
Abstract
Background:
Research on surgical strategies to minimize tunnel collisions in combined anterior cruciate ligament (ACL) reconstruction (ACLR) using the modified transtibial technique (MTT) and anterolateral augmentation is limited, unlike with independent tunnel drilling techniques.
Purpose:
To analyze the optimal drill orientations for the anterolateral ligament (ALL) femoral tunnel to minimize tunnel collisions and reduce damage to surrounding structures during combined ACLR with MTT and anterolateral augmentation procedures, accounting for far-cortex drilling (FCD) of the ALL femoral tunnel required for graft fixation.
Study Design:
Descriptive laboratory study.
Methods:
Three-dimensional reconstructed femoral models of patients who underwent ACLR with MTT between 2015 and 2018 were used. Geometric factors of femoral models were analyzed, and virtual ALL femoral tunnels were simulated to evaluate 45 drilling combinations. To assess potential damage to surrounding structures associated with ALL femoral tunnel drilling, femoral cortical violation caused by the ALL femoral tunnel itself was assessed under each drilling condition, whereas tunnel trajectories were analyzed to classify drilling conditions according to FCD. In addition, the minimum distance between the ACL and ALL femoral tunnels (MDBT) and the tunnel collision rate were evaluated.
Results:
A total of 27 patients were analyzed. In scenarios where FCD was not required for ALL graft femoral fixation, the optimal drill orientation for the ALL femoral tunnel was within the range of coronal −40° to −20°, eliminating cortex violation and tunnel collisions (mean MDBT, 9 ± 4.1 mm; collision rate 0%). When FCD was required for ALL graft femoral fixation, the optimal drill orientation was axial 40° and coronal 10°, resulting in the longest MDBT without the risk of femoral cortex violation (MDBT, 4.9 ± 3.5 mm; collision rate, 7.4%).
Conclusion:
During the combined surgeries for ACLR using MTT and anterolateral augmentation procedures, the optimal drill orientation of the ALL femoral tunnel was within the range of coronal −40° to −20° for techniques not requiring FCD and axial 40° and coronal 10° for those requiring FCD.
Clinical Relevance:
This study provides practical surgical guidance for optimizing ALL femoral tunnel orientation during combined ACLR using MTT and anterolateral augmentation. By accounting for whether FCD is required for ALL graft femoral fixation, the findings may help surgeons minimize tunnel collision and reduce the risk of femoral cortical violation, thereby potentially decreasing procedure-related complications.
Keywords
Tunnel collision is a relatively common complication observed during multi-ligament knee surgery.15,16 Because of the limited bone mass of the distal femur, collisions between tunnels can occur when ≥2 tunnels are created. Such collisions can damage the grafts and fixation devices, potentially leading to surgical failure.15,16 These collisions are particularly prevalent in simultaneous surgical procedures involving anterior cruciate ligament (ACL) reconstruction (ACLR) and anterolateral augmentation procedures (anterolateral ligament [ALL] reconstruction or lateral extra-articular tenodesis). As a result, several studies have been conducted to minimize the risk of tunnel collision during simultaneous ACL and anterolateral augmentation procedures, with a specific focus on the drill orientation for the ALL femoral tunnel.10,11,19,24,29,30,33
However, most previous studies analyzing tunnel collisions during ACLR and anterolateral augmentation procedures were based on anatomic ACLR,10,11,19,24,29,33 limiting their universal applicability across all ACL surgeries. Surgical techniques for ACLR include the transtibial approach and anatomic reconstruction methods, such as the transportal (anteromedial portal) or outside-in techniques. The transtibial technique uses a single tibial tunnel to guide the drilling of the femoral tunnel. In contrast, anatomic reconstruction involves independent femoral tunnels created via separate incisions or portals to allow for anatomic femoral tunnel placement. 25 While placing the femoral tunnel in an anatomic position during ACLR has biomechanical advantages, leading to increased utilization of transportal and outside-in techniques, the transtibial technique offers technical convenience and helps maintain graft isometry.25,34,36 Additionally, the modified transtibial technique (MTT), introduced relatively recently, addresses the limitations of the conventional transtibial technique by allowing the formation of an oblique femoral tunnel while maintaining the femoral tunnel close to the anatomic position.13,14,38,39
Nevertheless, no studies have yet analyzed the optimal drill orientation of the ALL femoral tunnel during ACLR using the MTT. The femoral tunnel created by the MTT has different geometric characteristics, such as tunnel length, inclination, and location, compared with those made by the transportal or outside-in techniques.21,22 Therefore, the findings of previous studies regarding tunnel collisions between the ACL and ALL femoral tunnel may not apply to cases involving the MTT. Given the ongoing increase in the frequency of anterolateral augmentation surgeries and the continued use of the MTT in ACLR,27,34-36 further research is needed to determine optimal surgical strategies to minimize tunnel collisions during combined ACLR using the MTT and anterolateral augmentation procedures.
Therefore, this study aimed to analyze the optimal drill orientations for the ALL femoral tunnel to minimize tunnel collisions and reduce damage to surrounding structures during combined ACL reconstruction with MTT and anterolateral augmentation procedures, accounting for far-cortex drilling (FCD) of the ALL femoral tunnel required for graft fixation. Given that various surgical techniques can be used for anterolateral augmentation procedures, and that the requirement for FCD depends on the fixation method (eg, FCD is generally required when suspensory fixation or certain types of interference screw fixation are used, whereas FCD is typically unnecessary when suture anchors are employed), we therefore sought to analyze drilling orientations separately depending on whether FCD was required.
Methods
This study was approved by the institutional review board, and informed consent was waived due to its retrospective nature. All methods were performed in accordance with the relevant guidelines and regulations—including the Declaration of Helsinki. Patients who underwent ACLR with the MTT during the period when this technique was routinely performed by a single senior surgeon (C.-H.C.) at our institution were included. In these cases, femoral graft fixation was performed using a femoral cross-pin fixation system (RigidFix; Depuy Mitek). Accordingly, the study population was limited to cases treated between March 2015 and February 2018. The inclusion criteria were as follows: (1) single-bundle ACLR performed using the MTT; (2) patients aged ≥18 years; and (3) postoperative computed tomography (CT) scans obtained within 1 week after surgery. Postoperative CT scans were performed in all patients who underwent ACLR at our institution, except those who declined the procedure. The scans were performed to evaluate surgical outcomes—including tunnel length, tunnel diameter, tunnel position, posterior wall blowout, and graft fixation status. Patients were excluded if any of the following criteria were met: (1) the use of surgical techniques other than the MTT; (2) revision ACLR; (3) the presence of osseous deformities in the affected lower limb; (4) concurrent surgical procedures for other ligament injuries; or (5) moderate to severe osteoarthritis (Kellgren-Lawrence grade >2).
Three-Dimensional Femur Model Reconstruction
A Sensation 64 scanner (Siemens Healthcare) was used for the CT scans, with the following tube parameters: 120 kVp and 135–253 mA. The imaging parameters included a slice thickness of 0.6 to 1 mm, a field of view of 134 to 271 mm, and an acquisition matrix of 512 × 512 pixels. Digital Imaging and Communications in Medicine data from CT scans were extracted from the Picture Archiving and Communication System (GE Medical Systems Information Technologies) and imported into Mimics software (Version 17; Materialize) for the segmentation of the 3-dimensional (3D) volumetric model of the femur.
Evaluation of the Geometric Factors
Using 3D-reconstructed femoral models, the ACL tunnel position was evaluated for height and depth. The femoral models were aligned according to a previously described method, and the medial femoral condyle was removed to expose the medial wall of the lateral femoral condyle. 17 A rectangular reference frame, defined by a line connecting the lowest point of the intercondylar notch and the outer margin of the lateral femoral condyle, was then used to determine tunnel height and depth (Figure 1A).17,18,37

(A) Evaluation of ACL tunnel position using a 3D-reconstructed femoral model. (B, C, D) Semi-automatic measurements of geometric factors, including the length of the ACL femoral tunnel, transepicondylar distance, volume of the distal femur, distance between the outlet of the ACL femoral tunnel and the femoral attachment of the ALL, and inclination angles of the ACL, observed in the (B) axial plane, (C) coronal plane, and (D) sagittal plane. ACL, anterior cruciate ligament; ALL, anterolateral ligament; 3D, 3-dimensional.
The analysis of geometric factors was conducted using a local coordinate setting. 19 The femoral long axis was determined by fitting a cylinder to the distal metaphysis, and the transepicondylar line connecting the medial and lateral epicondyles was established. The femoral model was rotated to align the transepicondylar line with the x-axis and the femoral long axis parallel to the z-axis on the sagittal plane. Based on this standardized orientation, key geometric parameters—including ACL femoral tunnel dimensions, distal femoral morphology, spatial relationships between the ACL tunnel and the ALL femoral attachment, and ACL inclination angles in the axial, sagittal, and coronal planes—were measured. ACL tunnel diameter and length were obtained using a semi-automated virtual cylinder that matched the existing femoral tunnel. The transepicondylar distance was measured along the transepicondylar line, and distal femoral volume was calculated below a reference plane at the level of the adductor tubercle. 8 The location of the femoral attachment of the ALL was determined to be approximately 8 mm proximal and 4.3 mm posterior to the lateral epicondyle on the outer cortex of the lateral femoral condyle in the sagittal plane. 5 The distance from the ACL femoral tunnel's outlet to the femoral attachment of the ALL was quantified as the distance between the center of the ACL femoral tunnel's outlet and the femoral attachment of the ALL. ACL inclination angles in the axial, sagittal, and coronal planes were calculated relative to the femoral reference axes (Figure 1, B, C, and D).
The test-retest reliability of the measurements was evaluated by repeatedly reconstructing the 3D femur model and measuring the specified variables in 2 consecutive sessions separated by a 3-week interval. A single experienced observer (J.L.), who was blinded to the patient information, performed these procedures. The mean of the 2 measured values for each variable was used to analyze the geometric factors.
Simulation of the ALL Femoral Tunnel
To simulate different orientations of the ALL femoral tunnel, a novel local coordinate system was established, distinct from the geometric factor evaluation. In clinical practice, the ALL femoral tunnel is typically drilled from its femoral attachment, using the medial epicondyle as a reference point for orientation. Thus, the neutral axis of drilling for the ALL femoral tunnel was defined as the line connecting the medial epicondyle and the femoral attachment of the ALL, denoted as 0° in the axial and coronal planes. To align the neutral axis with the x-axis, the femur model was rotated, and in the sagittal plane, the long axis of the femur was aligned parallel to the z-axis. For simulation purposes, a virtual representation of the ALL femoral tunnel was created as a cylinder with a 6-mm diameter and 30-mm length, to accommodate the largest tunnel size used by surgeons.2,7,9,26,32 Utilizing the neutral axis as a reference, simulations of the virtual ALL femoral tunnel were performed with angular variations in the axial plane ranging from 0° to 40° at intervals of 10°, and in the coronal plane from –40° to 40°. The maximum angulation of the ALL cylinder was limited to ±40°, as drilling at angles exceeding 40° may result in elliptical tunnels and cortical thinning. 15 Additionally, to avoid violating the posterior femoral cortex, only positive angles were considered for the orientation of the ALL cylinder in the axial plane. As a result, 45 drilling conditions were simulated for each patient. These 45 drilling combinations were designed to encompass the full range of clinically applicable orientations for the ALL femoral tunnel, and a similar analytical approach has previously been employed in a study to identify the optimal drilling orientation in anatomic ACL reconstruction. 19
For each drilling condition, the potential violation of the femoral cortex by the ALL cylinder and its corresponding FCD trajectory were examined. Furthermore, the minimum distance between the ACL and ALL femoral tunnels (MDBT) was measured. Femoral cortex violation by the ALL femoral tunnel was considered present if the ALL cylinder breached the femoral cortex. In contrast, exposure within 5 mm from the entrance of the ALL femoral tunnel was not classified as a violation (Figure 2A). The violation of the femoral trochlea or intercondylar notch by the trajectory of the ALL cylinder representing FCD was assessed by evaluating whether the central axis of the ALL cylinder passed through them (Figure 2B). The MDBT was defined as the shortest distance between the central axes of the ACL and ALL femoral tunnels, minus the sum of their respective tunnel radii (Figure 2C). This value was automatically calculated using Mimics software. A negative MDBT value indicated overlap between the 2 tunnel cylinders, corresponding to an actual tunnel collision. In addition, tunnel collision was also evaluated by applying a 2-mm safety threshold to the MDBT, based on a previous study suggesting that a minimum 2-mm bony bridge is necessary to avoid tunnel weakening or compromise. 15

A total of 45 drilling conditions were implemented for each femoral model. Evaluation was performed on (A) femoral cortex violation by the ALL cylinder for each drilling condition, (B) violation of the femoral trochlea or intercondylar notch by the trajectory of the ALL femoral tunnel (red line indicates penetration of the femoral trochlea, and blue line indicates cases with no penetration), and (C) the MDBT between the ACL femoral tunnel and ALL femoral tunnel.
Statistical Analysis
The statistical analyses were conducted using IBM SPSS Statistics for Windows (Version 26.0; IBM). A repeated-measures analysis of variance (ANOVA) was employed to examine changes in MDBT according to variations in the drill orientation of the ALL femoral tunnel. Post hoc pairwise comparisons were performed with adjusted P values obtained through Bonferroni corrections. The Cochran Q test was used to compare the occurrence of tunnel collisions and femoral cortex violations across drill orientations for the ALL femoral tunnels. Intraobserver reliability was assessed using intraclass correlation coefficients with a 95% CIs. Significance level was set at P < .05. Additionally, a post hoc power analysis for ANOVA was conducted using G*Power (Version 3.1.9.2; Heinrich-Heine-Universität, Düsseldorf), based on the final number of patients included in the study, with a significance level of 5%.
Results
Demographic and Geometric Characteristics
A total of 27 patients were included in this study. The demographic and geometric characteristics of the patients included in this study are presented in Table 1. The intraobserver reliability for the 3D reconstruction process and measurements ranged from 0.939 to 0.999.
Demographic and Geometric Characteristics of the Included Patients a
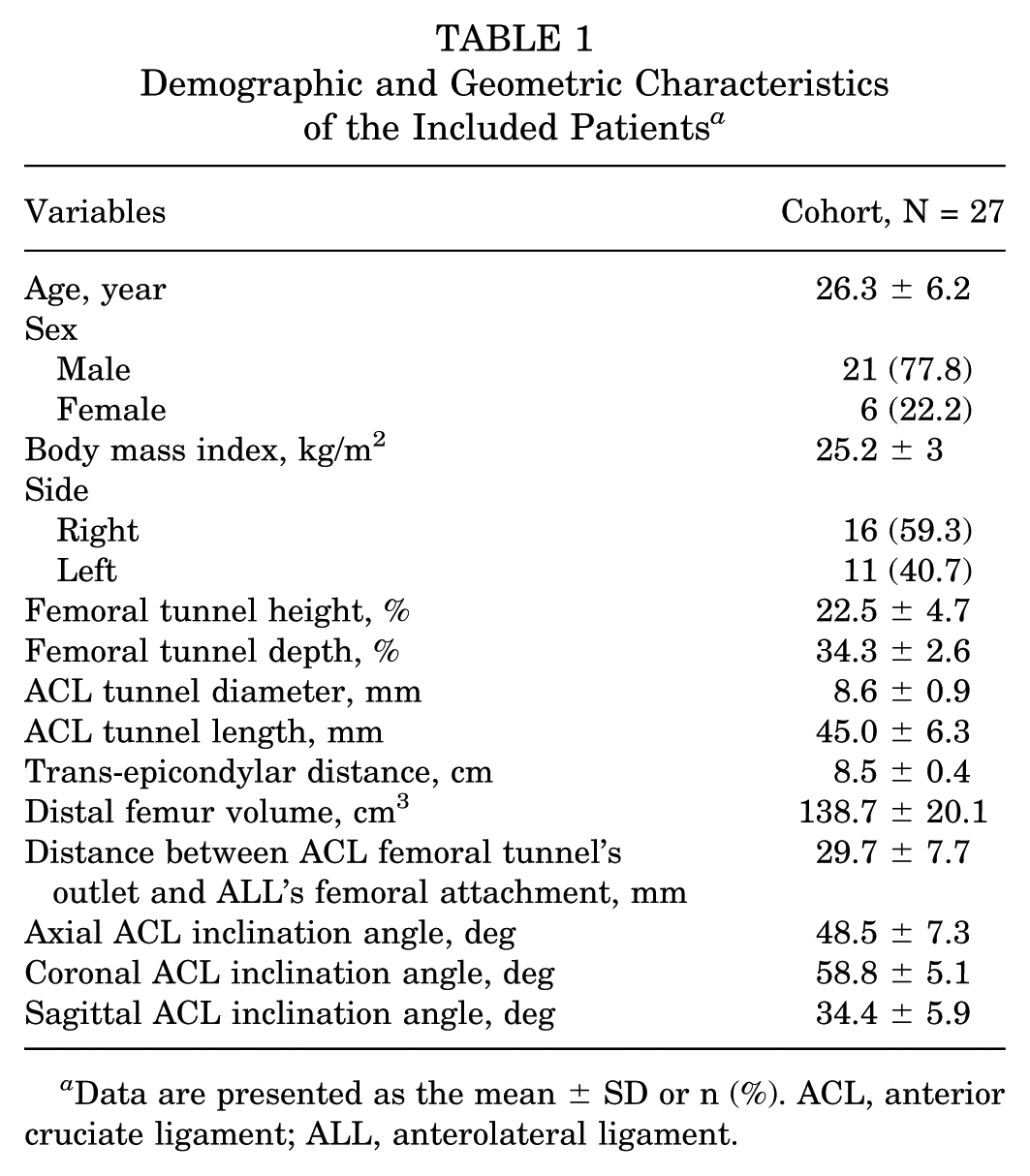
Data are presented as the mean ± SD or n (%). ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Assessment of Femoral Cortex Violation and Tunnel Trajectory Violation
The overall rate of femoral cortex violation caused by the virtual ALL femoral tunnel was 13.7% (166/1215), with no observed violations when the orientation of the ALL cylinder was ≤10° in the coronal plane (Table 2). There were no instances of trochlea or intercondylar notch violation caused by the virtual ALL femoral tunnel.
Violation Rates of the Virtual ALL Femoral Tunnels to the Cortex of the Femur a

Data are presented as %, unless otherwise indicated. ALL, anterolateral ligament.
Relative angle to the neutral axis, determined by a line connecting the femoral attachment of the ALL and the medial epicondyle of the femur.
P values for comparing different drill angles of the axial plane in the fixed coronal plane.
P values for comparing different drill angles of the coronal plane in the fixed axial plane.
The overall violation rate of the femoral trochlea or intercondylar notch resulting from the trajectory of the ALL femoral tunnel, representing FCD, was 38.7% (470/1215). No violations were observed with the trajectory of the ALL femoral tunnel for the femoral trochlea or intercondylar notch when the ALL cylinder was oriented ≥10° in the coronal plane (Table 3).
Violation Rates of the Virtual ALL Femoral Tunnel Trajectories to the Femoral Trochlea or Intercondylar Notch a
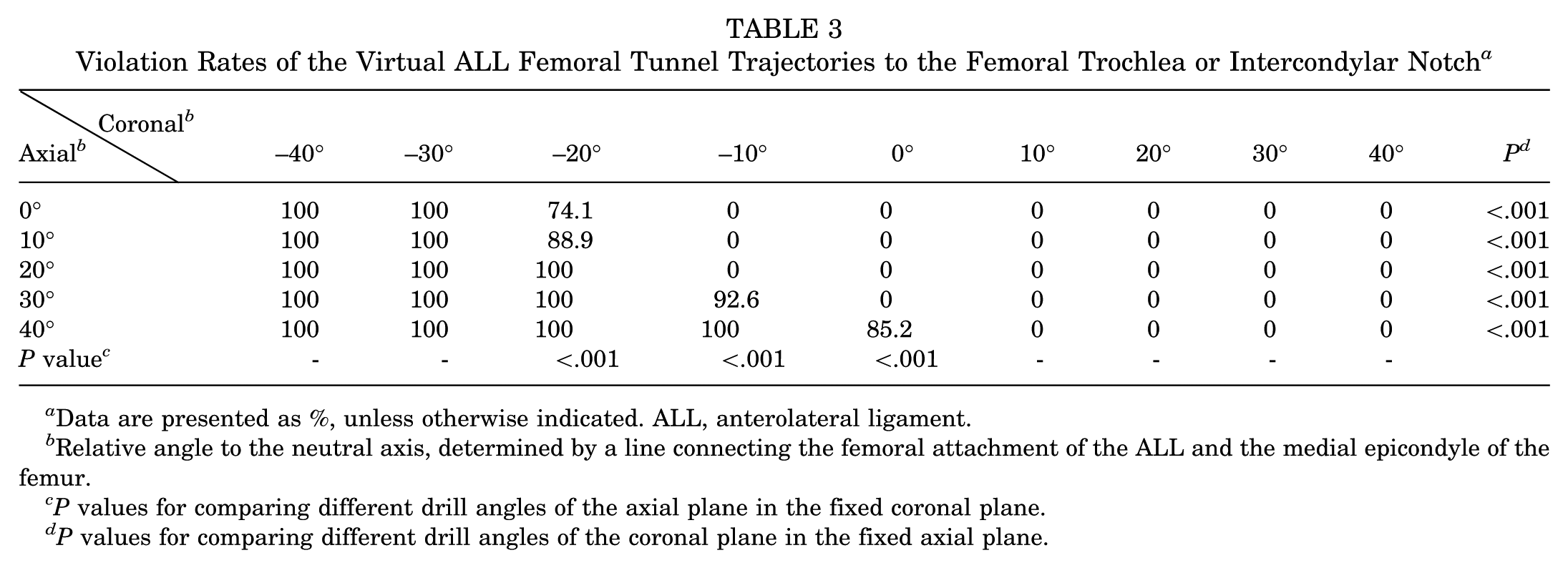
Data are presented as %, unless otherwise indicated. ALL, anterolateral ligament.
Relative angle to the neutral axis, determined by a line connecting the femoral attachment of the ALL and the medial epicondyle of the femur.
P values for comparing different drill angles of the axial plane in the fixed coronal plane.
P values for comparing different drill angles of the coronal plane in the fixed axial plane.
MDBT and Tunnel Collision
Significant differences in MDBT and collision rates were observed between the tunnels as the orientation of the virtual ALL tunnel changed in both the coronal and axial planes (Tables 4 and 5; Appendix 1 and 2). The MDBT was longest when the orientation of the ALL femoral tunnel was at coronal –40° and axial 40°, and no tunnel collisions were observed when the orientation of the ALL femoral tunnel was within the range of coronal –40° to –20° (mean MDBT, 9 ± 4.1 mm; 0% collision) (Figure 3A) (Tables 4 and 5). At coronal orientations of the virtual ALL cylinder ≥10°, where femoral cortex violation by the ALL tunnel trajectory was not observed, the longest MDBT with the lowest tunnel collision rate was observed at an axial angle of 40° and a coronal angle of 10° (MDBT, 4.9 ± 3.5mm; collision rate 7.4%) (Figure 3B) (Tables 2, 3, 4, and 5). Because no collision-free combination of angles existed under FCD-required conditions, a continuous safe range comparable to that identified in the non-FCD condition could not be established. Additionally, the analysis with a 2-mm clearance between the tunnels yielded consistent results (Appendix 3). Post hoc power analyses demonstrated statistical power greater than 0.99 across the evaluated comparisons.
Minimal Distance Between the ACL Femoral Tunnel and the Virtual ALL Femoral Tunnel a

Data are presented as mean ± SD, unless otherwise indicated. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Relative angle to the neutral axis, determined by a line connecting the femoral attachment of the ALL and the medial epicondyle of the femur.
P values for comparing different drill angles of the axial plane in the fixed coronal plane.
P values for comparing different drill angles of the coronal plane in the fixed axial plane.
Collision Rates Between the ACL Femoral Tunnel and the Virtual ALL Femoral Tunnel a

Data are presented as %, unless otherwise specified. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Relative angle to the neutral axis, determined by a line connecting the femoral attachment of the ALL and the medial epicondyle of the femur.
P values for comparing different drill angles of the axial plane in the fixed coronal plane.
P values for comparing different drill angles of the coronal plane in the fixed axial plane.

Optimal drill orientations for the ALL femoral tunnel to minimize tunnel collision with the ACL femoral tunnel created by the MTT and to reduce potential damage to surrounding structures based on the need for FCD. (A) In cases where FCD is not required, the recommended drill direction range is –40° to –20° in the coronal plane (blue cylinders). (B) In cases where FCD is necessary, the recommended drill directions are axial at 40° and coronal at 10° (orange cylinder). ACL, anterior cruciate ligament; ALL, anterolateral ligament; FCD, far-cortex drilling; MTT, modified transtibial technique.
Discussion
The most important finding of this study was the identification of optimal drill orientations for the ALL femoral tunnel that minimize tunnel collisions and reduce damage to surrounding structures during ACLR using the MTT, with relatively wide acceptable ranges: coronal −40° to −20° for techniques not requiring FCD, and axial 40° and coronal 10° for those requiring FCD. These findings could provide insights into the optimal surgical strategies to avoid tunnel collisions during the combined anterolateral augmentation procedure in ACLR using the MTT.
It has been reported that ACLR using the MTT demonstrates clinical outcomes comparable to those of independent tunnel-drilling techniques, including the transportal and outside-in techniques.3,13,14,31,39 MTT offers surgical convenience and allows preservation of graft isometry while enabling placement of the femoral tunnel close to the anatomic footprint.13,14,25,39 These potential advantages have led to its continued use among many surgeons.34,36 However, research on surgical strategies to minimize tunnel collisions during combined ACLR using the MTT and anterolateral augmentation procedure is lacking, unlike in independent tunnel drilling techniques. Tunnel collisions are commonly observed during combined ACL and anterolateral augmentation procedures.10,11,19,24,29,30,33 Due to the limited bone stock in the distal femur, creating multiple femoral tunnels in proximity may lead to tunnel collision. Such convergence can compromise graft integrity or fixation stability, potentially increasing the risk of reconstruction failure.15,16 Moreover, it has been suggested that densely clustered tunnels may weaken the structural integrity of the femoral condyle, thereby elevating the risk of osteonecrosis or condylar fracture, particularly in multiligament reconstruction4,28 Given the increasing frequency of anterolateral augmentation procedures due to their biomechanical benefits and favorable clinical outcomes,1,6,7,12,23,27,35 an analysis of surgical strategies to minimize tunnel collisions between the ACL and ALL femoral tunnels is necessary in cases of ACLR using the MTT.
This study highlights that the optimal drill orientation for the ALL femoral tunnel varies based on the need for FCD. In cases without FCD requirements for the ALL femoral tunnel, the recommended drill orientation spans from –40° to –20° in the coronal plane, providing a relatively broad acceptable range. On the other hand, when FCD is necessary, the optimal drill orientation is limited, with recommended orientations of 10° coronal and 40° axial. The observed differences are attributed to the need to consider not only the risk of tunnel collision and the cortex violation caused by the ALL femoral tunnel, but also the influence of tunnel trajectory. Previous study on ACLR with the transportal technique has also indicated varying optimal drill orientations depending on the FCD requirement. 19
Interestingly, ACLR using the MTT exhibited a wider range of optimal drill orientations for the ALL femoral tunnel than has generally been reported in the literature,10,11,19,24,29,30,33 with a relatively lower overall collision rate. Although direct comparisons with ACLR performed using the transportal or outside-in techniques were not conducted in the present study, integration of the geometric characteristics observed in our cohort with findings from a previous study 19 suggests that the observed differences may be attributable to the following geometric factors. Firstly, the ACL femoral tunnel formed by MTT was relatively more vertically oriented in the axial and coronal planes, increasing the distance from the drilling start point for the ALL femoral tunnel. The distance between the outlet of the ACL femoral tunnel and the ALL femoral attachment was greater with the MTT than has been reported in a previous study of ACLR performed using the transportal technique, 19 which may reduce the likelihood of tunnel collision by increasing the spatial separation between the tunnels. Secondly, the ACL femoral tunnel inclination in the sagittal plane was relatively low, further reducing the risk of collision with ALL femoral tunnels. These findings align with previous research suggesting the need for adjusting not only the orientation of the ALL femoral tunnel but also that of the ACL femoral tunnel to reduce tunnel collision in combined ACLR and anterolateral augmentation procedures. 19 Ultimately, the ACL femoral tunnel created through MTT exhibits geometric characteristics that potentially make it less prone to collision with the ALL femoral tunnel. By appropriately considering the suggested optimal drill orientations for the ALL femoral tunnel based on the FCD requirement during MTT-based ACLR, satisfactory outcomes can be achieved by reducing tunnel collisions and minimizing damage to surrounding structures.
Although this study is simulation-based, it has value because it proposes the optimal drill orientation for the ALL femoral tunnel in ACLR using the MTT. This parameter has not been previously studied. Furthermore, it has significant clinical utility by providing surgical strategies not only to minimize tunnel collisions but also to reduce the risk of damage to surrounding structures based on the requirement of FCD during surgery. In fact, applying the findings of a previous simulation study aimed at minimizing femoral tunnel collision during combined anatomic ACLR and anterolateral augmentation procedures has resulted in a noticeable reduction in tunnel collision rates in clinical practice.19,20 To further aid surgical planning, the proposed tunnel orientations may be selectively applied based on the intraoperative fixation requirements for the ALL graft. Specifically, when using suture anchors where FCD is not required, a broader coronal angle range (approximately coronal –40° to –20°, relative to the ALL femoral attachment) may be safely employed. In contrast, when suspensory or aperture fixation is planned—where FCD is necessary—a more constrained orientation is essential (approximately coronal 10° and axial 40°, relative to the ALL femoral attachment). Intraoperatively, the recommended tunnel orientations can be achieved by referencing palpable anatomic landmarks, such as the medial and lateral epicondyles, or by using a mobile fluoroscopic C-arm image intensifier or a goniometer. This study could serve as a guideline for reducing complications during simultaneous ACLR using MTT and anterolateral augmentation procedures, which can ultimately contribute to improved clinical outcomes.
Limitations
This study has several limitations. First, the number of patients included in this study is relatively small. The limited sample size may not adequately represent the full spectrum of anatomic variability, potentially affecting tunnel orientation planning. Furthermore, since the post hoc power analysis focused solely on the repeated-measures ANOVA for tunnel collision, the current dataset may not adequately capture anatomic variability across sex, age, or femoral morphotypes. These limitations may reduce the generalizability of the findings and introduce sampling bias, potentially affecting the robustness of the conclusions. Further validation in larger and more diverse cohorts is warranted. Second, since this study is based on 3D simulations using patients’ imaging data, discrepancies may exist between the actual surgical environment and the simulation. Third, the individual surgical techniques of the surgeon may have influenced the surgical outcomes, particularly the characteristics of the ACL femoral tunnel. Fourth, although various anatomic parameters for analysis, including the virtual ALL femoral tunnel, were established based on evidence from previous studies,2,5,7-9,32 they may not fully encompass the anatomic and surgical diversity. Therefore, the clinical application of the findings from this study should be carefully considered, with the aforementioned limitations taken into account.
Conclusion
During the combined surgeries for ACLR using MTT and anterolateral augmentation procedures, the optimal drill orientation of the ALL femoral tunnel was within the range of coronal −40° to −20° for techniques not requiring FCD and axial 40° and coronal 10° for those requiring FCD.
Footnotes
Appendix
Collision rates including 2 mm clearance between the ACL femoral tunnel and the virtual ALL femoral tunnel

| Coronal
a
|
−40° | −30° | −20° | −10° | 0° | 10° | 20° | 30° | 40° | P-value c |
|---|---|---|---|---|---|---|---|---|---|---|
| 0° | 0% | 0% | 63.0% | 85.2% | 100% | 100% | 100% | 100% | 92.6% | <0.001 |
| 10° | 0% | 0% | 14.8% | 55.6% | 85.2% | 96.3% | 100% | 100% | 100% | <0.001 |
| 20° | 0% | 0% | 0% | 18.5% | 55.6% | 81.5% | 85.2% | 96.3% | 96.3% | <0.001 |
| 30° | 0% | 0% | 0% | 3.7% | 25.9% | 51.9% | 74.1% | 81.5% | 85.2% | <0.001 |
| 40° | 0% | 0% | 0% | 3.7% | 7.4% | 22.2% | 44.4% | 51.9% | 70.4% | <0.001 |
| P Value b | - | - | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.002 |
ACL, anterior cruciate ligament; ALL, anterolateral ligament
Relative angle to the neutral axis, determined by a line connecting the femoral attachment of the ALL and the medial epicondyle of the femur.
P-value for comparing different drill angles of the axial plane in the fixed coronal plane.
P-value for comparing different drill angles of the coronal plane in the fixed axial plane.
Final revision submitted December 22, 2025; accepted December 25, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. This study was supported by a faculty research grant from Yonsei University College of Medicine (6-2024-0060).