
Abstract
Background:
Developmental dysplasia of the hip (DDH) and trochlear dysplasia (TD) are distinct pathologies with several important features in common. In addition to shared risk factors, both forms of dysplasia cause abnormal joint kinematics and force transmission, predisposing patients to pain, injuries to cartilage and soft tissue stabilizers, and ultimately arthritis.
Purpose:
To evaluate for an association between hip dysplasia and TD in skeletally mature patients with symptomatic hip dysplasia.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 48 patients with DDH who underwent periacetabular osteotomy were compared with 48 sex-matched patients who underwent hip arthroscopy for femoroacetabular impingement (FAI) between July 2014 and February 2021. All patients were skeletally mature. The Tönnis angle and lateral center-edge angle were measured on preoperative pelvis radiographs. Femoral version, trochlear depth, lateral trochlear inclination (LTI), tibial tubercle–trochlear groove distance (TTTG-d), and posterior lateral condylar angle (PLCA) were measured on preoperative magnetic resonance imaging scans of the symptomatic hip and ipsilateral knee. Continuous variables were compared between the patient groups using 2-sample t tests. Interobserver reliability was measured using the intraclass correlation coefficient.
Results:
Patients with DDH demonstrated a reduced trochlear depth compared with patients with FAI (3.6 vs 4.6 mm; P < .001). There were no differences between groups in femoral anteversion, LTI, TTTG-d, or PLCA. Two (4.2%) patients with FAI and 17 (35.4%) patients with DDH had a trochlear depth <3 mm (P < .001). One (2.1%) patient with FAI and 7 (14.6%) patients with DDH had an LTI <11° (P = .027). There was no difference between groups in frequency of a convex proximal trochlea, patient-reported ipsilateral knee pain, or ipsilateral knee procedures.
Conclusion:
Patients with DDH had reduced trochlear depth compared with patients with FAI, demonstrating a higher incidence of dysplastic trochlear features that may predispose patients to patellofemoral joint disease. Further research is needed to determine whether screening at-risk patients and treating TD will help to prevent symptomatic patellofemoral disease.
Developmental dysplasia of the hip (DDH) and trochlear dysplasia (TD) of the knee are distinct pathologies that share common risk factors, including female sex, family history, and history of breech position.1,19,20,26 Both DDH and TD predispose patients to pain, instability, and arthritis.1,10 A recent study examining ultrasound images of newborns showed that newborns with DDH were 2.4 times more likely to have TD, although it is unknown if this association persists into adulthood. 9
DDH research over the past several decades has been extraordinarily successful in identifying patients at risk and intervening, through either nonoperative treatment (bracing) or open reduction, in altering the natural history of the pathology. 24 The prevalence of DDH has been reported at 5 to 50 cases per 1000 hips.4,24 Effective protocols for referral and ultrasound screening identify DDH early. Nonoperative interventions alter natural history and reduce the risk or severity of arthritis and risk of early arthroplasty. 24
In contrast, TD has not received the same research focus or attention despite a high prevalence of approximately 10% in adults. 8 TD is an important risk factor for recurrent patellar instability and patellofemoral pathology. 11 In addition to sharing similar risk factors with DDH, the cartilaginous trochlea, like the developing acetabulum, has demonstrated an age-dependent capacity to remodel. 25
Despite high prevalence, early referral, and effective screening, protocols are not widely implemented despite shared risk factors and validated ultrasound measurements of the patellofemoral joint in pediatric patients. DeVries et al 9 built on work from the pediatric literature establishing and validating ultrasound as a valuable diagnostic tool for imaging the patellofemoral joint in infancy and childhood. The shape of the cartilaginous trochlea in infancy is similar to that of adults and can be accurately and reliably measured using ultrasound.13,14,16-18,20 Several magnetic resonance imaging (MRI) measurements have been validated for the evaluation of TD in adults. 21 Previously published works have established normal MRI values for trochlear depth and lateral trochlear inclination (LTI). On axial MRI scans, a trochlear depth ≤3 mm is highly sensitive and specific for TD. 23 Similarly, an LTI ≤11° on axial MRI has excellent sensitivity and specificity for patellar instability. 6
At our institution, patients with DDH or femoroacetabular impingement (FAI) routinely undergo preoperative MRI of the affected hip that includes images of the ipsilateral knee for the purpose of assessing femoral version. The knee MRI sequence is a T1-weighted axial sequence that enables us to assess validated features of TD. 21 The purpose of this study was to determine whether DDH is associated with TD in skeletally mature patients by evaluating the incidence of validated features of TD on MRI in patients with DDH. We hypothesized that there would be a significant association between radiographic features of DDH and TD in skeletally mature patients.
Methods
Institutional review board approval was obtained before initiating this retrospective review of medical records, and all included patients provided written informed consent. A power analysis was performed to estimate the needed sample size. Based on an assumption of a 20% change in the value of continuous variables used to measure trochlear and hip dysplasia, a sample size of 86 (43 per group) was calculated for the study.
Study Groups
A total of 48 skeletally mature patients who underwent periacetabular osteotomy (PAO) for DDH were matched by sex to 48 skeletally mature patients who underwent arthroscopic femoral osteoplasty for cam FAI. All 96 patients were seen by a single surgeon (S.Y.P.) at the hip preservation clinic for the chief complaint of hip pain. Patients with FAI were chosen for comparison, as both patient populations routinely undergo the same MRI protocol, including an axial sequence of the knee to assess femoral anteversion. No patients were excluded. All surgeries occurred between July 2014 and February 2021.
The patients with DDH were indicated for PAO for the diagnosis of acetabular dysplasia with undercoverage of the femoral head in the absence of arthritic changes of the hip, and a Bernese PAO was performed after they reached skeletal maturity to improve anterolateral coverage of the femoral head. Patients with FAI were used as the comparison group, as there was not a sample of patients with developmentally normal hips with the necessary MRI available for comparison. Patients with FAI were indicated for arthroscopic cam resection on the basis of cam or combined-type FAI, for failure of nonoperative treatment, and after reaching skeletal maturity. Sex matching was performed to minimize the effect of anatomic differences sometimes seen between women and men as a confounding variable.
Study Variables
Patient charts were retrospectively reviewed for any history of knee pain, instability, or injury at, or before, the time of their preoperative appointment. Patients were not excluded for a history of prior knee pain, injury, or surgery. Preoperative radiographs of the pelvis and MRI scans of the symptomatic hip and ipsilateral knee were retrospectively reviewed by 2 authors (A.T.F. and K.G.S.) for features of DDH and TD (Figure 1). Reviewers were not blinded to the diagnosis of DDH. As the patients in both study groups were seen at the clinic for hip pain, they did not undergo routine radiographic examination of the knee, so Dejour classification of TD was not possible for this study. As part of the new patient consultation, patients were asked general questions about their knee, including if they had a history of ipsilateral knee pain, injury, or surgery. They were not asked specifically about a history of patellar instability.

Representative (A) pelvic radiograph and (B) axial T1-weighted magnetic resonance imaging scan obtained in a patient with right hip dysplasia and ipsilateral trochlear dysplasia.
For DDH features, the lateral center-edge angle (LCEA) and Tönnis angle were measured on anteroposterior pelvic radiographs, and the anterior center-edge angle (ACEA) was measured on false-profile radiographs. For TD features, trochlear depth, LTI, tibial tubercle–trochlear groove distance (TTTG-d), femoral anteversion, and posterior lateral condylar angle (PLCA) were measured using axial T1-weighted MRI scans. Although patella alta is an important risk factor for patellar instability and patellofemoral symptoms, sagittal sequences were not available to measure this parameter and could not be reconstructed from the archived images.
Axial T1-weighted sequences of the knee and hip joints were used for all MRI measurements (Figure 2). Lateral knee radiographs were not available to review Dejour classification. LTI and trochlear depth were measured on the most proximal axial image with full cartilage coverage of the medial and lateral trochlear facets using the posterior condylar axis as reference. Measurements were made using the height and angle of the cartilage facets rather than the subchondral bone as the cartilage is a better representation of the joint surface. Cutoffs <11° (LTI) and <3 mm (trochlear depth) were used to diagnose TD.6,23 PLCA is determined by measuring the transepicondylar axis at the level of the lateral epicondyle and measuring the angle to the posterior lateral condyle. TTTG-d was measured as the lateral offset of the midpoint of the patellar tendon insertion at the tibial tubercle from the trochlear groove on the most proximal image where both medial and lateral trochlear facets were covered by cartilage using the posterior condylar axis as a reference.
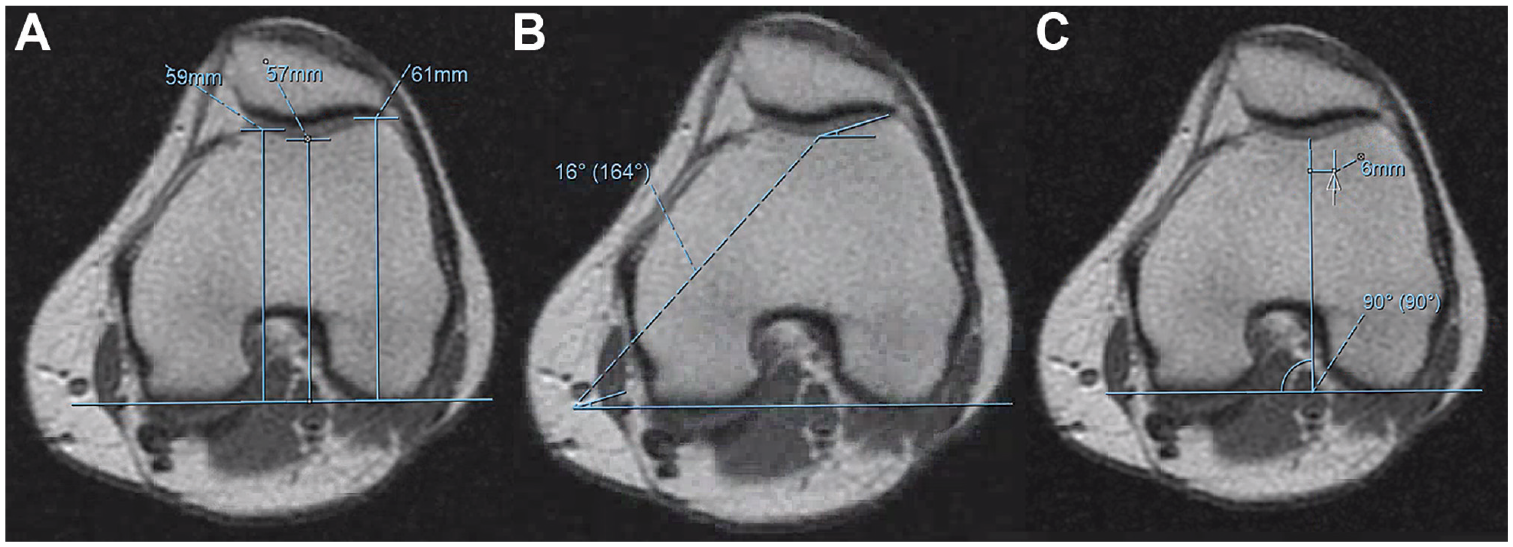
Representative magnetic resonance imaging measurements at the knee. (A) Trochlear depth is measured as the difference between the mean height of the cartilaginous facets and the height of the cartilaginous groove relative to the posterior condylar axis. (B) Lateral trochlear inclination is the angle between the cartilage of the lateral facet and the posterior condylar reference axis. (C) Tibial tubercle–trochlear groove distance is the distance between the midpoint of the insertion of the patellar tendon on the tibial tubercle and the trochlear groove measured parallel to the posterior condylar reference axis. All trochlear measurements were performed at the most proximal axial image where both facets are completely covered by cartilage.
Statistical Analysis
Descriptive statistics are reported with means and standard deviations for continuous variables and with counts and percentages for categorical variables. Two-sample t tests were used to analyze demographic, clinical, and radiographic differences between the DDH and FAI groups. All analyses were run in RStudio Version 1.1.456 (RStudio Team, http://www.rstudio.com/) using a 2-sided level of significance of .05.
Ten patients with DDH and 10 patients with FAI were randomly selected for repeat measurements for trochlear depth, LTI, and TTTG-d, and the intra- and interobserver reliabilities of the MRI measurements were calculated using the intraclass correlation coefficient (ICC). The repeat measurements were performed by a senior resident physician (A.T.F.) and a senior attending physician (K.G.S.) using predetermined axial T1 slices. 2
Results
There were no differences between patients with DDH and FAI in age, sex distribution, or height. The patients in the DDH group had a higher mean weight (75.3 vs 66.9 kg; P = .017) and BMI (27.3 vs 23.8 kg/m2; P = .002) than those in the FAI group. There were no significant differences between groups in surgery- or injury-related characteristics (Table 1). Regarding intraobserver reliability of the MRI measurements, moderate reliability was found for trochlear depth (ICC, 0.55) and good reliability was found for LTI (ICC, 0.81) and TTTG-d (ICC, 0.82). For interobserver agreement, poor reliability was found for trochlear depth (ICC, 0.27), moderate reliability for LTI (ICC, 0.54), and good reliability for TTTG-d (ICC, 0.78).
Data for Patients With DDH and FAI a

Data are reported as mean [SD] or n (%). Boldface P values indicate a statistically significant difference between groups (P < .05). DDH, dysplasia of the hip; FAI, femoroacetabular impingement.
Patients with DDH had reduced trochlear depth compared with patients with FAI (3.6 mm vs 4.6 mm; P < .001) (Figure 3). Hip-specific measurements showed that patients with DDH had decreased LCEA (13.5° vs 28.5°; P < .001), decreased ACEA (13.1° vs 29.5°; P < .001), and increased Tönnis angle (16.3° vs 6.0°; P < .00001) compared with patients with FAI (Figure 4). There was no difference in mean LTI between groups (17.4° vs 19.3°; P = .072) (Figure 4). No patients in either group had a supratrochlear spur.
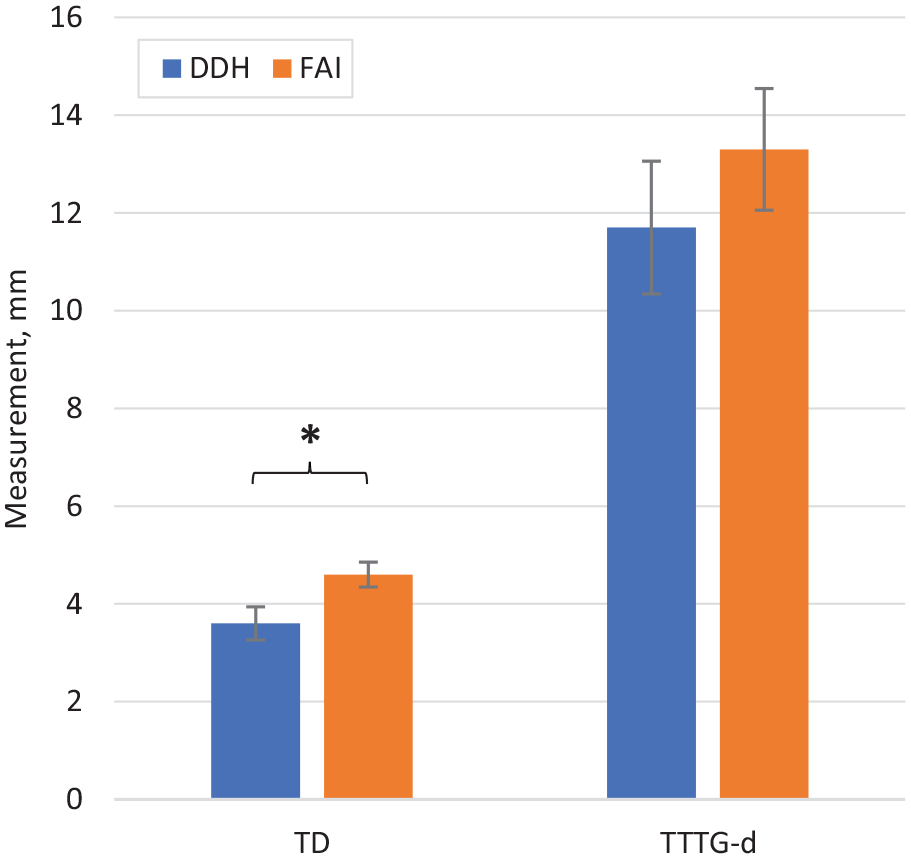
Dysplasia of the hip (DDH) and femoroacetabular impingement (FAI) group mean measurements for trochlear depth (TD) and tibial tubercle–trochlear groove distance (TTTG-d). Error bars indicate standard error of the mean. *P < .001.

Dysplasia of the hip (DDH) and femoroacetabular impingement (FAI) group measurements for lateral trochlear inclination (LTI) and posterior lateral condylar angle (PLCA). Error bars indicate standard error of the mean.
The incidence of TD on axial MRI differed significantly between groups (Figure 5). Two (4.2%) patients with FAI and 17 (35.4%) patients with DDH had a trochlear depth <3 mm (P < .001). No patients in either group had convex proximal trochlea (trochlear depth, <0 mm). One (2.1%) patient with FAI and 7 (14.6%) patients with DDH had an LTI <11° (P = .027). Each of the 8 total patients with an LTI ≤11° (1 patient with FAI, 7 patients with DDH) also had a trochlear depth ≤3 mm.

Percentage of each group with abnormal radiographic measurements for trochlear dysplasia (TD), lateral trochlear inclination (LTI), and both borderline and elevated tibial tubercle–trochlear groove distance (TTTG-d). Error bars indicate standard error of the mean. *P < .05.
There were no differences between patient groups for femoral anteversion, PLCA, TTTG-d, or incidence of knee pain (Table 2). There were no differences between patient groups for self-reported history of knee arthroscopy (3 patients with FAI, 2 patients with DDH) or knee pain (9 patients with FAI, 8 patients with DDH) preoperatively.
Comparison of Radiographic Measurements by Patient Group a

Data are shown as mean ± SD (95% CI). Boldface P values indicate a statistically significant difference between groups (P < .05). ACEA, anterior center-edge angle; DDH, dysplasia of the hip; FAI, femoroacetabular impingement; LCEA, lateral center-edge angle; LTI, lateral trochlear inclination; PLCA, posterolateral condylar angle; TD, trochlear dysplasia; TTTG-d, tibial tubercle–trochlear groove distance.
Discussion
Our results demonstrated that adult patients with DDH are more likely to have features of TD on MRI, specifically, reduced trochlear depth and reduced LTI. Reduced trochlear depth and reduced LTI represent decreased passive constraint to lateral patellar dislocation and are validated features of TD that predispose patients to patellofemoral joint disorders including lateral patellar instability.1,6,21,23 To our knowledge, this is the first study to use MRI to explore an association between DDH and TD in the skeletally mature population.
A 1-mm change in trochlear depth between patients with DDH and FAI is a small absolute difference but a significant 21% change between groups. Our results are comparable to recently published 3-dimensional volumetric data, which showed a 1.8-mm difference in trochlear depth between patients with symptomatic TD and normal controls. 22 Our methods differ somewhat from those of Pennock et al 22 in that we compared cartilaginous trochleae as opposed to bony trochleae. Furthermore, the difference in the percentage of patients with radiographically abnormal trochlear depth and LTI between groups is statistically significant.
While there was not a statistically significant difference in mean LTI between groups, there was a significant difference in the percentage of patients with abnormally low LTI. LTI represents passive constraint to lateral dislocation. LTI has previously been proposed as being diagnostic of TD, although it has been shown to correlate better with higher Dejour grades of TD than with lower grades. 15 Each of the 8 patients with LTI ≤11° (1 patients with FAI and 7 patients with DDH) also had a trochlear depth ≤3 mm. As such, LTI may be more specific and less sensitive than trochlear depth in the diagnosis of TD.
Risk factors for patellar instability outside of TD include patella alta, elevated tibial tubercle–trochlear groove offset, and patient age. 11 TD is also associated with degenerative changes in the patellofemoral joint. 12 These associations merit further study to improve the evaluation and treatment of symptomatic patellofemoral disease.
MRI has been reported to underestimate femoral anteversion compared with computed tomography, which may help to explain why there was no difference between groups in our study. 5 In the study population, there was no association between the radiographic features and clinical symptoms of TD.
Our data build on recently published data demonstrating a similar association between DDH and developmental TD in newborns and infants. 9 Subclinical TD can be present in patients with DDH and potentially contribute to patellofemoral joint disease over time. MRI-based studies have shown that remodeling of TD is possible after medial patellofemoral ligament reconstruction in certain age groups.3,7,25 If the trochlea can be remodeled under these conditions, then it may be feasible to use nonoperative interventions such as bracing and activity modifications to successfully treat TD and prevent the development of patellofemoral pain or patellar instability.
Similar to the rationale behind early treatment of DDH, early identification of TD before the development of patellofemoral instability or pain might allow for trochlear remodeling through noninvasive bracing to prevent the development of symptoms. It may be worthwhile to screen for patellofemoral joint pathology during the evaluation of hip dysplasia even if knee pain is not the patient's chief concern. Screening questions may include history of patellar instability, maltracking, and knee pain. Patients who screen positive for symptoms of TD may be considered for focused clinical evaluation of the patellofemoral joint and, if appropriate, dedicated imaging of the patellofemoral joint with radiographs and MRI scans.
Limitations
There are several important considerations that limit the generalizability of the study results, including its retrospective nature, suboptimal interobserver reliability of measurements, and use of patients with FAI as a comparison group. Differences in weight and BMI were seen between groups, which reflects that these groups represent distinct underlying patient populations. Poor interobserver reliability was seen for measurements of trochlear depth, LTI showed moderate reliability, and good reliability was seen for TT-TG. Our interobserver reliability stands in contrast to previous studies showing good reliability of these measurements for the assessment of the patellofemoral joint. 23 Asymptomatic controls with developmentally normal hips and the required MRI were unavailable in sufficient numbers to use as controls for this study. We also did not have assessments of sulcus angle or Dejour classification. Assessment of history of knee pain and function was limited to a general questionnaire at the time of the new patient consultation and did not specifically include history of patellar instability. Patients with hip dysplasia were not routinely screened for knee pain but were queried if they had any other joint pain or prior surgeries on initial evaluation for hip pain; thus, the incidence of prior history of knee pain or patellar instability may be underestimated. As this patient population was evaluated and treated for predominantly hip-based symptoms, patients did not undergo plain radiographs of the knee, which would help to evaluate for TD, including formal classification based on the Dejour classification of TD.
Conclusion
Patients with DDH were more likely to have features of TD on axial MRI than patients with FAI. Further research is needed to confirm if patients with hip dysplasia have a higher incidence of patellofemoral disease.
Footnotes
Final revision submitted May 7, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.T.F. has received education payments from Evolution Surgical. S.L.S. has received education payments from Evolution Surgical and Elite Orthopedics; consulting fees from Bioventus, DJO, Kinamed, Linvatec, Olympus America, Ceterix Orthopaedics, Pacira Therapeutics, Smith & Nephew, Vericel, JRF Ortho, LifeNet Health, and Flexion Therapeutics; nonconsulting fees from Arthrex, Linvatec, Smith & Nephew, and Synthes GmbH; royalties from Linvatec and ConMed; hospitality payments from Aesculap Biologics; and honoraria from Flexion Therapeutics, JRF Ortho, and Vericel. K.G.S. has received education payments from Evolution Surgical and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Stanford University (No. 5136).