and Estabrook 2017). Our basic LCS model is depicted in Figure 2. The LCS model estimates two primary parameters of interest. The first is mean baseline levels of an outcome, which is represented by the mean of an intercept factor, and the second is the mean change in the outcome over time, which is represented by the mean of a change factor. A random disturbance term, denoted by “D,” affords interindividual variation at baseline. By allowing the random error terms for the intercept and change factor to be correlated, the LCS model explicitly takes into account the degree to which baseline levels of an outcome are correlated with degree of change over time available for each case, thereby accounting for sample attrition (Enders 2010).
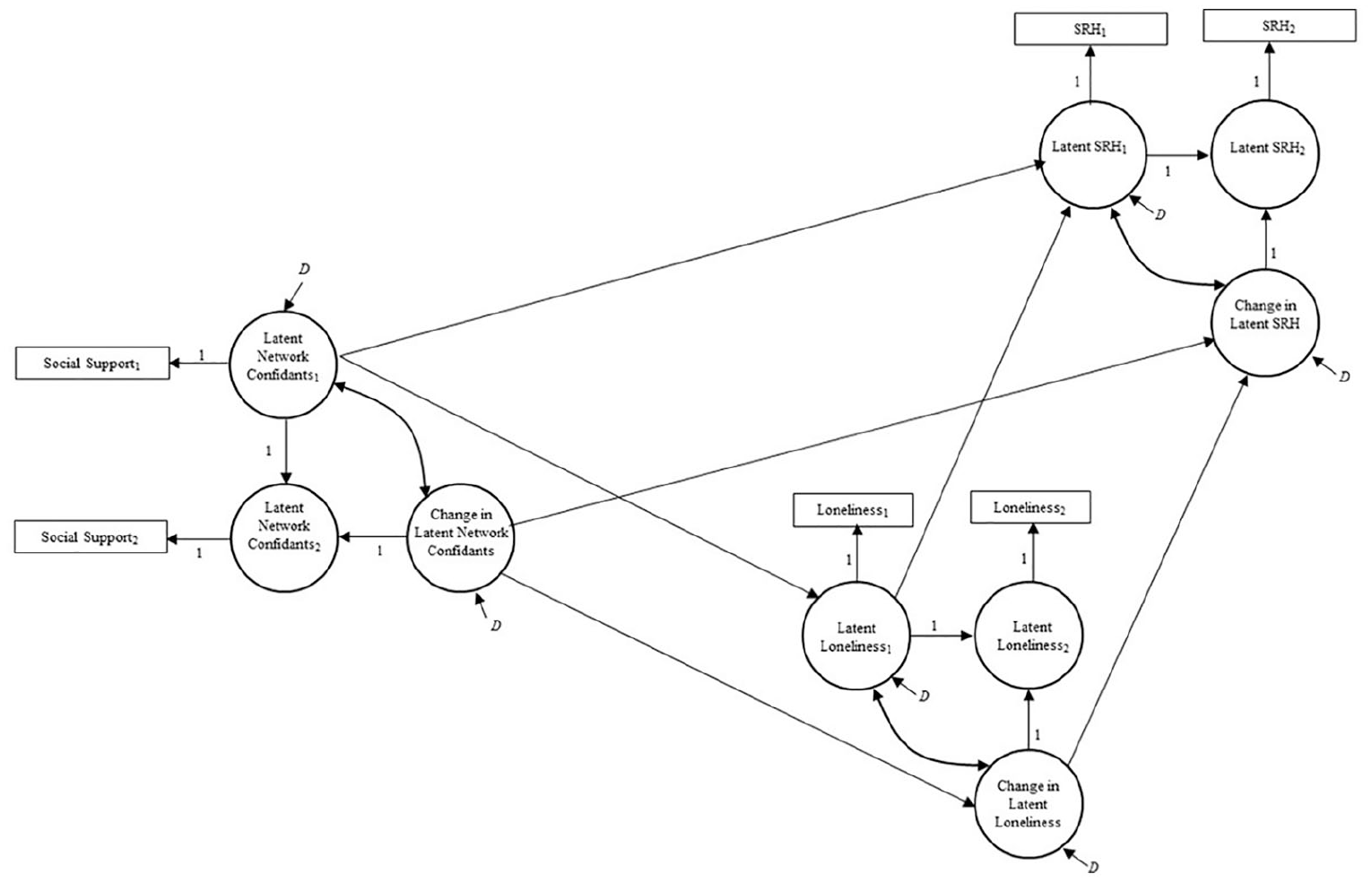
Sequential latent change score model of social network confidants, loneliness, and self-rated health during the COVID-19 pandemic.
Because the LCS model is estimated through structural equation modeling (SEM), LCS models can be estimated for multiple outcomes within the same model. As a result, as shown in Figure 2, baseline loneliness can be modeled as influenced by baseline number of social network confidants, while baseline self-rated health can be modeled as influenced by both baseline number of social network confidants and loneliness. Similarly, change in loneliness can be modeled as influenced by change in social network confidants, and change in self-rated health can be modeled as influenced by change in social network confidants and loneliness. The indirect pathways between network confidants and health can therefore be estimated as ab, which is the product of the association between the number of social network confidants and loneliness (a) and the association between loneliness and heath (b) (MacKinnon 2008).
All models are estimated using Mplus 8.3, and we display both metric and standardized coefficients. We also employ the maximum likelihood-robust estimation method that provides robust corrections for nonnormality and has been shown to produce suitable estimates of latent variables when indicators contain at least five response categories (Rhemtulla, Brosseau-Liard, and Savalei 2012). Full-information maximum likelihood (FIML) is used to address missing data, thereby accounting for sample attrition (Enders 2010). In testing indirect effects, we use bias-corrected bootstrapping, based on 5,000 bootstrap samples.
Results
Descriptive Statistics
Since we were interested in predicting changes in self-rated health—particularly declines in self-rated health—we first observe that roughly 27 percent of our analytic sample declined in self-rated health. Of those who experienced decreased self-rated health, 3 percent declined from fair to poor, 16 percent decreased from good to fair or poor, 47 percent decreased from very good to good, fair, or poor, with the majority (44 percent) decreasing from self-ratings of very good to good health. And 34 percent decreased from excellent health to a lower self-rated health category between March and May. Taken together, these patterns show marked changes in perceptions of health in such a short period of time—and that declines in perceptions of health were occurring at the middle and upper ends of the distribution of self-rated health scores.
Univariate LCS Analyses
Moving into our SEM analyses, as shown in Table 2, we estimated “empty” LCS models that did not contain predictors. These models provide estimates of baseline levels and mean changes in social network confidants, loneliness, and self-rated health, prior to examining the interrelationships between these three measures. The results for social network confidants show a mean number of confidants at baseline of 3.769 and a significant mean decrease in social network confidants of −0.435 over the course of the pandemic under study. Social network confidants therefore contracted over the course of the study. The variances of the disturbances for both factors are significant, though, indicating a significant degree of interindividual variation in the degree of change in network confidants.
Univariate LCS Models of Social Support, Loneliness, and Self-Rated Health (N = 2,456).
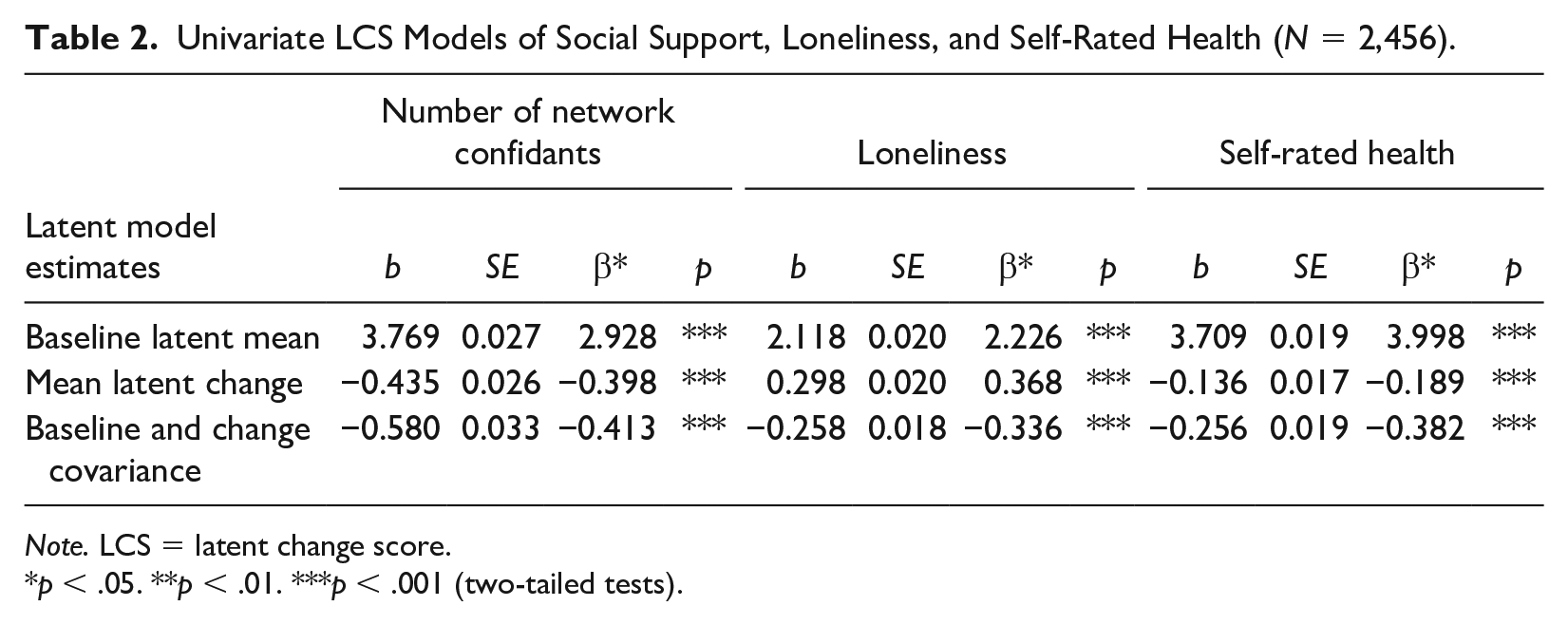
Note. LCS = latent change score.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
The empty model estimates for loneliness show a similar pattern. Mean loneliness at baseline is 2.118, and there is a significant mean increase in loneliness of 0.298. Loneliness therefore increased during the two-month study period. The factor variances for loneliness are also significant, though, indicating significant interindividual variation in increases in loneliness.
Given declines in the reported number of social network confidants and loneliness, we would expect to see commensurate decreases in health. The results for self-rated health support this expectation. The empty model indicates that mean self-rated health was 3.709 at baseline, and self-rated health decreased significantly over the course of the study, with a mean of −0.136. Taken together, these patterns indicate that a decrease in network confidants and an increase in loneliness were leading to declines in self-rated health. To investigate further, we next turn to the sequential LCS analyses that examine the interrelationships between these factors.
Figure 3 depicts these associations in a final LCS model, while Table 3 displays the results for the associations for all demographic controls. Focusing first on the baseline measures, we see support for the hypothesized framework of interrelationships. Baseline loneliness is significantly and inversely associated with baseline self-rated health with a standardized association of −0.217. The baseline number of social network confidants is also significantly associated with higher levels of loneliness. The indirect effect of social network confidants on self-rated health through loneliness was significant (ab = 0.033, p < 0.01). Furthermore, since the direct association between the baseline network confidants and baseline health is not significant, this is a case of “total mediation,” in which baseline loneliness entirely explains the association between baseline network confidants and baseline self-rated health (MacKinnon 2008).
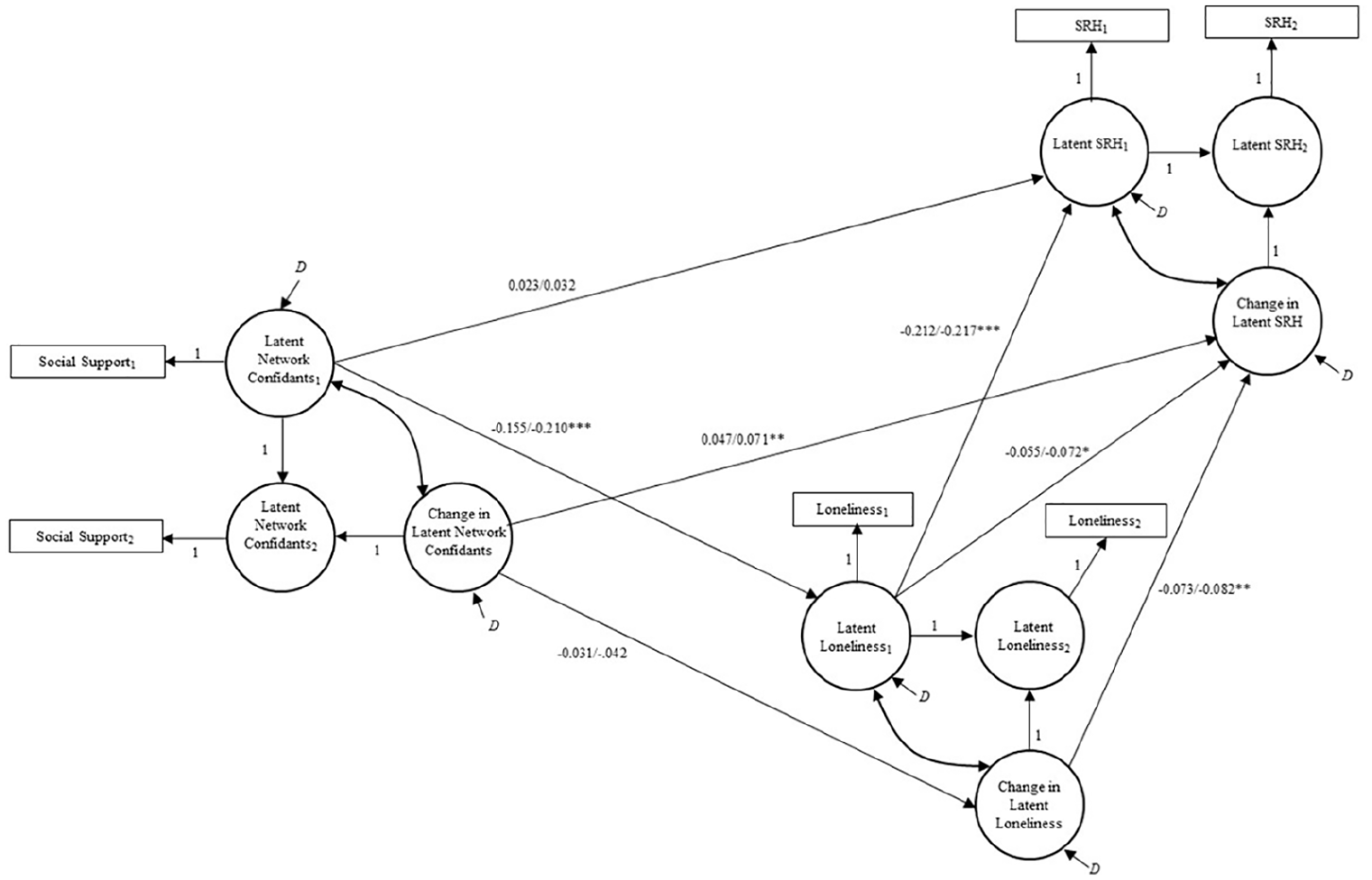
Results of latent change score model of social network confidants, loneliness, and self-rated health.
Relationships with Control Variables in Sequential LCS Model of Social Support, Loneliness, and Self-Rated Health (N = 2,456).
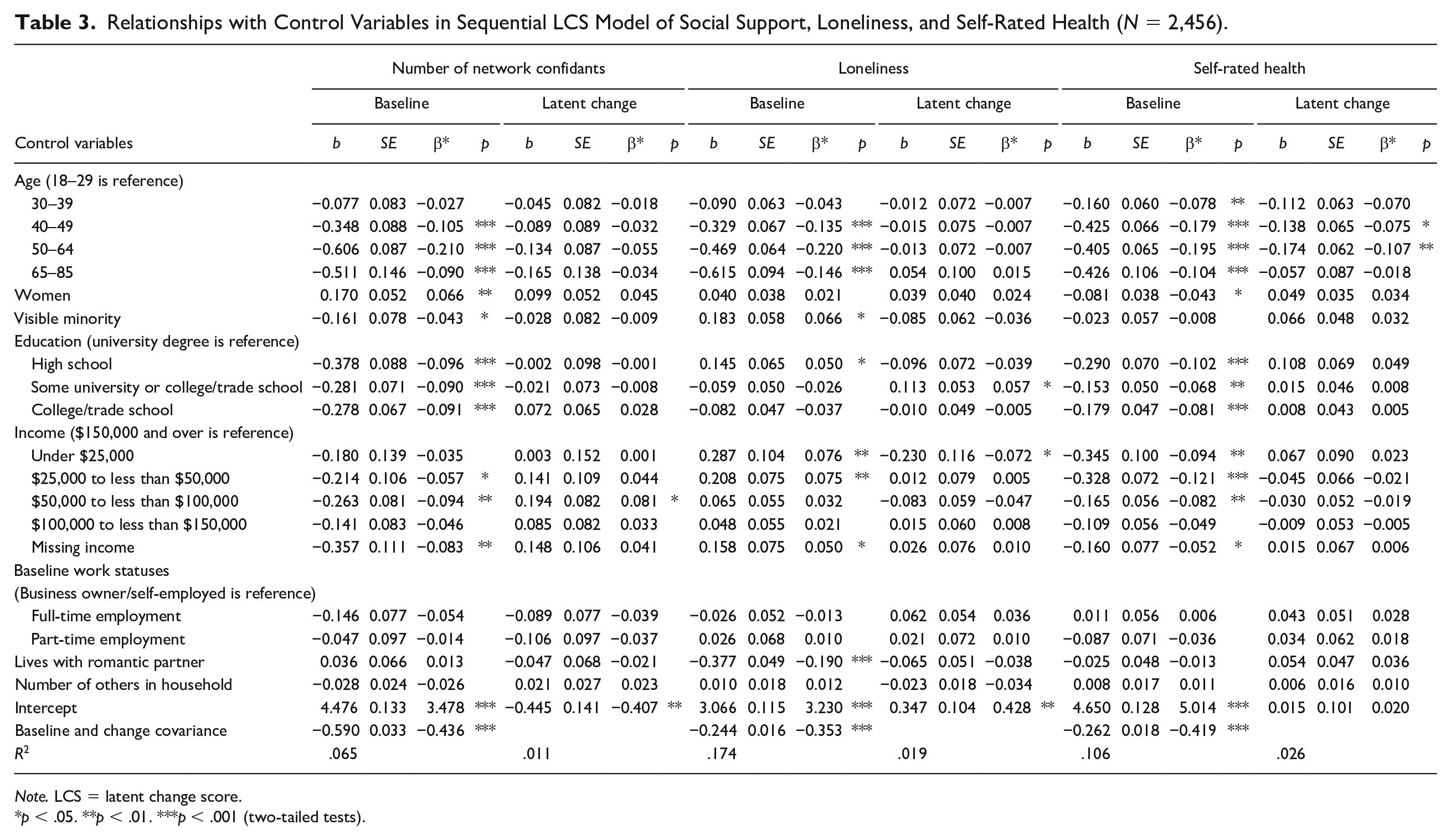
Note. LCS = latent change score.
p < .05. **p < .01. ***p < .001 (two-tailed tests).
Focusing next on the analyses of change, we see that changes in the number of social network confidants are not significantly associated with changes in loneliness. A lack of association between the two measures of change is unexpected, but likely reflects the degree to which there was a large-scale upward shift in a sense of isolation in the population that occurred irrespective of social network confidants. Contractions in social network members during the pandemic were significantly associated with declines in self-rated health ratings. Independent of changes in network confidants, change in loneliness was also significantly and negatively associated with declines in self-rated health. Furthermore, baseline loneliness is also negatively associated with change in self-rated health. Thus, even when we take the population increase in loneliness into account, we see that individuals who were lonelier on the eve of the pandemic were more susceptible to declining health as the pandemic progressed.
Discussion
The onset of the COVID-19 pandemic resulted in large-scale social distancing measures that required the cessation or diminution of social interactions. These measures were necessary for slowing the spread of the virus, but they also raised concerns about the adverse health effects of decreased social contact. The results of our research support these concerns. Although our initial survey occurred shortly after wide-spread social distancing measures were implemented, we observe declines in the number of social network confidants reported and increases in loneliness during the short two-month period. We also find that changes in both the number of social network confidants and loneliness contributed to explaining the decrease in self-rated health.
Prior research has documented the adverse consequences of loneliness for health, and scholars have suggested that North America is in the grip of an epidemic of loneliness (Jeste et al. 2020). The current study contributes to this body of work in two ways. First, it shows that, during the COVID-19 pandemic, there was an exacerbation of this putative loneliness epidemic. Whether or not the increase in loneliness persists or has long-term effects on well-being remains to be seen, but our findings indicate that loneliness accompanied the COVID-19 pandemic. Second, we observed that declines in social network confidants and increases in loneliness were each associated with declines in self-rated health during the pandemic.
Speaking first to the effects of loneliness, the declines in self-rated health resulting from loneliness are likely indicative of decrements in daily physical and mental functioning during the pandemic (Bjorner, Fayers, and Idler 2005; Mavaddat et al. 2011). Moreover, self-rated health has been shown to capture short-term and preclinical health problems (Caetano et al. 2013), as well as an increased risk of mortality (DeSalvo et al. 2006). Since loneliness is an evaluative construct that reflects individual’s assessment of social relationships failing to meet their needs (Hughes et al. 2004), it is not surprising that these effects would be observed at the outset of the COVID-19 pandemic. As the pandemic continues, however, additional attention should be afforded to the contribution of loneliness to any further health risks. In particular, if social reconnection with others does not occur once the pandemic reaches an end, insights from the evolutionary theory of loneliness suggest that these socially adrift individuals will be at a higher risk of further health physical declines due to persistent loneliness (Cacioppo and Hawkley 2009; Cacioppo et al. 2006).
It is also notable that people who started off lonelier on the eve of the pandemic ended up experiencing worse health regardless of how their loneliness changed over the first two months of the pandemic. This finding coheres with previous research showing that baseline levels of loneliness are associated with subsequent changes in health (Luo et al. 2012). Yet, that we observe this influence over only a two-month period suggests that the initial months of the COVID-19 pandemic composed a period of heightened vulnerability for population health during this crisis. Prior research demonstrates that self-rated health is reflective of stress responses (Leshem-Rubinow et al. 2015), and as people experienced a loss of social resources due to social distancing, they were likely more vulnerable to preexisting social stressors. Subsequent research into the health effects of the COVID-19 response should take care to consider how antecedent stressful conditions may have had further health effects due to increased vulnerabilities (and worse health perceptions) brought on by social distancing measures. For instance, groups that typically experience a greater degree of stress, such as minority groups, those of a lower socioeconomic status, and people with preexisting health conditions have been found to fare worse during the pandemic (e.g., Bierman et al. 2021; Hooper, Nápoles, and Pérez-Stable 2020; Stein and Ometa 2020 Wyper et al. 2020), and we may see this trend continue the longer social distancing protocols are in place.
As for social network conduits, at baseline, the consequences of having fewer social network conduits to discuss intimate matters with for loneliness entirely explained its association with perceptions of health at baseline. However, changes in social network confidants were not associated with changes in loneliness, resulting in independent effects on changes in perceptions of self-rated health. In other words, the lack of social network confidants prior to the COVID-19 pandemic may have worn on people and accrued into feelings of loneliness prior to the pandemic, in turn creating adverse indirect associations with perceptions of health at baseline. Yet, we found no evidence for this indirect association when it came to changes experienced specifically during the pandemic. Still, individuals who lost network confidants during the first two months of the pandemic also experienced a decline in self-rated health, suggesting other channels besides the evaluative component of loneliness as the satisfaction with relationship intimacy. It is possible that decreased network size led to additional problems coping during the pandemic, or reduced social trust which was also likely to be especially important during the increased threats raised by the pandemic. Declines in social trust may have been especially important as an explanatory mechanism, as recent research suggests that social trust declined in the wake of the pandemic, incurring detriments to well-being.
Policy Implications
The COVID-19 pandemic generated sweeping transformations in social interactions in a short period of time. Prior to the pandemic, many scholars had already expressed deep concerns about pervasive feelings of loneliness in North American society. The social distancing measures linked to the pandemic likely exacerbated these dynamics. Given this predicament, we suggest several policy implications that could follow from our findings.
Our research suggests that the establishment of stay-at-home and social distancing measures should include efforts to translate, evolve, and apply established practices to combat the loss of social network confidants and loneliness. Some potential strategies to address the loss of social connection could include the integration of brief and interactive screening tools for clinicians and health professionals to identify and make service referrals for those experiencing the adverse effects of social disconnection (de Oliveira Neto et al. 2020). Moreover, concomitant with these efforts should be concerted activities which make digital resources available for virtual counseling or telemedicine, especially in disadvantaged and underserved communities. Declines in health may become more apparent in the progression of the pandemic, necessitating greater access to remote medical care which would minimize the risk of virus transmission while still permitting greater access to medical care. Also providing access to remote-led exercise classes and other forms of physical activity promotion would further help to combat negative effects on population health.
More broadly, we turn our attention to programmatic ways of combatting social isolation beyond medical. We suggest an organized efforts to engage individuals in volunteer efforts to provide online support for others. We essentially suggest a national service corp dedicated to involving individuals in the battle against isolation. This could involve support forums, as well as the organization of social connections in which individuals could provide one-to-one support, as well as more basic opportunities for social interactions. Notably, providing these opportunities may have as much impact for people who volunteer to provide these services as those who receive them by instilling a sense of mattering in individuals that would counter-balance deleterious effects of declining social networks of confidants. Funds could also be allocated as part of a national campaign to nonprofits or community-based organizations to enhance social connections and engagement as we begin to emerge from the pandemic and reestablish social bonds.
We are especially concerned about the state of social connection following the pandemic. We especially suggest national monitoring efforts of the degree to which the pandemic may have created a “scarring” effect, in which social connection may not rebound after the pandemic. Evidence of a scarring effect would suggest the need for greater attention from a policy perspective for programmatic efforts to bolster individual social connections. In our view, “getting back to normal” will also encompass a careful recognition of the toll that social isolation exacted on individuals since the outset of the pandemic, and concentrated efforts to reconnect people once it is safe to do so. Community engagement events and municipal funding of grassroots organization that can help facilitate local community will especially be critical public investments in combatting long-term social isolation.
Limitations
A few limitations of our study deserve mention. First, we note that our results may be limited in their generalizability because participants were recruited online. This may lead to conservative estimates of the relationship between loneliness and health, however, because all of our respondents had some access to technology and could conceivably connect with close others once in-person gatherings were suspended. Second, our results may only be generalizable to the North American (Canadian) context, or other social contexts where social distancing measures could be practically implemented. In nations in which large-scale working from home, high population density, or extensive familial co-residence, the patterns we observe are likely to be less applicable.
Conclusion
Altogether, the results of our study suggest that social disconnection and loneliness is a major public health issue and that remaining “socially distant” can paradoxically be both protective and harmful to people. These measures can be protective in terms of helping to curb transmission of the virus, but harmful through consequences for social isolation and loneliness. The fundamental human need for social connection is greatest in times of adverse situations and events. Although social distancing requirements may continue to be necessary to curtail the spread of the virus, they will also tend to leave people desiring social connection. Bereft of this connection, we are likely to see residual health consequences at the population level beyond those related to the contraction of the coronavirus.
Footnotes
Authors’ Note
Alex Bierman and Laura Upenieks are co-first authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of Toronto COVID-19 Action Initiative 2020 (Fund # 508813) and Tri-Council Bridge funding supports this research (Scott Schieman, PI).