
Abstract
Background:
Tunnel collision during ligament surgery may impact graft integrity and fixation, potentially influencing surgical outcomes. Identifying the optimal anterolateral ligament (ALL) femoral tunnel orientation is therefore important to improve the overall success of combined anterior cruciate ligament (ACL) reconstruction (ACLR) and ALL reconstruction (ALLR).
Purpose:
To investigate whether the orientation of the ALL femoral tunnel in combined ACLR and ALLR affects the risk of femoral tunnel collision and subsequent clinical outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Medical records of patients who underwent combined ACLR and ALLR from 2018 to 2022 were reviewed, and those with at least 2 years of follow-up were evaluated. Patients were classified based on the orientation of the ALL femoral tunnel as targeted at the time of surgery, with tunnels created at 30° axial and 30° coronal (Group P) or 0° axial and −40° coronal (Group D). Between-group comparisons were conducted for radiological parameters—including the characteristics of the ACL and ALL femoral tunnels, tunnel collision rates, minimal distance between the tunnels (MDBT), and collision volumes—assessed using 3-dimensional knee models from postoperative computed tomography scans. In addition, functional scores, knee laxity, and intraoperative data were analyzed.
Results:
A total of 64 patients were included. Group D exhibited a significantly lower tunnel collision rate compared with group P (68.8% and 6.3% in groups P and D, respectively; P < .001), along with a larger MDBT (–5.5 ± 2.5 mm and 3.7 ± 4 mm in groups P and D, respectively; P < .001) and a smaller collision volume (92.2 ± 89.5 mm3 and 1.2 ± 3.5 mm3, respectively; P < .001). No significant differences were observed between groups in functional scores or knee laxity at the final follow-up. However, the surgical time for cases without combined meniscal procedures was significantly longer in group P (P = .025). Additional comparative analysis newly categorized by tunnel collision also revealed no differences regarding the surgical outcomes; however, surgical time was significantly longer in cases where tunnel collision occurred (P < .001 for both the overall cohort and cases without combined meniscal procedures).
Conclusion:
Distally directed drilling for the ALL femoral tunnel reduced the risk of tunnel collision in combined ACL and ALL procedures without compromising clinical outcomes. Although the tunnel collision itself did not affect surgical outcomes, distal drilling significantly reduced surgical time by minimizing collision risk, thereby optimizing the surgical process.
Keywords
The anterior cruciate ligament (ACL) reconstruction (ACLR) is a well-established surgical procedure known to provide favorable clinical outcomes.21,32 However, residual rotational laxity after ACLR is not uncommon and has been a significant concern among surgeons. 10 Notably, the expanded use of anterolateral augmentation procedures—anterolateral ligament reconstruction (ALLR) or lateral extra-articular tenodesis—has been shown to effectively address residual rotational laxity and contribute to improved clinical outcomes.2,3,7,13,26,27 Among these procedures, ALLR is showing a trend of increasing usage. 30
However, the issue of femoral tunnel collision in combined surgical procedures for the ACL and ALL has been raised.19,23,25,28,29,33 Because both tunnels are formed within the limited space of the lateral condyle of the distal femur, there is a risk of one tunnel interfering with the other during the tunneling process. This femoral tunnel collision, reported to occur in up to 70% of cases according to the literature, can theoretically complicate surgery and pose risks of damage to the graft tendon and fixation device.9,16 Consequently, various studies have explored methods to mitigate this issue, with most proposing anterior and proximal tunnel drilling to reduce tunnel collision.19,23,25,28,33 Nevertheless, actual clinical outcomes of these approaches have not yet been reported. Given that most existing findings are derived from laboratory studies,19,25,28,33 they may not fully reflect actual clinical settings. Moreover, the impact of femoral tunnel collision on clinical outcomes remains unknown. Because even minor misalignments in femoral tunnel placement may negatively impact surgical outcomes, potentially leading to increased rotational laxity or graft failure, femoral tunnel collision may also have a detrimental effect on surgical outcomes. Considering the recent proposal of distally directed tunnel drilling as a new method to reduce tunnel collision,19,29 an assessment of collision risk based on tunnel orientation and its consequent clinical implications is warranted. The analysis of surgical outcomes related to the femoral tunnel orientation for the ALL, based on actual clinical applications rather than laboratory studies, could provide more practical clinical guidance for surgeons.
Therefore, this study aimed to investigate whether the orientation of the ALL femoral tunnel in combined ACLR and ALLR affects the risk of femoral tunnel collision and subsequent clinical outcomes. It was hypothesized that creating the ALL femoral tunnel in a distal orientation would reduce the risk of femoral tunnel collision and lead to more favorable clinical outcomes in patients undergoing combined ACLR and ALLR.
Methods
The present study received approval from the institutional review board of our institution, which waived the requirement for informed consent because of the retrospective design of the study (ID No.: 2024-04-005-001). The electronic medical records of patients who underwent anatomic single-bundle ACLR combined with ALLR by a single senior author (Y.-J.S.) between October 2018 and February 2022 were retrospectively reviewed. The eligibility of patients for inclusion in this study was evaluated. The exclusion criteria were established as follows: (1) age >50 years; (2) follow-up period of <2 years; (3) grade 0 or 1 in preoperative pivot-shift test; (4) multiple ligament reconstruction (eg, combined posterior cruciate ligament and posterolateral corner reconstruction); and (5) revision surgery. Patients with grade 1 pivot shift were excluded to maintain homogeneity within the study group, as combined ACLR and ALLR is typically performed for patients with higher pivot shift grades. Furthermore, patients whose ACL femoral tunnel or ALL femoral tunnel was not located in an anatomic position, as evaluated using a 3-dimensional (3D) computed tomography (CT) model based on reference values from previous studies,5,31 or those lacking follow-up outcome data, were also excluded. Finally, patients eligible for inclusion in this study were classified into 2 groups according to the drilling orientation of the ALL femoral tunnel as targeted at the time of surgery (group P, ALL tunnel created at 30° in the axial plane [anterior] and 30° in the coronal plane [proximal]; group D, ALL tunnel created at 0° in the axial plane and −40° in the coronal plane [distal]) (Figure 1). The angle of the drilling was measured according to an intraoperative sterilized goniometer.

Flowchart of the included patients. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Operative Technique
For ACLR, the outside-in femoral drilling technique was employed. When an ACL remnant was present at the femoral attachment, the posteromedial transseptal approach was used to preserve the remnant while achieving adequate visualization. 15 In cases where the empty wall sign was observed or the remnant tissue was minimal, the femoral attachment was visualized through the anteromedial portal, and the outside-in guide was positioned accordingly. The drilling target was the attachment of the anteromedial bundle within the ACL femoral footprint, which was marked using an arthroscopic radiofrequency ablator. Subsequently, the outside-in ACL femoral guide was inserted through the anterolateral portal, positioning its tip at the previously marked location. The Flipcutter drill (Arthrex) was then passed through the guide sleeve set at a 105° angle to ream to the diameter matching that of the graft. Retrograde reaming was conducted to a depth of approximately 10 mm within the femoral cortex. An autogenous hamstring tendon, folded double or triple, with a diameter of 8 to 10 mm, was used as the ACL graft. 14
For anterolateral augmentation procedures, anatomic ALLR was performed using a peroneus longus allograft with an approximate diameter of 5 mm. A longitudinal incision approximately 3 cm in length was made just above the lateral epicondyle of the femur. The lateral epicondyle was exposed after the incision of the iliotibial band. The starting point for drilling the ALL femoral tunnel was determined to be just posterior and superior to the lateral epicondyle, which was directly identified as a landmark during surgery.5,24 Furthermore, an image intensifier was used for additional verification. The tibial tunnel of the ALL was created 1.5 cm distal to the articular surface, positioned midway between the Gerdy tubercle and the anterior border of the fibula head. 5 The drilling of both the femoral and tibial tunnels reached a depth of approximately 30 mm. The ALL graft was fixed at approximately 30° of knee flexion to prevent excessive graft tension during the knee range of motion, immediately after fixing the ACL graft in full knee extension.5,11,12
Regarding the drill orientation of the ALL femoral tunnel, the senior author initially adopted an anterior and proximal drilling orientation from October 2018 to August 2020 based on findings from a previous study. 25 However, because of the high incidence of femoral tunnel collision observed with the aforementioned drill orientation in our cohorts, the drilling method was modified from August 2020 to adopt a distally oriented approach, based on recent laboratory findings. 19 For anterior and proximal drilling orientations, the aim was 30° in the axial plane and 30° in the coronal plane, followed by fixation using a 6-mm biodegradable interference screw (group P). In the case of distal drilling orientation, the aim was 0° in the axial plane and −40° in the coronal plane, and fixation was achieved using a 4.75-mm knotless SwiveLock suture anchor (Arthrex) without far-cortex drilling (group D) (Figure 2).
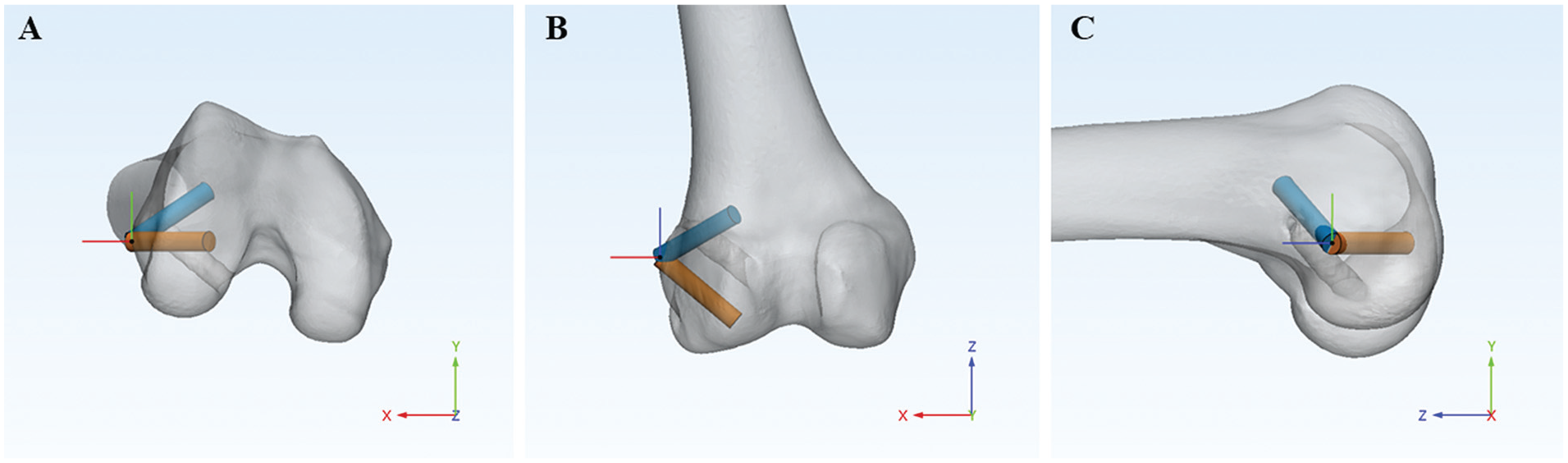
Two different orientations of the ALL femoral tunnels. The blue cylinder represents an ALL femoral tunnel oriented at 30° in the axial plane and 30° in the coronal plane. The orange cylinder represents an ALL femoral tunnel oriented at 0° in the axial plane and −40° in the coronal plane. (A) Axial plane. (B) Coronal plane. (C) Sagittal plane. ALL, anterolateral ligament.
Radiological Measurements Using 3D Knee Models
At our institution, postoperative CT scanning using a high-resolution 16-channel CT scanner (SOMATOM Sensation; SIEMENS) was performed within 1 week after surgery for all patients undergoing ACLR to assess tunnel position, cortical wall blow-out, and graft fixation status. To determine the characteristics of the ACL and ALL femoral tunnels in this study, the Digital Imaging and Communications in Medicine files obtained from the CT scans were imported into medical imaging software (Mimics, Version 17; Materialize), which enabled the segmentation of a 3D volumetric model of the knee. Using reconstructed 3D knee models, the ACL femoral tunnel location (height and depth), ALL tunnel position, diameter of the ACL and ALL tunnels, inclination angle of the ACL and ALL tunnels in the coronal, axial, and sagittal planes, minimal distance between the tunnels (MDBT), and collision volume were measured (Figure 3).

(A) Measurement of the ALL femoral tunnel position relative to the lateral epicondyle in the sagittal plane. (B and C) Measurement of the inclination of the ACL and ALL femoral tunnels in the axial and coronal planes relative to the transepicondylar line. (D) Measurement of the inclination of the ACL and ALL femoral tunnels in the sagittal plane relative to the long axis of the distal femur. (E) Assessment of the MDBT by measuring the distance between the central axes of the ACL and ALL femoral tunnels and then subtracting the radii of the respective cylinders. (F) Semiautomatic calculation of the collision volume by removing the overlapping portion of the ACL and ALL femoral tunnels. ACL, anterior cruciate ligament; ALL, anterolateral ligament; MDBT, minimal distance between the tunnels.
The preparation of the femur model for evaluating ACL femoral tunnel position, represented as height and depth, was conducted in accordance with methods described in previous studies.17,31 A rectangular reference frame, defined by a line passing through the lowest points of the intercondylar notch and the outer margin of the lateral femoral condyle, was utilized to assess the positions of the ACL femoral tunnels. The height of the tunnel was evaluated as the ratio of the distance from the upper part of the reference frame to the tunnel to the vertical length of the reference frame. In contrast, the depth of the tunnel was evaluated as the ratio of the distance from the posterior part of the reference frame to the tunnel to the anterior-posterior length of the reference frame.
Subsequently, a local coordinate system was newly established to evaluate other radiological variables. 19 Initially, the central axis of the cylinder that most accurately conformed to the distal metaphysis of the femur was designated as the long axis of the femur. Then, a line connecting the medial and lateral epicondyles was identified and referred to as the transepicondylar line. The femoral model was then rotated to ensure that the transepicondylar line aligned perfectly with the x-axis. Finally, an additional rotation was performed to confirm the alignment of the long axis of the femur with the z-axis on the y-z plane (sagittal plane). Based on this established local coordinate system, the remaining radiological variables were measured. For the ALL femoral tunnel position, the distance from the lateral epicondyle to the center of the ALL femoral tunnel was calculated relative to the lateral epicondyle in both the superior and posterior directions on the sagittal plane (Figure 3A). The diameters of the ACL and ALL femoral tunnels were analyzed during the reconstruction of their respective cylinders, which were aligned with the existing femoral tunnels in the 3D reconstructed model. The inclination angles of the ACL and ALL femoral tunnels were measured in the axial, coronal, and sagittal planes, respectively (Figure 3, B-D). The axial and coronal inclination angles were determined by measuring the angles between the long axis of each femoral cylinder and the transepicondylar line in the axial and coronal planes, respectively. Similarly, the sagittal inclination angle was calculated by measuring the angle between the long axis of each femoral cylinder and the long axis of the distal femur in the sagittal plane. The MDBT was determined by subtracting the radii of the ACL and ALL cylinders from the minimum distance between their central axes (Figure 3E). A negative MDBT value indicated a tunnel collision. Finally, the collision volume between the tunnels was semiautomatically calculated using imaging software (Figure 3F).
To evaluate the reliability of the radiologic measurements, an experienced orthopaedic surgeon (H.-S.M.), who was blinded to patient information, performed model preparation and measurements twice, with a 4-week interval between each session.
Evaluation of Clinical Outcomes and Intraoperative Data
For the evaluation of clinical outcomes, the International Knee Documentation Committee (IKDC) subjective score was used for subjective assessment. In contrast, the IKDC objective score, the manual pivot-shift grade, and the side-to-side difference (SSD) in anterior tibial translation measured by Telos stress radiograph were used for objective evaluation.8,18 The IKDC objective score classified knee function into 4 grades: (A) normal; (B) nearly normal; (C) abnormal; and (D) severely abnormal. The overall grade reflected the lowest grade received in any assessed category. 4 The manual pivot-shift test results were categorized as follows: 0 indicating absent (normal); 1 indicating glide (nearly normal); 2 indicating jump (abnormal); and 3 indicating transient lock (severely abnormal). Telos stress radiographs of both knees were obtained using a Telos device (Telos) under a load of 150 N. 22 The radiographs were taken with the knee in 30° of flexion, ensuring that both femoral condyles were perfectly superimposed. The SSD value was calculated by comparing the anterior tibial translation of the unaffected knee with that of the affected knee. The analyses were based on medical records documented before surgery and at the final follow-up. Moreover, the types of combined meniscal procedures and the surgical time were evaluated. The surgical time was determined as the time from skin incision to closure, based on records documented immediately after surgery, excluding any overlapping time required for graft preparation.
Statistical Analysis
Statistical analyses were performed using SPSS Statistics for Windows Version 26.0 (IBM). Comparisons of continuous variables between groups were conducted using the Student t test for variables satisfying the normality assumption; otherwise, the Mann-Whitney U test was used. For categorical variables, the Pearson chi-square test or the Fisher exact test was applied. Continuous variables were presented as means and standard deviations, while categorical variables were described as numbers.
A post hoc power analysis was also conducted for the rate of femoral tunnel collision, as the primary endpoint of this study was to analyze femoral tunnel collisions according to the surgical methods. The power analysis was performed using G*POWER software Version 3.1.9.6 (Heinrich Heine Universität, Düsseldorf), based on the number of patients finally included in this study and setting the significance level at 5%. To assess the reliability of radiologic measurements, intraclass correlation coefficients (ICCs) with 95% CIs were calculated. Statistical significance was set at P < .05.
Results
Out of 97 patients, 64 patients were eligible to be included in this study. These patients were classified into 2 groups based on the drilling orientation of the ALL femoral tunnel at the time of surgery (Group P: 32 patients; Group D: 32 patients) (Figure 1). There were no statistical differences between the groups for demographic data (Table 1). Among the patients included in this study, no surgical failures were observed during the follow-up period, 20 nor were there any complications requiring additional intervention, except for 1 patient in Group P who exhibited postoperative knee stiffness.
Comparison of Patient Characteristics and Intraoperative Data a
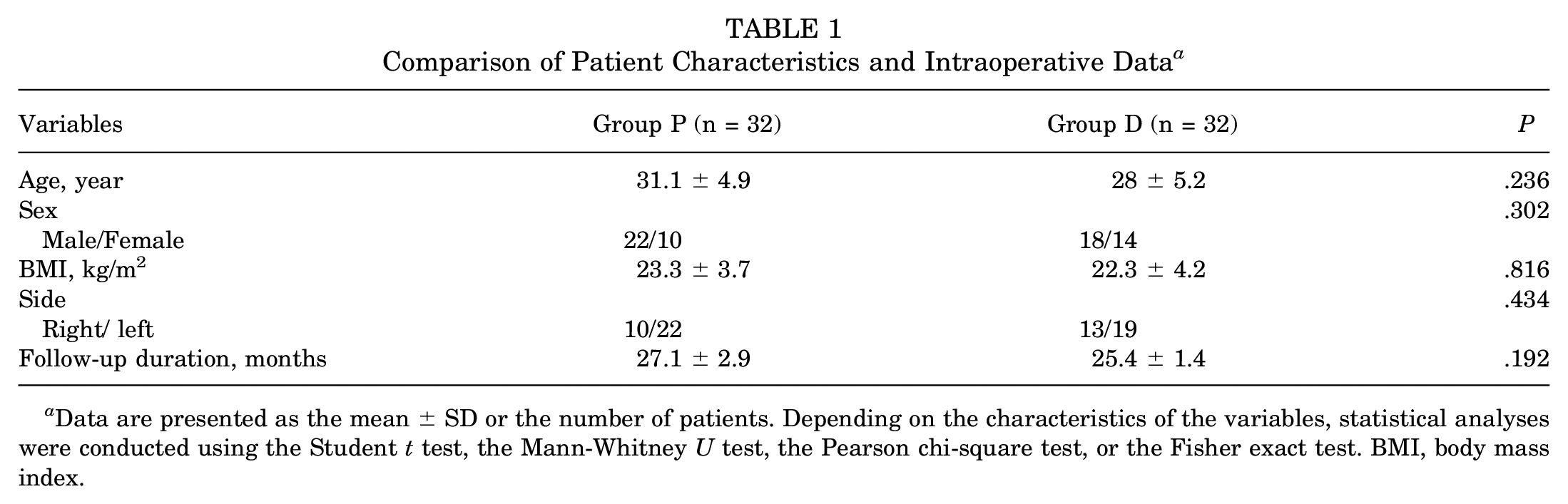
Data are presented as the mean ± SD or the number of patients. Depending on the characteristics of the variables, statistical analyses were conducted using the Student t test, the Mann-Whitney U test, the Pearson chi-square test, or the Fisher exact test. BMI, body mass index.
To analyze the results regarding local geometric data and tunnel collision, radiological parameters were compared between the groups. The location and diameter of the ACL femoral tunnel and the ALL femoral tunnel showed no significant differences between the groups. The inclination angles of the ACL femoral tunnel in all planes did not differ between groups. However, the inclination angles of the ALL femoral tunnel did show differences in all planes, consistent with the classification of groups based on the drilling orientation of the ALL femoral tunnel (P = .02 for the axial plane; P = .006 for the coronal plane; and P < .001 for the sagittal plane) (Table 2). In addition, significant differences were found between the groups regarding femoral tunnel collision data. Group D had a significantly lower tunnel collision rate compared with Group P (68.8% collision rate in Group P and 6.3% in Group D; P < .001). Furthermore, Group D showed a larger MDBT and a smaller collision volume compared with Group P (P < .001 for both MDBT and collision volume between tunnels) (Table 2). The post hoc power for the comparison of the collision rate between tunnels was >99.9%. The 95% CIs of the ICCs for radiological parameters ranged from 0.82 to 0.97, indicating excellent measurement reliability.
Comparison of Radiological Parameters a

Data are presented as the mean ± SD or the number of patients. Depending on the characteristics of the variables, statistical analyses were conducted using the Student t test, the Mann-Whitney U test, the Pearson chi-square test, or the Fisher exact test. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Relative to the lateral epicondyle on the sagittal plane.
A positive value indicates that the drill direction is toward the proximal or anterior part. A negative value indicates that the drill direction is toward the distal or posterior part.
When comparing the functional scores and knee laxity before surgery and at the final follow-up, no statistically significant differences were observed between the groups. However, when comparing intraoperative data, the surgical time for patients without combined meniscal procedures was found to be significantly longer in Group P (P = .025) (Table 3).
Comparison of Clinical Outcomes and Intraoperative Data a

Data are presented as the mean ± SD or the number of patients. Depending on the characteristics of the variables, statistical analyses were conducted using the Student t test, the Mann-Whitney U-test, the Pearson chi-square test, or the Fisher exact test. IKDC, International Knee Documentation Committee; Intraop, intraoperative; Preop, preoperative; SSD, side-to-side difference.
18 patients in group P and 11 patients in group D.
To evaluate the surgical outcomes based on tunnel collision, a new grouping was performed according to the presence of tunnel collision. In the comparative analysis between newly classified groups, no statistical differences were observed in functional scores and knee laxity. However, surgical time was shown to be significantly longer in cases where tunnel collision was observed, regardless of whether combined meniscal procedures were performed (P < .001 both for the overall cohort and cases without combined meniscal procedures) (Table 4).
Comparison Between Groups Newly Classified According to Tunnel Collision a
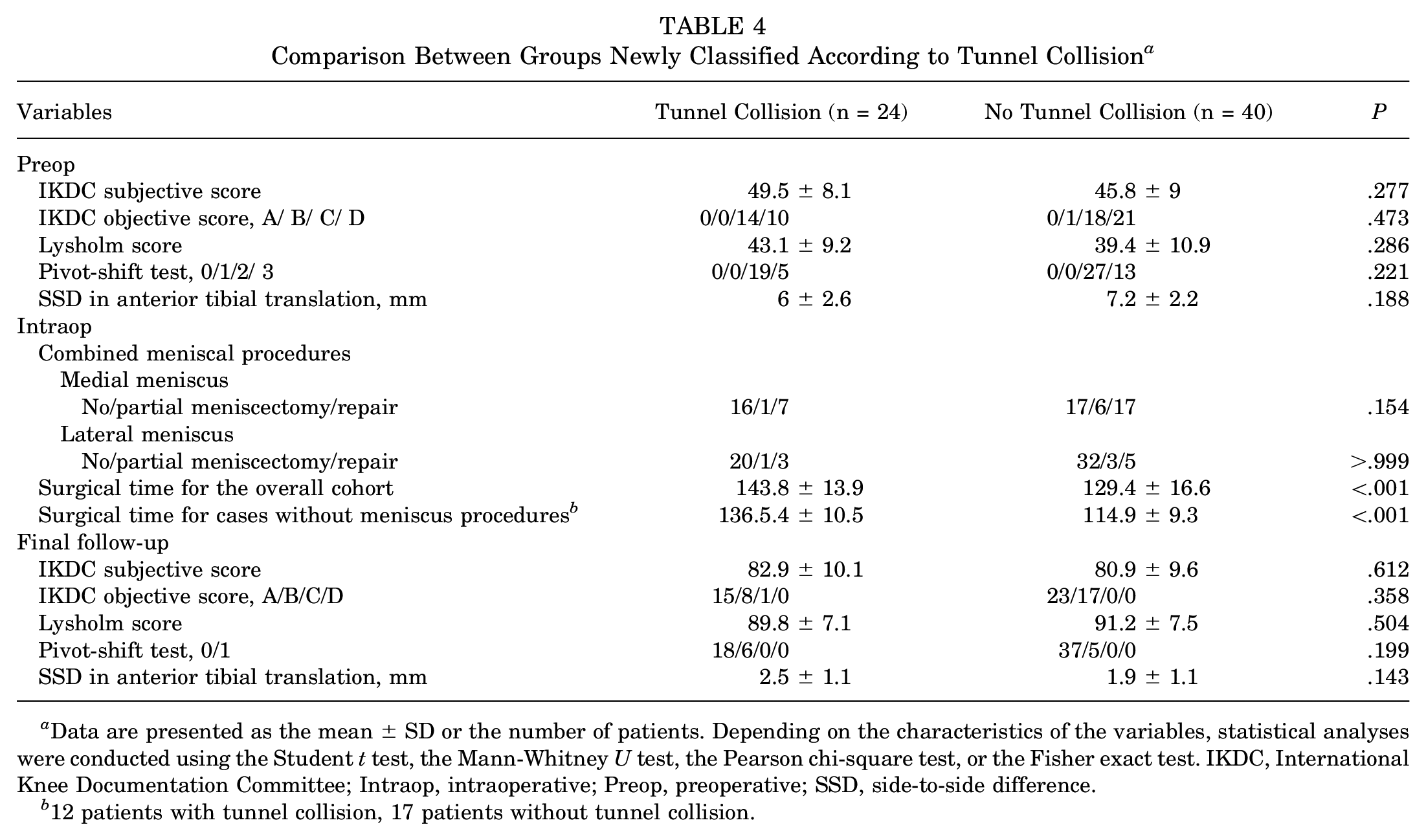
Data are presented as the mean ± SD or the number of patients. Depending on the characteristics of the variables, statistical analyses were conducted using the Student t test, the Mann-Whitney U test, the Pearson chi-square test, or the Fisher exact test. IKDC, International Knee Documentation Committee; Intraop, intraoperative; Preop, preoperative; SSD, side-to-side difference.
12 patients with tunnel collision, 17 patients without tunnel collision.
Discussion
The primary finding of this study is that, in combined surgical procedures for the ACL and ALL, distally directed drilling for the ALL femoral tunnel significantly reduced the incidence of tunnel collision. However, neither the direction of the ALL femoral tunnel nor the resulting occurrence of tunnel collision had a noticeable impact on clinical outcomes. Nevertheless, the surgical time was significantly reduced when the ALL femoral tunnel was directed distally, suggesting that this approach may improve surgical efficiency by minimizing the likelihood of tunnel collision and reducing the risk of potential surgical complications.
In combined surgical procedures for the ACL and ALL, the frequent observation of femoral tunnel collisions has led to numerous studies being conducted to reduce this risk.19,23,25,28,29,33 While previous studies have provided clinically valuable insights, most have relied on cadaveric or simulation research, raising concerns that they may not fully reflect actual surgical conditions.19,25,28,33 Indeed, laboratory settings cannot comprehensively replicate the effects of individual patient anatomy, real-time surgical forces, or the influence of surrounding soft tissues, which makes it challenging to generalize laboratory-based results to the surgical environment. Furthermore, the impact of the orientation of the ALL femoral tunnel and the resulting tunnel collision on clinical outcomes remains unknown. Therefore, in this study, a representative drilling orientation for the ALL femoral tunnel was applied in a clinical setting, and the resulting clinical outcomes were evaluated.
This study demonstrated that, in combined surgical procedures for ACL and ALL, a distal drilling orientation for the ALL femoral tunnel is associated with a reduced incidence of tunnel collision (6.3%) compared with anterior and proximal drilling orientations (68.8%). The incidence of femoral tunnel collision observed with anterior and proximal drilling orientation was substantial, consistent with findings reported in previous studies.19,25 A pronounced difference in tunnel collision rates was observed between the 2 surgical techniques, with consistent findings in the MDBT results. These findings align with those of recent studies. According to Moon et al, 19 who analyzed the optimal drill orientation based on the necessity of far cortex drilling for the fixation of the ALL graft, distal drilling orientation (axial 0° and coronal −40°) showed the lowest tunnel collision rate at 2.6%, aligning closely with the 6.3% collision rate observed in this study. Furthermore, a recent clinical study also reported that distal and anteriorly directed ALL femoral tunnels are associated with relatively fewer collisions. 29 Although the reported collision rates vary slightly across studies despite similar drill orientations, these differences are likely influenced by surgical techniques, anatomic variations, and other factors. It is possible that the reduced tunnel collision rate associated with distal ALL femoral tunnel drilling, compared with anterior and proximal orientations, reflects the orientation of the ACL femoral tunnel. Because of the specifics of ACLR, the ACL tunnel is generally directed anteriorly and proximally, increasing the likelihood of convergence when additional tunnels are created in similar directions. The findings of this study, derived from actual clinical experience, are expected to serve as valuable evidence in determining the optimal drilling orientation among the various methods proposed to date for the ALL femoral tunnel to minimize the risk of tunnel collision in combined ACL and ALL procedures.
In addition to evaluating femoral tunnel collision, this study also analyzed clinical outcomes based on the orientation of the ALL femoral tunnel, revealing no significant differences between groups in both subjective and objective measures. Furthermore, when patients were regrouped according to the presence of tunnel collision, no differences in clinical outcomes were observed, suggesting that femoral tunnel collision may not directly impact surgical results. Theoretically, tunnel collision could potentially damage the graft or fixation device and thereby affect surgical outcomes 16 ; however, the actual clinical findings in this study showed different results. This discrepancy is likely attributable to the following factors. First, in the cohort included in this study, appropriate additional measures were taken if tunnel collision was detected or suspected during surgery. Some degree of observation for tunnel collision is possible intraoperatively using an arthroscope, and suspicion of tunnel collision may also arise if graft passage is hindered. In such cases, the senior author implemented additional measures, such as reducing the diameter of the distal end of the ALL graft or adjusting the fixation device. These modifications, while also potentially contributing to an increase in surgical time, are thought to have minimized potential damage to the graft or fixation devices, thereby reducing any possible impact on clinical outcomes. Second, in instances where tunnel collision occurred but was minimal, grafts might have been led to fit more tightly within the tunnel due to a potential compression effect. Therefore, even if tunnel collision is detected in combined surgical procedures for ACL and ALL, it is considered that surgeons may not need to be overly concerned about clinical outcomes, provided that appropriate measures are taken or no specific issues are encountered during final graft fixation.
Nevertheless, the drill orientation of the ALL femoral tunnel and the resulting tunnel collision were found to potentially influence surgical time. When the ALL femoral tunnel was in an anterior and proximal orientation, especially when a collision occurred, surgical time was significantly prolonged, likely because of additional measures taken to address the collision. While prolonged surgical time may not directly affect surgical outcomes, it could become a potential source of subsequent complications, such as tourniquet pain, deep vein thrombosis, or postoperative infection.1,6 Therefore, even if there is no direct impact on surgical outcomes, directing the ALL femoral tunnel distally during combined surgical procedures for ACL and ALL is recommended to facilitate a more streamlined procedure and minimize potential complications.
Femoral tunnel collision during combined surgical procedures for ACL and ALL remains a challenging issue. Although this study revealed that tunnel collision does not significantly affect surgical outcomes, it can complicate the surgical procedure and still poses a potential source of complications. To minimize these risks, it can be suggested that the drilling orientation for the ALL femoral tunnel be directed in a distal direction. By evaluating the surgical outcomes of representative drill orientations for the ALL femoral tunnel that have been proposed to date in actual clinical settings, this study could offer surgeons practical insights that may enhance procedural outcomes.
Limitations
This study has several limitations. First, as a retrospective study, the possibility of bias in evaluations cannot be excluded. Second, the findings of the present study are based on short-term follow-up results. Notably, although tunnel collision did not appear to affect surgical outcomes, this finding may be limited to short-term results, and its potential influence on graft integration or long-term stability cannot be ruled out. Third, the sample size was relatively small. Although a post hoc power analysis was conducted, it was not performed for all variables. Fourth, as a single senior surgeon performed the surgical treatments, the findings related to the surgical time may not be generalizable to other surgeons.
Conclusion
Distally directed drilling for the ALL femoral tunnel reduced the risk of tunnel collision in combined ACL and ALL procedures without compromising clinical outcomes. Although the tunnel collision itself did not affect surgical outcomes, distal drilling significantly reduced surgical time by minimizing collision risk, thereby optimizing the surgical process.
Footnotes
Final revision submitted March 25, 2024; accepted June 5, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by DongtanSacred Heart Hospital, Hallym University College of Medicine (ID No.: 2024-04-005-001).