
Abstract
Background:
Psychological readiness encompasses fear of reinjury, confidence in performance, and risk appraisal. It is increasingly recognized as a critical factor influencing return to play (RTP) after anterior cruciate ligament (ACL) reconstruction (ACLR). Elite athletes typically exhibit high self-efficacy and a strong athletic identity while also facing intense external pressure to return. While these dynamics undoubtedly influence their response to injury and psychological recovery after ACLR, the precise differences in psychological readiness between elite and nonelite athletes have not been reported.
Purpose:
To compare psychological readiness between elite and nonelite athletes after primary ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 756 participants were included in this study. There were 252 elite athletes and 504 propensity score–matched, nonelite athletes (1:2 ratio). Elite athletes were those who played professional sport, represented their country at international competitions, or played intercounty-level Gaelic Games. Psychological readiness was compared between groups preoperatively and at 3, 6, and 9 months postoperatively using the ACL Return to Sport after Injury scale (ACL-RSI). Participants were contacted at 1 year and 2 years postoperatively to record if they had returned to play. Multivariable analysis was used to identify factors (eg, age, sex, elite level) associated with ACL-RSI scores at 9 months.
Results:
Preoperative ACL-RSI scores did not differ significantly between elite and nonelite groups (50.6 ± 27.4 vs 48.1 ± 26.6; P = .28). However, elite athletes had higher scores at 3 months (58.6 ± 23.4 vs 53.1 ± 21.9; P < .001), 6 months (67.4 ± 19.9 vs 63.1 ± 19.4; P = .01) and 9 months (72.7 ± 19.9 vs 68.6 ± 19.2; P = .009). Elite athletes had significantly higher RTP rates at 1 year (86% vs 69%; P < .001) and 2 years (94.3% vs 86.7%; P < .002). Multivariate analysis revealed that International Knee Documentation Committee score at 9 months (β = 1.10; 95% CI, 0.95-1.25; P < .001) and male sex (β = 3.7; 95% CI, 0.8-6.6; P < .01) were most associated with increased ACL-RSI scores at 9 months. After adjusting for other factors, elite status was not an independent predictor of psychological readiness.
Conclusion:
Our study demonstrated that preoperative ACL-RSI scores were comparable between elite and nonelite athletes. However, elite athletes had consistently higher ACL-RSI scores during rehabilitation and ultimately greater RTP rates. Knee function and male sex are the strongest predictors of ACL-RSI score. Being an elite athlete is not a primary predictor of psychological readiness, and psychological intervention should be considered in all athletes.
Anterior cruciate ligament (ACL) injuries disrupt athletic participation, often requiring extensive rehabilitation and time away from sport.7,12 Although returning to sport and preinjury performance level remains a top priority for most athletes, many do not achieve this goal despite attaining satisfactory knee function.2,4 A systematic review by Arden et al 3 demonstrated that 65% of athletes returned to their preinjury level of sport and 55% returned to competitive sport after surgery. For elite athletes, the rate of return to play (RTP) is estimated to be between 83% and 95%, although findings on their performance upon returning vary due to the variety of assessment methods used.13,16
Recent research suggests that inability to RTP may stem as much from psychological barriers, such as fear of reinjury and confidence in knee stability, as from physical limitations.2,6,31 The ACL–Return to Sport after Injury (ACL-RSI) scale, which captures fear, confidence, and risk appraisal, has emerged as a key measure of psychological readiness. 33 Lower ACL-RSI scores have been associated not only with a reduced likelihood of returning to play but also an increased risk of reinjury after ACLR. 4,22,26
Despite growing attention to psychological recovery, gaps persist in our understanding of athletes’ responses to ACL injuries, the trajectories of their ACL-RSI scores, and the factors influencing higher or lower psychological readiness. Elite athletes often possess high self-efficacy and a strong athletic identity, but also face intense pressure to return quickly.11,18,23 While these dynamics shape psychological recovery, the precise differences in psychological readiness between elite and nonelite athletes have not been reported. It has been shown that elite athletes have a greater mood disturbance in response to ACL injury due to anxiety and frustration regarding the potential consequences of the injury on their future performance. 24 In contrast, nonelite athletes may benefit from reduced external pressure yet lack access to specialized support systems.
The first aim of this study was to compare the ACL-RSI scores between elite and nonelite athletes preoperatively to assess their psychological response to injury and the prospect of undergoing surgery. Second, we analyzed the ACL-RSI scores of elite and nonelite athletes during the rehabilitation period at 3, 6, and 9 months postoperatively. Third, RTP rates were compared at 1 year and 2 years. Finally, we aimed to identify factors that predict ACL-RSI scores at 9 months postoperatively. Our hypothesis was that elite athletes would demonstrate higher ACL-RSI scores at all time points and that elite level would be predictive of improved psychological readiness.
Methods
Participants
All elite athletes who underwent primary ACLR under the care of 2 orthopaedic surgeons (R.M., M.J.) between January 2014 and December 2018 were identified. Data were collected prospectively and analyzed retrospectively. All participants provided informed consent before their involvement in this research, and our institution granted ethical approval to undertake this study. Elite participants were included if they were aged between 18 and 35 years. We defined “elite” as those competing at the intercounty level in the Gaelic games. For rugby players, we included those who played professionally for an Irish provincial team or in another country. Elite soccer players included those who played professionally or in the League of Ireland Premier Division. Athletes in other sports such as hockey, netball, basketball, and martial arts were considered elite if they represented their country at international competitions. Patients were excluded from this study if they had suffered a multiligament knee injury or had undergone revision ACLR.
Nonelite athletes were individuals engaged in sports at a local club level or recreationally, without meeting the criteria for “elite” outlined above. Propensity score matching (1:2 ratio) was used to create a cohort of nonelite athletes with comparable characteristics to the elite group. Propensity scores were calculated using the following patient variables: age, sex, sport played, graft type, medial meniscal tear treatment, lateral meniscal tear treatment, chondral injury presence. Matching was performed using the nearest neighbor method without replacement, applying a caliper width of 0.05 SD. Covariate balance was assessed using standardized mean differences, with values of <0.1 indicating satisfactory matching. 30
Surgical Technique
ACLR was performed by 2 fellowship-trained sports knee surgeons (R.M., M.J.) using similar arthroscopic techniques for either bone–patellar tendon–bone (BPTB) or Hamstring (HT) autograft reconstruction. BPTB grafts were secured using metal interference screws (Softsilk; Smith & Nephew) on both the femoral and the tibial sides, while HT grafts were fixed using an EndoButton (CL Ultra; Smith & Nephew) for femoral fixation and a nonabsorbable screw (Biosure PK; Smith & Nephew) for tibial fixation. Tunnel positions were placed at the anatomic footprints of the original ACL, and femoral drilling was performed through an anteromedial portal. During the surgical procedure, routine arthroscopy was performed to address any coexisting meniscal and chondral pathology, which was treated accordingly.
Rehabilitation
After surgery, all patients were allowed to weightbear as tolerated immediately without a brace. Crutches were used for approximately the first 2 weeks. Elite athletes undertook rehabilitation supervised by their team, whereas nonelite athletes attended their local rehabilitation specialist. Follow-up assessments were scheduled with the surgeons at 2 weeks, 3 months, 6 months, and 9 months after surgery to monitor their progress. As part of the postoperative assessment, the participants underwent several physical tests at our institution to track their rehabilitation progress (range of motion, strength, biomechanics). The exact testing protocols have been previously described. 14 During these follow-up assessments, the orthopaedic surgeons set minimum criteria for participants to focus on before returning to sport. These included the absence of joint effusion, restoration of quadriceps strength with effective control during single-leg squats, normal patterns in running, and a limb symmetry index of ≥90%. Patients were not required to pass a formal return-to-sport testing protocol. This study defined RTP as the unrestricted resumption of a patient's preinjury sport in line with the definition from the 2016 consensus statement on return to sport. 1
Outcome Measures
All participants completed a preoperative questionnaire at the time of initial consultation, which collected data about their demographics, level of sports participation, and Marx Activity Scale score. 20 The main outcome measure of this study was the ACL-RSI score. 33 The ACL-RSI is a psychometric tool specifically designed to measure an athlete's psychological readiness to return to sport after ACL reconstruction. It assesses 3 primary psychological constructs: emotions (fear of reinjury), confidence in performance, and risk appraisal. The scale consists of 12 items, each rated on a scale from 0 to 100, where 100 indicates the highest level of psychological readiness. The total score is obtained by averaging the responses, providing a quantitative measure of an athlete's readiness to return to sport. 33 The ACL-RSI scale has demonstrated sufficient responsiveness for evaluating the efficacy of psychological interventions at the group level, with a score difference of 1.3 points indicating a genuine clinical change rather than measurement error. 32 The ACL-RSI score was collected preoperatively at the time of initial consultation and again at 3 months, 6 months, and 9 months postoperatively. Additionally, the International Knee Documentation Committee (IKDC) score was also completed at 9 months of follow-up to give an overview of knee symptoms and function. 10 Participants were followed up by email and telephone to record whether they had returned to play at 1 year and 2 years postoperatively.
Statistical Analysis
Patient demographics were reported as descriptive statistics. Continuous variables were displayed as mean ± SD or median (IQR), whereas categorical variables were displayed as numbers and percentages. Patient demographics in the elite and nonelite groups were compared using the χ2 test. Because ACL-RSI scores were not normally distributed, the Mann-Whitney U test was used to compare preoperative and follow-up scores between groups. The association between ACL-RSI scores and RTP was evaluated using logistic regression and reported as odds ratios (ORs).
To examine associations between patient characteristics (eg, sex, age, elite level) and ACL-RSI scores at 9 months, linear regression was used. Candidate variables were first identified via univariate regression, using a threshold of P < .10 for inclusion in the multivariable model. Multicollinearity was evaluated using variance inflation factors, with a cutoff of 5 indicating potential collinearity issues. A forward stepwise selection method was then applied to construct the final multivariate regression model. 9 Following this, additional post hoc univariable analyses were conducted on factors significantly associated with ACL-RSI to assess the magnitude of their association. For example, the effect of sex was illustrated graphically and Spearman rank correlation coefficient was calculated to evaluate the relationship between the ACL-RSI score and IKDC score at 9 months. The threshold for statistical significance was set at a P value <.05. Data analysis and graphical presentation were performed using STATA Version 18.0 (StataCorp LLC).
Results
A total of 756 participants were included in this study. There were 252 elite athletes and 504 matched, nonelite athletes. The baseline demographics (age, sex, body mass index, sport played) for both cohorts were comparable (Table 1). A similar proportion of patients underwent BPTB graft reconstruction in both cohorts (94% vs 92%; P = .49). The presence of meniscal and chondral injuries was also similar. The elite group had a higher preoperative activity level (Marx, 13.6 ± 4.0 vs 11.2 ± 5.0; P < .001) and a slightly shorter time from injury to surgery (2.1 ± 1.8 vs 2.9 ± 2.2 months; P < .001) (Table 1). The overall rate of follow-up at 2 years was 92.7% (n = 701/756).
Baseline Patient Demographics for Elite Athletes and Nonelite Athletes a

Data are presented as n (%) or mean ± SD unless otherwise indicated. P-values reaching statistical significance are highlighted in bold. BMI, body mass index; BPTB, bone–patellar tendon-bone; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; PFJ, patellofemoral joint. ACL-RSI Scores (Elite vs Nonelite).
There was a wide distribution of preoperative ACL-RSI scores for both elite and nonelite athletes across all sports (Figure 1, A and B). Preoperatively, there was no statistically significant difference in mean ACL-RSI scores between the elite and nonelite groups (50.6 ± 27.4 vs 48.1 ± 26.6; P = .28) (Table 2). However, elite athletes demonstrated an 8-point improvement (15.8% increase) compared with a 5-point improvement (10.4% increase) among nonelite athletes during the first 3 months of the rehabilitation period (Table 2). Consequently, at 3 months, the elite cohort had significantly higher mean ACL-RSI scores (58.6 ± 23.4) compared with the nonelite cohort (53.1 ± 21.9) (P < .001). Similarly, mean ACL-RSI scores for the elite cohort were higher at 6 months (67.4 ± 19.9 vs 63.1 ± 19.4; P < .01) and 9 months (72.7 ± 19.9 vs 68.6 ± 19.2; P < .009) (Table 2). At 1-year follow-up, the RTP rate was 86% for elite athletes versus 69% for nonelite athletes; P < .001. By 2-year follow-up, the RTP rate for elite athletes was 94.3% compared with 86.7% for nonelite athletes (P < .002). For elite athletes, each additional point on the ACL-RSI corresponded to a 6.1% higher odds of return (OR, 1.061; 95% CI, 1.02-1.10; P < .002). Among nonelite athletes, each 1-point increase in the ACL-RSI score was associated with a 6.3% higher odds of returning to sports at 2 years (OR, 1.063; 95% CI, 1.04-1.08; P < .001). The mean IKDC scores were 83.8 ± 9.5 for elite athletes and 83.6 ± 9.5 for nonelite athletes at 9 months (P = .42).
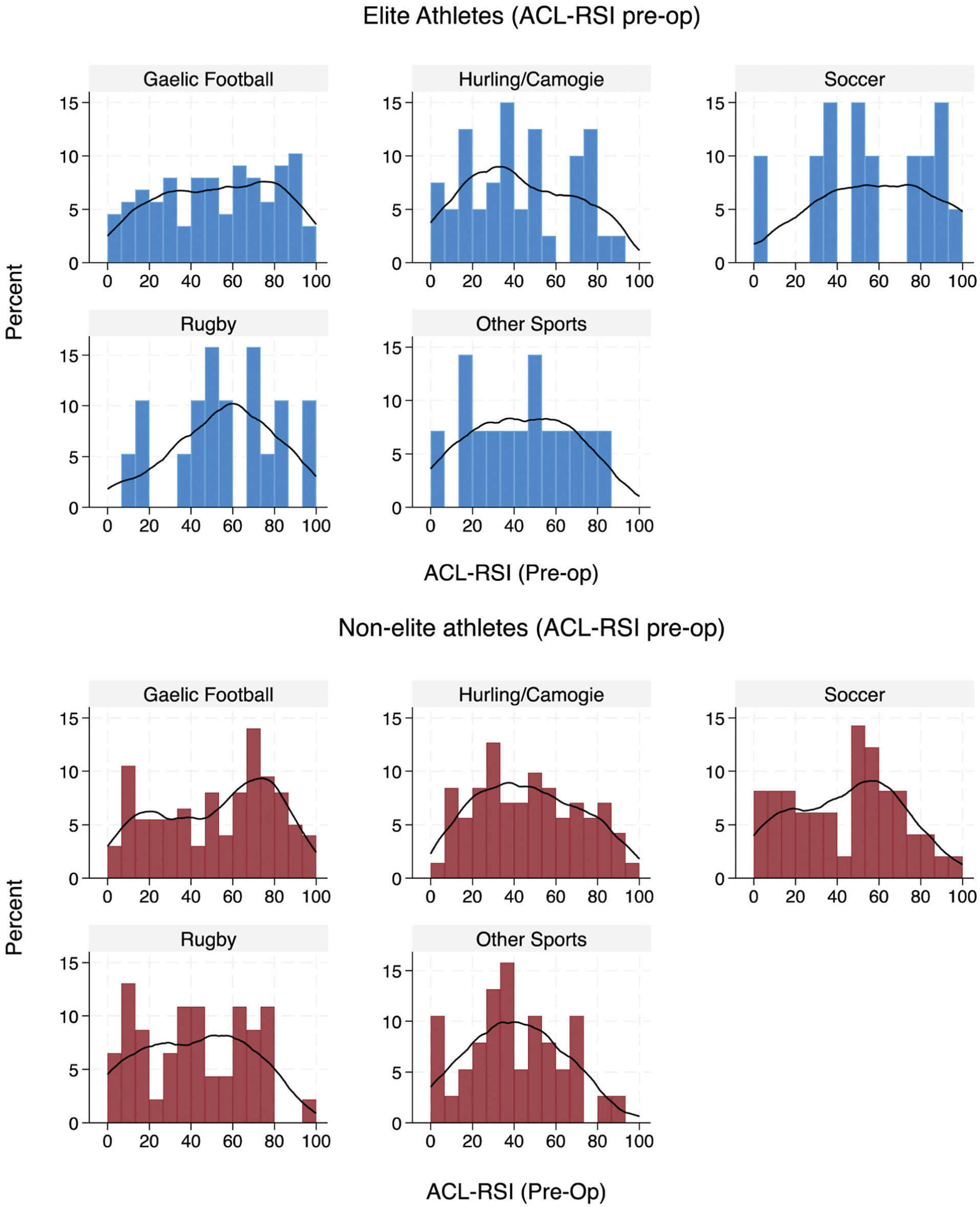
Histograms and kernel density plots showing the distribution of preoperative (Preop) Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scores for elite (blue) and nonelite (red) athletes divided into different sports.
Comparison of Mean ACL-RSI Scores Between Elite and Nonelite Athletes a

Data are presented as mean ± SD or n (%). P-values reaching statistical significance are highlighted in bold. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury scale.
Multivariable Analysis of Factors Associated With ACL-RSI Score at 9 Months
Univariate analysis identified the following variables as significantly associated with increased ACL-RSI scores at 9 months postoperatively: male sex (β = 7.4; 95% CI, 4.3 to 10.5), elite level (β = 4.0; 95% CI, 0.7 to 7.3), having a higher preoperative Marx score (β = 0.6; 95% CI, 0.2 to 0.9), a shorter time from injury to surgery (β = −1.4; 95% CI, –2.1 to −0.6), playing Gaelic football (β = 6.5; 95% CI, 0.3 to 12.7), BPTB graft use (β = 6.6; 95% CI, 1.0 to 12.1) and an increased IKDC score at 9 months (β = 1.10; 95% CI, 0.96 to 1.23) (Table 3).
Univariate Analysis of Factors Associated With ACL-RSI Score at 9 Months a

ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; BMI, body mass index; BPTB, bone–patellar tendon–bone; IKDC, International Knee Documentation Committee; LFC, lateral femoral condyle; LTP, lateral tibial plateau; MFC, medial femoral condyle; MTP, medial tibial plateau; PFJ, patellofemoral joint.
In the multivariate model, male sex (β = 3.7; 95% CI, 0.8-6.6; P < .013) and higher IKDC scores at 9 months (β = 1.10; 95% CI, 0.95-1.25; P < .001) remained significant. Overall, the multivariable model was statistically significant (R2 = 0.33; F(10, 515) = 25.63; P < .001) (Table 4). Post hoc comparison of elite and nonelite athletes stratified by sex is demonstrated in Figure 2, A and B. This demonstrated that at 9 months, ACL-RSI scores were highest in elite, male athletes.
Multivariate Linear Regression Analysis of Factors Associated With ACL-RSI Score at 9 Months a
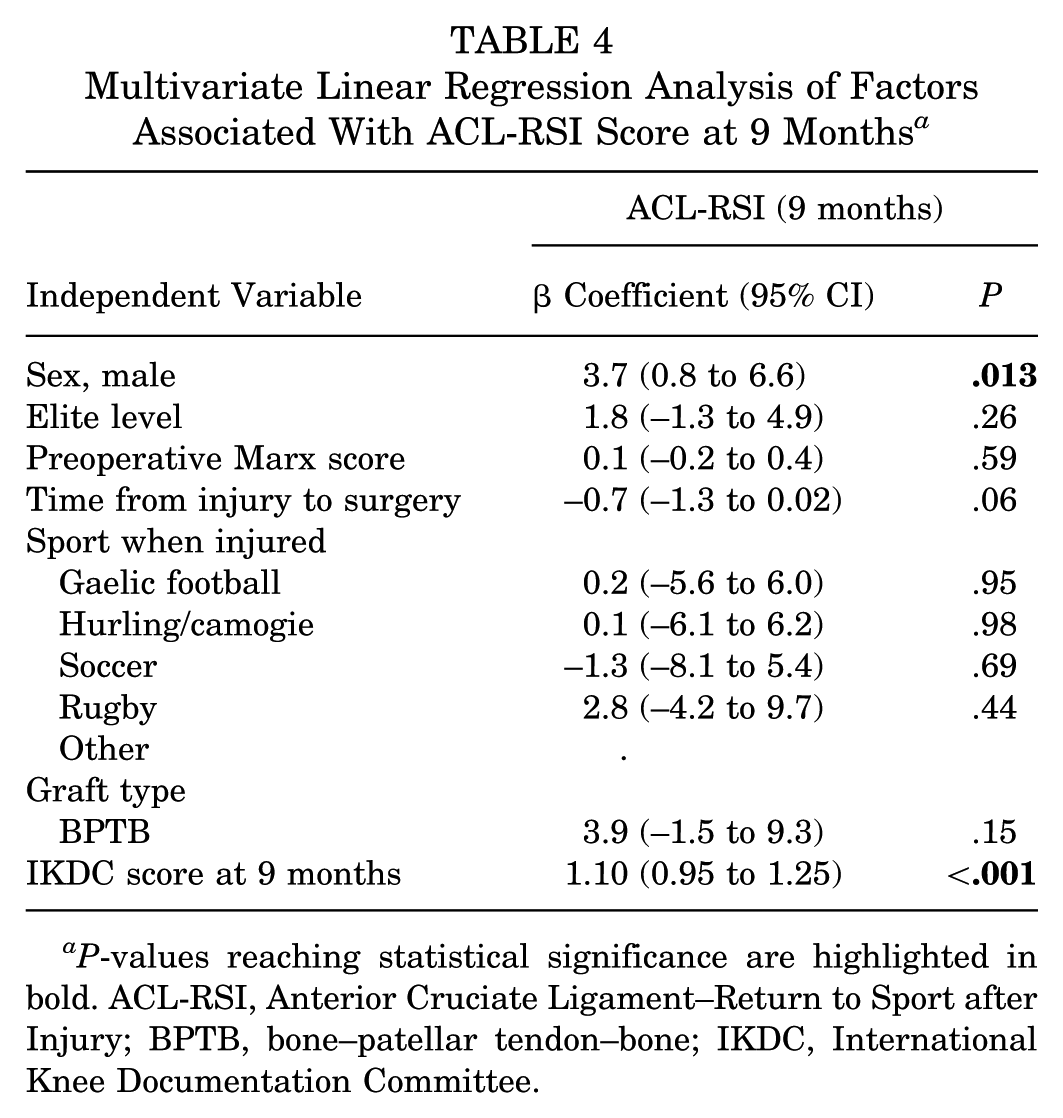
P-values reaching statistical significance are highlighted in bold. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; BPTB, bone–patellar tendon–bone; IKDC, International Knee Documentation Committee.

Improvement trajectory in Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) score throughout rehabilitation for elite and nonelite athletes (stratified by sex). Markings outside of the IQR bars represent outliers. Preop, preoperative.
Discussion
This study identified distinct differences in psychological readiness between elite and nonelite athletes. A major finding of our study was that preoperative ACL-RSI scores were comparable between the 2 cohorts (50.6 vs 48.1 points; P = .28), suggesting that performing at an elite level does not inherently influence baseline reaction to injury and the prospect of undergoing surgery. However, elite athletes exhibited higher ACL-RSI scores at all time points, reaching significantly higher ACL-RSI scores by 9 months (72.7 vs 68.6 points; P < .009) and ultimately achieving higher RTP rates at 1 year (86% vs 69%; P < .001) and 2 years (94.% vs 86.7; P < .002). Multivariable analysis revealed that knee function and male sex were the strongest predictors of ACL-RSI score. This highlights the importance of effective rehabilitation and that there are sex-based differences in psychological response to ACL injury.
This study found that preoperative ACL-RSI scores vary widely, reflecting a diverse range of responses to injury among elite and nonelite athletes across different sports. It is therefore likely that factors beyond elite performance, such as personality traits, coping mechanisms, and athletic identity, play a more significant role in the initial response to injury. 35 This observation is interesting considering previous research has suggested that competitive athletes may experience increased mood disturbances after an ACL injury due to frustration and fear of not returning to their previous performance level. 24 However, emotional responses to injury are likely more nuanced and highly individual, influenced by personal circumstances, previous injury experiences, availability of support systems, and emotional resilience.
This study also demonstrated that elite athletes had higher ACL-RSI scores at all time points compared with nonelite athletes. This may be a reflection of their self-efficacy, which refers to an individual's confidence in his or her ability to maintain control over goal attainment despite challenges or obstacles. Self-efficacy is developed through successfully overcoming previous challenges. 5 It may also be due to a strong athletic identity, which has been found to play a crucial role in rehabilitation adherence and level of sports participation.8,17 Importantly, our results show that subjective knee symptoms and function were the main determinants of psychological readiness. This is relevant because elite athletes are more likely to have access to comprehensive medical and psychological support systems. Furthermore, RTP rates were significantly higher, especially at 1 year postoperatively. Therefore, it would appear that external pressures unique to elite athletes (team or sponsor expectations, career disruption) influence the timing and motivation to return. It is also important to note that a significant part of their identity can be tied to the sport, meaning an extended time away from competition can affect their sense of self-worth. 28
Another key observation from our analysis was that male athletes, whether or not they were elite, had significantly greater psychological readiness than their female counterparts, scoring approximately 4.4 points higher on the ACL-RSI at 9 months postoperatively. Several other studies have identified lower psychological readiness in female athletes at the end of rehabilitation.15,29,34 A study by Webster et al 34 analyzed the factors associated with ACL-RSI scores at 12 months and reported that male athletes scored approximately 5.8 points higher than female athletes. The other factors identified in their study were similar to ours, including a shorter time interval from injury to surgery, higher IKDC scores, and more frequent sports participation before surgery. While their study also found an association between improved ACL-RSI scores and younger age, they included participants of all ages, whereas our study focused on athletes aged between 18 and 35. 34 The growing evidence that sex significantly influences ACL-RSI scores underscores the need to identify the unique challenges female athletes encounter during rehabilitation and to develop targeted interventions to address them.
The ACL-RSI scores of male elite (77.1 points) and nonelite (75 points) athletes at 9 months in this study were quite high compared with other studies. 29 In fact, these scores are close to the scores achieved by a baseline cohort of uninjured male athletes in another study (80 points). 27 This is reflected in the high rates of RTP in this study, which are typically seen in the Gaelic games and the field sports played in Ireland. 21 The participants in this study also underwent supervised strength and biomechanical testing at regular intervals at our hospital, which may have influenced their self-efficacy and confidence in their physical recovery to make a full return.
Psychological recovery has been identified as a potentially modifiable factor that can be targeted during ACL rehabilitation to improve RTP rates. Previous studies have shown that over 40% of patients have psychological reasons for not returning to play.19,35 However, it is important to note that when analyzing the effect of these interventions, the ACL-RSI score is responsive to measuring psychological changes at the group level but less responsive when individuals are assessed alone given the complexity of individual psychological responses. 32 Webster et al32 found that the smallest detectable change (the minimum score change that surpasses measurement error) was 1.8 for male patients and 1.7 for female patients when analyzed as part of a group, but >20 points when assessed individually. When selecting those who required psychological intervention, previous studies have set the cutoff score for the ACL-RSI at 56 points at 12 months.4,25 Other studies have identified ACL-RSI cutoff values ranging from 51 to 60 points at 6 months after ACLR. 29
Strengths and Limitations
The strengths of this study are the large sample size, prospective data collection with a high response rate, and the 2-year follow-up. However, this study also had several limitations. A variety of postoperative rehabilitation protocols were used and no formal RTP protocol was employed because of the size of the cohort and the number of sports involved. Therefore, the extent of psychological support received by different participants was unknown. However, these variations may increase the generalizability of the findings, as they may reflect the diversity of rehabilitation processes employed. Furthermore, while the ACL-RSI score was completed during the same appointment that patients attended their strength and functional tests, we did not strictly control when the questionnaires were administered. Although the difference between completing the ACL-RSI score before and after completing functional testing has not been reported in the literature, athletes’ perception of their readiness to return to sport may be influenced by how well they believed they performed during the tests and the feedback they would have received from their rehabilitation specialist.
Conclusion
Our study demonstrated no significant difference between the preoperative ACL-RSI scores of elite and nonelite athletes. However, elite athletes had higher ACL-RSI scores during rehabilitation. IKDC score at 9 months and male sex were the 2 factors most strongly associated with improved psychological readiness at 9 months. Being an elite athlete is not a primary predictor of psychological readiness and psychological intervention should be considered in all athletes. Future studies should investigate the role of psychological intervention in improving rates of return to sport in elite and nonelite athletes, although they must be sex specific.
Footnotes
Final revision submitted May 29, 2025; accepted July 8, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.M. receives research funding under the Strategic Academic Recruitment (StAR) programme of the Royal College of Surgeons Ireland. The content of this manuscript is solely the responsibility of the authors and was not influenced by the funding entity. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from UPMC Sports Surgery Clinic (reference No. 25-AFM-010).