
Abstract
Background:
Femoral trochlear dysplasia (FTD) is a major factor affecting the stability of the knee joint. Congenital patellar dislocation (CPD) is usually accompanied by distal FTD. Few studies have investigated trochlear development following surgery in skeletally immature patients.
Purpose:
To observe trochlear remodeling following surgical extensor realignment and stabilization in children with CPD and to analyze the factors associated with this remodeling.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective analysis was conducted on surgical cases of CPD treated at 2 centers between January 2014 and June 2023. The recorded data comprised patient age, sex, side, presence of syndromic CPD, genetic testing results, and magnetic resonance imaging (MRI) findings, including the trochlear depth index (TDI), lateral trochlear inclination (LTI), and medial condylar trochlear offset (MCTO). Pre- and postoperative knee joint range of motion and Lysholm scores were also collected. The surgical procedure involved lateral retinacular release, resection of the redundant medial capsule, lengthening suture of the quadriceps femoris, and a Roux-Goldthwait procedure.
Results:
In total, 58 cases (80 knees) of pediatric FTD (a modified MRI classification of FTD: 19 mild (type A), 28 moderate (type B), 4 severe (type C), 7 special type) with a mean ± SD age of 34.4 ± 3.68 months (range, 14-64 months) were followed up for 2.46 ± 0.73 years. A total of 40 cases (52 knees) were of the idiopathic type and 18 cases (28 knees) were of the syndromic type. Pre- and postoperative TDI, MCTO, and LTI improved significantly (all P < .0001). The patellar redislocation rate was 1.7%; all had full knee motion, with a mean Lysholm score of 96.
Conclusion:
The dysplastic trochlea in CPD postoperation can remodel in skeletally immature patients.
Keywords
Singer first described congenital patellar dislocation (CPD) in 1856, and Conn later defined the condition in 1925 using 4 diagnostic criteria: (1) permanent lateral patellar dislocation, (2) limited active knee extension, (3) unrestricted passive knee range of motion (ROM), and (4) the absence of the patella in the femoral trochlear groove at birth. 10 Because the patellofemoral joint lacks postnatal sliding and the patella itself is inherently dysplastic, CPD is often accompanied by femoral trochlear dysplasia (FTD)15,16,21
Trochlear morphology is a key factor of patellar stability.5,6,14,20,24 While FTD affects <2% of the general population, it is present in 62% to 96% of patients with patellar instability.3,4 This condition involves abnormalities in the shape and depth of the trochlear groove, primarily affecting the cranial portion of the distal femoral epiphysis. 14 The development of the trochlea was traditionally considered genetically predetermined and static after birth. Recent evidence, however, demonstrates trochlear plasticity can allow for remodeling after surgical correction of recurrent or habitual patellar dislocation in children.16,18 It is therefore hypothesized that successful realignment and stabilization surgery can improve trochlear development indices in skeletally immature children with CPD.
Methods
A retrospective analysis was conducted on CPD patients treated at 2 centers (Dalian Women and Children’s Medical Group and Beijing Jishuitan Hospital) between January 2014 and June 2023. Inclusion criteria were (1) children with CPD aged ≤72 months; (2) no previous knee surgery; (3) disease diagnosis confirmed by surgical intervention; and (4) complete and well-preserved imaging data, including preoperative knee magnetic resonance imaging (MRI). Exclusion criteria included (1) age >72 months, and (2) traumatic patellar dislocation.
The patients were grouped based on a modified MRI classification of trochlear dysplasia to compare the trochlear shaping after surgical correction. Trochlear dysplasia was classified into 3 types based on MRI findings: type A (mild) in 19 cases, type B (moderate) in 28 cases, and type C (severe) in 4 cases. An additional 7 cases exhibited a distinct trochlear morphology associated with nail-patella syndrome. The defining features of each type and the measurements of the distal femoral trochlear evaluation indices (TDI, MCTO, LTI) are presented in Table 1. Representative imaging findings are shown in Figure 2.
The collected data comprised patient age, sex, laterality, the presence of syndromic CPD with corresponding genetic testing results, and MRI findings, including the trochlear depth index (TDI), lateral trochlear inclination (LTI), and medial condylar trochlear offset (MCTO). Preoperative and postoperative knee ROM was recorded. Postoperative physical examination assessed patellar tracking by testing lateral displacement at 30° of knee flexion and by passively flexing and extending the knee to confirm satisfactory positioning within the intercondylar groove. Follow-up documentation noted condition of patellar dislocation and the Lysholm score.
Equipment and Materials
Patients were imaged in a supine position with 20° to 30° of knee flexion using a 1.5-T MRI scanner (Siemens Impact Expert) equipped with a quadrature knee coil. Children aged ≤5 years received a chloral hydrate enema for sedation. The imaging protocol comprised sagittal intermediate-weighted sequences, axial fast spin-echo T2-weighted fat-suppressed sequences (3.0-mm slice thickness, 0.3-mm spacing), coronal T1-weighted spin-echo images, and axial 3-dimensional double-echo steady-state gradient-echo sequences. All images were reviewed on a Merge PACS workstation, where measurements were obtained using its digital tools.
Image Interpretation
All images were independently reviewed by a fellowship-trained orthopaedic surgeon (L.H.) and a radiologist (W.G.), both with >10 years of experience in musculoskeletal MRI, who were blinded to participant personal information and clinical history. All distances and angles were measured on the same workstation. Interobserver reliability was assessed to verify measurement consistency. Any discrepancies were resolved through consensus and adjudication by a third reviewer (J.F.), a musculoskeletal MRI diagnostic physician with 20 years of experience.
Measurement Protocol
To address limitations of the Dejour classification in pediatric cases, objective indices were used: TDI, LTI, and MCTO (evaluating groove depth, lateral condylar inclination, and medial condylar development, respectively). The axial slice of MRI that has the largest anteroposterior diameter of the lateral condyle should be selected for measurement. 19
To address the limitations of the Dejour classification in pediatric cases, we employed the objective indices of TDI, LTI, and MCTO, which respectively assessed groove depth, lateral condylar inclination, and medial condylar development. Measurements were taken from the axial MRI slice displaying the greatest anteroposterior diameter of the lateral condyle. 19
First, referring to Figure 1, the tangent line (f) was defined along the border of the posterior femoral condyles, with a parallel line (f ’) drawn through the deepest point of the trochlear groove. The lateral femoral condyle height (distance a) and medial femoral condyle height (distance b) were measured, and the trochlear height was defined as the minimum distance from the deepest trochlear point to line f (distance c, Figure 1). The TDI was calculated as ([a+b]/2 –c). LTI was measured as the angle between line f’ and line g, which connected the highest point of the lateral condyle and the lowest point of the trochlear groove, according to Carrillon et al. 3 MCTO was derived from the formula b – c. Trochlear morphology was classified using a modified MRI–based, 3-part classification system (Table 1, Figure 2).

Diagram of measurements obtained by using transverse sections as described in the Methods section. The tangent line (f) was defined along the border of the posterior femoral condyles, with a parallel line (f’) drawn through the deepest point of the trochlear groove. The lateral femoral condyle height (distance a) and medial femoral condyle height (distance b) were measured, and the trochlear height was defined as the minimum distance from the deepest trochlear point to line f. Lateral trochlear inclination (LTI) was measured as the angle between line f’ and line g, which connect. LTI, lateral trochlear inclination.
Modified Magnetic Resonance Classification of Trochlear Dysplasia a
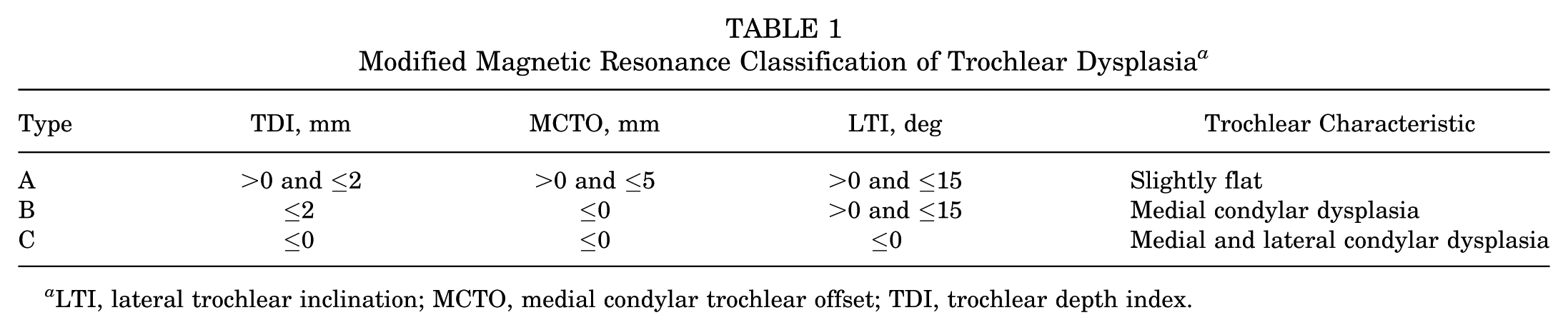
LTI, lateral trochlear inclination; MCTO, medial condylar trochlear offset; TDI, trochlear depth index.

(A) Normal knee magnetic resonance (MR) images obtained from of a 3-year-old boy. (B) Congenital patellar dislocation (CPD) type A knee MRIs obtained from a 14-month-old girl. (C) The MRIs of the 14-month-old girl at 2 years postoperatively. (D) CPD type B knee MRIs obtained from a 3-year-old girl. (E) The MRIs of the 3-year-old girl at 5 years postoperatively. (F) CPD type C knee MRIs obtained from a 15-month-old girl. (G) The MRIs of the 15-month-old girl at 2 years postoperatively. All lines in the panels refer to Figure 1.
Surgical Procedure
Under general anesthesia, the patient was positioned supine with a thigh tourniquet inflated to 300 mmHg. A 7-cm anterior knee incision was made, revealing the patella fixed to the lateral side of the lateral femoral condyle. The lateral retinaculum was released and the redundant medial capsule was resected. The quadriceps femoris was selectively lengthened and sutured according to the degree of its contracture. As the preoperative tibial tubercle–trochlear groove measurement exceeded 25 mm, a Goldthwait procedure was performed: the lateral half of the patellar tendon insertion was transected, passed deep to the medial half, and shifted posteromedially. An absorbable suture anchor (2.9 mm; Johnson & Johnson) was used to fix the tendon to the anteromedial tibial metaphysis (Figure 3). Postoperative management involved immobilization with a long-leg brace, followed by early quadriceps isometric exercises after anesthesia recovery, ROM training at 3 weeks, and partial weightbearing at 6 weeks.

Surgical procedure. (A) Patella fixed on the lateral side of the lateral condyle of the distal femur. (B) Lateral retinacular release. (C) Resection of the redundant medial capsule. (D) Patella substantially returned to the central position of the knee joint. (E) Patella sutured to the remaining medial capsule. (F) Lateral half of the patellar ligament separated and woven. (G) Lateral half of the patellar ligament transposed medially. (H) Absorbable screw fixation.
Statistical Analysis
All data were analyzed using SPSS 26.0. First, the normality test of the data was conducted using skewness-kurtosis test, normally distributed variables were presented as mean ± SD, and the nonnormally distributed variables were presented as median (IQR). Intergroup comparisons of these variables used the rank-sum test. Categorical data were presented as percentages. Intergroup comparisons of these data used the chi-square test or Fisher exact test. Bonferroni correction was applied for pairwise comparisons. A 2-sided P value <.05 was considered statistically significant. The Shapiro-Wilk test was used to assess the normality of continuous data, and the Levene test was used to check for homogeneity of variance. Cohen kappa was used as the measure of interobserver reliability for MRI-derived quantitative measurements (TDI, LTI, and MCTO). Analysis of variance was used to assess differences among the various types of FTD data. Pearson chi-square test and Fisher exact test were used to evaluate the differences in the proportions of each subtype. Multilevel models were conducted to assess the impact of different measurement indicators before and after surgical intervention. A P value <.05 was considered statistically significant.
Results
Cohort Characteristics
This study included 58 patients (80 knees) with a mean age of 34.4 ± 3.68 months (range, 14-64 months) and comprised 25 male and 33 female patients (Table 2). The mean follow-up duration was 2.46 ± 0.73 years (range, 2-6 years). Of the total, 40 cases (52 knees) were idiopathic, while 18 cases (28 knees) were syndromic. The syndromic cases included 1 genitopatellar syndrome, 2 Larson syndrome, 1 Rubinstein-Taybi syndrome, 1 Ehlers-Danlos syndrome, 2 Kabuki syndrome, 7 nail-patella syndrome, 2 Down syndrome, 1 Say-Barber-Biesecker-Young-Simpson (SBBYSS) syndrome, and 1 small patella syndrome.
Baseline Characteristics of the Study Sample a

Data are presented as n (%). Modified magnetic resonance classification of femoral trochlear dysplasia: type A, trochlea is slightly flat; type B, dysplasia of the medial condyle; type C, dysplasia of the medial and lateral condyles.
Figure 4 presents the age distribution at surgery. Patients were categorized into 3 surgical age groups: ≤30 months, 31 to 39 months, and ≥40 months (P > 0.05) (Table 2).

Age distribution of congenital patellar dislocation surgery.
Clinical Follow-up and Complications
Only 1 patient, who also had Ehlers-Danlos syndrome, experienced patellar subluxation postoperatively, whereas no dislocations occurred in the remaining children. The patellar redislocation rate was 1.7% (1/58). Preoperatively, 37 patients exhibited a restricted range of knee flexion and extension. Three cases involved bilateral CPD; since the contralateral side had not yet undergone surgical correction, normal lower limb activity was not fully restored. The other patients achieved full knee ROM postoperatively, with no effect on leg length. One patient presented with patella baja, exhibiting an Insall-Salvati index of 0.78, while the others ranged from 0.93 to 1.18. The mean Lysholm knee score at the final follow-up was 96 points (range, 89-100).
One patient developed a postoperative incision infection, which required abscess drainage 1 week after surgery and resulted in delayed wound healing at 3 weeks. Two patients with quadriceps muscle strength of grade 4 received rehabilitation treatment. No patient reported knee pain.
Evaluation of Trochlear Development
Type A, mild (preoperative: TDI, 1.31 ± 0.12 mm; MCTO, 0.81 ± 0.70 mm; LTI, 13.3°± 3.18°; postoperative: TDI, 1.53 ± 0.15 mm; MCTO, 0.95 ± 0.69 mm; LTI, 13.5°± 2.75°). Type B, moderate (preoperative: TDI, 0.13 ± 0.43 mm; MCTO, –1.07 ± 0.51 mm; LTI, 8.4°± 2.05°; postoperative: TDI, 1.15 ± 0.30 mm; MCTO, 0.08 ± 0.63 mm; LTI, 10.3°± 2.63°). Type C, severe (preoperative: TDI, −0.97 ± 0.61 mm; MCTO, −0.84 ± 0.34 mm; LTI, –4.4°± 1.34°; postoperative: TDI, −0.99 ± 0.53 mm; MCTO, −0.80 ± 0.27 mm; LTI, –4.9°± 2.29°). Comprehensive intergroup differences for variables related to the classification of trochlear dysplasia are presented in Table 3. We report excellent interobserver reliability for the measurement: Cohen kappa coefficient was 0.89 (95% CI, 0.82-0.96; P < .001), which is consistent with the threshold for “excellent reliability” (κ > 0.75). The relative changes in measurements from the preoperative to the postoperative varied among the different trochlear dysplasia types, as shown in Figure 5. Patients were divided into 3 age groups (≤30 months, 31-39 months, ≥40 months), with no significant statistical differences in trochlear dysplasia indices between groups (Table 4).
The Performance of TDI, MCTO, and LTI in Different Types of Trochlear Dysplasia a

Data are presented as mean ± SD. LTI, lateral trochlear inclination; MCTO, medial condylar trochlear offset; postop, postoperative; preop, preoperative; TDI, trochlear depth index.

Changes in trochlear depth index (TDI), lateral trochlear inclination, and medial condylar trochlear offset pre- and postsurgery for trochlear dysplasia.
Statistical Results of Various Indicators in Preoperative and Postoperative Periods for Patients in Different Age Groups a

Data are presented as mean ± SD or median (IQR). LTI, lateral trochlear inclination; MCTO, medial condylar trochlear offset; postop, postoperative; preop, preoperative; TDI, trochlear depth index. After the operation, TDI, MCTO, and LTI were improved, with more significant changes in TDI and MCTO. Group A is the type A basis for modified magnetic resonance imaging classification of femoral trochlear dysplasia, group B is type B, and group C is type C.
Discussion
Following surgical realignment and stabilization of the extensor mechanism in children with CPD, the patellar groove can eform. Postoperative measurements averaged 0.49 mm for TDI, 0.03 mm for the MCTO, and 6.3° for LTI. These values represent an improvement over the preoperative means of 0.15 mm for TDI, −0.7 mm for MCTO, and 5.7° for LTI. In type A, the depth of the trochlear groove, the development of the medial and lateral condyles, and the inclination of the lateral groove all improved. For the moderate type B, all 3 indices showed much more significant improvement than type A. In severe type C cases, a concave trochlear groove did not form postoperatively; instead, a tracklike structure congruent with the patella developed. With follow-up ranging from 2 to 6 years, skeletal immaturity persisted in these patients, and they remained under observation at the time of this study’s publication.
Traditionally, trochlear morphology was considered to be genetically determined,8,15 but emerging evidence highlights mechanical stress as a driver of bone remodeling. 11 In the patellofemoral joint, functional loading during knee flexion stimulates trochlear development. 9 Wang et al 23 animal studies show that early patellar reduction prevents trochlear flattening in rabbits. Clinical studies have also reported this observation. 12 Benoit et al 1 reported on 8 patients with 12 knees of habitual patellar dislocation, with a mean age of 10.3 years (range, 7-14 years) at the time of surgery. After patellar stabilization surgery, there was a statistically significant improvement in the sulcus angle (mean preoperative angle was 160° (153°-169°); mean postoperative angle was 141° (137°-142°). Fu et al 7 reported on 23 patients with 23 knees, with a mean age of 9.6 years (range, 7-11 years), and a follow-up of 48.7 months (range, 43-56). For children with recurrent patellar dislocation combined with trochlear dysplasia, early (before epiphyseal closure) surgical correction can improve the morphology of the femoral trochlea.
Our research found that most cases of CPD were accompanied by trochlear dysplasia, with 51 out of 58 cases. The mean age was 34.4 ± 3.68 months (range, 14-64 months). This cohort was significantly younger than those reported by Benoit et al 1 and Fu et al, 7 suggesting a potentially greater capacity for morphological adaptation. The follow-up period was 2 to 6 years, and the bones were not mature. The mean TDI value was 0.15 mm, the mean MCTO value was −0.7 mm, and the mean LTI value was 5.7°. Pfirrmann et al 17 pointed out that when TDI is ≤3.0 mm, the sensitivity and specificity for diagnosing mature bone FTD are 100% and 96%, respectively. Stepanovich et al 2 indicated that when MCTO is ≤1.0 mm, the sensitivity and specificity for diagnosing FTD are 93% and 75%, respectively. Stepanovich et al 22 found that when LTI is ≤17°, the specificity for diagnosing immature bone (9-16 years of age) FTD is 96%, and the sensitivity is 50%. Among them, 7 cases were not accompanied by trochlear dysplasia, all of which were nail-patella syndrome, characterized by habitual patellar dislocation, patellar dysplasia or absence, and a significantly deepened trochlear groove. Johnson and Milicic 13 believed that the presence of habitual patellar dislocation at birth can be diagnosed as CPD, so these 7 cases were also included in this group of cases. The development of the trochlea in our patients with CPD was more complex, and the previously rarely reported type C (severe) was discovered. Its characteristics are that both the medial and the lateral condyles of the distal femur are dysplastic, forming an archlike trochlear shape, with TDI value <0 mm, MCTO value ≤0 mm, and LTI value ≤0°. Neither has it been reported in Dejour classification, nor has it been reported in MRI classification. 25 One of the cases had a genetic test indicating a mutation in the KAT6B gene, suggesting SBBYSS syndrome and genitopatellar dysplasia syndrome. Genetic testing was not performed on the other 3 patients.
Limitations
The limitation of this study is that the number of cases is still relatively small, but it is a larger case report of this disease among the existing reports. The inclusion of cases with various syndromes, such as patellar syndrome, may have influenced the results. This group of cases did not take into account the influence of the classification of the patella on the postoperative shaping of the trochlea. This can be considered in future studies. The follow-up time should be further extended, and possibly more convincing evidence can be obtained. Based on age, a more detailed division can be made to obtain more valuable data. We look forward to more prospective studies with multicenter cases. And further research is needed to elucidate its underlying mechanism for all reserchers in this field.
Conclusion
After surgical extensor realignment and stabilization of the patella in children with CPD, the trochlea can remodel. The overall morphology of the trochlea in type C after surgery shows no significant improvement, while type A and type B show different degrees of remodeling.
Footnotes
Final revision submitted December 23, 2025; accepted December 26, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: Beijing Jishuitan Hospital Joint Laboratory Innovation Transformation Project (LH-202208) Guizhou Science and Technology Cooperation Results–LC (2024) 103. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the institutional ethical review board of Dalian Women and Children’s Medical Group (No. FEJT-KY-2025-107).