
Abstract
The aim of this study was to pinpoint the subcultural variations in Kuwaiti society that contribute to the spread of the coronavirus. Additionally, this study sought to identify which social activities (SAs) are most likely to contribute to the virus’ propagation. Using an opportunistic sampling technique, 3,736 Kuwaiti respondents from all six governorates in Kuwait were selected. An electronic questionnaire was used. It included social and demographic variables, respondents’ background (Urban/Bedouin), and creed (Muslim Sunni/Muslim Shiite). Some scales were used: SA, HCCS, SCES, and SCS. SPSS was used. The main statistical techniques employed in SPSS were ANOVA, t-tests, chi-square, and linear regression. The data indicate that the most frequent sources responsible for transmitting infection have come from family members in households and marriage activities. Significant differences among education, age, gender, and place of living in SA, HCCS, CSES, and SCS were found. Significant differences were found between participants with Urban and Bedouin roots and Sunni and Shiite Muslims in HCCS, SCES, and SCS. Data showed significant differences between social groups in some of their living conditions. Findings demonstrate the significant influence of an individual’s social behavior and cultural values on interactions during the COVID-19 pandemic. Health issues are impacted by cultural variations in social distances between social groups.
Introduction
The impact of the COVID-19 pandemic exceeds its effects on individuals’ physical and mental health. The COVID-19 pandemic has impacted behavioral norms and cultural attitudes worldwide. Due to the person-to-person transmission of the SARS-CoV-2 virus through droplets, mainly occurring via close physical and interpersonal contact, health organizations implemented several restrictions to control the virus outbreak (Jin et al., 2020). These health measures followed World Health Organization (WHO) recommendations, such as social distancing, wearing face masks, and using antiseptics and gloves to minimize the risk of contracting COVID-19 (WHO, 2021). Since the emergence of the COVID-19 pandemic, cross-cultural research has been conducted worldwide to examine its impact on individuals’ mental health, well-being, economic crises, educational performance, and lifestyle behaviors (Cavanaugh et al., 2023; Hassan et al., 2023; Naseer et al., 2023; Rehman & Ahmad, 2023; Zhang et al., 2023). Previous studies have found a significant impact of the pandemic on individuals’ daily lifestyle habits, social interactions, and interpersonal contact (McGrail et al., 2020; Pedersen & Favero, 2020; Sorokowska et al., 2022).
In an attempt to explain human behavior within certain cultural groups, the theory of cultural models of behavior was developed. It is regarded as a theoretical framework that may be applied to understand how individuals mold their ideas and actions. This framework is related to the notion that culture is made up of common meanings that explain how people in a society view and react to their surroundings (Holland & Quinn, 1987).
As evidenced by studies conducted during the COVID-19 epidemic, the idea contends that cultural factors have a role in the problem of social distancing. According to one study, a society’s nature can be classified as either collectivistic or individualistic. A study conducted on the US, Australia, and 79 other countries, collectivistic cultures were more dedicated to adhering to social distancing laws and guidelines during the pandemic, while individualistic societies were more inclined to violate them. The researchers speculate that this phenomenon might be caused by social ideals emphasizing a sense of social obligation (Feng et al., 2023).
Furthermore, a society’s social norms have a big influence on how people behave. Adherence tends to increase and social distancing techniques become embedded in moral principles and a community’s collective identity when clear and explicit standards are established. Social distancing behaviors and adherence to associated rules are more likely to be consistently displayed by societies that actively support and able to maintain such social values. (Hagger et al., 2020; Mercer & Mollborn, 2023). In addition, it is found that societies with lower levels of uncertainty avoidance tend to delay compliance with social distancing measures. In contrast, those with strong uncertainty avoidance adopted social distancing more rapidly, reflecting a cultural preference for structured and organized crisis responses (Nair et al., 2022). The theory of cultural models offers a framework for understanding the extent to which individuals comply with and adhere to social distancing measures. It also allows for meaningful comparisons between human cultures based on these behavioral responses.
Culture, Perceptions and Attitudes Toward Diseases
The most well-known definition of culture in literature comes from Tylor (1871), who defined it as the “complex whole” that consists of knowledge, beliefs, art, morals, laws, conventions, and other skills and behaviors that people acquire as members of society (P:1). Some anthropologists focus on culture as a learned and shared idea (Lyman, 2008), whereas others emphasize culture as “shared knowledge and values” (Seidler, 2010). Additionally, some people use culture as a means of expressing themselves through modern conceptions of symbols (Peterson, 1979). Based on many cross-cultural studies (Kahissay et al., 2017; Workneh et al., 2018), population perceptions and attitudes toward unknown diseases, new epidemics, and pandemics are strongly related to their cultural beliefs and attitudes. Depending on their cultural concepts of such diseases, certain modes of medication or treatment are more likely to be accepted and adopted, different explanations and symptoms will be recognized, and infected individuals may be stigmatized.
Napier et al. (2014) addressed how society can succeed in constraining the outbreak of any disease or pandemic if the decision-makers of health institutions consider the local population’s cultural perceptions and concepts toward the disease. Bruns et al. (2020) explored the cultural aspect of interpersonal distance during the COVID-19 pandemic, highlighting how it might cause negative feelings of neglect among affected populations and lead to stigmatization. Proper public health interventions must be aligned with the cultural perceptions of the disease to avoid any negative feelings toward the treatment or infected individuals. Velamoor and Persad (2020) reviewed the COVID-19 pandemic from a cultural perspective and stated that populations worldwide have different responses, coping behaviors, and beliefs based on their cultural orientations and values. As an example, people who live in cultures that value individualism tend to favor and choose an independent approach in their daily practices, unlike those who grow up in societies that value collectivism (De Vaus et al., 2018; Markus & Kitayama, 1991). The following studies (Allcott et al., 2020; Harper et al., 2021; Wise et al., 2021) revealed several factors that lead people to adopt precautionary health regulations to avoid SARS-CoV-2 contamination, such as the source of health information about the virus’ mode of transmission and individuals’ cultural beliefs.
During the COVID-19 pandemic, the WHO recommended maintaining a social distance of at least 1 m between individuals to lower the probability of contracting the SARS-CoV-2 virus (Chu et al., 2020; WHO, 2021). Thiebaut et al. (2021) noted that people’s social interactions, such as interpersonal touch behaviors, changed after the onset of the COVID-19 pandemic. People prefer to interact verbally rather than physically, especially those who are highly vulnerable to disease, due to social responsibility and the desire not to make others sick with the virus. Sorokowska et al. (2017) demonstrated that as part of daily social interactions, the range of interpersonal distance varies depending on culture, social relationships, and personality. Hall (1966) found that the range of interpersonal distance between two or more individuals depends on their feeling of comfort, which can vary based on the context, blood relation, or acquaintances. As an example, in non-intimate contexts, the interpersonal distance between individuals can range from 0.46 to 3.7 m, compared to a lesser distance for family or close friends. Sorokowska et al. (2017) found that the mean distance between individuals is determined based on the relationship, with 0.32 m for close friends, 0.92 m for acquaintances, and 1.35 m for strangers.
Culture and Method of Greeting
Globally, there are different types of intercultural welcomes, mainly formed by society’s culture. In many cultures, greeting styles are not only expressions of politeness but also symbolic of deeper social values such as humility, respect, or status (Fergusons, 1981; Liu, 2016; Schottman, 1995; Toshmatov & Niyozmatova, 2024). As an important function in human communication, greetings serve multiple important meanings, greeting act as a social lubricant it helps “break the ice” and set a positive tone for initiating conversation with others. Additionally, greetings symbolize respect by acknowledging the other person’s presence and demonstrating an interest in engaging them in conversation. Finally, greetings are deeply immersed in cultural norms and social etiquette. Using an appropriate form of greeting in each cultural context demonstrates cultural awareness and sensitivity, showing that one respects local traditions and social expectations (Al-Qinai, 2011; Toshmatov & Niyozmatova, 2024).
As a type of greeting, Zhu (2013, p. 52) defines handshaking as a polite act when people are welcoming each other and it differs across cultures. For instance, in China, it is more appropriate and acceptable to handshake others softly, whereas in the United States, it is more predictable and respectful to handshake others firmly. In addition, Zhu (2013, p. 53) notes that in Thailand, to signify humbleness, people press their palms together in a prayer-like gesture (the wai), while in Japan, people bow to each other to express formality and respect. Similarly, greeting customs in the Arab world are steeped in religious, cultural, and social tradition.
Moreover, Al-Qaderi et al. (2017) conducted a study among four participants from four different cultures (Yemeni, Chinese, Turkish and Polish) to examine the influence of each culture on individuals’ behavior practice by comparing 15 selected paralanguage features. The study identified these paralanguage features, which include attitude, performance, and reaction toward each. Findings of the study reveal that paralanguage features that were alike among these four cultures were nodding, eye contact, yawning, and knocking on the door, whereas the main dissimilarities were in greetings, waving goodbye, and handshaking. Among these four cultures, handshaking differed according to gender, setting, and intimacy with the other person. In Yemeni, Polish, and Turkish cultures, handshaking is common among males only. Whereas in a business setting; handshaking is common and acceptable for both males and females among these four cultures. In Chinese culture, handshaking is common only with strangers.
In Muslim countries, Islam influences many greeting customs; for instance, it is considered inappropriate for a strange man to shake hands with a woman, and similarly, Muslim women typically do not shake hands with strange men. Exchanging common verbal greeting, such as “As-salāmu ‘alaykum” (“peace be upon you”), between common and stranger people in Muslim countries is considered as a polite and welcoming response (Al-Qinai, 2011; Hudson, 1996; Khalaf, 2016). After reviewing related literature on greetings in both English and Arabic, it is evident that Arabic greeting formulas are generally more elaborate than their English counterparts. This distinction can be attributed to differences in social customs, cultural traditions, and religious values. Arabic greetings are deeply embedded in Islamic principles, particularly the concept of “al-radd bi-mithlih aw afdal” (the same or better response), which encourages reciprocating a greeting with one that is equal or more gracious. For instance, when greeted with “As-salāmu ‘alaykum” (“peace be upon you”), the socially and religiously appropriate response is “Wa ‘alaykum as-salām wa raḥmatullāhi wa barakātuh” (“and upon you be peace, and the mercy and blessings of Allah”). This religious component makes Arabic greetings not only a social ritual but also a spiritual one, reinforcing communal harmony and respect. In contrast, English greetings tend to be shorter and less formal, often lacking the layered religious and cultural meaning found in Arabic expressions (Bouchara & Qorchi, 2016; Khalaf, 2016).
Culture and Physical Greetings
Proximity, or interpersonal distance, refers to the physical space individuals maintain between themselves during interactions. If the distance between speakers feels too close or too far, it may convoy implicit information about their relationship and cause discomfort, prompting individuals to adjust their position to reestablish a comfortable communication zone based on their cultural norms, comfort levels, and social expectations. A closer distance often indicates familiarity, affection, or a desire for intimacy, while a greater distance may suggest formality, unfamiliarity, or emotional detachment (Kim et al., 2009). For example, in Arabic culture, same-gender friends or relatives may greet each other with gentle handshakes, cheek kisses, or even a hand placed over the heart to show sincerity and warmth. In conservative settings, in Eastern countries such as China, especially between unrelated men and women, verbal greetings and non-contact gestures are used out of respect for cultural norms surrounding modesty (Zhu, 2013, p. 54). Sorokowska et al. (2017) observed cultural differences in physical distance during social interactions between Europeans and North Americans. Southern Europeans tend to maintain closer interpersonal distances compared to North Americans and Northern Europeans.
COVID-19 Pandemic and Modes of Greeting
During the COVID-19 pandemic, some modes of greeting had a significant negative impact on individuals’ health due to the rapid transmission of the virus through extremely close interpersonal distance, such as kissing on the cheek or nose-to-nose greetings. In different cultures, greetings vary, some people shake hands, while others kiss each other on the face or nose-to-nose, and still others through bowing. Thus, many health recommendations and regulations during the pandemic recommended avoiding these close-contact greetings and replacing them with verbal greetings (Bruns et al., 2020).
A study in Japan conducted by Suppasri et al. (2021) among 600 individuals during the COVID-19 pandemic demonstrates the role of cultural behavior in minimizing the impact of the outbreak. The findings of the study illustrate that frequently washing hands was already a regular habit among Japanese people before the COVID-19 pandemic, with 70% of participants reporting this practice, these findings contrast with the higher rate of positive cases in the U.S. and Europe. Additionally, more than one-third of participants stated that they take off their shoes upon entering their homes. Regarding interpersonal touch behaviors and expressions of affection, such as hugging, shaking hands, and kissing, approximately 70% of participants reported that they did not engage in these behaviors before the pandemic. Yezli and Khan (2020) presented another example of how the COVID-19 pandemic radically altered the social lifestyle behaviors and cultural norms of the Saudi population, which values social gatherings and physical greetings such as kissing on the cheek. Several public health regulations were enforced, including social distancing, partial curfews, preventing physical greetings, and wearing masks when gathering.
Kuwait and COVID-19
Once the first confirmed case of COVID-19 was reported in Kuwait on February 23, 2020, several health regulations were imposed by the Kuwaiti public health authority to constrain the spread of the virus. These regulations required physical and social distancing due to the rapid dissemination dynamics of COVID-19. Many countries worldwide enforced various regulations, such as quarantine or partial and complete curfews (Iacobucci, 2020; Paules et al., 2020; Velavan & Meyer, 2020). In Kuwait, from March 2020 to May 2020, the Kuwaiti Ministry of Health imposed a partial and complete lockdown. During this time, people’s daily schedules were radically altered due to the closure of schools, workplaces, malls, houses of worship, and parks.
Numerous studies have been conducted from various perspectives to examine the impact of COVID-19 pandemic in Kuwait on individuals’ psychological wellness and mental health (H. Al-Ma’Seb & Al-Sejari, 2022; Alsairafi et al., 2021; Al-Sejari & Al-Kandari, 2022; Al-Kazi et al., 2021), household and family activities during the partial lockdown (Al-Kazi et al., 2021), and precautionary health behaviors (Al-Sejari & Al-Ma’Seb, 2021, 2022).
Two significant factors – religious sectarian affiliation and ancestry – have a significant impact on the various subcultures that comprise Kuwaiti society. The population is descended from either Urban populations, who historically lived in coastal and agricultural areas or tribal Bedouin roots that historically inhabited desert regions. The majority of Kuwaitis are Muslims, and they live side by side with a tiny Christian minority comprising less than 1% of the population. There are two main Muslim sects: Sunni and Shiite.
Numerous sociological and ethnographic studies have examined the cultural and even health-related differences between various social groups. These studies have specifically observed Disparities in life-cycle rituals, such as marriage, birth, and funeral practices, which are closely related to human life stages and act as indicators of cultural variety (Al-Kandari, 2008; Al-Zaben, 1994; Oudah, 1988; Sabieh, 1980). Given their emphasis on direct face-to-face contact during communal gatherings, these practices have consequences for behaviors connected to social distancing and are intimately tied to patterns of social interaction.
Moreover, Al-Kandari (2010) conducted an ethnographic study that examined the annual events Kuwaiti society and shed light on the cultural differences in social interactions between various groups, particularly between Sunni and Shiite communities. The study noted significant variations in social activities and social gathering customs, such as greetings, hugging, kissing, nose-touching (a customary gesture), and physical closeness. In situations where physical distance is necessary, these cultural manifestations of intimacy may present challenges. However, the survey also highlighted the presence of common traditions and practices that bring Kuwaitis together during significant social and sectarian gatherings.
The aim of this study was to pinpoint the subcultural variations in Kuwaiti society that contribute to the spread of the coronavirus. Additionally, this study sought to identify which social activities (SAs) are most likely to contribute to the virus’ propagation. The study focused on the role of social distancing in this context. This study aimed to identify potential social factors responsible for the spread of COVID-19 in Kuwaiti culture, examine differences among sociodemographic variables, and identify differences between Bedouin, Urban, Sunni Muslim, Shiite, and male/female groups in the Health Conditions Commitment Scale (HCCS), Social Communication Embarrassment Scale (SCES), and Sociocultural Communication Scale (SCS). Our study investigated differences in respondents’ experiences with COVID-19, whether they have been infected by friends or relatives, and the associations between sociocultural variables and HCCS, SCES, and SCS. The study’s hypotheses are:
− There are significant differences among levels of education, governorates, household types, and age categories with the HCCS, Sociocultural Effect of Personal Communication, and SCS.
− There are significant differences among HCCS, SCES, and SCS and their dimensions, as well as the number of family members, rooms, and bedrooms in households within the sample groups (Urban or Bedouin, Sunni or Shiite, and male or female).
− There are significant differences between Urban and Bedouin respondents, as well as between Sunni and Shiite, regarding their own COVID-19 infection, contracting the virus from friends or relatives, and the person expected to have infected them.
− There is significant association between sociocultural factors and HCCS, SCES, and SCS.
Method
Sample
Using an opportunistic sampling technique, 3,736 Kuwaiti respondents aged between 17 and 79 years were selected (M = 31.17; SD = 13.24). Among the participants, 31.4% were male and 67.4% were female. The respondents, who were selected from Kuwait’s six governorates, willingly answered the questionnaire. The respondents’ socioeconomic backgrounds, educational backgrounds, and social groups varied. Online questionnaires were used to attract respondents. After receiving the survey link via email and WhatsApp which is considered as one of the most popular social media platforms, respondents filled it out. The time frame for the study was after the COVID-19 pandemic. The sample was collected, and the study was carried out once life had returned to normal following COVID-19. Participants were asked to recollect noteworthy infections and health incidents associated with the pandemic during this time.
None of the authors of this study had previously conducted any investigations using human subjects. Informed consent was electronically requested at the start of the questionnaire, and participation was completely voluntary. The goal of the study, the anonymity of their answers, and their freedom to discontinue participation at any moment without facing repercussions were all made abundantly evident to the participants. Although participants in the study had to be at least 17 years old, no sensitive or identifying information was gathered. According to ethical guidelines for low-risk, anonymous survey research, participants between the ages of 17 and 20 were deemed competent to supply informed permission. While Kuwait’s legal age of majority is 21, participants in this age group were given ethical protections appropriate to their age and cognitive capacity in accordance with regional research norms. A statement outlining eligibility requirements and consent procedures was provided at the beginning of the survey.
Variables
The primary instrument used in this investigation was an electronic questionnaire. Social and demographic factors included in the questionnaire were age, gender, governorate, economic condition, education level, respondents’ background (Urban/Bedouin), and creed (Muslim Sunni/Muslim Shiite). Additionally, the questionnaire included a list of possible SAs that could spread infection. Household items were requested. Respondents were asked to identify the type of home they owned (e.g., villa or government house), the number of family members living there, the number of rooms and bedrooms, the number of employees living there, and the size of the home. The questionnaire included questions about infections, asking respondents whether they had contracted COVID-19 (yes or no), whether they had been infected by friends or family (yes, no, or maybe), and who had infected them (close relatives, other relatives, friends, or coworkers).
The SA scale includes 36 activities related to social distancing. This scale was created by the Texas Medical Association (TMA), which shows the risk factors during COVID-19. The scale ranges from 1 to 10 and is ranked by physicians from the TMA Committee on Infectious Diseases and the TMA COVID-19 Task Force (Story, 2020). Examples of risk factors include “opening the mail,”“grocery shopping,”“eating at a buffet,”“having dinner at someone else’s house,” and “going to a hair salon or barbershop.” This scale was translated into Arabic by the researcher and used in this study.
Three major scales were used in this study. The HCCS measures a person’s commitment to their health, comprising seven items. Examples include sanitizing hands, washing hands with soap, meeting few people, and practicing social distancing when appropriate. A Likert scale was employed, with “Always” = 5 and “Never” = 1. SCES measures social communication shame, comprising five items. Examples include feeling ashamed for not shaking a friend’s hand, not kissing a friend after a long absence, or not kissing an older person’s head. A Likert scale was employed, ranging from “Strongly agree” = 5 to “Strongly disagree” = 1. SCS measures intercultural communication and includes 11 items. These items encompass actions such as kissing friends, hugging friends, shaking relatives’ hands, and shaking friends’ hands. A Likert scale was employed, ranging from “Strongly agree” = 5 to “Strongly disagree” = 1.
These three measures were used to reveal a set of interpretive meanings. A set of sociocultural variables was used to reveal the differences between them and the three measures. The variables used were education, place of residence, type of home – its components and size – family including its members, age group, and cultural segments of local cultures (Bedouin and Urban, Sunni and Shiite). Furthermore, statistical correlations between these three measures and a set of socio-cultural factors and variables were disclosed.
The validity of these scales was confirmed by six faculty members of the Social Sciences College at Kuwait University. Reliability was assessed using Cronbach’s alpha to ensure the consistency of these scales. All scales showed high consistency, with reliability ratings ranging from 0.84 to 0.95 (HCCS = 0.84; SCES = 0.92; SCS = 0.95).
Statistical Procedures
We entered and analyzed the data using SPSS (version 26). Inferential and descriptive statistical methods were employed, including ranking, mean, standard deviation, and percentages. One-Way ANOVA was used to examine the differences among education levels, governorates, and age categories with the HCCS, SCES, and SCS. In addition, t-tests were used to examine the differences between roots, faith, and gender on HCCS, SCES, SCS, and dimensions, as well as the number of family members, rooms, and bedrooms in households among the sample, which included Urban or Bedouin, Sunni or Shiite, and male or female respondents. A Chi-Square test was used to examine the percentage differences between Urban and Bedouin as well as Sunni and Shiite respondents in terms of COVID-19 infection, contracting the virus from friends or relatives, and the person expected to infect them. To predict and examine the association between sociocultural factors and HCCS, SCES, and SCS, a linear regression was used.
Results
To answer the research question related to the most potential SAs that may transmit infection among Kuwaitis, Table 1 presents the percentages, frequencies, and rankings.
Percentage, Frequencies and Rank of Potential Social Activities That May Transmit Infection.

Table 1 shows that family interaction variables and their associated SAs are ranked first and second as reasons respondents believe may transmit infection among Kuwaitis. The data indicate that the most frequent sources responsible for transmitting infection have come from family members in households and marriage activities, such as weddings and engagement parties. Social gatherings, such as general parties and social visits, ranked third. Respondents believe these gatherings are more frequent sources of transmission. Hospital and clinic environments, including regular doctor visits, hospital stays, and visiting patients at the hospital, ranked fourth. Activities such as sleeping at a hotel, pumping gasoline, praying at a mosque (for men only), and attending a match are considered less effective in transmitting infection.
To examine the differences among levels of education, governorates, household types, and age categories with the HCCS, Sociocultural Effect of Personal Communication, and SCS, Table 2 presents these differences by using One-Way ANOVA.
Mean, SD, F Ratio and p Value of Level of Education, Governorates, and Age Categories With the Health Conditions Commitment, Communication Social Embarrassment and Sociocultural Communication Scales by Using One Way-ANOVA.

For the respondents’ educational levels, Table 2 shows significant differences among the three levels of education (high school or less, graduate, and postgraduate) in the three scales (HCCS, SCES, and SCS). Respondents with higher levels of education showed a higher mean commitment to health conditions, suggesting that they are more aware of following health guidelines in their daily lives. In contrast, respondents with higher education levels scored lower means in communication, social embarrassment, and sociocultural communication compared to respondents with lower education levels. Respondents with higher education levels are more aware of their communication behaviors. The same applies to different age groups (24 years or below, 25–40 years, and 41 years or above). Significant differences among the three age groups in the three scales were found. Older age group respondents have a higher mean in health condition commitment, suggesting that they are more aware of following health guidelines in their daily lives. Conversely, these respondents have lower means in communication, social embarrassment, and sociocultural communication compared to the other age groups (24 years or below and 25–40 years). Older age groups are more aware of their communication behaviors.
The living regions were examined across six governorates (the Capital, Hawalli, Ahmadi, Farwaniyyah, Jahra, and Mubarak Al-Kabeer). Significant differences among the six governorates were found in the three scales (HCCS, SCES, and SCS). Jahra governorate, which has a high level of residents with Bedouin roots, showed a lower mean in health condition commitment and a higher mean in communication, social embarrassment, and sociocultural communication. On the other hand, the Capital and Hawalli governorates, with a high level of residents with Urban society roots, showed higher means in health condition commitment and lower means in communication, social embarrassment, and sociocultural communication. Respondents living in the Capital and Hawalli governorates are more aware of following health guidelines in their daily lives and of their communication behaviors. Respondents with higher education levels, older age, and residing in governorates with a high level of residents with Urban society roots were more aware of following health guidelines and their communication behaviors. Education level, age, and governorate are relevant factors related to health condition commitment, communication, social embarrassment, and sociocultural communication.
To examine the differences among HCCS, SCES, and SCS and their dimensions, as well as the number of family members, rooms, and bedrooms in households within the sample groups (Urban or Bedouin, Sunni or Shiite, and male or female), Table 3 presents these differences by using t-test.
Mean, Standard Deviation and t Value for Health Conditions Commitment, Communication, Social Embarrassment, and Sociocultural Communication Scales and dimensions, and Number of Family Members, Rooms, and Sleeping Rooms at the Household in Sample Who Belong to Urban or Bedouin, Sunni and Shiite and Male or Female by Using t-Test.

p < .05. **p < .01. ***p < .001.
To examine differences between participants with Urban and Bedouin roots, Table 3 shows that significant differences were found in all items and dimensions of HCCS (except one item), SCES, and SCS. Additionally, significant differences were found between participants with Urban and Bedouin roots in the number of family members and number of rooms. Data showed no significant differences in the overall HCCS. However, out of the seven items on this scale, significant differences were found in six items. Data indicated that participants with Urban roots have higher means in their health condition commitment, such as using sanitizer, meeting a small number of people, practicing social distancing when appropriate, and wearing masks when out, compared to Bedouins. Conversely, participants with Bedouin roots have higher commitments to room ventilation and sitting in open areas.
For the overall SCES, a significant difference was found between participants with Urban and Bedouin roots. Data showed that participants with Bedouin roots have higher means in the overall scale and in all its dimensions. Participants with Bedouin roots have higher means in feeling ashamed for not shaking a friend’s hand, not kissing a friend, not seeing a friend for a long time, not kissing an older person’s head, not shaking an older person’s hand, and not kissing a child compared to participants with Urban roots. Participants with Bedouin roots experience more communication-related social embarrassment compared to urban participants.
In sociocultural communication, significant differences were found between the two social groups in the Behaviors Communication Scales and all its dimensions. Participants with Bedouin roots scored higher in the overall scale and in specific behaviors such as shaking hands with friends and relatives, hugging friends and relatives, kissing friends and relatives, accepting dinner invitations, attending men’s and women’s gatherings, attending SAs, and maintaining physical closeness with friends and relatives while gathering, compared to participants with Urban roots.
Data showed significant differences between these two social groups in their living conditions, specifically in the number of family members and the number of rooms in the household. Participants with Bedouin roots have more family members and more rooms in their households compared to participants with Urban roots. However, no significant difference was found between the two groups in the number of bedrooms in the household. This implies overcrowding.
Differences between Sunni and Shiite Muslims were examined. Significant differences were found between the two social groups in all three scales: HCCS, SCES, and SCS. Sunni Muslim participants scored higher on all these scales compared to Shiite Muslim participants. In terms of health communication commitment, Sunni Muslim participants showed higher means for wearing masks when out, room ventilation, and sitting in open areas compared to Shiite Muslim participants. These differences were significant, whereas no significant differences were found in the other items. Additionally, Sunni Muslim participants showed higher means in all items and dimensions of the SCES (e.g., feeling shame for not shaking a friend’s hand, not kissing a friend, not seeing a friend for a long time, not kissing an older person’s head, not shaking an older person’s hand, and not kissing a child who came close). These differences were significant. Out of 11 items in the SCS, eight dimensions were found to be significant for Sunni Muslim participants. Data showed that Sunni Muslim participants had higher means in shaking hands with friends, hugging friends, shaking hands with relatives, hugging relatives, kissing friends, kissing relatives, and maintaining physical closeness with both friends and relatives while gathering. No significant differences were found in the other dimensions. Data showed significant differences between these two faith groups in their living conditions, specifically in the number of family members living in the household, the number of rooms, and the number of bedrooms. Sunni Muslim participants have more family members, more rooms, and more bedrooms in their households compared to Shiite Muslims.
Gender differences were examined in HCCS, SCES, and SCS. Significant differences were found between males and females on all three scales. Females showed higher means in HCCS than males, whereas males showed higher means in SCES and SCS. For the HCCS dimensions, females showed higher means in washing hands with soap, using sanitizer, meeting a small number of people, wearing masks when out, room ventilation, and sitting in open areas. In the SCES, males had higher means in feeling shame for not shaking friends’ hands and for not shaking an older person’s hand. No significant differences were found in the other items. In sociocultural communication, males have higher means than females in shaking friends’ hands, accepting dinner invitations, attending gatherings and SAs, and maintaining physical closeness with relatives and friends. Conversely, females have higher means than males in hugging friends, hugging relatives, and kissing relatives.
To examine the differences between Urban and Bedouin as well as between Sunni and Shiite respondents regarding COVID-19 infection, contracting the virus from friends or relatives, and the person expected to have infected them, Table 4 presents these differences as percentages by using Chi-Square.
Percentage Differences Between Urban and Bedouin and Sunni and Shiite in the Respondents Have Been Infected by COVID-19, Infected by Friends or Relatives and the Person Who Expect Infected Him/Her by Using Chi-Square.

There were notable distinctions between respondents with Bedouin and Urban communities regarding their likelihood of contracting COVID-19 and who they expected to infect them (first family, relatives, friends, and coworkers). The percentage of respondents with Bedouin ancestry (35.4%) is higher than that of respondents with Urban ancestry (27.0%). Additionally, first cousins infected 51.4% of respondents with Urban roots and 50.1% of respondents with Bedouin backgrounds. The corresponding significance levels were (p < .001) and (p < .05). There were no significant differences between Sunni and Shiite respondents who had contracted COVID-19, been infected by friends or family, or contracted the virus from someone they expected to infect them.
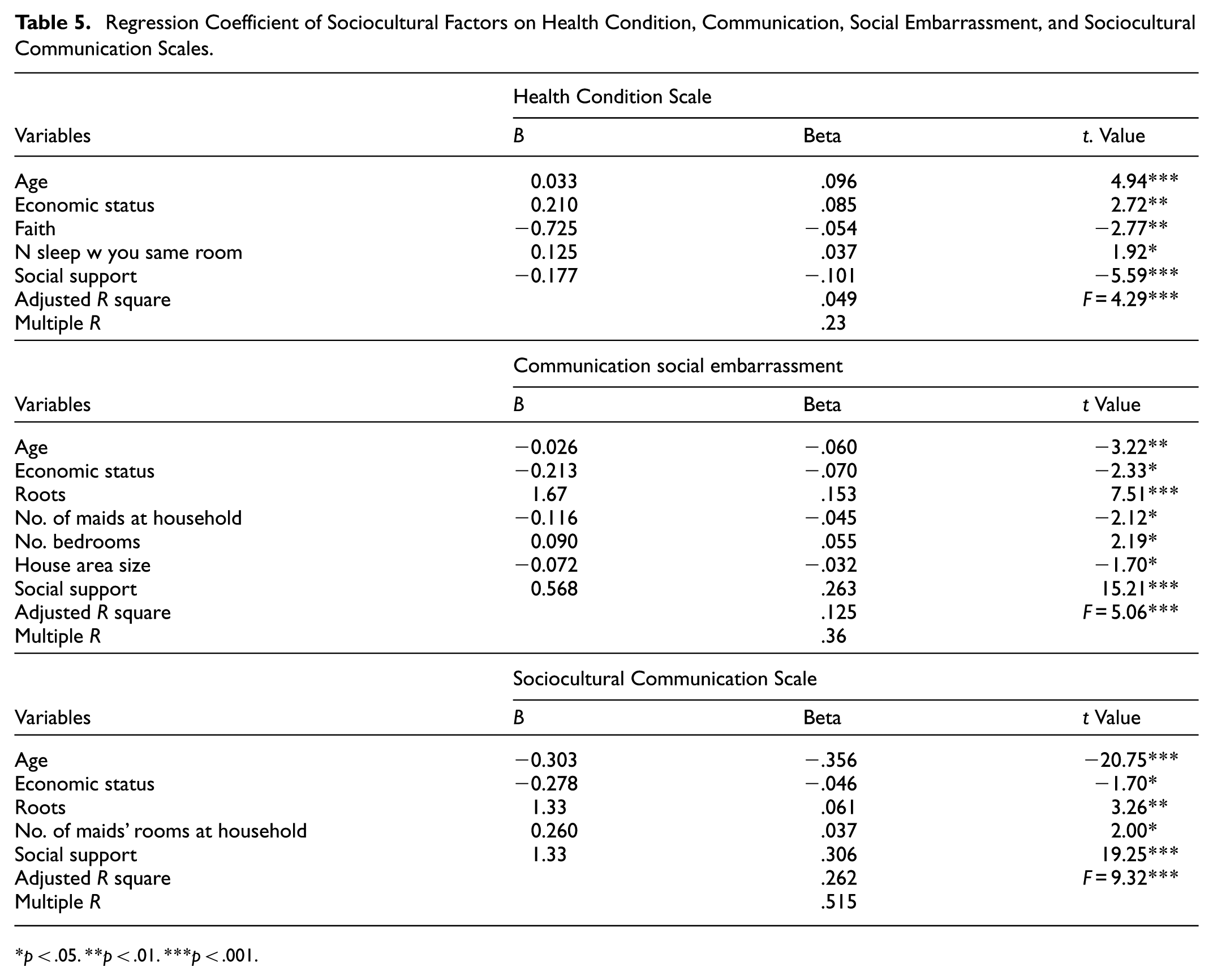
To predict and examine the association between sociocultural factors and HCCS, SCES, and SCS, Table 5 presents the predicted and associated variables for these scales by using linear regression.
Regression Coefficient of Sociocultural Factors on Health Condition, Communication, Social Embarrassment, and Sociocultural Communication Scales.
p < .05. **p < .01. ***p < .001.
The variables most closely related to health condition are age, economic status, faith, the number of people sharing a room with the respondent and social support, as demonstrated in Table 5. Conversely, there are characteristics that influence social shame in communication, such as age, economic status, roots, family members, number of maids in the household, number of bedrooms, size of the house, and social support. In addition, the variables most closely related to influencing sociocultural communication are age, economic status, roots, number of maids in the house and social support.
Discussion
Our findings demonstrate the significant influence of an individual’s social behavior and cultural values on interactions during the COVID-19 pandemic. During the worldwide pandemic, many health instructions were issued by health institutions to control the spread of the virus. The most effective method of reducing virus transmission is physical and social distancing due to the mode of spreading of the SARS-CoV-2 virus (WHO, 2021). Herein, respondents believe that the most common means of coronavirus transmission among Kuwaitis during the pandemic were attending weddings and engagement parties, as well as social gatherings with family and friends. These beliefs held by Kuwaiti respondents reflect their respect and intimacy toward their family and friends. Accepting invitations and attending SAs show the value of hospitality and are considered social duties and obligations in Arabian Gulf culture (Almusallam, 2024). Conversely, being in health institutions such as clinics or hospitals was believed to be the second leading cause of infection with the virus after social gatherings, as they were considered contamination settings for coronavirus among Kuwaiti respondents. This finding can be attributed to the respondents’ awareness of health-related information about the means of virus transmission between individuals. This awareness is due to the regular messages and daily health reports about the transmission, signs, and medical therapy of coronavirus that health centers send to individuals.
Respondents with higher levels of education were more aware of following health protocols in their daily lives, such as washing hands with soap, wearing masks when going out, and meeting with fewer people to avoid contracting the virus from infected individuals. This finding is comparable to the study by Xuyu et al. (2020) about primary school students in Wuhan, China, which found that a student’s grade, mother’s level of education, and father’s occupation were the main factors associated with health precautions during the pandemic, such as mask-wearing and handwashing. More than half of the students (51.6%) reported wearing face masks, and 42.05% of the students used hand hygiene more frequently than others.
Older age groups, specifically those aged 41 and above, were more aware of following health guidelines reported by the WHO during the COVID-19 pandemic. These guidelines included avoiding sitting in close areas, using sanitizer, and practicing social distancing in their daily lives. These findings can be attributed to the higher caution of older individuals about getting infected with the virus because many of them are diagnosed with chronic diseases at this age. Contracting the virus would significantly affect their health and might cause life-threatening conditions or death. Moreover, this finding indicates a high level of health-related information about COVID-19 among Kuwaiti participants. This is comparable to the study by Aldousari and Al-Sejari (2021) in Kuwait, which presents high awareness among respondents about health precautions and hygiene procedures to reduce the possibility of getting the virus. For instance, 56.8% of respondents reported cleaning their hands well by washing with soap, and 61.4% reported rubbing their hands with alcohol.
Older respondents were more aware of maintaining physical distance from others during social gatherings. To avoid contracting the virus through physical interaction during the pandemic, respondents refrained from shaking hands with older people or friends and kissing an older person’s head or children. These findings reveal that older individuals were more aware of WHO health instructions regarding the COVID-19 virus and followed these instructions despite cultural norms and customs of greeting others. This finding is comparable to other studies (Aldousari & Al-Sejari, 2021; Al Sulais et al., 2020; Parikh et al., 2020) that show high levels of precautionary practices against COVID-19 among respondents, such as maintaining social and physical distance, wearing masks, and hand washing due to fear and worry of contracting the virus.
The effect of cultural traditions and daily lifestyle behaviors on greeting and welcoming relatives and friends during the pandemic among Kuwaiti respondents significantly differed based on their residential area. Respondents who live in the Jahra governorate and are descendants of Bedouin society valued following cultural customs and manners of greeting others – such as shaking hands, hugging, and kissing – more than keeping physical distance, wearing masks, and sitting in small groups as recommended by health institutions during the pandemic. Our findings are similar to two studies (Roy et al., 2020; Zhong et al., 2020) conducted in India and China during the pandemic, which reported different health procedures among respondents. A study in Hubei, China, by Zhong et al. (2020) reveals that most men were more hesitant to follow basic health precautions against the COVID-19 virus, such as wearing masks in open areas and avoiding crowded places. Conversely, a study in China by Roy et al. (2020) during the pandemic reported different findings, showing that almost all participants were following basic health regulations and procedures to control the spread of the COVID-19 pandemic, such as wearing masks, using antiseptics, and washing hands more frequently.
Results reveal significant differences between the two Muslim faiths in following health restrictions and procedures regarding greeting and welcoming others and respecting health instructions to prevent infection with the virus. The present study finds that Sunni Muslim participants were more cautious and keener to follow health instructions to prevent infection, such as wearing masks, sitting in open areas, and ensuring room ventilation, compared to Shiite Muslim participants. Conversely, Sunni Muslim participants were more physically interactive with others, such as kissing and hugging relatives and friends when accepting invitations for social events and gatherings. These social behaviors of greeting are related to Kuwaiti culture and traditions, which value physical interactions over verbal and distant greetings when welcoming others. In Arabic culture, kissing an older person’s forehead and cheek reflects positive feelings such as respect, affection, and warmth. The findings of the current study are similar to those of a study conducted in sub-Saharan Africa, which shows that respondents with strong belief and faith that God will protect them from the COVID-19 virus were more hesitant to follow basic health precautions, such as avoiding crowded places and practicing social or physical distancing (World Economic Forum).
The cultural backgrounds of all members of society, including those from the Sunni and Shiite faiths, can be used to interpret this disparity. We know that Sunni Muslims comprise the majority of the population and that many of them are descended from Bedouin tribes. In contrast to Shiite Muslims, who have a relatively small percentage of people from tribal backgrounds, the Sunni component of society is mostly made up of members of Sunni Bedouin tribes. As mentioned earlier, tribal members are more dedicated to social exchanges like kissing, especially on the nose, keeping a close physical distance during greetings and offering salutations. Considering how many of them adhere to the Sunni religion, this could help to explain why they are more physically engaged.
Additionally, compared to Shiite sect members, Sunni believers are more cautious about adhering to health precautions to avoid infection, such as wearing masks, sitting in open areas, and making sure there is adequate ventilation. This may be because Shiite religious practices and beliefs, which are practiced all year round, frequently do not take place outdoors and make it challenging to follow certain health regulations. According to an ethnographic study conducted in Kuwait (Al-Kandari, 2024), public health has been affected by religious events, the majority of which were private gatherings. The well-known outbreak that killed numerous people gathered in a “Hussainiya”– a place of worship where adherents of the Shiite sect gather to perform their rituals – was one case mentioned in this study. Several elderly individuals died, and others were hospitalized as a result of the outbreak, which happened when an infected person attended a closed meeting and spread the sickness. These discrepancies between the two sects may be explained by the intense dedication to attending these events.
Finally, our findings illustrate that demographic factors such as age, residential area, and education have a significant impact on Kuwaiti respondents’ social behavior of greeting and communicating with others, daily lifestyle activities, and following health instructions to control the spread of the COVID-19 virus compared with other factors. This study finds that adherence to health precautions and procedures during the COVID-19 pandemic in daily life, as well as physical activities and SAs, was higher among older respondents with urban roots, those holding higher education degrees, and those living in the Capital governorate. This finding is comparable to a study by Wolf et al. (2020) in the United States, which revealed that 21.9% of respondents said their daily lifestyle schedules altered drastically due to the pandemic.
The study’s conclusions demonstrated the influence of culture on human behavior during the pandemic, based on cultural models of conduct. Individuals’ actions were impacted by a certain cultural trend in society, which altered how individuals viewed and responded to the pandemic and evaluated the risks involved. According to the study, community members’ social interactions within the family structure, attendance at and involvement in social events like weddings, and other interactive social activities were the main ways that COVID-19 spread among them. These activities are associated with social norms, values, conventions, and beliefs that highlight the significance of these relationships in the local culture. The results also revealed that the differences between social variables are not entirely homogeneous, whether in terms of education, age groups, place of residence, or even gender differences. These differences in pandemic response are influenced by social and cultural contexts. Furthermore, the distinctions between social groups – for example, between people with Urban ancestry and those with Bedouin ancestry – and between the two religious groups with respect to social shyness and the extent of compliance with health recommendations – indicate the presence of unique behavioral patterns that surely impact the degree of commitment to health measures and social distancing.
The degree of adherence to social distancing was influenced by social norms and values, which in turn had an impact on the spread of Coronavirus. This confirms the findings of the cultural models of behavior, which hold that a deeply ingrained cultural behavioral model – one that establishes what is deemed necessary or acceptable in social interactions – is the basis for individual decisions about adherence to health regulations and guidelines. The results of the study also support the cross-cultural theory, which postulates that cultural variables influence the level of social distancing commitment. This explains why different social groups has different health habits. Social interactions and relationships are influenced by cultural diversity in society. This diversity also shapes the degree of adherence to health measures and the avoidance of risky behaviors during the epidemic, demonstrating the extent to which cultural structures impact health adherence.
Conclusion
Data shows that there is a tendency to infer cultural causality. The results highlight how social behaviors, cultural norms, and demographic traits significantly influenced health-related behaviors during the COVID-19 pandemic. Disparities in infection origins, adherence to health recommendations, and social interaction patterns were linked to cultural and social environment variations, which are based on variances in origin, living circumstances, and sectarian affiliation. To improve the efficacy of preventative measures and lessen the spread of infectious illnesses in future health emergencies, it is crucial to acknowledge these contextual differences when creating culturally sensitive, focused public health initiatives.
For the limitation of the study, it should be noted that the COVID-19 pandemic’s restrictions prevented access to larger and more randomized participant pools, which is why the sample was drowned. Although the large sample size has been selected, we acknowledge that this approach may impact the representativeness of the sample and introduce potential bias, thus affecting the generalizability of the findings. More studies are needed and there are several suggestions for research that could be conducted. These could include studies that compare various geographic and environmental contexts – like rural and urban communities, or look at how social values and norms affect health compliance, adherence to preventive measures, and avoiding health risks, as well as how religion, religiosity, and sectarian differences impact acceptance of and adherence to health guidelines. Thorough research should also focus on factors related to families, society, and demographics, as well as general methods of controlling illness. To investigate public health symptoms in local communities and the methods used to address them, ethnographic research in particular may prove useful.
Footnotes
Acknowledgements
The authors used an AI-based language editing tools to improve the clarity and readability of the manuscript. All content was reviewed and verified by the authors for accuracy and integrity.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors of a study have access to the research data related to it. When asked for, it is available.
References
 ,
,