
Abstract
Background:
In combined anterior cruciate ligament (ACL) and anterolateral ligament (ALL) reconstruction, there is a risk of collision between the femoral tunnels of the ACL and ALL.
Purpose:
To identify (1) the optimal knee flexion angle when creating the femoral tunnel for ACL reconstruction using the transportal technique and (2) the optimal orientation of the ALL femoral tunnel to minimize collisions between the tunnels.
Study Design:
Controlled laboratory study.
Methods:
Computed tomography scans from 10 participants were used to create 3-dimensional (3D) models. A 3D-reconstructed knee model at 90°of flexion was virtually further flexed to 5 different angles (100°-140°; 10° interval). Relationship between the ACL femoral tunnel created at 5 different flexion angles using transportal technique and ALL femoral tunnel created with 25 orientations (5 axial × 5 coronal) were analyzed. The minimal distance between tunnels was measured, and collisions between tunnels were investigated. The characteristics of each tunnel including tunnel length and wall breakage were also assessed.
Results:
An ACL femoral tunnel created at a knee flexion angle of 140° inevitably overlaps with ALL femoral tunnels in all orientations. Considering tunnel length and posterior wall blowout, knee flexion angles from 120° to 130° were considered suitable for ACL femoral tunnel drilling. The optimal ALL drill orientations to minimize collision between the tunnels were identified as axial 20° to coronal 0°, axial 30° to coronal 0°, and axial 30° to coronal 10°, demonstrating no collision between tunnels when the ACL femoral tunnel was created at a knee flexion of 120° to 130°.
Conclusion:
A knee flexion angle within the range of 120° to 130° in ACL femoral tunnel drilling and ALL drill orientations of axial 20° to coronal 0°, axial 30° to coronal 0°, and axial 30° to coronal 10° can be recommended as optimal conditions for creating tunnels while minimizing intertunnel collision in combined ACL and ALL reconstruction.
Clinical relevance:
This study provides practical guidelines for surgeons by identifying a safe range of knee flexion angles for ACL femoral tunnel creation using the transportal technique and optimal ALL femoral tunnel orientations. Applying these results may improve tunnel integrity, and enhance the success of combined ligament reconstructions.
Keywords
Anterior cruciate ligament (ACL) reconstruction has been the primary treatment for ACL injuries with significant instability to restore stability and function, and reduce long-term arthritic changes in the knee joint.34,45 However, residual rotational instability remains in up to 25% of cases after ACL reconstruction.6,29,33,42 To address the issue of residual rotational instability that can persist even after ACL reconstruction, combined lateral extra-articular procedures with ACL reconstruction have shown promise,24,25,32 significantly reducing graft rerupture rates and improving meniscal repair survival.39,40
The 2 most common lateral extra-articular procedures are anterolateral ligament (ALL) reconstruction and lateral extra-articular tenodesis (LET). While each has advantages and disadvantages, there is no biomechanical or clinical superiority of one technique over the other.19,27 ALL reconstruction offers the advantage of achieving anatomic reconstruction while sparing the iliotibial band. Studies have also reported less overconstraint with ALL reconstruction compared with LET procedures.16,44 As a result of these advantages, many surgeons prefer anatomic ALL reconstruction over LET, and a variety of techniques for ALL reconstruction have been described in the literature.5,14,38,41 For femoral tunnel drilling in combined ACL and ALL reconstruction, both single and dual femoral tunnel techniques have been described. In the single femoral tunnel technique, the ACL and ALL grafts are passed together through the same tunnel. 38 In contrast, other studies have utilized a dual femoral tunnel approach, creating separate tunnels for the ACL and ALL.5,41 The use of a separate tunnel offers the advantage of enabling an additional ALL reconstruction at the anatomic native footprints regardless of the ACL femoral tunnel drilling methods and no restriction on graft selection. However, a disadvantage of using separate tunnels is the risk of tunnel convergence, as both the ACL and the ALL tunnels are created in the lateral femoral condyle.18,36,37
Previous cadaveric and simulative studies have suggested an optimal ALL tunnel orientation to minimize collisions between tunnels.18,20,30,36,37,41 A previous study recommended an angle of axial 30° and coronal 30° to minimize collisions between the tunnels, 36 but the authors noted that a high risk of collisions persists even with this angle. Another study recommended an angle of axial 40° and coronal 10° in orientation of ALL femoral tunnel drilling by demonstrating a narrow safe zone. 30 Even so, previous studies are limited because they did not consider the trajectory of the ACL femoral tunnel, which is another variable that influences collision between tunnels in combined ACL and ALL reconstruction.18,20,30,36,37,41 Consequently, to analyze the relationship between ACL and ALL femoral tunnels, not only the orientation of the ALL femoral tunnel but also the trajectory of the ACL tunnel should be considered.1,8 In ACL reconstruction using transportal technique, the trajectory of the ACL femoral tunnel varies depending on the knee flexion angle during tunnel drilling. 8 Depending on the trajectory of the created ACL femoral tunnel, the ALL tunnel can be safe or completely violated. To our knowledge, there has not been a study that analyzed the collision between the ACL and ALL tunnels considering both the trajectory of the ACL femoral tunnel and orientation of ALL femoral tunnel at the same time. To improve rotational stability, combining LET with ACL reconstruction can help prevent tunnel convergence issues that may occur with ALL reconstruction. However, as previously mentioned, ALL reconstruction has certain advantages over LET, and some surgeons prefer it due to its technical feasibility. Accordingly, this study aimed to identify the optimal knee flexion angle when creating the femoral tunnel in ACL reconstruction using the transportal technique and the optimal orientation of femoral tunnel drilling for ALL reconstruction to minimize collision between the tunnels in combined ACL and ALL reconstruction. The hypothesis of this study was that knee hyperflexion during ACL tunnel drilling, combined with a proximally and posteriorly directed ALL femoral tunnel, would increase the likelihood of collisions between the ACL and ALL femoral tunnels.
Methods
This study is a 3-dimensional (3D) simulation study using computed tomography (CT) images collected from the participants between May and September 2023. CT scans were performed on 10 participants with their right knee flexed. The inclusion criteria were (1) age of >19 years and (2) no surgical history in the index knee. Exclusion criteria included (1) definite deformity of the femur and tibia; (2) radiographically osteoarthritic changes with Kellgren-Lawrence grade ≥2; and (3) history of fracture around the knee or ligamentous and meniscal and articular cartilage injuries. The CT scanner Sensation 64 (Siemens Healthcare) was used for all examinations, with tube parameters set at 120 to 140 kVp and 86 to 140 mA. The slice thickness, field of view, and acquisition matrix were 0.6 to 1 mm, 195 to 333 mm, and 512 × 512 pixels, respectively. This study received approval from the institutional review board, which waived the requirement for informed consent, given that this study utilized 3D-reconstructed models from previously collected image data.
3D CT Model Reconstruction and Virtual Further Flexion of 3D Knee Models
Digital Imaging and Communications in Medicine data from the CT scans were extracted from a picture archiving and communication system (GE Medical Systems Information Technologies) and imported into Mimics software (Version 17; Materialise), a semiautomated tool capable of segmenting the 3D volumetric model of the knee. In CT scans of actual participants, the maximal knee flexion angle recorded was 90°. This study utilized CT images obtained at this flexion angle. The reconstructed 90°-flexed 3D knee model for each patient was virtually flexed further to create models at 100°, 110°, 120°, 130°, and 140° (Figure 1). The transepicondylar axis connecting the medial and lateral epicondyles served as the rotation axis for knee flexion. 9 The femur was rotated by 10° from 100° to 140°, considering the possible range of flexion angles during actual ACL reconstruction, particularly when utilizing the anteromedial portal for ACL femoral tunnel drilling. To create the 100°, 110°, and 120° knee flexion models, the femur was translated posteriorly by 1.5 mm for each 10° flexion according to the normal biomechanics reported in the previous study. 26 Within these flexion angles, femoral gliding movement is predominant and rolling is minimal. 21 For 130° and 140° knee flexion models, the femur was additionally translated posteriorly by 4.6 mm for each 10° flexion to incorporate femoral rollback movement during terminal flexion. 21 Axial rotation of femur relative to tibia was not considered because axial rotation of the femur relative to the tibia is rarely observed beyond 90° of flexion according to previous studies.21,26

Creation of 100°-, 110°-, 120°-, 130°-, and 140°-flexed 3-dimensional knee models from 90° knee flexion models.
Simulation of ACL Femoral Tunnel Drilling
According to the method of previous studies,7,43 to determine the center of the ACL femoral footprint, rotation of the 3D-reconstructed femoral model was adjusted to ensure complete overlap of the posterior margins of the medial and lateral condyles, mimicking a true lateral radiograph. The medial femoral condyle was removed from the entire femoral model at the center of the intercondylar notch. A grid parallel to the view was then drawn on the medial wall of the lateral femoral condyle (Figure 2A). 7 A line representing the intercondylar notch roof (Blumensaat line) was determined connecting the most anterior and posterior points of the intercondylar notch roof. The center of the ACL femoral footprint was determined using the quadrant method described in a previous study, 43 where it was located at 28.4% (depth) off the line tangential to the posterior border of the femoral condyle along the line parallel to the intercondylar notch roof line and 35.7% (height) off the intercondylar notch roof line along a line perpendicular to intercondylar notch roof line (Figure 2A).7,43 The height of the accessory anteromedial portal, which is the starting point for ACL femoral tunnel drilling, was determined based on the plane representing the tibial plateau, the height of the medial meniscal, and the femoral tunnel diameter. The previously reported mean heights of the anterior horn and the body of the medial meniscus were 5.32 mm and 5.03 mm, respectively. 11 The femoral tunnel diameter was set at 9 mm, which is generally the largest diameter for a quadruple hamstring graft. 12 Accordingly, the height of the center of the portal was determined to be 10.5 mm (6 mm for meniscus + 4.5 mm for the radius of the tunnel) above the tibial plateau. The tibial plateau plane was created using the best-fit technique, which forms a plane that best represents the marked tibial plateau area. A plane parallel to and 10.5 mm above the tibial plateau plane was then created (Figure 2B). Considering the 9-mm tunnel diameter, the center point of the virtual accessory anteromedial portal that could reach the ACL footprint closest to the medial femoral condyle while leaving a 3.5-mm gap (2.5 mm for mean cartilage thickness 22 + 1 mm for safe margin) was selected on this plane. Simulation of ACL femoral tunnel drilling was performed using a virtual cylinder, connecting the center of the accessory anteromedial portal to the center of the ACL femoral footprint and extending to the far cortex of the lateral femoral condyle (Figure 2B).

Determination of anterior cruciate ligament (ACL) footprint and portal points for ACL tunnel drilling. (A) The ACL femoral footprint was determined using the quadrant method, positioned at 28.4% (depth) from the posterior border of the femoral condyle and 35.7% (height) from the line parallel to the intercondylar notch roof and tangential to the lowest point of the femoral condyle. (B) The portal point was established to be positioned 10.5 mm above the joint line, ensuring that the 9 mm–diameter cylinder, which represents the reamer insertion, maintains a 3.5-mm gap from the femoral condyle to avoid violation.
Simulation of ALL Femoral Tunnel Drilling
A coordinate setting was established to simulate the creation of virtual ALL femoral tunnels. The femoral model was rotated to align the transepicondylar axis parallel to the x-axis and the femoral long axis parallel to the z-axis in the sagittal plane. According to x- and z-axes, the y-axis was also determined. The femoral attachment of ALL was set to the point located 8 mm posterior and 4.3 mm proximal to the lateral epicondyle. 10 In the clinical setting, the drilling of the ALL femoral tunnel typically starts from the femoral attachment of the ALL, with the medial epicondyle commonly used as an anatomic landmark to set the drill orientation. 30 Therefore, a line connecting the medial epicondyle and the femoral attachment of the ALL was defined as the neutral axis of drill orientations (0° in the axial and coronal planes, respectively). 30 The ALL femoral tunnel was represented by a virtual cylinder with a length of 30 mm and a diameter of 6 mm to accommodate the largest tunnel in actual operation used by surgeons.5,13,15,30 Utilizing the neutral axis as a reference, the virtual ALL femoral tunnel was simulated to change orientations at intervals of 10° from 0° to 40° anteriorly in the axial plane and from 0° to 40° proximally in the coronal plane (Figure 3A). Considering that a posteriorly oriented ALL tunnel would violate the posterior femoral cortex and that because a distally oriented ALL orientation would violate the intercondylar notch by the trajectory of the ALL tunnel, ALL tunnel orientation was set to be anterior and proximal. The upper limit of the angulation was set at 40° because drilling the tunnel at an angulation exceeding 40° is known to result in an elliptical tunnel aperture and cortical thinning.28,35

Simulation of virtual anterolateral ligament (ALL) femoral tunnel and measurement of minimal distance between tunnels (MDBT). (A) ALL femoral tunnels were simulated in 25 orientations (5 axial × 5 coronal). (B) Measurement of the MDBT. The minimal distance between the central axes of the anterior cruciate ligament (ACL) and ALL tunnel is measured, with the radii of the ACL and ALL cylinders subtracted to obtain the MDBT. Red lines are central axes of the ACL and axial 40°–coronal 0° ALL tunnel. The MDBT of these tunnels is calculated to be 7.26 mm, derived from subtracting the radii of the 2 tunnels, 4.5 mm and 3 mm, from the total distance of 14.76 mm. (C) Violation of femoral trochlea by the trajectory of axial 40°–coronal 0° ALL tunnel was indicated by the red point.
Evaluation of Relationship Between the Tunnels and Measurement of Parameters of Individual ACL and ALL Tunnels
For each of the 5 ACL femoral tunnel conditions created at 5 different flexion angles, a total of 25 (5 axial × 5 coronal) ALL femoral tunnel conditions were simulated, resulting in a total of 125 conditions for each patient. The minimal distance between the tunnels (MDBT) was measured according to the method previously described. 30 The MDBT was obtained by subtracting the ACL and ALL cylinders’ radial values from the minimal distance between the central axes of each cylinder (Figure 3B). Tunnel collision was determined to have occurred when the MDBT value was negative.
Additionally, various parameters of each tunnel were also assessed. The distance between ALL femoral attachments and the ACL tunnel outlet was measured for each condition. The length of the ACL femoral tunnel was measured for each knee flexion angle during ACL femoral tunnel drilling. The proportion in which tunnels were created shorter than the critical minimal length of 25 mm was investigated. 4 The presence of tunnel wall breakage of each ACL and ALL tunnel, respectively, was evaluated for each condition. The tunnel wall breakage was considered present if the virtual cylinder was exposed outside the femoral cortex in the middle of the tunnel. Additionally, if the cylinder was exposed for >5 mm continuously from the entrance, this was also considered a tunnel wall breakage because such tunnels form broad and elliptical tunnel orifices, making it difficult to ensure rigid and appropriate fixation at the exact desired attachment site. 3 The presence of a violation by the trajectory of the ALL femoral tunnel, which is the direction of the guide pin in the actual operation, into the femoral trochlea or posterior femoral cortex was also assessed for each condition (Figure 3C).
Statistical Analysis
All statistical analyses were performed using SPSS Version 26.0 (IBM), with statistical significance defined as P < .05. Values are presented as mean ± SD unless otherwise indicated. A repeated-measures analysis of variance (ANOVA) was used to analyze differences in MDBT. For post hoc comparisons, P values were adjusted using Bonferroni corrections. Cochran Q test was performed to compare the proportion of tunnel collisions and femoral cortex violation of ALL tunnels in different knee flexion angles and the different drill orientations of ALL tunnels. To assess the test-retest reliability of the 3D simulation and measurements, a single observer (S.-H.J.), blinded to patient information and previously measured data, reconstructed the 3D knee flexion models and performed the measurements at 4-week intervals. Intraobserver reliability was calculated using intraclass correlation coefficients. A post hoc power for repeated-measures ANOVA was calculated with G*Power software (Version 3.1.9.2; Heinrich Hein Universitat).
Results
The age, height, and body mass index of the included patients were 35 ± 2.1 years, 180 ± 6.1 cm, and 23.2 ± 2.1 kg/m2, respectively. In the evaluation of relationship between the tunnels, compared with the ACL femoral tunnel created at a higher flexion angle, the tunnel created at a lower flexion angle tended to be measured to be farther away from the ALL tunnel resulting in high mean MDBTs (Table 1) and low collision rates (Table 2). When the ACL femoral tunnel was created at a knee flexion angle of 140°, most tunnels overlapped with ALL femoral tunnels in all orientations, resulting in negative values of MDBT and high collision rates. The intraclass correlation coefficient for the intraobserver reliability for ACL femoral tunnel length, distance between centers of ACL tunnel outlet and ALL femoral attachment, and MDBT measurement was 0.930 to 0.956. A post hoc power for repeated-measures ANOVA was calculated to be >99.0%. The distance between ALL femoral attachments and the ACL tunnel outlet also tended to become shorter when the femoral tunnel of the ACL was created at a higher flexion angle (Table 3). A 140° flexion angle was not appropriate because of the short distance between the tunnels, leading to an increased risk of tunnel collision. When verifying the suitability of the tunnel considering the parameters of the ACL femoral tunnel itself, the ACL femoral tunnel created at a lower flexion angle tended to have a shorter tunnel length and a higher rate of tunnel wall breakage (Table 3). Most ACL femoral tunnels created at 100° and 110° flexion angles showed a high percentage of tunnel wall breakage. Therefore, knee flexion angles at 120° and 130° could be considered suitable for ACL femoral tunnel drilling in combined ACL and ALL reconstructions.
Minimal Distance Between ACL Tunnel and ALL Tunnel a

Data are presented as mean ± SD. P values were derived from the repeated-measures analysis of variance. Zero or negative values of the minimal distance between tunnels mean the collision between tunnels. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Knee flexion angle when drilling the ACL femoral tunnel.
ALL femoral tunnel orientation.
Collision Between ACL and ALL Tunnels a

Data are presented as percentages. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Knee flexion angle when drilling the ACL femoral tunnel.
Not appropriate: ACL femoral tunnel drilling in this flexion angle results in a high percentage of posterior femoral cortex violation.
ALL femoral tunnel orientation.
Appropriate knee flexion angle during ACL femoral tunnel drilling and ALL femoral tunnel drill orientations.
Not appropriate: ALL femoral tunnel violates the femoral cortex.
Not appropriate: ALL femoral tunnel trajectory violates the femoral trochlea.
Not appropriate: ACL and ALL femoral tunnels collide in all situations with a high percentage.
Evaluation of Parameters of ACL Tunnels a

Data are presented as mean ± SD unless otherwise indicated. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
Knee flexion angle when drilling the ACL femoral tunnel.
Considering the effect of the orientation of ALL femoral tunnels on the distance between tunnels, the distance between the tunnels tended to decrease as the orientation of the ALL tunnel was directed more proximally in the coronal plane for ACL femoral tunnels created at angles of 100° to 130°. In the axial plane, the distance between the tunnels tended to increase as the orientation of the ALL tunnel was directed more anterior (Table 1). Accordingly, less proximally and more anteriorly directed ALL femoral tunnels ensured lower collision rates between the tunnels (Table 2). According to the rate of tunnel wall breakage of the ALL femoral tunnel drilled at different orientations, the ALL tunnels, which were oriented proximally, showed a risk of posterior wall breakage (Table 4). In addition, proximally oriented ALL tunnels resulted in a more elliptical tunnel orifice, which became even more pronounced when oriented further anteriorly. ALL tunnels with excessively elliptical orifices (exposing >5 mm of simulated ALL tunnel cylinder) were considered violations of the femoral cortex (Table 4). Violation rates of the ALL femoral tunnel trajectories, which is the direction of the guide pin in the actual operation, for the femoral trochlea or femoral posterior cortex are also described in Table 4. The trajectory of the ALL femoral tunnel violated the femoral trochlea in a high percentage of 90% when it was created in axial 40° to coronal 0°. The trajectory violated the posterior femoral cortex when it was oriented only proximally, axial 0° to coronal 30° to 40°.
Evaluation of Parameters of ALL Tunnels a
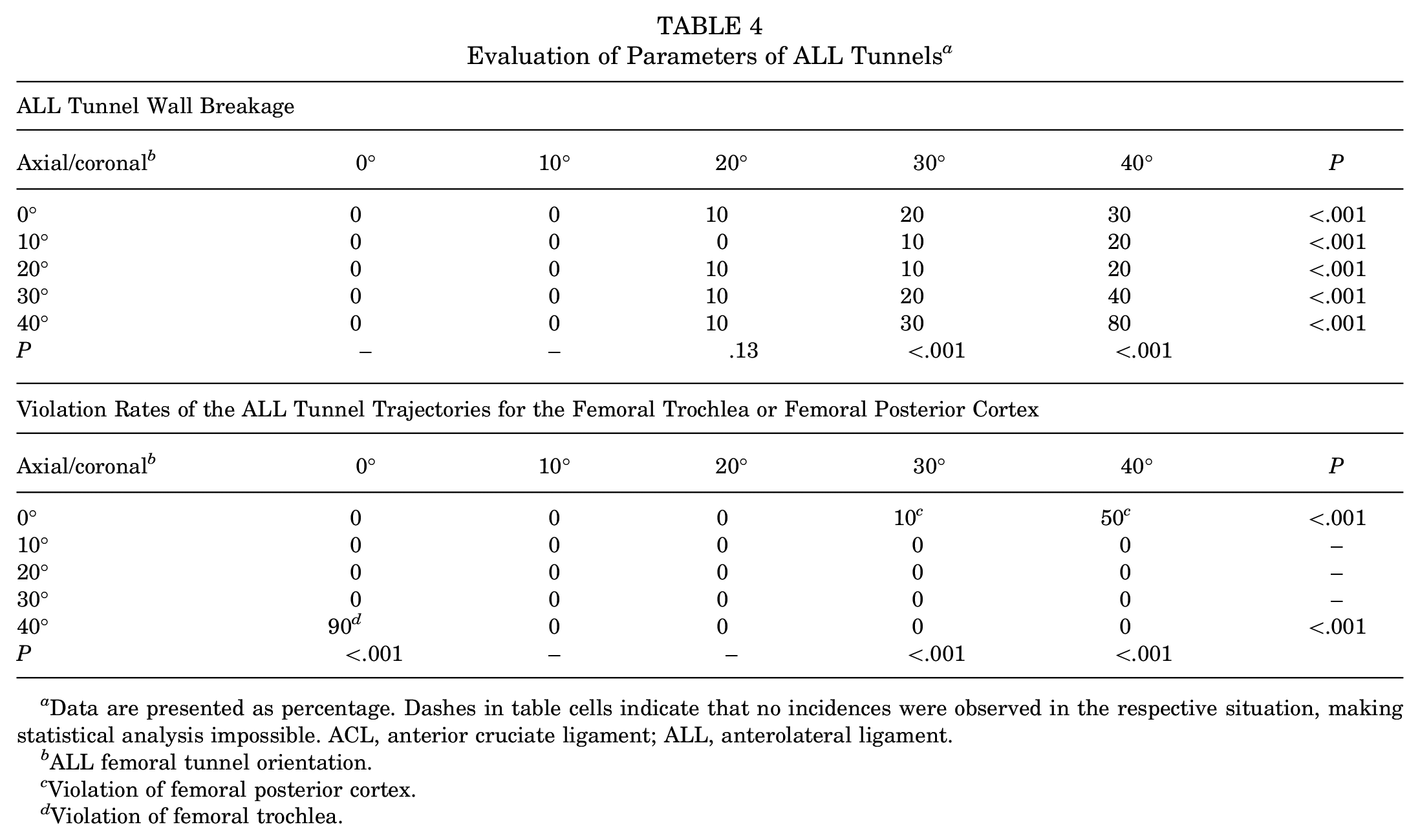
Data are presented as percentage. Dashes in table cells indicate that no incidences were observed in the respective situation, making statistical analysis impossible. ACL, anterior cruciate ligament; ALL, anterolateral ligament.
ALL femoral tunnel orientation.
Violation of femoral posterior cortex.
Violation of femoral trochlea.
When considering the distance between the tunnels and characteristics of created tunnels, the appropriate flexion angle in creating a femoral tunnel for the ACL was 120° and 130°, and optimal ALL drill orientations were identified as axial 20° to coronal 0°, axial 30° to coronal 0°, axial 30° to coronal 10°, and axial 40° to coronal 10° (superscript e in Table 2). Figure 4 depicts a safe zone for ALL drill target points. Within this area, “zone 1 – the triangular zone formed by the trajectory points of axial 20°–coronal 0°, axial 30°–coronal 0°, and axial 30°–coronal 10°” can be considered to be a more appropriate target point, as targeting “zone 2 – the triangular zone formed by the trajectory points of axial 30°–coronal 0°, axial 30°–coronal 10°, and axial 40°–coronal 10°” may potentially encounter the patellar bone in extension or penetrate the quadriceps tendon in knee flexion. 2 Considering this zone, the axial 40° to coronal 10° orientation is excluded, leaving 3 optimal ALL drill orientations: axial 20° to coronal 0°, axial 30° to coronal 0°, and axial 30° to coronal 10°.

Safe zone on the femoral cortex for the target of ALL tunnel orientation was depicted connecting the trajectories of ALL femoral tunnels, which was determined to be appropriate to minimize collision between tunnels (axial 20°–coronal 0°; axial 30°–coronal 0°; axial 30°–coronal 10°; axial 40°–coronal 10°). Within this zone, “zone 1 – the triangular zone formed by the trajectory points of axial 20°–coronal 0°, axial 30°–coronal 0°, and axial 30°–coronal 10°” was considered the optimal target area, as targeting “zone 2 – the triangular zone formed by the trajectory points of axial 30°–coronal 0°, axial 30°–coronal 10°, and axial 40°–coronal 10°” may potentially penetrate the extension mechanism, impeding free knee flexion and extension during procedures.
Discussion
The principal findings of this study were as follows: when the flexion angle increased during the creation of the ACL femoral tunnel, the distance between the ACL and ALL tunnels decreased, increasing the likelihood of collisions. Conversely, a decreased flexion angle shortened the ACL tunnel length and increased the probability of posterior wall breakage. Accordingly, a knee flexion angle of 120° to 130° was suitable for minimizing collisions while ensuring sufficient ACL tunnel length without risking posterior wall breakage. When the ACL femoral tunnel was created at 120° to 130° of flexion, a more anterior and less proximal orientation of the ALL tunnel tended to increase the distance between the ACL and ALL tunnels. The appropriate orientations of the ALL tunnel to minimize collisions with the ACL tunnel were identified as axial 20° to coronal 0°, axial 30° to coronal 0°, axial 30° to coronal 10°, and axial 40° to coronal 10°. However, axial 40° to coronal 10° was excluded to avoid potentially encountering the patellar bone in extension or penetrating the quadriceps tendon in knee flexion. The target region for ALL tunnel orientation was analyzed as a triangular region formed by the 3 trajectories: axial 20° to coronal 0°, axial 30° to coronal 0°, and axial 30° to coronal 10° (zone 1 in Figure 4). When ALL drill orientations targeted this region, ALL tunnels did not collide with the ACL femoral tunnel created at knee flexion angles of 120° and 130° in all participants.
Tunnel collisions during combined reconstruction can occur in up to 70% of cases. 18 Such collisions can cause serious problems, including damage to the graft and fixation devices, compromising secure fixation of the graft. 28 As combined ACL and ALL reconstruction gains clinical evidence and becomes more common,25,32,39 avoiding tunnel collisions is recognized as highly important. When analyzing collisions between ACL and ALL tunnels, factors affecting the creation of each tunnel must be considered. However, most previous studies have overlooked conditions related to ACL tunnel creation. Several factors influence the trajectory of the ACL tunnel, with the flexion angle during tunnel creation being the most important variable.8,23,41 Some authors have suggested a more posteriorly directed ACL tunnel drilling to reduce collision risk, but without providing reproducible guidelines.30,41 Furthermore, no studies have considered the knee flexion angle to date, despite its being the most critical factor influencing ACL trajectory. The present study demonstrated that when the knee was flexed beyond 130° during ACL tunnel creation, the distance between the ACL and ALL tunnels tended to decrease, making tunnel collisions inevitable regardless of the ALL tunnel orientation. Conversely, as knee flexion decreases, the ACL tunnel outlet shifts more proximally and posteriorly, away from the femoral attachment of the ALL. However, at angles <120°, the ACL tunnel length significantly shortens, and there is a high possibility of posterior wall blowout. Therefore, when a surgeon plans to perform additional ALL reconstruction, attention should be paid to maintaining a flexion angle of 120° to 130° during ACL tunnel creation to avoid excessive or insufficient flexion.
Regarding ALL reconstruction, previous studies have proposed appropriate ALL tunnel orientations based on cadaveric or 3D simulation studies.20,30,36,37,41 In the cadaveric studies by Jette et al 20 and Smeets et al, 36 the safest ALL tunnel drill orientation was reported as axial 30° to coronal 30°. However, in these studies, all ACL tunnels were created at a knee flexion of 120° to 125°, and the diameters were smaller than those used in our study. According to our study, the axial 30° to coronal 30° ALL tunnel was not the safest angle. The ALL tunnel created at this angle had a relatively safe relationship with the ACL tunnel made at a lower flexion angle of 120°, but the ALL tunnel created at this angle showed a 100% collision rate with the ACL tunnel created at a higher flexion angle of 130°. These conflicting results may be attributed to smaller tunnel diameter settings and the creation of the ACL tunnel at a low flexion angle in previous studies. Recent 3D-simulation studies, utilizing postoperative CT images of patients who underwent isolated ACL reconstruction, have reported an appropriate ALL tunnel orientation to minimize collisions as being more anterior and less proximal.30,41 Stordeur et al 41 proposed orientations (axial 40° to coronal 10°, axial 35° to coronal 5°, axial 30° to coronal 0°) that closely align with the safe zone suggested by our study. Moon et al 30 suggested an axial 40° to coronal 10° orientation as a safe angle for ALL procedures requiring far cortex drilling, which aligns with our findings. However, in previous studies,30,41 even when the ALL tunnel was created at the recommended orientation, collisions occurred in a considerable proportion of patients (20% 41 and 38.5% 30 ). This inevitably high rate of tunnel collisions may be attributed to uncontrolled knee flexion angles during ACL femoral tunnel drilling. To prevent tunnel collisions in combined ACL and ALL reconstruction, it is essential to consider not only the orientation of the ALL femoral tunnel but also the conditions for ACL tunnel creation. Our study carries significant clinical importance by investigating the ALL femoral tunnel orientation to minimize tunnel collisions while also examining knee flexion angle as a contributing factor in ACL femoral tunnel creation.
Limitations
This study has several limitations. First, it had a relatively small sample size, introducing a possibility of selection bias. However, despite the small sample size, statistically significant results with sufficient power were observed. Second, this study was conducted exclusively on male participants. A small lateral femoral condyle has been identified as a risk factor for tunnel collisions 36 ; when targeting females, the MDBT may be smaller, potentially yielding different outcomes. Third, this study was based on virtual simulations using 3D CT scans. However, 3D CT scans have limitations in capturing soft tissue structures, which hinders the complete reconstruction of an actual knee model. In addition, CT images taken at 90° of knee flexion were used to create 3D knee flexion models at various angles in this study. We aimed to replicate conditions resembling an actual flexed knee model by reflecting subtle movements during knee flexion.21,26 However, femorotibial joint movements are complex and continuously change during flexion, involving axial rotation, flexion-extension, and posterior translation.17,31 These complexities make it difficult to fully replicate normal knee biomechanics in a 3D knee flexion model. Consequently, the virtual 3D knee flexion model used in this study may differ slightly from actual in vivo conditions. Furthermore, simulation experiments—such as the creation of virtual ACL and ALL tunnels—may not fully replicate real surgical procedures. Nonetheless, a key strength of simulation studies lies in the ability to explore a wide range of scenarios that may not be feasible to investigate experimentally due to limitations in data or practicality. In this study, 125 different scenarios were simulated using a single model.
Conclusion
In ACL and ALL combined reconstruction surgery, a comprehensive consideration of both the ALL tunnel orientation and the ACL tunnel trajectory is essential to avoid collisions between the 2 femoral tunnels and ensure stability for each; therefore, a knee flexion angle within the range of 120° to 130° is recommended for femoral tunnel creation, along with ALL drill orientations of axial 20° to coronal 0°, axial 30° to coronal 0°, and axial 30° to coronal 10°.
Footnotes
Final revision submitted March 31, 2025; accepted April 25, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gangnam Severance (No. 3-2023-0467).