
Abstract
Background:
Collision risks between femoral tunnels during combined anterior cruciate ligament (ACL) and anterolateral ligament (ALL) reconstruction have been reported. However, studies on collision risks between tibial tunnels and optimal ALL tibial tunnel orientation are lacking.
Purpose:
To analyze the optimal orientation of the ALL tibial tunnel to minimize collisions with the ACL tibial tunnel while preventing injury to the saphenous nerve in combined reconstruction.
Study Design:
Descriptive laboratory study.
Methods:
Preoperative magnetic resonance imaging (MRI) and postoperative computed tomography (CT) images of patients who underwent primary ACL reconstruction using the anteromedial portal technique were analyzed. Only patients with preoperative MRI scans including thin-cut images (<1 mm) were included for 3-dimensional (3D) reconstruction. Patients who underwent ALL reconstruction or had poorly 3D-reconstructed essential structures were excluded to ensure accurate reproduction of bony attachments and landmarks associated with ALL. Bony structures of the knee joint, including the proximal tibia with the actual ACL tibial tunnel, were reconstructed from the postoperative CT scans. The greater saphenous vein (GSV), which runs together with the saphenous nerve, was reconstructed from the preoperative MRI and subsequently transferred to the CT model, maintaining the appropriate positional relationship. Twelve orientations of the ALL tunnel (at 10° intervals, ranging from 0° to 20° anteriorly and from 0° to 30° distally) were simulated with the final 3D model, starting from the ALL tibial footprint (midpoint between the Gerdy tubercle and the fibular head, 10 mm distal to the joint line), to measure the distances between the ALL tunnel trajectory and other structures (ACL tibial tunnel, GSV) by each orientation.
Results:
A total of 35 out of 304 patients were included in this study. An anteriorly oriented ALL tunnel decreased the minimum distance to the ACL tibial tunnel (MD-ACL) and increased minimum distance to the GSV (MD-GSV) (all P < .001). A distally oriented ALL tunnel increased MD-ACL and decreased MD-GSV (all P < .001). Optimal ALL tunnel orientation was 10° anterior to 30° distal (MD-ACL, 14.6 ± 4.0 mm; MD-GSV, 27.8 ± 12.4 mm) and 20° anterior to 30° distal (MD-ACL, 11.5 ± 3.6 mm; MD-GSV 43.6 ± 12.9 mm), considering both collisions with the ACL tunnel and the potential risk of injury to the saphenous nerve.
Conclusion:
The optimal orientations of the ALL tibial tunnel to avoid collision with the ACL tibial tunnel and prevent saphenous nerve injury are 10° anterior to 30° distal and 20° anterior to 30° distal for far-cortex drilling techniques, starting from the midpoint between the Gerdy tubercle and the fibular head, 10 mm distal to the joint line.
Keywords
As the anterolateral ligament (ALL) has gained renewed attention as a rotational stabilizer secondary to the anterior cruciate ligament (ACL),4,6,23,31 surgeons are increasingly combining anterolateral augmentation procedures with ACL reconstruction, showing promising long-term outcomes, including a significant reduction in ACL rerupture rates and improved survival for meniscal repairs.30,31,33 -35,38,41 Among the procedures,17,25 ALL reconstruction (ALLR) offers the advantage of achieving anatomic reconstruction with minimal injury to the iliotibial band. Although clinical evidence of overconstraint is lacking, 9 it raises less concern for overconstraint compared with lateral extra-articular tenodesis.10,14,40
Various methods are utilized for ALLR, including 1 reported by Sonnery-Cottet et al, 32 which uses the same femoral tunnel for both ACL and ALL. However, methods creating a separate ALL femoral tunnel are also widely employed, offering the advantage of independence from the surgeon’s ACL reconstruction technique. 6 However, there is a possibility of collision with the ACL tunnel when using this method.21,28 Particularly, the method requiring far cortex drilling (subsequently pulling the whipstitched suture or graft to the opposite side and fixing it [interference screw or suspensory fixator] while applying tractional force) is reported to be challenging to avoid collisions even when drilled at an ideal orientation.21,36 To address this problem, Moon et al 21 recommended fixation using a closed socket–type fixator, such as a knotless suture anchor, which does not require far cortex drilling on the femoral side. However, utilizing a closed socket–type fixation method at both ends lacks the ability to control graft tension during ligament reconstruction surgery. A biomechanical study in ALLR has suggested that graft tension can affect the biomechanical properties of the reconstructed ALL graft. 10 Therefore, when fixing the tibial side, rather than fixing both sides with closed socket–type fixators, proper tension control through methods requiring far cortex drilling is considered appropriate. However, forming the ALL tunnel on the tibial side also risks collision with the ACL tibial tunnel and potential saphenous nerve injury, which passes through the posteromedial knee, during the drilling process. Currently, there is no study on the collision risks or optimal ALL tibial tunnel orientation for this technique.
This study aimed to analyze the optimal orientation of the ALL tibial tunnel to minimize collisions with the ACL tibial tunnel while preventing injury to the saphenous nerve. The hypothesis was that a distally, slightly anteriorly oriented ALL tibial tunnel orientation would achieve this purpose.
Methods
Patient Selection
This study included patients who underwent primary ACL reconstruction from March 2015 to September 2023. Among these patients, only those diagnosed with an ACL injury by preoperative magnetic resonance imaging (MRI) performed at our institution (Gangnam Severence Hospital) and who subsequently underwent ACL reconstruction surgery were selected. This selection criterion was based on the availability of homogeneous MRI sequences performed with the same equipment (Philips Achieva 3.0-T MRI ), ensuring consistent image quality. Moreover, the MRI scans included thin cuts of <1 mm for 3-dimensional (3D) reconstruction.
Patients who underwent concomitant ALL reconstruction were excluded to ensure accurate reproduction of bony attachments and landmarks associated with ALL in postoperative computed tomography (CT) scans. Additionally, patients with poorly reconstructed 3D essential structures in this study from preoperative MRI scans were excluded from the study. This study was reviewed and approved by our institutional review board (Gangnam Severance Hospital). Due to the retrospective nature of the study and the minimal risk involved, patient consent was waived.
Surgical Techniques of ACL Tibial Tunnel Placement
All surgical procedures were performed by a single senior surgeon (S.-H.K.) using consistent techniques for ACL reconstruction. For ACL tibial tunnel placement, an ACL tibial guide (ACUFEX Director Drill Guide; Smith & Nephew) set at approximately 55° was inserted through the anteromedial portal, viewing from the high parapatellar anterolateral portal. The tibial tunnel aperture was targeted at the center of the ACL remnant, approximately two-fifths of the distance between medial and lateral tibial spines and about 15 mm anterior to the posterior cruciate ligament. 13 The tibial tunnel drilling started in the anteromedial area of the proximal tibia, just proximal to the pes anserinus and lateral to the anterior margin of the medial collateral ligament. After guide pin insertion, reaming started with a 5–mm diameter reamer and was enlarged to match the ACL graft diameter. The ACL femoral tunnel was created independently using the anteromedial portal technique, as previously described. 22
3D Reconstruction of Preoperative MRI Scans, Postoperative CT Scans, and Final Model
Postoperative CT scans (Sensation 64; Siemens Healthcare) were performed for all patients with their consent. Digital Imaging and Communications in Medicine data from the preoperative MRI scans and the postoperative CT scans were extracted from a picture archiving and communication system (GE Medical Systems Information Technologies) and imported into Mimics software (Version 17; Materialize), a semiautomated tool capable of segmenting the 3D volumetric model. Thin slices (MRI, 0.6-mm thickness; CT, 1-mm thickness) were available for both modalities, ensuring the favorable quality of the 3D-reconstructed model. 20
The bony structures of the knee joint and greater saphenous vein (GSV) were 3D reconstructed from the preoperative MRI. The GSV was well visualized on the MRI at the posteromedial aspect of the knee joint. As the GSV is known to run parallel to the saphenous nerve in the proximal tibial area, 39 it was later used as a reference line to determine the risk of saphenous nerve injury. The knee joint, including the actual ACL tibial tunnel of the patients, was reconstructed from the postoperative CT scans (Figure 1A). The proximal tibia and GSV from the MRI were merged with the CT model using the registration technique of the 3-matic software (Version 13; Materialise), ensuring precise alignment of the tibial bony margins from both imaging modalities (Figure 1B). The final simulation model included the proximal tibial and fibular bone obtained from the CT scans, along with the GSV reconstructed from the MRI, maintaining the appropriate positional relationship with the tibia (Figure 1C).

Reconstruction of the final model for the simulation study. (A, B) Bony structures and the greater saphenous vein were reconstructed from the preoperative magnetic resonance imaging (MRI). The knee joint, including the actual anterior cruciate ligament (ACL) tibial tunnel, was reconstructed from the postoperative computed tomography (CT) scans. To align the MRI and CT models, which have different coordinates, their bony margins were merged based on the tibia. (C) The final model for the simulation.
ALL Tunnel Simulations
A local coordinate setting was established for the simulation using the final 3D knee model. Reference lines were determined to set up the coordinate system (Figure 2). First, the centers of the medial and lateral tibial plateau were determined by fitting circles around the edges of each plateau. 37 The line connecting the centers of the 2 circles was designated as the transtibial axis line (Figure 2A). Second, the anatomic axis of the proximal tibia was established by identifying the central axis of the cylinder that best matched the proximal metaphysis of the tibia (Figure 2B). Third, the final 3D knee model was rotated to align the transtibial axis line with the x-axis and further rotated to align the proximal tibial anatomic axis parallel to the z-axis on the y-z plane (sagittal plane) (Figure 2, A and B).

The local coordinate settings and determination of the anterolateral ligament (ALL) tibial tunnel. (A) The transtibial axis line was determined, with the x-axis aligned accordingly. (B) The z-axis was aligned with the anatomic axis of the proximal tibia on the y-z plane. (C) A point located 10 mm from the bony margin of the lateral tibial plateau, equidistant from Gerdy tubercle and fibular head, was identified as the center of the ALL tibial attachment.
The center point of the ALL tibial attachment was determined based on previous anatomic studies.4,7,31 A line was created to bisect the line connecting the center point of Gerdy tubercle and the center of the fibular head. A point located 10 mm from the bony margin of the lateral tibial plateau along this bisecting line was identified as the center of the ALL tibial attachment (Figure 2C). Subsequently, a neutral ALL tibial tunnel was created with a diameter of 6 mm and a length of 30 mm. A 6-mm diameter was chosen to accommodate the thickest diameter commonly used in actual surgeries.3,6,21 A neutral trajectory line parallel to the x-axis was established, originating from the ALL attachment and extending medially (Figure 3A). Following this trajectory, the neutral ALL tunnel was created with a length of 30 mm (Figure 3A).

Simulation of virtual anterolateral ligament (ALL) tibial tunnels. (A) A neutral ALL tibial tunnel (0° in the axial plane–0° in the coronal plane) was created along the neutral ALL tunnel trajectory, which is parallel to the x-axis starting from the center of the ALL tibial attachment. (B, C) virtual ALL tunnels and tunnel trajectories were created in 12 different orientations.
Using the neutral ALL tunnel and trajectory (0° in the axial plane–0° in the coronal plane) as a reference, virtual ALL tibial tunnels were simulated to change orientations at intervals of 10°. The orientations ranged from 0° to 20° anteriorly in the axial plane and from 0° to 30° distally in the coronal plane. For each case, 12 different orientations of ALL tibial tunnels were simulated (Figure 3B). The consideration of posteriorly directed ALL tunnels was excluded due to the potential risk of violating the posterior cortex of the proximal tibia, which could endanger the posterior neurovascular bundles. Additionally, such an orientation would bring tunnel trajectory closer to the saphenous nerve at the opposite side of the knee (Figure 3C). Similarly, proximally directed ALL tunnels were not considered, as they would be directed toward the joint surface.
Measurements and Evaluation of Parameters
The centers of ACL tibial tunnel orifices at both ends were connected to create the central axis line of the ACL tibial tunnel (Figure 4A). The position of the ACL tibial tunnel orifice was evaluated for depth and width using a previously reported method. 19 The angles formed by the central axis of the ACL tibial tunnel and the z-axis in the coronal and sagittal planes were measured as coronal axis angle and sagittal axis angle of the ACL tibial tunnel, respectively (Supplemental Material, available separately; Figure A1).
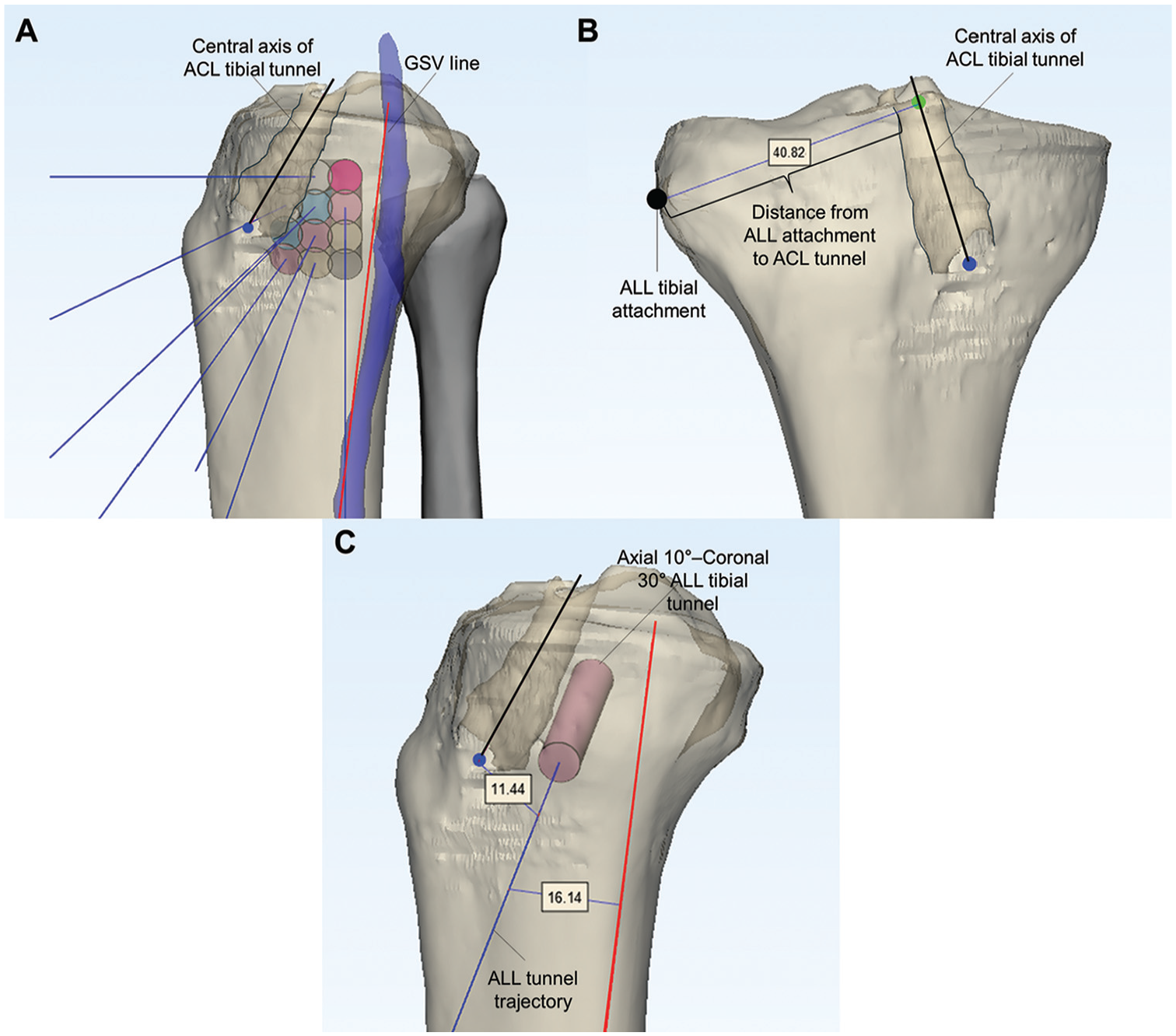
Measurements of the parameters. (A) The central axis of the anterior cruciate ligament (ACL) tibial tunnel and the line representing the greater saphenous vein (GSV) line were used in the measurements. (B) The distance from the anterolateral ligament (ALL) tibial attachment to the ACL tibial tunnel was measured by subtracting the radius of the ACL tunnel from the shortest distance between the center of the ALL tunnel attachment and the central axis of the ACL tunnel. (C) The minimum distance to the ACL tibial tunnel and GSV were measured using the shortest distances from the lines representing each structure.
Subsequently, a line best representing the most anterior margin of the GSV was established as the “GSV line” (Figure 4A). The shortest distance between the center of the ALL tunnel attachment and the central axis of the ACL tunnel was measured, with the radius of the ACL tunnel subtracted from this distance to obtain the distance from the ALL attachment to the ACL tunnel (Figure 4B).
The minimum distance to the ACL tunnel from the ALL tunnel trajectory (MD-ACL) was measured for each situation (Figure 4C). To measure MD-ACL, the radius of the ACL tunnel was subtracted from the shortest distance between the lines representing the central axis of the ACL tunnel and the ALL tunnel trajectory. Collision with the ACL tunnel was considered to be present when the MD-ACL value was negative. The minimum distance to the GSV from the ALL tunnel trajectory (MD-GSV) was measured as the shortest distance between the ALL tunnel trajectory and the GSV line at the medial aspect of the knee (Figure 4C). A distance of <10 mm was considered indicative of a potential risk of injury to the GSV, which was also interpreted in this study as a potential risk of saphenous nerve injury.
Statistical Analysis
Statistical analyses were conducted using SPSS Version 26.0 (IBM), with statistical significance defined as P < .05. Values were presented as mean ± SD unless otherwise specified. Repeated-measures analysis of variance was used to analyze differences in MD-ACL and MD-GSV in each situation. The Cochran Q test was performed to analyze differences in the proportion of collision rate between the ACL tunnel and the ALL tunnel trajectory and the possibility of injury to the GSV in each situation. To assess the test-retest reliability of the simulation process and measurements, a single observer blinded to the patient information and previously measured data (S.-H.J.), reperformed the simulation process and measured the parameters at 4-week intervals. Intraobserver reliability for MD-ACL and MD-GSV, which were the primary outcomes of the simulation, was calculated using intraclass correlation coefficients. Intraclass correlation coefficient values in the measurements through the simulation process were 0.918 to 0.965, showing excellent reliability. 15 A post hoc power for repeated-measures analysis of variance was calculated with G*Power software (Version 3.1.9.2; Heinrich Hein Universitat, Dusseldorf), which showed a statistical power of >99% for the significant results.
Results
A total of 35 patients were included in this study (Figure 5). Demographic characteristics are outlined in Table 1. The mean diameter of the ACL tibial tunnel of the patients was 8.7 ± 0.6 mm (range, 7-10 mm). The mean distance from the ALL tibial attachment to the ACL tibial tunnel was 40.7 ± 3.3 mm (range, 34.5-45.9 mm). Notably, when reaming an ALL tibial tunnel shorter than 34.5 mm, which was the minimum value observed among the included cases, there was no possibility of collision with the ACL tunnel, regardless of the direction in which the ALL tibial tunnel was created.

Patient flow diagram. ACL, anterior cruciate ligament; ALL, anterolateral ligament; MRI, magnetic resonance imaging.
Demographic and ACL Tibial Tunnel Characteristics a

Values are presented as mean ± SD or n. ACL, anterior cruciate ligament.
MD-ACL increased as ALL tunnel orientations became more distally oriented (in the coronal plane) and decreased as they became more anteriorly oriented (in the axial plane) (Table 2). MD-GSV decreased with more distally oriented ALL tunnel orientations and increased with more anteriorly oriented ones (Table 2). The collision rate with the ACL tunnel in each direction showed the same trend as the MD-ACL (Table 3). 0° anterior and between 10° and 30° distal and between 0° and 20° anterior and 30° distal were identified as safe orientations for the ALL tunnel when only considering collisions with the ACL tunnel. However, there was a notable potential risk of injury to the GSV when the ALL tunnel was created directly at 0° relative to the neutral axis in the axial plane. Slightly anteriorly directed ALL tunnels (10° and 20°) posed no possibility of injury to the saphenous nerve, which can be indirectly assessed based on the course of the GSV (Table 3).
Minimum Distance to the ACL Tibial Tunnel From the ALL Tunnel Trajectory (MD-ACL) and Minimum Distance to the Greater Saphenous Vein From the ALL Tunnel Trajectory (MD-GSV) a

Values are presented as mean ± SD. ACL, anterior cruciate ligament; ALL, anterolateral ligament; GSV, greater saphenous vein; MD, minimum distance.
The P values were obtained through repeated-measures analysis of variance test.
Collision Rate With ACL Tunnels and Potential Risk of Injury to Greater Saphenous Vein and Saphenous Nerve a

Values are presented as percentages. Dashes indicate items with no incidence, so statistical analysis was not feasible.
The P values were obtained through Cochrane Q test. ACL, anterior cruciate ligament.
A distance of <10 mm was considered indicative of a potential risk of injury to the greater saphenous vein, which was also interpreted in this study as a potential risk of saphenous injury.
Overall, 10° anterior and 30° distal and 20° anterior and 30° distal were determined to be the optimal orientations for the ALL tibial tunnel, considering both collisions with the ACL tibial tunnel and the potential risk of injury to the saphenous nerve. 10° anterior and 30° distal orientation demonstrated a longer MD-ACL, while 20° anterior and 30° distal demonstrated a longer MD-GSV.
Discussion
The principal findings of this study were as follows: (1) The optimal orientations for the ALL tibial tunnel were 10° anterior and 30° distal and 20° anterior and 30° distal, indicating a slightly anteriorly and distally oriented direction (when ALL tibial tunnels were created using methods that perform far cortex drilling and enable control of the graft tension). (2) Directing the ALL tibial tunnel more distally helps avoid collision with the ACL tibial tunnel, while heading slightly anteriorly helps prevent injury to the saphenous nerve and GSV. (3) As a secondary finding, when the ALL tibial tunnel is created as a closed socket–type limited to the lateral cortex without far cortex drilling, starting midway between the fibular head and Gerdy tubercle, reaming up to about 35 mm can avoid collision with the ACL tibial tunnel regardless of the orientation. For reaming >35 mm, consideration of the orientations is necessary.
To our knowledge, this study is the first to analyze the optimal ALL tibial orientation. There are some studies describing the tibial fixation method of ALLR involving drilling to the far cortex and fixating the graft with an adjustable suspensory fixator or interference screw, similar to the surgical method covered in this study.2,8,11,16 The tibial tunnel orientations of the study were somewhat similar to this study’s result (distally and anteriorly oriented).2,8,16 In a technical note by Boutsiadis et al, 2 the ALL tibial tunnel was drilled in a retrograde fashion, starting from a point anterior to the ACL tunnel orifice on the anteromedial tibial cortex and directed toward the ALL tibial attachment site, with a warning to be careful of collision with the ACL tunnel and excessive thinning of the anterior tibial cortex. However, the appropriate orientation was not specifically described in the previous studies.
This study’s purpose stemmed from 2 necessities. The first is the requirement for the use of a short ALL tunnel during the femoral fixation of ALLR. Several cadaveric or 3D simulation studies have reported a high probability of collision between the ALL and the ACL femoral tunnel when using the methods of femoral fixation that require far cortex drilling.21,28,29,36 While ideal orientations for ALL femoral tunnels were recommended, it has been mentioned that even with the most ideal orientations, the possibility of collisions with the ACL tunnel cannot be completely avoided without adjusting the ACL femoral tunnel as well.1,21,36 Therefore, Moon et al 21 recommended a method of femoral fixation utilizing only short ALL femoral sockets, such as suture anchor fixators, directing the ALL tunnel anteriorly and distally, without invading the femoral notch (Figure 6A). Second is the necessity for graft tension control in ligament reconstruction surgeries. 27 Even if suture anchor fixation is inevitably performed for femoral fixation to avoid collisions, as mentioned above, one end should have a fixation method that allows for proper graft tension control. In knee ligament surgery, undertensioning of the graft can lead to residual laxity and loss of biomechanical effectiveness of the graft, while overtensioning can result in overconstraint. 27 The same principles can likely be applied to ALLR. If undertensioned, the ALL graft may not function properly as a rotational stabilizer, and if overtensioned, concerns regarding overconstraint may arise. Thus, in this study, we investigated the optimal ALL tibial tunnel orientation when utilizing the tibial fixation system that involves the far cortex drilling and enables the control of the graft tension.

Anterolateral ligament (ALL) reconstruction technique illustration on a right knee. A knotless suture anchor is used for femoral fixation of the ALL graft. For tibial fixation, a guide pin is inserted from the ALL attachment to the far cortex. ALL tunnel is then reamed for 30 to 35 mm to accommodate the ALL graft. Subsequently, the whipstitch of the ALL graft is passed to the opposite side under the guidance of the guide pin. Finally, after achieving proper tensioning with the traction of the whipstitch threads (asterisk), ALL graft is fixed with a bioabsorbable screw. (A) Anterolateral oblique view, (B) anteromedial oblique view.
The results of this study indicated that the optimal ALL tibial tunnel direction was 10° anterior and 30° distal and 20° anterior and 30° distal, which was a slightly anteriorly and distally oriented direction. When directed approximately 30° distally, in most of the patients the trajectory of the ALL tunnel surpassed the distal portion of the ACL tibial tunnel entrance at the far cortex, significantly reducing the probability of collision with the ACL tunnel. However, even in the distal 30° direction, too much anteriorly oriented ALL tunnel should be avoided, as it can violate the tibial tubercle or cause excessive thinning of the anterior cortex. 2 In this study, although we aimed to analyze the relationship between ALL trajectory and the saphenous nerve, reconstructing the saphenous nerve using MRI was impossible. Studies on the course of the saphenous nerve indicated that it runs posteriorly with the GSV in the proximal portion of the knee joint and the lower leg.5,26,39 Therefore, we assumed that the reconstructed GSV via MRI reflected the saphenous nerve. If the trajectory of the ALL tunnel passes anterior to the GSV, it can be interpreted that there would be low possibility of injury to the saphenous nerve.
As a clinical application of the study, the authors used a knotless suture anchor for the femoral fixation, which required only short reaming of the closed socket. Drilling for short, closed socket was oriented distally (40° in the coronal plane) as Moon et al 21 recommended. During the tibial fixation, a guide pin was inserted from the ALL attachment to the far cortex, oriented distally and slightly anteriorly. Subsequently, an ALL tunnel of 30 to 35 mm was reamed to accommodate the ALL graft, after which the whipstitch of the ALL graft was passed to the opposite side. Finally, after the proper tensioning with the traction of the whipstitch threads, the ALL graft was fixed with bioabsorbable screws (Figure 6).
Limitations
The present study is not without limitations. First, as a simulation study, the findings may not fully reflect actual surgical conditions. However, simulation studies offer the advantage of reproducing various scenarios with limited data. In this study, we were able to conduct analyses by simulating 12 situations per patient using MRI and CT images. Second is the applicability of this study’s results. Although these techniques are being utilized by the authors, it appears that many orthopaedic surgeons worldwide perform ALLR in various ways. Additionally, the clinical significance of ALL graft tension has not yet been established. Nevertheless, there is currently limited study on the optimal orientation of the ALL tibial tunnel, and presenting these results clearly, rather than relying solely on an individual surgeon’s experience, would contribute significantly to the existing literature. Third, the CT-MRI fusion technique has recently been utilized to map vascular structures accurately onto CT-defined bony anatomy, particularly in complex tumor resection surgeries.12,18,24 However, when applied to joints, accurately reconstructing bony contours on MRI, as is done with CT, can be challenging. Even if visual alignment of the CT-MRI 3D images appears precise, subtle errors can still occur, which needs to be more verified. Last, the need for appropriate ALL graft tension control, which was one of the motivations for conducting this study, has not yet been investigated. While further studies on this aspect are needed, it is established in the principles of ligament reconstruction surgery that fixation should be performed with appropriate graft tension.
Conclusion
The optimal orientations of the ALL tibial tunnel to avoid collision with the ACL tibial tunnel and prevent saphenous nerve injury were 10° anterior and 30° distal and 20° anterior and 30° distal for surgical techniques requiring far-cortex drilling and enabling the appropriate control of the graft tension.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671251327414 – Supplemental material for Optimal Anterolateral Ligament Tibial Tunnel Orientation to Prevent ACL Tunnel Collision and Saphenous Nerve Injury
Supplemental material, sj-pdf-1-ojs-10.1177_23259671251327414 for Optimal Anterolateral Ligament Tibial Tunnel Orientation to Prevent ACL Tunnel Collision and Saphenous Nerve Injury by Se-Han Jung, Min Jung, Kwangho Chung, Hyun-Soo Moon, Sungjun Kim, So-Heun Lee, Chong-Hyuk Choi and Sung-Hwan Kim in The Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors would like to thank MID (Medical Illustration & Design), as a member of the Medical Research Support Services of Yonsei University College of Medicine, for providing excellent support with medical illustration.
Final revision submitted October 23, 2024; accepted November 20, 2024.
The authors declared that there are no conflicts of interesting in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Yonsei University, Gangnam Severance Hospital (No. 3-2024-0039).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.