
Abstract
Background:
Sparse objective data are available documenting changes of trochlear shape after trochleoplasty.
Purpose/Hypothesis:
The purpose was to investigate whether standardized magnetic resonance imaging (MRI) measurements that characterize trochlear dysplasia (TD) change significantly after arthroscopic deepening trochleoplasty (ADT) combined with medial patellofemoral ligament (MPFL) reconstruction. It was hypothesized that MRI measurements would approximate normal values.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent ADT between October 2014 and December 2017 were considered for this study. The preoperative inclusion criteria for ADT surgery were patellar instability, a dynamic patellar apprehension sign at 45° of flexion, a lateral trochlear inclination (LTI) angle of <11°, and failed physical therapy. MRI was performed pre- and postoperatively, and standardized MRI measurements were calculated: LTI angle, trochlear depth, trochlear facet asymmetry, cartilage thickness, and trochlear height. The Banff Patella Instability Instrument 2.0 (BPII) score, Knee injury and Osteoarthritis Outcome Score (KOOS), and Kujala score were obtained pre- and postoperatively.
Results:
A total of 16 knees in 15 patients (12 female and 3 male; median age, 20.9 years; range, 14.1-51.3 years) were evaluated. The mean follow-up time was 63.6 months (range, 23-97 months). The median LTI angle improved from 1.25° (range, –25.1° to 10.6°) preoperatively to 10.7° (range, –17.7° to 25.8°) postoperatively (P < .001), trochlear depth increased from 0.0 mm (range, –4.2 to 1.8 mm) to 3.23 mm (range, 0.25-5.3 mm) (P < .001), and trochlear facet asymmetry improved from 4.55% (range, 0.0%-28.6%) to 17.8% (range, 0.0%-55.6%) (P < .003). Cartilage thickness was unchanged: 4.5 mm (range, 1.9-7.4 mm) preoperatively and 4.9 mm (range, 0.6-8.3 mm) postoperatively (P = .796). BPII, KOOS, and Kujala scores improved significantly (P < .0034 for all).
Conclusion:
Combined ADT and MPFL reconstruction led to statistically significant and clinically relevant improvements in patient-reported outcomes and standardized MRI measurements that characterize TD. The improvements corresponded to those obtained by open trochleoplasty. No significant reduction in cartilage thickness was seen.
Keywords
Deepening trochleoplasty is a well-established procedure to stabilize the patella in patients with patellar instability and severe trochlear dysplasia (TD). Systematic reviews and meta-analyses have found low rates of redislocation and complication. 18,22,23,43 The aim of a deepening trochleoplasty is to create a more normal shape of the trochlear groove, meaning a deeper and often a more lateralized groove, in order to provide better engagement and stability of the patella. It is believed that deepening trochleoplasty changes the shape of the trochlea in the direction of a normal groove, but to our knowledge, no study has systematically assessed standardized magnetic resonance imaging (MRI) measurement before and after trochleoplasty. Deepening trochleoplasty can be performed by open or arthroscopic techniques. The open techniques by Dejour and Deroche 13 and Bereiter 26 are the most well known and generally recognized. The arthroscopic deepening trochleoplasty (ADT), an arthroscopic variant of the Bereiter technique, was described by Blønd and Schöttle 9 in 2010. Clinical studies on this technique are sparse, but good clinical outcomes have been reported in cases with severe TD and patellar instability. 6,8 Concerns have been raised as to whether the technique is capable of changing the trochlear groove in the direction of the desired, more normal shape.
The aim of the present study was to investigate whether standardized MRI measurements that characterize TD would change significantly after ADT. We hypothesized that MRI measurements would approximate normal values after ADT.
Methods
Patients
This was a retrospective cohort study with prospectively gathered follow-up data. The study protocol was approved by the regional ethics committee of the greater Copenhagen area. Patients were included from the first author’s (L.B.’s) surgical lists at Aleris Private Hospital in the period between October 2014 and December 2017. Patients were eligible for inclusion if they had undergone ADT and medial patellofemoral ligament (MPFL) reconstruction (MPFL-R), spoke Danish, had an available preoperative MRI scan, and had filled out preoperative patient-reported outcome measures. If patients fulfilled the inclusion criteria, there were no exclusion criteria. If data were missing in the questionaries, patients were contacted by phone to obtain the missing information. Patients were invited twice to participate in the study by mail, and if they did not respond, they were contacted twice by phone. Patients gave written informed consent to participate in the study.
Arthroscopic Deepening Trochleoplasty Procedure
Indication for ADT was recurrent patellar instability, dynamic patellar apprehension in 45° of flexion, a lateral trochlear inclination angle <11° according to Carrillon et al, 10 and failed physical therapy. ADT was performed with an updated technique from Blønd. 6 Knees with small, grade 3 to 4 lesions in the trochlear cartilage were included. Chronologic age is not regarded as a limitation for the surgery; however, the general medical status of the patient has an impact, especially if cartilage status is impaired such as in the presence of subchondral bone sclerosis and/or there seem to be other risk factors for impaired healing potential of the cartilage flap. Through 2 standard anterior arthroscopic portals and 2 extra suprapatellar portals, a cartilage flap was released by shaver burs, and the trochlear groove was deepened and lateralized. At the end of the procedure, the cartilage flap was refixed by absorbable tapes and sutures, similar to the fixation technique for open Bereiter deepening trochleoplasty. 16 The MPFL was reconstructed using a gracilis tendon in a double-bundle inlay technique with bony fixation at both the patellar insertion and the femoral insertion site. No tibial tubercle osteotomies or rotational osteotomies were performed.
MRI Measurements
MRI was performed pre- and postoperatively on 1.5-T imaging systems. The preoperative scans, which were acquired retrospectively, were performed on different systems at outside facilities before referral to our center. The postoperative MRI scans were performed on a GE MRI Signa Voyager 1.5-T 28.0 (GE Healthcare) using an 8-channel cardiac coil (patient in supine position without quadriceps contraction, with the affected knee completely or nearly completely extended in the knee coil). Sagittal, coronal, and axial images were obtained. Measurements were obtained independently by 2 orthopaedic surgeons specializing in patellofemoral surgery (L.B. and K.W.B.). In the prestudy period, several collaborative training sessions were performed to reduce interobserver variability. The mean of the measurements from the 2 reviewers was then calculated.
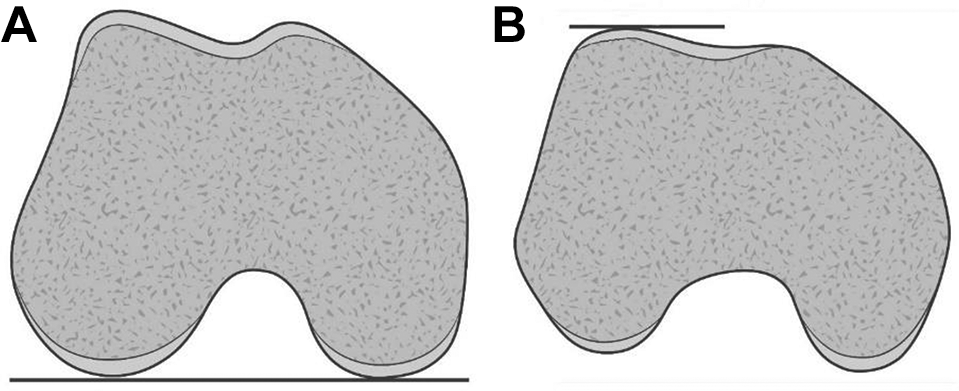
The measurements were performed at the 4 most proximal axial slices visualizing the trochlear cartilage (levels 1-4, with level 1 most proximal). The thickness of the axial slices was 3.5 mm and the distance between slices was 0.5 mm, so the measurements were performed 0 to 3.5 mm, 4 to 7.5 mm, 8 to 11.5 mm, and 12 to 15.5 mm from the proximal boarder of the trochlea (Figure 1). To secure measurement at similar levels pre- and postoperatively, a measurement from the notch to the proximal border of the trochlea was performed on sagittal view at the center of the knee with the anterior cruciate ligament well-defined. The most proximal slice on axial view was the first slice distal to this point at both scans. All of the measurements were performed on the cartilage surface and not the bone. 37,42 The posterior condylar line was defined as a line tangent to the most posterior extent of the femoral condyles. 19 The following measurements were performed: (1) lateral trochlear inclination (LTI) angle, (2) trochlear depth, (3) trochlear facet ratio (percentage), (4) anterior-to-posterior (AP) trochlear measurement (percentage), (5) cartilage height, (6) tibial tubercle–trochlear groove (TT-TG) distance, (7) lateral patellar inclination (LPI) angle, (8) extent of trochleoplasty, and (9) length of trochleoplasty.

(A) Preoperative and (B) postoperative axial magnetic resonance imaging scans of the same knee. The measurements were performed at the 4 most proximal axial slices visualizing the trochlear cartilage: level 1: 0-3.5 mm from the proximal border of the trochlea; level 2: 4-7.5 mm; level 3: 8-11.5 mm; and level 4: 12-15.5 mm. The artifact in the patella is a titanium suture anchor after 2 previous attempts of reconstruction of the medial patellofemoral ligament.
LTI Angle
The LTI angle is a numeric measure of the trochlear slope and an indicator of the osteocartilaginous support for the patella. 2 The LTI angle has been said to be the single most important objective measurement in respect to evaluation of TD. 19,30 The newer 2-image MRI technique from Joseph et al 19 was used to measure the LTI angle (Figure 2). However, at the time of the preoperative evaluation, the technique from Joseph et al had not yet been published, and therefore the preoperative evaluation was based on the single-image technique described by Carrillon et al. 10 In the 2-image method, the angle is measured between the posterior condylar line and a line along the lateral trochlear cartilage surface at the most proximal slice that contains cartilage. When a convex or spurred trochlea was present, the line along the lateral trochlear cartilage surface was defined as the best-fit line representing the tangential line between the cartilaginous surface of the lateral trochlea and apex of the convexity. According to Cheng et al, 11 the normal mean is 21° and an LTI angle <9° indicates TD.
Illustrations of how to measure the lateral trochlear inclination (LTI) angle using the 2-image technique. 19 (A) Axial view at the level where the femoral condyles are most prominent and the posterior condylar line is tangential to both femoral condyles. (B) Best-fit or tangential line to the cartilage on a slightly convex lateral trochlea. The LTI angle is the angle between the lines in (A) and (B).
Trochlear Depth
A shallow trochlear groove is one of the key characteristics of TD. Earlier studies showed the depth to increase after deepening trochleoplasty. 3,44 To measure trochlear depth, we used the method from Escala et al. 15 Two lines parallel to the posterior condylar line were made: 1 line intersecting the shallowest point of the trochlea and 1 line intersecting the top of the cartilage on the lateral femoral condyle. The trochlear depth was the distance between the 2 lines. In cases with a convex trochlear configuration, the depth was recorded as negative.
Trochlear Facet Ratio
Trochlear facet asymmetry is a parameter for quantifying the medialization of the groove and thereby is connected to the TT-TG distance. 31,39 Both Ntagiopoulos et al 27 and Banke et al 3 observed that the TT-TG distance was reduced by a trochleoplasty moving the center of the new trochlear groove laterally. To measure the facet ratio, we used the method from Pfirrmann et al. 32 The facet ratio was calculated as the ratio of the length of the medial trochlear facet to the length of the lateral trochlear facet. The mean normal facet ratio is 57%, and a ratio <40% indicates TD if measured at 3 cm above the tibiofemoral joint line. 32
AP Trochlear Measurement
Biedert and Bachmann 5 characterized TD by the AP measurement of the femoral condyles and the trochlear groove. The 3 measurements are a ratio between the width of the knee, the height of the 2 femoral condyles, and the height of the trochlea. The measurements are the shortest distance from the posterior condylar line to the top of the lateral condyle, to the lowest point of the trochlea, and to the top of the medial condyle, respectively. According to Biedert and Bachmann, a central height to width ratio >77% indicates too much bone central in the trochlea and, thus, TD.
Cartilage Height
Concerns have been raised with respect to cartilage changes after trochleoplasty, and data are sparse regarding long-term consequences for the trochlear and patellar cartilage. We measured the cartilage height on T1-weighted axial MRI slices at the center of the articulation between the patella and the lateral facet of the trochlea. The measurement was conducted perpendicular to the joint line and from the bone-to-cartilage transition on the trochlea to the bone-to-cartilage transition on the patella. In cases where it was difficult to measure cartilage height because of patellar-trochlear incongruency, the measurement was omitted (Figure 3).
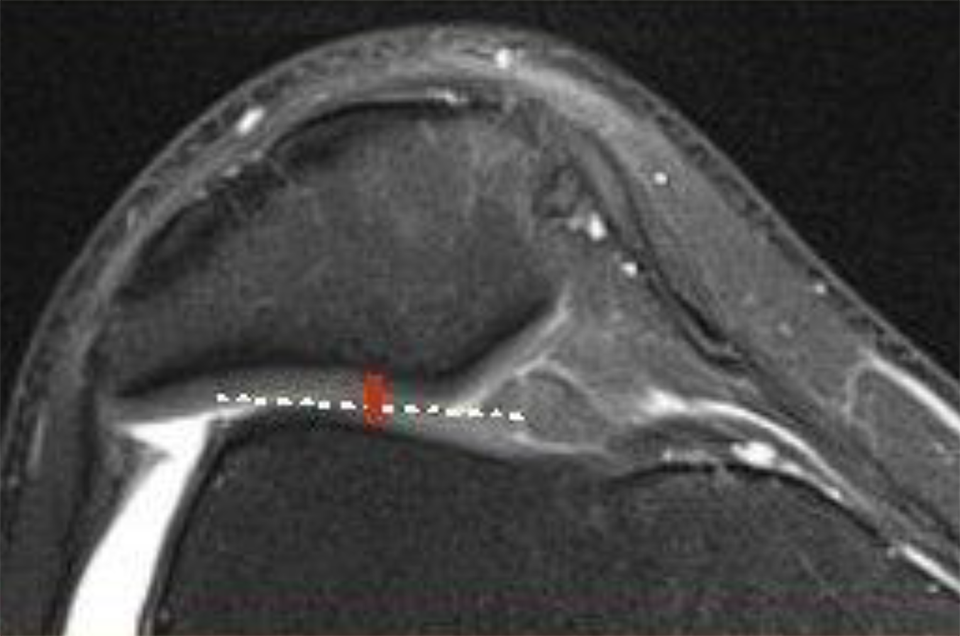
Magnetic resonance imaging scan demonstrating how the cartilage height on the patella (red line) and the lateral facet of the trochlea (dashed white line) was measured.
TT-TG Distance
It was previously described that the TT-TG distance was reduced after trochleoplasty moving the center of the new trochlea laterally. 3,27 We assessed the TT-TG distance using the most distal and proximal axial slice displaying full cartilage coverage of the trochlear groove and the most proximal slice of the patellar tendon insertion on the tibial tuberosity. 28,31 The TT-TG was defined as the distance between the midpoint of the tibial insertion of the patellar tendon and the deepest point of the trochlear groove when measured parallel to the tangent along the posterior femoral condyles (posterior condylar axis).
LPI Angle
The LPI angle (or patellar tilt) is related to TD as a consequence of a reduced trochlear slope. When the trochlear slope is normalized by a deepening trochleoplasty, the patellar tilt correspondingly reduces. 3,29 To evaluate patellar tilt, we used the measurement of LPI angle, a newer cross-sectional, 2-image technique from Pace et al. 29 LPI angle is the angle between the posterior condylar line and an intraosseous line between the major axis of the patella in the transverse plane and going from the outer points of the patella laterally and medially, respectively. The MRI axial image with the widest cross section of the patella was selected for the patellar orientation. 15,29
Extent of Trochleoplasty
In most cases, scarring of the bone was observed secondary to the trochleoplasty procedure. This scarring was used to estimate how far from the notch the trochleoplasty extended. The measurement was performed on the sagittal slice with the most distal extent of scarring. Representing the most distal aspect of the trochlea, a line perpendicular to the femoral axis intercepting the most distal part of the femoral notch was drawn. The extent of the trochleoplasty was the distance between the point and the line (Figure 4A).

(A) Demonstration of the extent of the arthroscopic deepening trochleoplasty (ADT) with respect to the distal part of the trochlea. (B) Demonstration of the distance from the proximal extension of the trochlear cartilage to the distal part of the trochlea. The length of the ADT is this distance minus the extension.
Length of Trochleoplasty
On sagittal view, the distance between the most proximal extent of the trochlear cartilage and a line perpendicular to the femoral axis intercepting the most distal part of the femoral notch, minus the extent of trochleoplasty, represents the overall length of the ADT (Figure 4B).
Patient-Reported Outcomes
The patients’ self-perceived function was evaluated pre- and postoperatively with the Banff Patella Instability Instrument 2.0 (BPII 2.0), the Knee injury and Osteoarthritis Outcome Score (KOOS), and the Kujala score. 17,20,21 The preoperative scores were obtained within 4 weeks before the surgery. The postoperative scores were obtained between August 2021 and December 2021.
The BPII 2.0 score is expressed as a percentage between 0 and 100, with 100 indicating no symptoms. The score was developed to evaluate patellar instability and has been found to have high validity, reliability, and responsiveness. 17 The KOOS was originally developed to evaluate knee symptoms in patients who have osteoarthritis and is used regularly in patients who have patellar instability. The Kujala score is probably the most commonly used score regarding patellofemoral instability, although it was originally developed to evaluate patellofemoral disorders in general and was not focused on dislocations. The complications deep infection, reduced range of motion, deep vein thrombosis, redislocation, and subluxations were registered. Minor complications such as superior wound infections were not registered.
Statistical Analysis
The sample size was determined by the availability of patients. No power calculation was performed. Pre- and postoperative findings were compared using the Wilcoxon signed-rank test. The significance level was set at P < .05. Calculations were performed using SOFA statistical computer software.
Results
A total of 32 patients were treated with ADT and MPFL-R by the first author in the inclusion period. Of those, 20 patients met the inclusion criteria for this study. Two patients did not respond, 1 patient did not want to participate, 1 patient was abroad, and 1 patient was pregnant and could therefore not undergo postoperative MRI. One patient had bilateral surgery, and both knees were included in the study. Thus, 16 knees in 15 patients (12 female and 3 male) were enrolled. Median age at the time of surgery was 20.9 years (range, 14.1-51.3 years). The mean time to follow-up was 63.6 months (range, 23-97 months). Five of the included patients had previous failed surgeries, 2 patients had undergone MPFL-R once and 2 patients twice, and 1 patient had arthroscopic debridement of cartilage.
Pre- and postoperative measurements are found in Tables 1 and 2. The median length of the trochleoplasty was 26.5 mm (range, 15.0-36.9 mm), and the median extent of the trochleoplasty was 9.5 mm (range, 3.5-16.7 mm) from the notch. In this cohort of 15 patients (16 knees), we did not observe any cases of patellar redislocation or subluxation, deep vein thrombosis, infection, reoperation, or reduced range of motion.
Pre- and Postoperative Patient-Reported Outcome Scores and Magnetic Resonance Imaging Measurements a

a Data are reported as median (range). Bolded P values indicate statistically significant difference between groups (P < .05). AP, anteroposterior; BPII 2.0, Banff Patellofemoral Instability Instrument BPII 2.0; KOOS, Knee injury and Osteoarthritis Outcome Score; LPI, lateral patellar inclination; LTI, lateral trochlear inclination; TT-TG, tibial tubercle–trochlear groove distance.
b Axial magnetic resonance imaging measurements were performed at the 4 most proximal axial slices visualizing trochlear cartilage: level 1: 0-3.5 mm from the proximal border of the trochlea; level 2: 4-7.5 mm; level 3: 8-11.5 mm; and level 4: 12-15.5 mm. The most proximal slice was a median distance of 32.1 mm from the notch.
Pre- and Postoperative Lateral Trochlear Inclination Angle and TT-TG Distance Measured Proximally for Each Knee

a Axial magnetic resonance imaging measurements were performed at the 4 most proximal axial slices visualizing trochlear cartilage: level 1: 0-3.5 mm from the proximal border of the trochlea; level 2: 4-7.5 mm; level 3: 8-11.5 mm; and level 4: 12-15.5 mm. The most proximal slice was a median distance of 32.1 mm from the notch. Post, postoperative; Pre, preoperative; TT-TG, tibial tubercle–trochlear groove.
Discussion
The findings from this study indicate that ADT surgery was capable of changing the trochlear groove configuration in a positive direction, to such a degree that statistically significant changes in MRI measurements used to evaluate TD could be observed. Most measurements improved with the procedure, but they did not reach normal values. Moreover, a statistically significant and clinically relevant improvement was seen in the 3 patient-reported outcome measures. In respect to the safety of the procedure, no complications were observed.
The LTI angle showed statistically significant improvement at all 4 levels. At level 1, the median LTI angle changed from 1.3° preoperatively to 10.7°after surgery. This result is in accordance with the finding from Zimmerman et al, 45 who demonstrated that the LTI angle increased from 0.5° preoperatively to 9.9° after open trochleoplasty. We evaluated the LTI angle using the 2-image technique by Joseph et al, 19 and because this measurement focuses on a more proximal location than the original one from Carrillon et al, 10 the threshold for TD was reduced from 11° to 8.9°. We chose LTI angle as the primary measurement for TD because this parameter best reflects the osteocartilaginous stability or constraint provide by the lateral trochlear slope, which has been biomechanically demonstrated by Rezvanifar et al, 33 and because Cheng et al 11 suggested defining TD by the LTI angle alone. Balcarek et al 2 observed that LTI angle decreased at higher grades of TD evaluated by the Dejour classification. We did not include the commonly used Dejour classification in this study given its low reproducibility 7 and its subjectivity. Further, a biomechanical study by Van Haver et al 41 did not demonstrate any significant differences between the 4 Dejour types with respect to instability.
Some studies have implied that trochleoplasty might be indicated only in revisions after failed MPFL-R, because failed MPFL-R is not common. 34 Schlumberger et al 34 reported midterm results (mean, 4.7 years) of 49 adolescent patients who had patellar instability; of those, 19 patients had TD type B and 7 patients had TD type C or D. The 3 failed cases in the study had TD type B. The investigators found no significant difference in outcome scores (Lysholm, Kujala, Tegner, and International Knee Documentation Committee) between the patients with versus without TD, perhaps because the study was underpowered. In contrast, a meta-analysis by Balcarek et al 2 found a significantly reduced rate of MPFL failure among patients who had patellar instability due to severe TD if the MPFL-R was combined with trochleoplasty, compared with those who had isolated MPFL-R. That being said, a randomized controlled trial with long-term follow-up using adequate outcome scores is required. In our study, the trochlear depth showed statistically significant improvement on all 4 levels, from median 0.00 mm to 3.23 mm on level 1, which is in accordance with previous studies investigating open trochleoplasty. 1,15,24,38
We found statistically significant improvement in trochlear facet asymmetry on all 4 levels, from median 4.55% to 17.8% on level 1. This figure is difficult to compare with previous studies, given the level of measurement. Traditionally, trochlear asymmetry is measured 30 mm above the joint line; however, in our study, the most proximal level was a median of 32.1 mm above the notch and was thereby more proximal, giving significantly lower values. 1,4,24 Increased TT-TG distance is often seen in TD due to a medialized trochlear groove, an increased external torsion of the tibia, or a laterally placed tibial tubercle. 31,39 ADT aims to normalize this by lateralization of the trochlear groove, as shown in previous studies of open trochleoplasty. 3,27 Interestingly, we found conflicting data on whether this was achieved. We observed that the trochlear asymmetry was improved significantly, indicating that lateralization of the trochlear groove was achieved. Despite this finding, we did not see a statistically significant reduction of the TT-TG distance after ADT. An explanation for this lack of reduction of TT-TG distance is difficult, but it could be due to the use of different MRI scanners before and after surgery. The TT-TG distance is highly influenced by knee position and degree of flexion, and differences in leg position and size of the coil among institutions might have led to this confusing finding. 14
We found a statistically significant improvement in AP trochlear measurement on all 4 levels. Biedert and Bachmann 5 found a mean value of 77% in a group of knees with TD and a value of 73% in a group of normal knees. The AP trochlear measurement helps to reveal whether there is too much bone formation centrally proximal in the trochlea and/or whether the lateral trochlea is hypoplastic. Our findings at the proximal level, with a median value of 78.8% (range, 72.0%-84.0%) preoperatively and a median value of 73.7% (range, 69.5%-83.6%) postoperatively, seem comparable with the findings by Biedert and Bachmann; however, there were considerable individual variations.
The median LPI angle improved in a statistically significant manner from 20.7° to 14.7°; this result is in accordance with findings from Banke et al, 3 who found that the mean patellar tilt decreased from 24.2° before open trochleoplasty to 15.8° after the procedure.
Osteoarthritic changes are found in approximately 18% of patients at long-term follow-up after Bereiter trochleoplasty. 22 It is not known whether trochleoplasty accelerates the development of patellofemoral osteoarthritis by cartilage damage or whether this is the natural history of patients who have considerable TD. The findings from this midterm follow-up do not answer that question but do support the findings from Schöttle et al, 36 who observed no histologic or arthroscopic signs of arthritic changes after trochleoplasty. Schmeling 35 reported that in a series of 488 open trochleoplasties during a 17-year period, no cases had converted to joint replacement, even though the majority of patients already had existing cartilage damage at the time of the operation and some had significant cartilage damage (Outerbridge grade 3 to 4).
Criticism has been raised that the ADT procedure might be insufficient compared with the open Bereiter technique, because a straight shaver bur would have difficulty reaching the more distal part of the trochlea due to its curvature. We have included measurement of the length of the ADT and the extent to which the ADT procedure reached the more distal aspect of the trochlear groove. No other studies have reported on these measurements, and we are uncertain about their importance. We included the measurements because of skepticism among surgeons who perform open trochleoplasty as to whether it is technically possible to reach far enough distal with the ADT technique.
The mean length of the ADT was 26.5 mm and the mean extent of the trochleoplasty was 9.5 mm from the notch. Those figures indicate that the ADT might extend sufficiently distal; however, no comparable data are available on open trochleoplasties. Furthermore, it has been stated that only the most proximal part of the trochlear groove, the part that represents the trochlear prominence, needs to be deepened and that a more distal deepening might be pointless and unwanted. 40
Many MRI measurements have been used to investigate TD. 30 We chose the measurements in the present study based on several reasons. Cho et al 12 applied an artificial computer neural network to perform a quantitative classification of TD on computed tomography scans of a mixture of 25 normal and dysplastic knees. Those investigators found that trochlear depth, central anterior posterior distance divided by width (Biedert and Bachmann 5 ), and LTI angle were the most important parameters for assessing TD.
In the current study, the BPII 2.0 score showed statistically significant and clinically relevant improvement, from 37.2 preoperatively to 74.3 postoperatively. This corresponds to the results from a case series of mixed surgeries after failed MPFL-R and a control group of similar procedures in nonrevision cases, where Zimmermann et al 46 found that the BPII 2.0 score increased from 28.6 to 68.0 in the revision group and from 43.8 to 75.5 in the control group. In a case series of open trochleoplasty and MPFL-R, Mengis et al 25 found that the BPII 2.0 score increased from 46.5 preoperatively to 80.4 postoperatively. We found statistically significant improvements in KOOS and Kujala scores, which were comparable to 2 case series from Blønd 6 and Blønd and Haugegaard 8 on combined ADT and MPFL-R.
Limitations
The study was limited by several factors. Most important, the lack of standardization of the preoperative MRI scans introduces a bias because the pre- and postoperative MRI scans might not be directly comparable. Our finding of increased cartilage thickness after ADT might be attributable to any of several reasons, such as the use of different measurement points (despite efforts to avoid this), edema in the cartilage, or some kind of regeneration of cartilage thickness as observed in the medial knee compartment after high tibial osteotomy to correct varus deformity. As demonstrated by Egund et al, 14 the TT-TG distance is a variable figure and is sensitive to leg position. It is a well-known phenomenon among radiologists that TT-TG varies substantially from one MRI scanner to another, due to different leg positions and coil sizes. To optimize reliability of axial measurements, we calculated the distance from the notch to the most proximal trochlear cartilage, standardizing the level of the 4 measurements. Other limitations were that no control group was included, a clinical examination at the follow-up was omitted due to the COVID-19 situation during this period, and the number of included patients was too low to evaluate the safety of this procedure as well as the risk of continuous instability.
Conclusion
Combined ADT and MPFL-R led to statistically significant improvements of standardized MRI measurement that characterize TD and clinically relevant improvements in patient-reported outcomes. The improvements correspond to those obtained by open trochleoplasty. No significant reduction in cartilage thickness was seen. This study provides data to indicate that ADT in combination with MPFL-R is feasible and is capable of significantly improving the abnormalities that characterize TD; however, the trochlear configuration is not normalized. Patients can expect to achieve statistically significant and clinically relevant improvement. The procedure does not seem to induce cartilage thinning at midterm follow-up.
Footnotes
Final revision submitted January 18, 2023; accepted February 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Magnetic resonance imaging scanning facilities were provided by Aleris Private Hospital. L.B. has received consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the regional ethics committee of the Greater Copenhagen area (reference No. 21296).