
Abstract
Background:
Adolescents experience the highest rates of both ipsilateral and contralateral reinjury following anterior cruciate ligament (ACL) reconstruction (ACLR). Psychological readiness has been shown to be associated with ACL reinjury although the exact relationship is unclear because prior investigations have neither tracked its evolution over time nor stratified results by age and sex.
Purpose:
To perform an age- and sex-specific, longitudinal analysis of the relationship between Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) score and the risk of ipsilateral/contralateral ACL injury in adolescents.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A consecutive cohort of adolescents (<18 years old) who underwent primary ACLR at a single center completed the ACL-RSI preoperatively and at 3, 6, and 9 months. Functional strength and jump metrics were also collected at 9 months. Return to play (RTP) and the incidence of second ACL injury were recorded at 5 years. Differences in ACL-RSI were evaluated and receiver operating characteristic curves were used to quantify the discriminative ability of the ACL-RSI score.
Results:
There were 539 adolescents included. The RTP rate was 89.7% at a mean time of 10.8 ± 3.1 months. The rate of second ACL injury was 22.2% (ipsilateral 9.7%; contralateral 12.5%) at 5 years. Adolescents who sustained a contralateral ACL injury had higher ACL-RSI scores at 9 months for male patients (85.1 ± 14.4 vs 76.7 ± 17.6; P = .004) and at 6 months for female patients (79.9 ± 15.2 vs 67.8 ± 20.2; P = .017) than those who remained uninjured. In contrast, male adolescents who suffered graft rupture recorded lower 9-month ACL-RSI scores than uninjured peers (66.2 ± 18.5 vs 76.7 ± 17.6; P = .003). The ACL-RSI was predictive of ipsilateral reinjury in male adolescents but not in females.
Conclusion:
Serial ACL-RSI scores yield distinct, sex-specific risk profiles in adolescents. Low scores during rehabilitation identify athletes vulnerable to ipsilateral graft failure, whereas rapidly rising, high scores indicate those at risk for contralateral reinjury. This highlights the need to interpret the ACL-RSI score taking age and sex into consideration.
Keywords
Anterior cruciate ligament (ACL) injuries are common in those participating in high-demand sports that involve pivoting and rapid changes in direction.10,17 These injuries result in significant time away from sport and require extensive rehabilitation to restore knee function.4,11 The risk of a second ACL injury, to either the reconstructed knee or the contralateral knee, is one of patients' main concerns when returning to sport.9,19 Therefore, extensive research has focused on identifying factors that predict second ACL injury to guide rehabilitation strategies and develop protocols that support safe return to play (RTP). 11
The rates of second ACL injury are highest in younger athletes.4,25,30 It is estimated that patients aged <20 years old have reinjury rates as high as 25% to 35%, 6 times the risk of older patients.3,30,33 However, the specific factors contributing to the heightened risk in young patients remain unclear. It is likely multifactorial, with age acting as a proxy for other underlying risk factors. 28 For example, younger athletes are more likely to participate in high-risk sports involving jumping, cutting, and pivoting, and they tend to return to these activities sooner after surgery.4,5 This early return can occur before they fully regain strength and functional ability, significantly increasing their reinjury risk. 5 Moreover, adolescence constitutes a pivotal stage of neurocognitive maturation because the prefrontal cortex has not fully developed, meaning younger patients can be more impulsive and less risk-averse than adults. 23
Clinicians increasingly acknowledge the role of psychological factors and their association with return to play and ACL reinjury.2,31 A study by O’Connor et al 18 demonstrated that psychological readiness had little or no relationship with athletes’ strength and power measures. It concluded that psychological and physical recovery after ACL reconstruction (ACLR) are separate elements of recovery that should be addressed individually. Psychological readiness to return to play is often measured using the ACL–Return to Sport after Injury (ACL-RSI) scale, which provides insights into an athlete's confidence, fear of reinjury, and risk appraisal. 29 Recently, McPherson et al 15 demonstrated that patients <20 years old who experienced a second ACL injury (ipsilateral or contralateral) had significantly lower ACL-RSI scores at 12 months postoperatively. In contrast, Ueda et al 27 found that patients with higher ACL-RSI scores at 3 months had an increased rate of second ACL injury. The discordance in these results is likely because these papers did not distinguish between subsequent ipsilateral and contralateral ACL injury. Moreover, because of small cohort sizes, the influence of confounding variables such as age and sex, factors known to affect ACL-RSI scores, was not fully evaluated.24,32 The ACL-RSI score was also measured at different time points in each paper.
Therefore, the aim of our study was to further examine the relationship between ACL-RSI score and the risk of second ACL injury risk in adolescent athletes. Importantly, ipsilateral and contralateral reinjury were evaluated separately. The ACL-RSI scores were also evaluated longitudinally at multiple time points (preoperatively and 3, 6, and 9 months) and stratified by sex to provide a more nuanced view of the recovery of psychological readiness. Our hypothesis was that lower ACL-RSI scores would be associated with an increased risk of ipsilateral and contralateral ACL injury and that specific thresholds could be used to predict those who sustained a second ACL injury.
Methods
This study evaluated a consecutive cohort of 539 adolescent patients (aged <18 years old) who underwent primary ACLR at a single center between January 2014 and December 2018. Participants were selected from the practices of 2 orthopaedic knee surgeons (R.M. and M.J.) and provided informed consent before their inclusion in the research. Patients were excluded if they underwent multiligament knee surgery. Our hospital granted ethical approval for this study. Data for each participant were collected prospectively at the time of surgery, and patients were followed for 5 years postoperatively.
Before surgery, all patients completed a questionnaire capturing demographic details, mechanism, and date of injury. During surgery, all patients received a patellar tendon or hamstring (semitendinosus or gracilis) autograft. Diagnostic arthroscopy was also performed at the time of ACLR, during which the presence of concomitant meniscal and chondral pathology was recorded and treated.
Rehabilitation began immediately postoperatively, with emphasis placed on the early restoration of quadriceps activation. Patients were advised to weightbear as tolerated with crutches for the first 2 weeks. Once discharged, each patient's rehabilitation was supervised by a rehabilitation specialist of his or her choice. All patients were scheduled to meet with the rehabilitation team at our hospital for consultation and assessment at 3, 6, and 9 months. During these assessments, a series of physical performance metrics were collected to guide rehabilitation. We analyzed these data to ensure that significant functional deficits did not explain second ACL injury. Before data collection, all participants completed a standardized warm-up that included a 2-minute jog, 5 bodyweight squats, and 2 submaximal followed by 3 maximal single-leg countermovement jumps (SLCMJs). Testing began with the 2 submaximal and 3 maximal trials of the SLCMJ as well as of the single-leg drop jump (SLDJ). The nonoperated limb was always tested first. For the purpose of this study, we present the data from functional testing at the 9-month assessment, as this is traditionally the time point at which a patient can be considered safe for RTP.
For the SLCMJ, participants stood on 1 leg in the center of a force plate with their hands on their hips. They performed a countermovement by lowering their body before jumping as high as possible. During the SLDJ, participants stood on a 20-cm box with 1 foot and rolled off the edge, landing on the force plate, before immediately jumping as high as possible while minimizing ground contact time. Consistent verbal encouragement and standardized instructions were provided to ensure maximal effort across all jumps.
Following the jump tests, participants underwent isokinetic testing using a Cybex Norm dynamometer (Computer Sports Medicine Inc) to measure the peak torque of the quadriceps and hamstring muscle groups. Torque was recorded in newtons and normalized to body mass (N/kg) for both the operated and the nonoperated limbs. The limb symmetry index (LSI) was also calculated using the formula: LSI = (injured limb value/non-injured limb value) × 100. Testing was conducted in a seated position at an angular velocity of 60 deg/s. Participants completed 3 sets of 5 repetitions, with the first set serving as a warm-up to allow familiarization. A maximal effort was required during the second and third sets. For analysis, the set with the lowest coefficient of variance (threshold <0.1) was selected.
The primary outcome measure for the study was the ACL-RSI scale, which evaluates an athlete's psychological readiness to return to sport following ACL reconstruction. 29 This validated tool assesses 3 key psychological domains: emotional response (including fear of reinjury), confidence in performance, and risk appraisal. The scale consists of 12 items, each scored from 0 to 100, with higher scores indicating greater psychological readiness for RTP. The ACL-RSI has been validated for use in adolescent and pediatric patients. 7 Scores were collected preoperatively and at 3, 6, and 9 months postoperatively.
Patients also recorded if and when they had returned to play. RTP was defined as the unrestricted return to sport, based on the 2016 consensus statement on return to sport. 1 They also reported whether they had sustained a new ACL injury to the ipsilateral or contralateral knee. Patients who experienced a new ACL injury to either knee were also identified during the follow-up period or if they returned to the clinic before the scheduled follow-up time with a confirmed diagnosis of ipsilateral or contralateral ACL injury on magnetic resonance imaging.
Statistical Analysis
For analysis, patients were classified based on whether they had sustained an ipsilateral ACL injury, contralateral ACL injury, or were uninjured. Descriptive statistics were calculated for the demographics of all patients. All variables were assessed for normality of distribution using a Q-Q plot and the Shapiro-Wilk test. Continuous variables such as strength and jump test performance were reported as mean ± SD and compared across the 3 groups using the Student t test. Proportions of categorical variables, such as the rate of RTP and the incidence of second ACL injury, were compared using the chi-square test. The Mann-Whitney U test was used to test differences in the ACL-RSI scores at each time point (preoperative, 3 months, 6 months, 9 months). All ACL-RSI analyses were performed for patients who indicated they had returned to the sport after their ACLR. Subgroup analyses were performed to explore any significant differences between male and female sex for the injured and uninjured groups.
The ability of the ACL-RSI scale to discriminate between those who sustained a second ACL injury (ipsilateral or contralateral) and those who did not was assessed using receiver operating characteristic (ROC) curve analysis. The area under the curve (AUC) served as a summary measure of the ROC curve and reflected the probability that the ACL-RSI would correctly discriminate between those who experienced an ipsilateral or a contralateral ACL injury and those who did not. An AUC of 0.5 indicated no discriminative ability, while values closer to 1 indicated progressively better discrimination. The following interpretation of AUC values was used: ≥0.9 excellent, ≥0.8 to <0.9 very good, ≥0.7 to <0.8 good, ≥0.6 to <0.7 moderate, ≥0.5 to <0.6 poor. 8 Once the ROC curve was generated, diagnostic sensitivity (true positive rate) and specificity (true negative rate) were determined for each potential cutoff value. The Youden index (J = sensitivity + specificity – 1) was employed to identify the optimal cutoff point of the ACL-RSI scale, with values ranging from 0 (useless test) to 1 (perfect test). Higher Youden index values thus indicated a more effective threshold for predicting ACL reinjury from the ACL-RSI score. Statistical significance was set a priori at P < .05. Statistical analyses were performed in STATA Version 18.0.
Results
A total of 539 adolescent patients met the inclusion criteria for this study. The mean age was 15.9 ± 1.1 years. There were 174 patients (32.3%) aged between 13 and 15 years old and 365 patients (67.7%) aged 16 to 17 years old (Table 1); 336 patients (62.3%) were male and 203 patients (37.7%) were female. The main sports played were Gaelic football (46.0%), hurling/camogie (17.4%), soccer (12.4%), and rugby (12.6%). The majority of initial ACL injuries were noncontact injuries (60.9%), with the most common mechanisms of injury being sidestepping (46.6%) and jumping/landing (21.3%). All patients indicated before undergoing surgery that they aimed to return to their sport. Bone–patellar tendon–bone (BPTB) graft was used for 404 patients (75.0%), and hamstring tendon (HT) autograft was used for 135 patients (25.0%). Overall, 23 underwent extra-articular tenodesis (4.3%). The details of concomitant meniscal and chondral injuries are presented in Table 1.
Baseline Patient Demographics for Adolescent Athletes a

Data are presented as n (%) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; BPTB, bone–patellar tendon–bone.
Strength and Jump Test Performance Measures at 9 Months
There were differences in quadriceps strength, jump test performance, and LSI between patients who experienced ipsilateral ACL reinjury and those who did not (Table 2). At 9 months postoperatively, patients with ipsilateral reinjury demonstrated significantly higher quadriceps strength (240.6 ± 39.5 N/kg vs 216.0 ± 51.8 N/kg; P = .003) and quadriceps LSI (93.7% ± 10.6% vs 88.6% ± 14.6%; P = .02) compared with the no reinjury group. Additionally, ipsilateral reinjury patients had better performance in the SLDJ test (12.7 ± 3.6 cm vs 11.3 ± 3.8 cm; P = .02) and marginally improved results in the SLCMJ test (P = .046). Contralateral injury was not significantly associated with quadriceps strength, hamstring strength, or jump test performance (Table 2).
Comparison of Strength and Jump Test Performance Measures at 9 Months Postoperatively for Those Who Experienced Ipsilateral and Contralateral ACL Reinjury and Those Who Did Not a

Data are presented as mean ± SD. Measures were recorded on the side of the initial ACL injury. ACL, anterior cruciate ligament; LSI, limb symmetry index; SLCMJ, single-leg countermovement jump; SLDJ, single-leg drop jump.
Return to Play
Data were available for 97.6% (526/539) patients after exclusion of 13 patients who were lost to follow-up (Figure 1). The overall RTP rate was 89.7% (n = 472/526) and there was no statistically significant difference between males and females (90.6% [299/330] vs 88.3% [173/196]; P = .39). The overall mean time from surgery to RTP was 10.8 ± 3.1 months. There was no difference in the time to return between those who suffered a second ACL reinjury and those who did not (10.6 ± 2.3 months vs 10.8 ± 3.2 months; P = .92).

Flowchart of patient inclusion in the analysis. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; ACLR, anterior cruciate ligament reconstruction; Pre-op, preoperative.
There was no statistically significant difference in the mean preoperative ACL-RSI for those who achieved RTP (47.9 ± 26.1) compared with those who did not RTP (41.7 ± 23.3) (P = .13). However, at 3 months the ACL-RSI score was significantly higher in the group who achieved RTP (59.9 ± 22.3 vs 44.8 ± 23.8; P < .001). At 6 months, the difference was (69.8 ± 19.1 vs 47.3 ± 21.6; P < .001). At 9 months, those who returned to play again had a significantly higher mean ACL-RSI score (77.5 ± 17.7 vs 52.5 ± 23.0; P < .001).
Concerning sex, there was no difference in preoperative ACL-RSI between male adolescents (47.1 ± 26.6) and their female counterparts (47.1 ± 24.5) (P = .10). However, at 9 months, the male ACL-RSI was higher than that of the female score (76.0 ± 19.1 vs 72.5 ± 20.6; P = .001).
Ipsilateral ACL Reinjury and ACL-RSI by Sex
For the ipsilateral reinjury analysis, the 472 patients who returned to play were included (Figure 1). The rate of second ACL injury was 22.2% (n = 105/472) at 5 years follow-up. Ipsilateral reinjury occurred in 9.7% (n = 46/472). Stratified by sex, the incidence was 6.9% (12/173) for females adolescents and 11.4% (34/299) for males (P = .12). The reinjury rate was 4.6% for BPTB grafts and 18.5% for HT grafts. Preoperatively, there were no statistically significant differences in ACL-RSI scores between those who experienced an ipsilateral ACL injury, regardless of whether they were male or female (Table 3). However, by 6 months postoperatively, male patients who had an ipsilateral reinjury demonstrated significantly lower ACL-RSI scores compared with those who did not (64.2 ± 17.0 vs 71.1 ± 18.7; P = .04). This finding in male patients became even more pronounced at 9 months (66.2 ± 18.5 vs 76.7 ± 17.6; P = .003). In contrast, no statistically significant differences in ACL-RSI scores were observed between female adolescents who experienced an ipsilateral injury and those who did not, at any time point (Table 3).
Comparison of ACL-RSI Scores Between Ipsilateral ACL–Reinjured Male and Female Patients a

Data are presented as mean ± SD or (AUC) value (95% CI). ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; AUC, area under the curve; NRI, no reinjury.
The ROC analysis of ipsilateral reinjury and male ACL-RSI score at 9 months produced an AUC of 0.71 (95% CI, 0.65-0.76), indicating that lower ACL-RSI scores were moderately predictive of ipsilateral ACL injury (Figure 2).

ROC curve illustrating the ability of 9-month ACL-RSI scores to predict ipsilateral ACL injury in male adolescents. The AUC of 0.71 (95% CI, 0.65-0.76) indicates a predictive relationship, where lower ACL-RSI scores are associated with a higher risk of ipsilateral injury. The optimal cutoff of 48 points had a Youden index of 0.38 (sensitivity, 54%; specificity, 83%). ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; AUC, area under the curve; ROC, receiver operating characteristic.
Contralateral Injury and ACL-RSI by Sex
Contralateral injury analysis was performed on 472 adolescents who returned to play. The overall rate of contralateral injury was 12.5% (59/472). The rate of contralateral injury was 11.0% (19/173) for female adolescents and 13.4% (40/299) for males (P = .45) at 5-year follow-up. The rate of contralateral injury was 13.0% for BPTB grafts and 13.8% for HT grafts. Preoperatively, there was no difference between the ACL-RSI scores of those who experienced a contralateral injury and those who did not. However, by 6 months postoperatively, male adolescents with contralateral injuries demonstrated significantly higher ACL-RSI scores compared to those without reinjury (75.9 ± 16.7 vs 71.1 ± 18.7; P = .046). This difference became more pronounced at 9 months, with male patients in the contralateral injury group reporting a mean score of 85.1 ± 14.4 compared with 76.7 ± 17.6 in the noninjured group (P = .004). Similarly, among females, those who experienced a subsequent contralateral injury had significantly higher scores at 6 months (79.9 ± 15.2 vs 67.8 ± 20.2; P = .017). However, by 9 months, although the mean ACL-RSI was higher, it was not statistically significant (Table 4).
Comparison of ACL-RSI Scores Between Contralateral ACL–Injured Male and Female Patients a

Data are presented as mean ± SD. The AUC is reported as value (95% CI). ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; AUC, area under the curve; NRI, no reinjury.
The AUC for 9-month ACL-RSI scores in male patients predicting contralateral ACL injury was 0.66 (95% CI, 0.60-0.71) (Figure 3). A Youden index of 0.30 was observed at 77.1 points, corresponding to 82% sensitivity and 49% specificity for contralateral ACL injury. For female patients at 6 months postoperatively, the AUC was 0.70 (95% CI, 0.62-0.77), indicating good predictive ability (Figure 4). A Youden index of 0.46 was observed at 82 points, corresponding to 69% sensitivity and 77% specificity for contralateral ACL injury. These findings suggest that ACL-RSI scores at these key time points have utility in predicting contralateral ACL injury for adolescent patients.
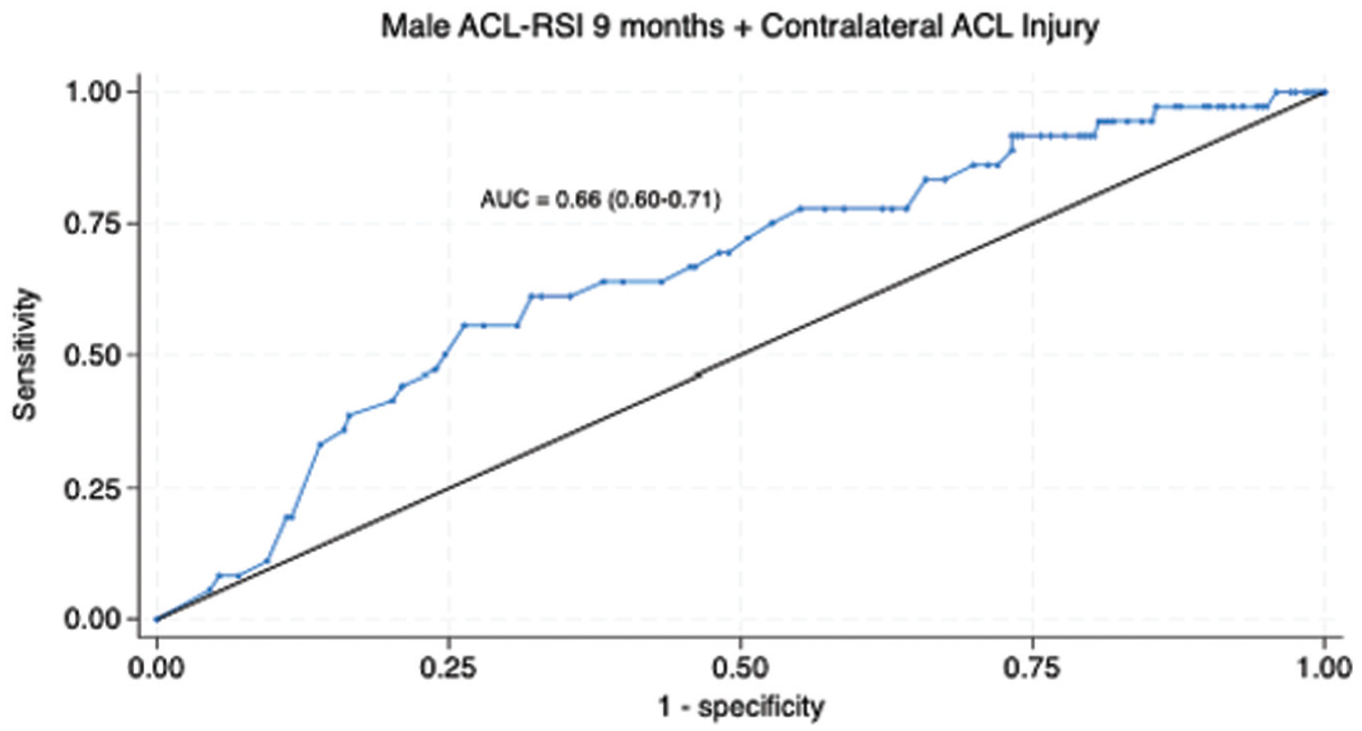
ROC curve illustrating that the ACL-RSI score at 9 months in male adolescents has a good predictive ability for subsequent contralateral ACL injury with an AUC of 0.66 (95% CI, 0.60-0.71). The optimal cutoff score of 77.1 points had a Youden index of 0.30 (sensitivity, 82%; specificity, 49%). ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; AUC, area under the curve; ROC, receiver operating characteristic.

ROC curve illustrating that the ACL-RSI score at 6 months in female adolescents has a good predictive ability for subsequent contralateral ACL injury with an AUC of 0.70 (95% CI, 0.62-0.77). The optimal cutoff of 82 points had a Youden index of 0.46 (sensitivity, 69%; specificity, 77%). ACL, anterior cruciate ligament; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; AUC, area under the curve; ROC, receiver operating characteristic.
Discussion
The most important finding of this study was the association between higher ACL-RSI scores at the end of rehabilitation and an increased risk of contralateral ACL injuries for both male and female adolescent athletes returning to sport. Higher scores in the contralateral injury group were most evident at 9 months for boys (85.1 ± 14.4 vs 76.7 ± 17.6; P = .004) and at 6 months for girls (79.9 ± 15.2 vs 67.8 ± 20.2; P = .017). Another critical finding was the association between lower ACL-RSI scores and ipsilateral ACL injuries, particularly in male athletes at 9 months (66.2 ± 18.5 vs 76.7 ± 17.6; P = .003). These findings underscore the importance of addressing psychological readiness as a distinct component of rehabilitation. Furthermore, they highlight the importance of considering age, sex, and timing when interpreting the ACL-RSI score.
The rate of second ACL injury at 5 years in our cohort was high (22.2%: ipsilateral, 9.7%; contralateral, 12.5%). These findings underscore adolescence as a distinct high-risk period for reinjury that requires dedicated analysis and tailored interventions. Several other studies have identified age as a significant predictor of ACL reinjury.3,4,30 Shelbourne at al 25 and Webster et al 30 demonstrated that patients <20 years of age have up to a 6-fold graft rerupture risk and a 3-fold contralateral injury risk. Data from the Kaiser Permanente ACL registry have indicated that the revision rate can be as high as 32% for patients <21 years of age. 14 Several hypotheses have been proposed to explain this. First, adolescents are thought to return to high-demand, pivoting sports and have an increased likelihood of returning too early, with residual functional deficits. 5 Timing of RTP is a crucial consideration given that returning to sport too early has consistently been linked with reinjury. 4 However, we found no difference in the time to RTP between the group that reinjured their knee and those that did not (10.6 ± 2.3 vs 10.8 ± 3.2 months; P = .92). We also did not find any consistent deficits in strength or jump test performance between the groups who suffered second ACL injury and those who remained uninjured. It is possible that other factors such as tissue laxity, biomechanical alterations, and hormonal fluctuations during adolescence play a significant role in reinjury.12,13 Our findings indicate that psychological factors may play a more influential role in driving ACL reinjury among adolescents compared with other age groups.
The results of our study suggest that adolescents with higher ACL-RSI scores are more likely to RTP. However, those who returned to play with higher ACL-RSI scores at 9 months were also more likely to sustain a contralateral ACL injury. Studies have shown that patients with high confidence have 5 times higher odds of meeting RTP criteria compared with those lacking confidence (odds ratio, 4.59). 21 However, few have thoroughly analyzed the association between ACL-RSI and contralateral ACL injury. Previous studies analyzing the risk of “reinjury” have focused on graft reinjury or have combined the outcome measure into a single variable—second ACL injury—because of smaller sample sizes. 34 Paterno et al 21 found that 31.7% of those in the “confident group,” based on Knee injury and Osteoarthritis Outcome Score (KOOS) Quality of Life (QOL) subscale scores, experienced a second ACL injury compared with 16.2% in the “lacking confidence” group (odds ratio, 2.4). Another study by Paterno et al 20 defined the “high-risk” profile of patients who were at an increased risk of second ACL injury as young girls who exhibited good performance on the single-leg triple hop for distance (>1.3 times bodyweight) with excellent limb symmetry (>98.5%) and high self-reported confidence on the KOOS QOL subscale. In a matched cohort of 43 patients, Ueda et al 27 observed that athletes with ACL-RSI scores >65 points experienced a significantly higher second ACL injury rate than those with scores <65 points (17.6% vs 3.4%; P = .001). Collectively, these findings carry significant clinical implications for how clinicians interpret ACL-RSI scores when making return-to-sport decisions. We suggest that instead of a minimal cutoff for ACL-RSI scores during RTP protocols, it should be interpreted within a "safe zone" that accounts for the athlete's level of physical rehabilitation.
Our results demonstrated that male adolescents with lower ACL-RSI scores at 6 and 9 months demonstrated an elevated risk of ipsilateral reinjury. This aligns with the findings of McPherson et al, 15 who reported that younger patients who experienced a second ACL injury had lower mean ACL-RSI scores at 12 months than those who remained uninjured (60.8 vs 71.5 points). McPherson et al 15 demonstrated that a cutoff score of 76.7 on the 12-month ACL-RSI score had 90% sensitivity and 47% specificity for predicting a second ACL injury in patients aged <20 years (AUC, 0.66). Another study by McPherson et al 16 demonstrated a smaller improvement in ACL-RSI scores throughout rehabilitation among injured patients compared with their uninjured counterparts (9.2 vs 24.9 points; P = .016). Both findings were specific to patients <20 years old, suggesting that younger patients have specific emotional and psychological responses to injury. 2 Using a different psychometric tool, Paterno et al 19 further highlighted that individuals with high kinesiophobia (measured by the Tampa Scale of Kinesiophobia) were 13 times more likely to experience ipsilateral ACL injury. It is possible that low psychological readiness may lead to subtle avoidance behaviors, such as favoring the noninjured leg during landing or cutting, which can alter biomechanics and increase stress on the ACL graft.
We found no difference in ACL-RSI score among female adolescents who sustained an ipsilateral ACL reinjury and those who did not. This finding contrasts with male-dominated studies, where lower ACL-RSI scores were more frequently observed in injured groups, emphasizing the importance of conducting sex-specific analyses. Zarzycki et al 34 analyzed the influence of psychological readiness on second ACL injury risk in female athletes. They identified that females who suffered second ACL injuries had significantly higher ACL-RSI risk appraisal scores than their uninjured peers. Other studies such as Piussi et al 22 applied an ACL-RSI cutoff score of 71 along with other psychometric measures but failed to differentiate between those who sustained second ACL injuries and those who did not. Their study reported an AUC of 0.55, indicating the ACL-RSI was only marginally better than chance in predicting second injuries. However, these studies did not account for age, sex, or second ACL injury type (ipsilateral vs contralateral). In contrast to these studies, we evaluated ACL-RSI scores across multiple time points and stratified scores by sex. There is currently no clear explanation for the sex-specific nature of ACL-RSI scores. It has been proposed that females demonstrate greater risk appraisal, which may also contribute to lower RTP rates. 26 Increased media attention on the high incidence of ACL injuries in females may also heighten fear of reinjury. In addition, rehabilitation priorities, experiences, and perceptions differ between sexes, potentially influencing psychological readiness.6,26 Clinically, this highlights the need to interpret the ACL-RSI score taking age and sex into consideration. Future research should be cautious when interpreting unstratified ACL-RSI data, as this approach may mask important differences between subgroups.
Strengths and Limitations
The strengths of this study lie in its comprehensive assessment of the association between ACL-RSI score and second ACL injury in a large cohort of adolescent athletes. We also had a robust follow-up rate of 97.6%. We also included a high number of second ACL injuries (105 injuries) so could distinguish between ipsilateral and contralateral reinjury risk. This study also explored sex-specific patterns, which are critical for understanding how best to use the ACL-RSI score. Furthermore, the longitudinal design, with ACL-RSI assessments at multiple time points postoperatively (3, 6, and 9 months), provided insights into how psychological readiness evolves over time and at which point it is most valuably assessed.
However, the study has several limitations. First, tools such as ACL-RSI were not specifically designed to assess reinjury risk, and their psychometric properties may not fully capture the multifactorial nature of ACL recovery. Second, while sex differences were examined, key confounders such as graft type, sport type, and competition level, each known to influence reinjury risk, must be considered when interpreting the ACL-RSI and reinjury risk. Third, lateral extra-articular tenodesis, which also affects reinjury risk, has been increasingly used in adolescents since the time of the study. Finally, the study did not control for the variability in rehabilitation protocols or adherence, which could influence both ACL-RSI scores and reinjury rates. Future studies should aim to address these limitations by incorporating more objective measures of rehabilitation adherence and physical readiness.
Conclusion
This study highlights an important relationship between psychological readiness and the risk of ipsilateral and contralateral ACL injury after ACLR in adolescent athletes. We found that patients with higher ACL-RSI scores had an increased likelihood of returning to play, but they also had an increased risk of contralateral ACL injury regardless of sex. In contrast to this, lower ACL-RSI scores in male adolescents were associated with subsequent ipsilateral ACL injuries. These results highlight the importance of both considering psychological readiness during rehabilitation and interpreting the ACL-RSI score differently according to patient age and sex.
Footnotes
Final revision submitted October 3, 2025; accepted November 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.M. receives research funding under the Strategic Academic Recruitment Programme of the Royal College of Surgeons in Ireland. The content of this manuscript is solely the responsibility of the authors and was not influenced by the funding entity. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Sports Surgery Clinic (reference No. 25-AFM-010).