
Abstract
Background:
The relationship between meeting return-to-sport criteria and psychological readiness after anterior cruciate ligament (ACL) reconstruction is unknown.
Purposes:
To examine (1) whether patients who met 1 of the criteria for return to sport had higher psychological readiness than those who did not meet any of the criteria and (2) if those who met more criteria had higher psychological readiness.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This study included 144 patients who underwent unilateral ACL reconstruction. All patients had regularly participated in some sport activities before an ACL rupture. At 12 months postoperatively, each patient completed 3 knee function tests (isokinetic quadriceps strength, isokinetic hamstring strength, and single-leg hop distance) and 2 self-reported measures (International Knee Documentation Committee [IKDC] 2000 subjective form and ACL–Return to Sport after Injury [ACL-RSI] scale); the ACL-RSI scale was used to measure psychological readiness to return to sport. The 4 criteria for return to sport were a limb symmetry index (LSI) ≥90% for each of the 3 function tests in addition to an IKDC score ≥90. Multivariate regression analysis was used to determine the association between meeting the individual criteria and the ACL-RSI score. In addition, the patients were divided into 5 groups according to the number of criteria met, and the Kruskal-Wallis and Steel-Dwass tests were used to compare the ACL-RSI scores among the groups.
Results:
Overall, 23 patients (16.0%) met none of the criteria for return to sport, 27 (18.7%) met 1 of the criteria, 34 (23.6%) met 2 criteria, 35 (24.3%) met 3 criteria, and 25 (17.4%) met all 4 criteria. Meeting the criteria for the hamstring strength LSI (P = .002), single-leg hop distance LSI (P = .004), and IKDC subjective score (P < .001) was each associated with higher ACL-RSI scores. Significant differences in ACL-RSI scores were found between patients who met none versus 2, 3, and 4 of the return-to-sport criteria (P < .001 for all) and between patients who met 1 versus 4 criteria (P < .001).
Conclusion:
Meeting return-to-sport criteria was positively associated with psychological readiness, and the patients who met multiple criteria had higher psychological readiness.
Keywords
Returning to preinjury sport activities and preventing graft reinjuries are important outcomes after anterior cruciate ligament (ACL) reconstruction. However, the results have not been satisfactory, as the rate of return to preinjury sport remains 65% 4 and that of reinjuries is 10% to 22%, 35 despite improved restoration of knee stability. Recent studies have reported that psychological factors as well as knee function affect returning to preinjury sport after ACL reconstruction. 5,9,18,25
The ACL–Return to Sport after Injury (ACL-RSI) scale is a validated measurement tool to quantify emotional well-being, confidence in performance, and risk appraisal of reinjuries. 31 Because the scores are associated with not only return to sport 3,16,21,22,27 but also secondary ACL injuries, 21 clarifying the factors associated with the ACL-RSI score is important to improve both return-to-sport and secondary ACL injury rates. Several studies have shown that postoperative knee function, such as that assessed using the International Knee Documentation Committee (IKDC) 2000 subjective form and single-leg hop distance, is associated with the ACL-RSI score. 1,20,26,33 The results suggested that proper restoration of knee function may be associated with a higher ACL-RSI score.
Limb symmetry indices (LSIs) of lower extremity muscle strength and hop performance, calculated by dividing the muscle strength and performance of the involved leg by the uninvolved leg, are frequently used as indicators of the recovery of knee function and physical performance. An LSI >90% is considered to be an acceptable threshold for return to sport after ACL reconstruction. 7,10 Previous studies have reported that meeting these return-to-sport criteria was associated with a higher rate of return to preinjury sport 23,24,29,34 and with a reduced risk of ACL reruptures. 19,32 Because it has also been reported that the ACL-RSI score is related to both the return-to-sport rate 3,16,22,27 and secondary ACL injuries, 21 a positive relationship between psychological readiness to return to sport and meeting return-to-sport criteria has been suggested but not examined.
This study aimed to clarify whether patients who met return-to-sport criteria had higher ACL-RSI scores than did those who did not meet any of the criteria. We also sought to investigate whether the patients with higher ACL-RSI scores met more return-to-sport criteria. We hypothesized that patients who met multiple return-to-sport criteria would have higher ACL-RSI scores than would those who did not meet any of the criteria and that the score would be higher as the number of criteria met increased. The results of this study may help to construct a rehabilitation strategy for return to sport and psychological readiness.
Methods
Patients
This was a single-center, cross-sectional study. Included were patients who underwent unilateral ACL reconstruction between April 2017 and December 2019 and underwent knee function measurements at approximately 12 months after ACL reconstruction. All patients were regular participants in some sport activities before an ACL rupture. Patients were excluded for the following reasons: bilateral ACL reconstruction, multiligament reconstruction and other surgery during or after ACL reconstruction except meniscectomy or meniscal repair, history of ACL reconstruction on the ipsilateral or contralateral side, history of lower limb surgery, no participation in any sport regularly before the ACL injury, or incomplete data. Ethics committee approval for this study was received, and all included patients provided informed consent.
Age at surgery, sex, body mass index, preinjury Tegner activity score, time from injury to surgery, surgical technique (single bundle or double bundle), medial or lateral meniscal injuries (requiring surgical treatment: meniscectomy or repair), and cartilage injuries were recorded from patient interviews and medical records.
Surgical and Rehabilitation Procedures
All patients underwent single-bundle or double-bundle ACL reconstruction using a bone–patellar tendon–bone graft or hamstring tendon (semitendinosus and/or gracilis) autograft as previously described. 17 All patients underwent the same postoperative rehabilitation regimen consisting of a time-based protocol for the first 6 months, with a focus on improvement of range of motion deficits, lower extremity muscle strength, and functional limitations. Patients were allowed to participate in sport-specific practices approximately 9 months after surgery if the surgeon determined that there was no obvious impairment in the knee joint (full range of motion, good quadriceps and hamstring strength, no effusion, and no pain). The following criteria were also considered to allow return to sport: (1) LSI of isokinetic quadriceps and hamstring strength (at 60 deg/s) ≥90%, (2) LSI of single-leg hop performance ≥90%, and (3) no major problems during sport-specific movements. If the patient did not achieve the criteria, he or she was advised not to return to sport. However, the criteria were not strictly applied to all the patients, and the final decision was made via a discussion among the surgeon, physical therapist, trainer (athletic trainer or coach), and patient.
Knee Function Measures
Isokinetic quadriceps and hamstring strength at 60 deg/s were measured using an isokinetic dynamometer (Genu PLUS; Inter Reha). Muscle strength testing was performed after patients warmed up using a stationary cycle ergometer at a low resistance for 5 minutes. Strength tests were performed using 2 practice contractions, followed by 5 maximal-effort contractions at 60 deg/s with the healthy limb first, followed by the operated limb. The peak extension and flexion torque were recorded, and the LSI was calculated by dividing the peak torque of the involved leg by the peak torque of the uninvolved leg and multiplying by 100.
The single-leg hop was measured for performance testing. We recorded the maximal distance between 2 trials for the operated and uninvolved limbs. Single-leg hop performance was expressed via the LSI, which was calculated by dividing the maximal distance of the involved limb by the maximal distance of the uninvolved limb and multiplying by 100.
The IKDC subjective form was used to measure patient-reported knee function. This joint-specific outcome measure consists of 18 items, and scores range from 0 to 100, with higher scores indicating better subjective knee function. The IKDC subjective form has been shown to be a valid, reliable, and responsive measure of outcomes after ACL reconstruction. 12,14
Anterior knee laxity was measured using a KT-2000 arthrometer (MEDmetric) with maximum manual force. The side-to-side difference in anteroposterior tibial displacement between the operated and contralateral knees was recorded. The heel-height difference was measured to evaluate the loss of knee extension. 28
Criteria for Return to Sport
After referring to previous studies, 7,29,30 we evaluated the following 4 criteria used typically to screen patients for return to sport:
isokinetic quadriceps strength LSI ≥90%,
isokinetic hamstring strength LSI ≥90%,
single-leg hop distance LSI ≥90%, and
IKDC subjective score ≥90.
Patients who could not perform a single-leg hop because of knee pain, anxiety, or other reasons were considered as having a single-leg hop distance LSI <90%. 24
Psychological Readiness to Return to Sport
Each patient completed the Japanese version of the ACL-RSI scale before the knee function measurements. This scale consists of 12 items and includes 3 domains: emotions, confidence, and risk appraisal. Each score was summed and averaged between 0 and 100, with higher scores indicating greater psychological readiness. This scale has been previously validated for use in patients after ACL reconstruction. 13,31
Study Groups
We used an original self-administered question to determine which patients returned to preinjury levels of sport after surgery: “Have you been able to return to the sport that you had played before the injury?” Based on a 2016 consensus statement, 2 return to sport was defined as participating in a match or practice game for the same preinjury sport. Based on the responses to this question, patients were divided into 2 groups: the return-to-sport (RTS) group and the no return-to-sport (NRTS) group.
Statistical Analysis
Continuous variables were presented as the mean ± standard deviation. The Shapiro-Wilk test was used to confirm the normality of continuous variables. Categorical variables were presented as frequencies and percentages and were treated as dummy variables in the analyses.
Patient characteristics, surgical data, and postoperative knee function were compared between the RTS and NRTS groups using the unpaired t test, Mann-Whitney U test, and chi-square test. The proportion of patients meeting each return-to-sport criterion was calculated. Univariate and multivariate regression analyses were used to investigate whether an individual return-to-sport criterion was associated with the ACL-RSI score. For the multivariate analysis, we entered age at surgery, sex, preinjury Tegner score, and time from injury to surgery as covariates, which were shown to be associated with the ACL-RSI score according to a study by Webster et al. 33
In addition, the patients were divided into 5 groups according to the number of criteria met (0-4). The proportion of each group based on the number of criteria met was calculated, and the Jonckheere-Terpstra trend test was used to determine whether the ACL-RSI score increased with the number of criteria met. The Kruskal-Wallis and Steel-Dwass tests were used to compare the ACL-RSI scores among the 5 groups. All statistical analyses were performed using EZR for Windows (Version 1.37). 15 Statistical significance was determined a priori at P < .05.
The sample size was calculated using G*Power (Version 3.1.9.4) to achieve an alpha level of .05 and a beta of 80% with a medium effect size of 0.15. Considering the number of independent variables in the multivariate linear regression analysis, the minimum sample size was 103 patients.
Results
Patient and Return-to-Sport Data
Included in this study were 144 patients (Figure 1). Overall, 11 patients who could not perform a single-leg hop because of knee pain, anxiety, or other reasons were included and were considered as having achieved an LSI <90% for this variable.
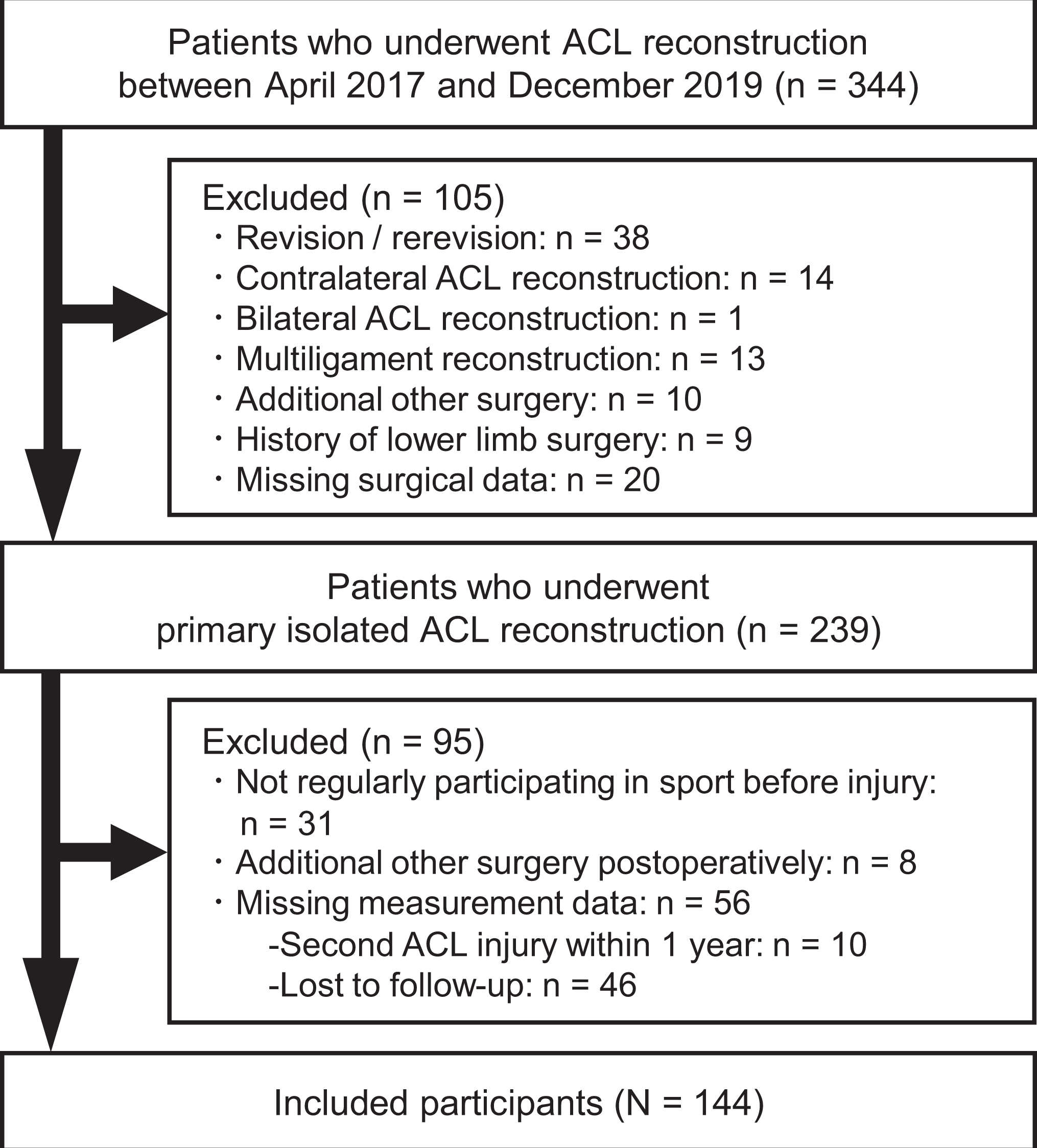
Flowchart of patient inclusion. ACL, anterior cruciate ligament.
Patient characteristics, surgical data, and knee function at 1 year after surgery are shown in Tables 1 and 2. Of 144 patients, 95 patients (66.0%) were included in the RTS group, and 49 patients (34.0%) were included in the NRTS group. The RTS group was significantly younger than the NRTS group (P = .02). Values were significantly higher in the RTS group than in the NRTS group for the quadriceps strength LSI (P = .04), hamstring strength LSI (P = .01), single-leg hop distance LSI (P = .02), IKDC subjective score (P < .001), and ACL-RSI score (P < .001).
Patient Descriptive and Surgical Data a
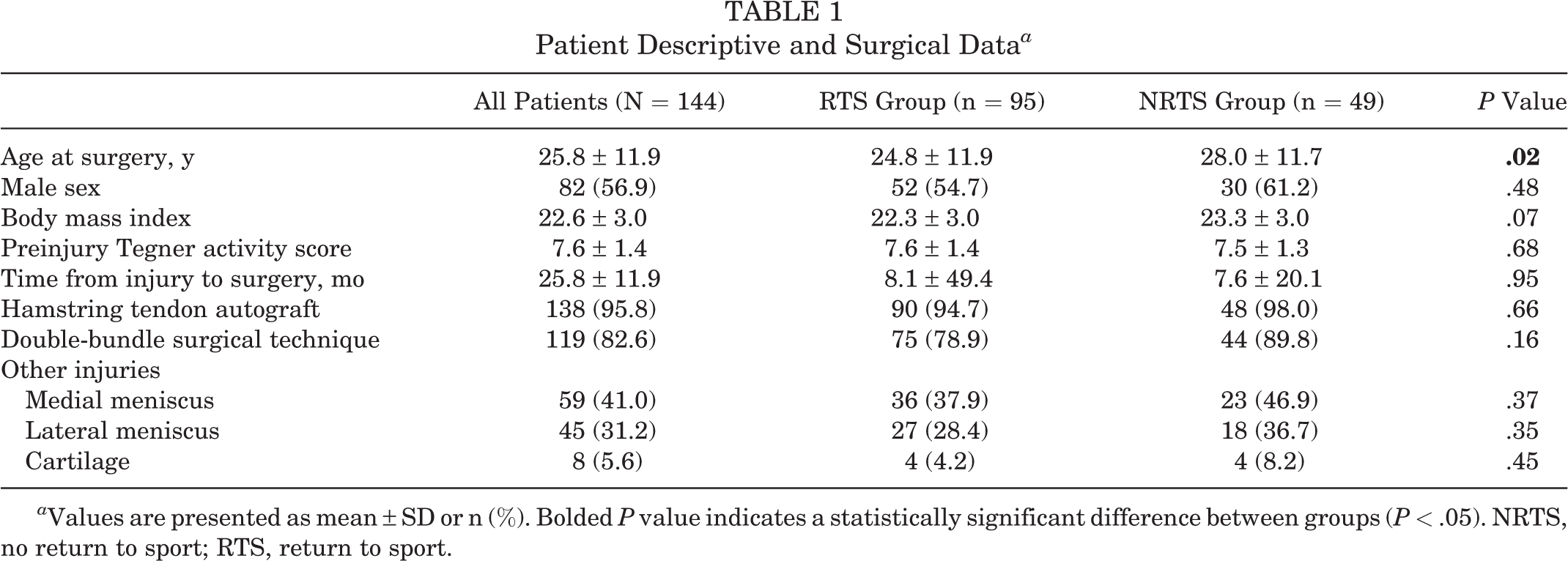
a Values are presented as mean ± SD or n (%). Bolded P value indicates a statistically significant difference between groups (P < .05). NRTS, no return to sport; RTS, return to sport.
Postoperative Knee Function a
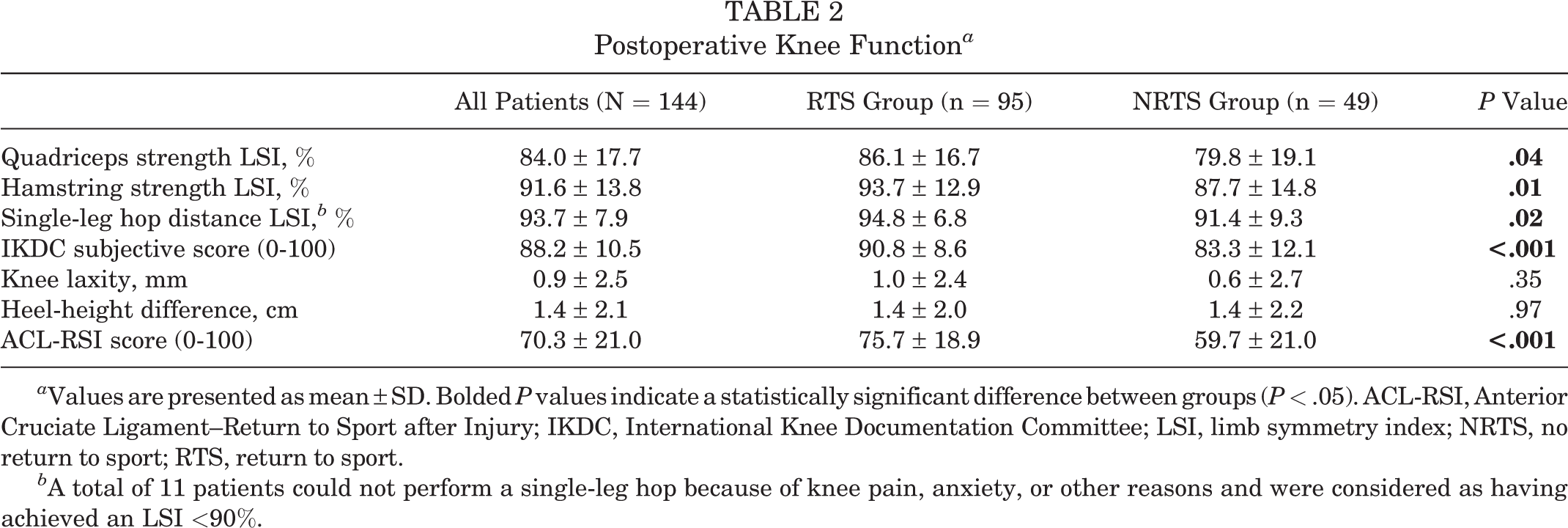
a Values are presented as mean ± SD. Bolded P values indicate a statistically significant difference between groups (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; LSI, limb symmetry index; NRTS, no return to sport; RTS, return to sport.
b A total of 11 patients could not perform a single-leg hop because of knee pain, anxiety, or other reasons and were considered as having achieved an LSI <90%.
Association Between Return-to-Sport Criteria and ACL-RSI Score
The proportion of patients who met the criteria for the quadriceps strength LSI, hamstring strength LSI, single-leg hop distance LSI, and IKDC subjective score were 37.5% (n = 54), 52.1% (n = 75), 67.4% (n = 97), and 51.4% (n = 74), respectively. In the univariate analysis, patients who met the return-to-sport criteria for hamstring strength, single-leg hop distance, and IKDC subjective score had higher ACL-RSI scores (P < .001 for all). However, meeting the criterion for quadriceps strength was not associated with the ACL-RSI score in the univariate analysis. The multivariate logistic regression analysis with age at the time of surgery, sex, preinjury Tegner score, and time from injury to surgery as covariates showed similar results to those of the univariate analysis (P ≤ .004 for all) (Table 3).
Association Between Return-to-Sport Criteria and ACL-RSI Score a
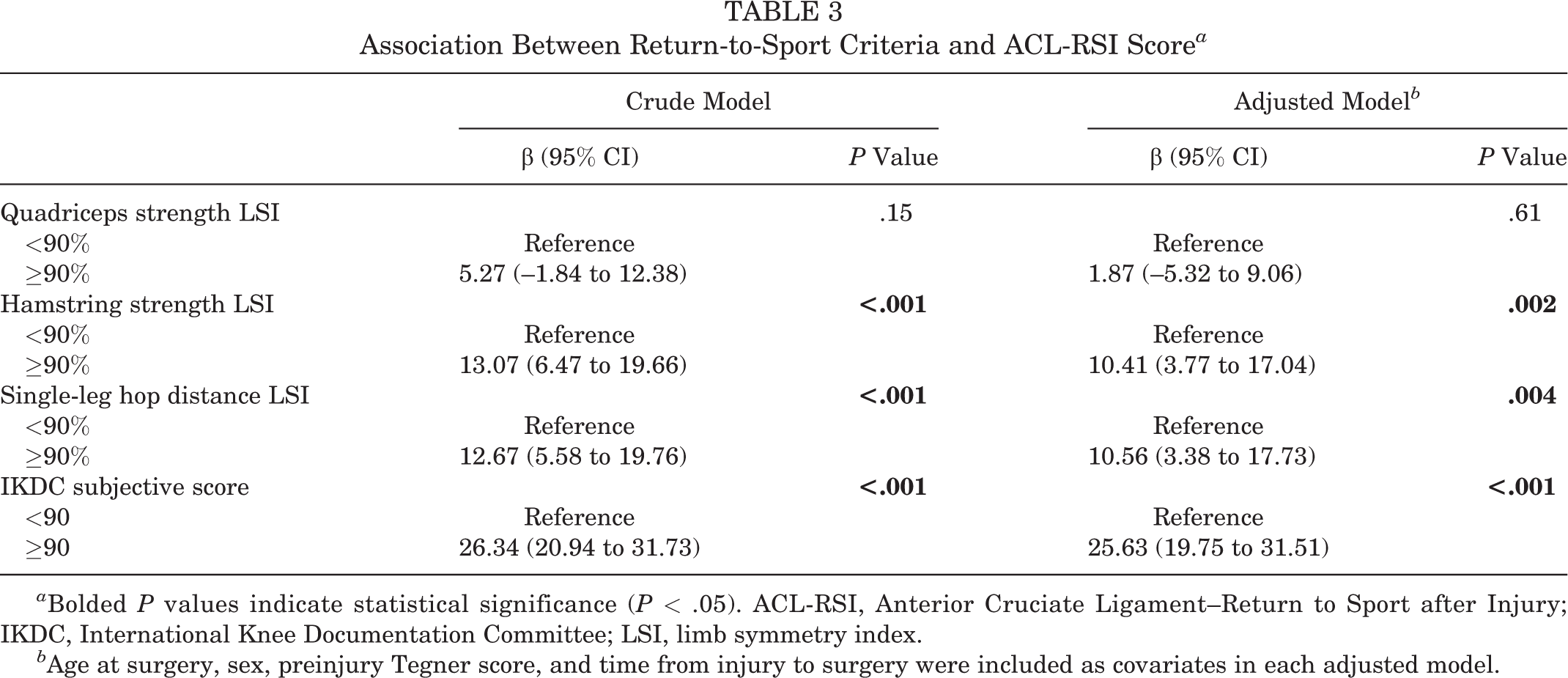
a Bolded P values indicate statistical significance (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; LSI, limb symmetry index.
b Age at surgery, sex, preinjury Tegner score, and time from injury to surgery were included as covariates in each adjusted model.
Association Between Number of Criteria Met and ACL-RSI Score
Overall, 23 patients (16.0%) met none of the criteria for return to sport, 27 (18.7%) met 1 of the criteria, 34 (23.6%) met 2 criteria, 35 (24.3%) met 3 criteria, and 25 (17.4%) met all 4 criteria (Table 4).
Distribution of Patients According to Number of Return-to-Sport Criteria Met a
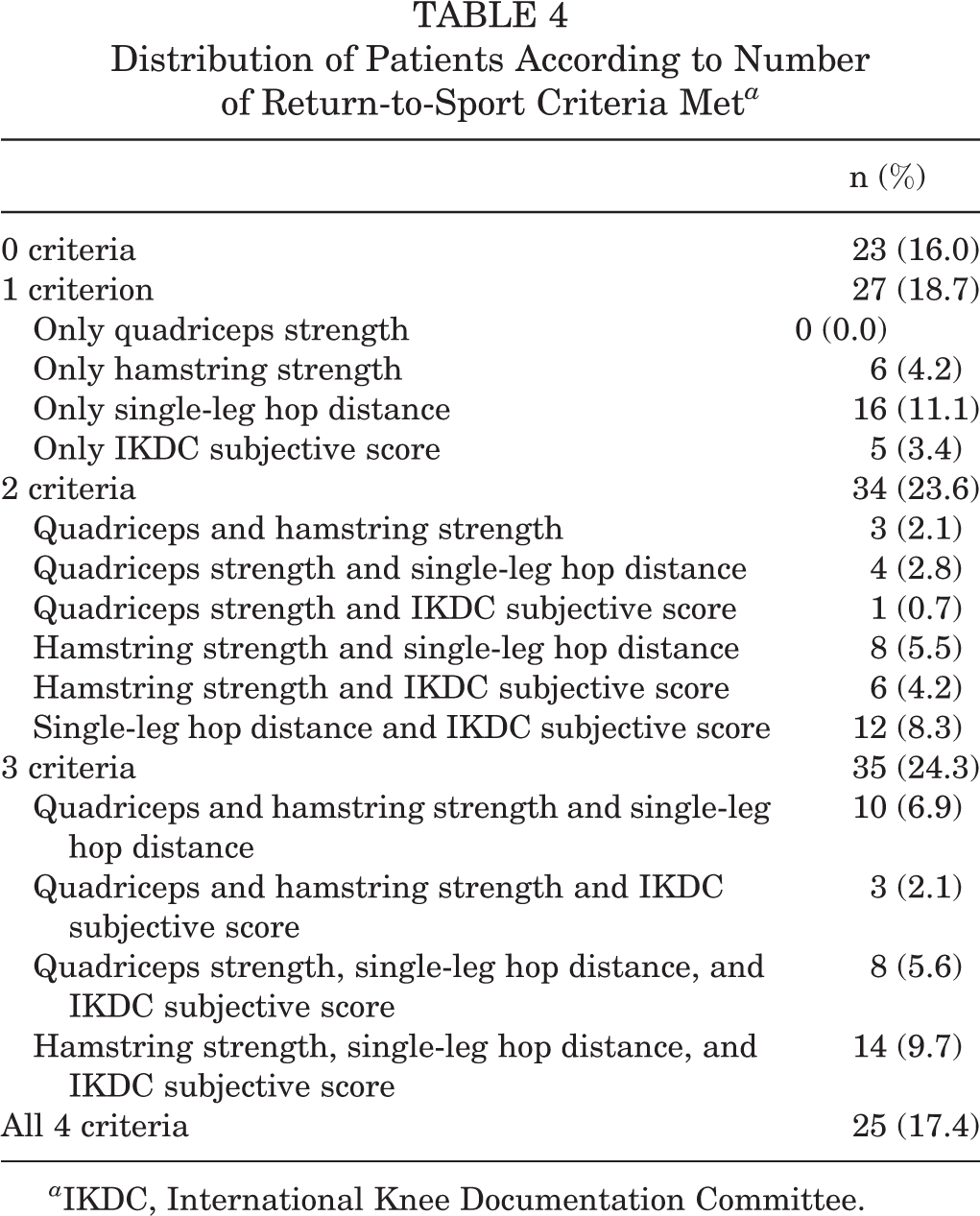
a IKDC, International Knee Documentation Committee.
The results of the Jonckheere-Terpstra trend test indicated that the mean ACL-RSI score significantly increased as the number of criteria met increased (P < .001). Although the difference was not statistically significant between consecutive groups, significant differences were found between patients who met no criteria (51.3 ± 15.5) and those who met 2 criteria (72.9 ± 22.1), 3 criteria (74.7 ± 17.7), and 4 criteria (85.7 ± 12.4) (P < .001 for all). A statistically significant difference was also observed between patients who met 1 criterion (63.1 ± 20.3) and 4 criteria (P < .001) (Figure 2).
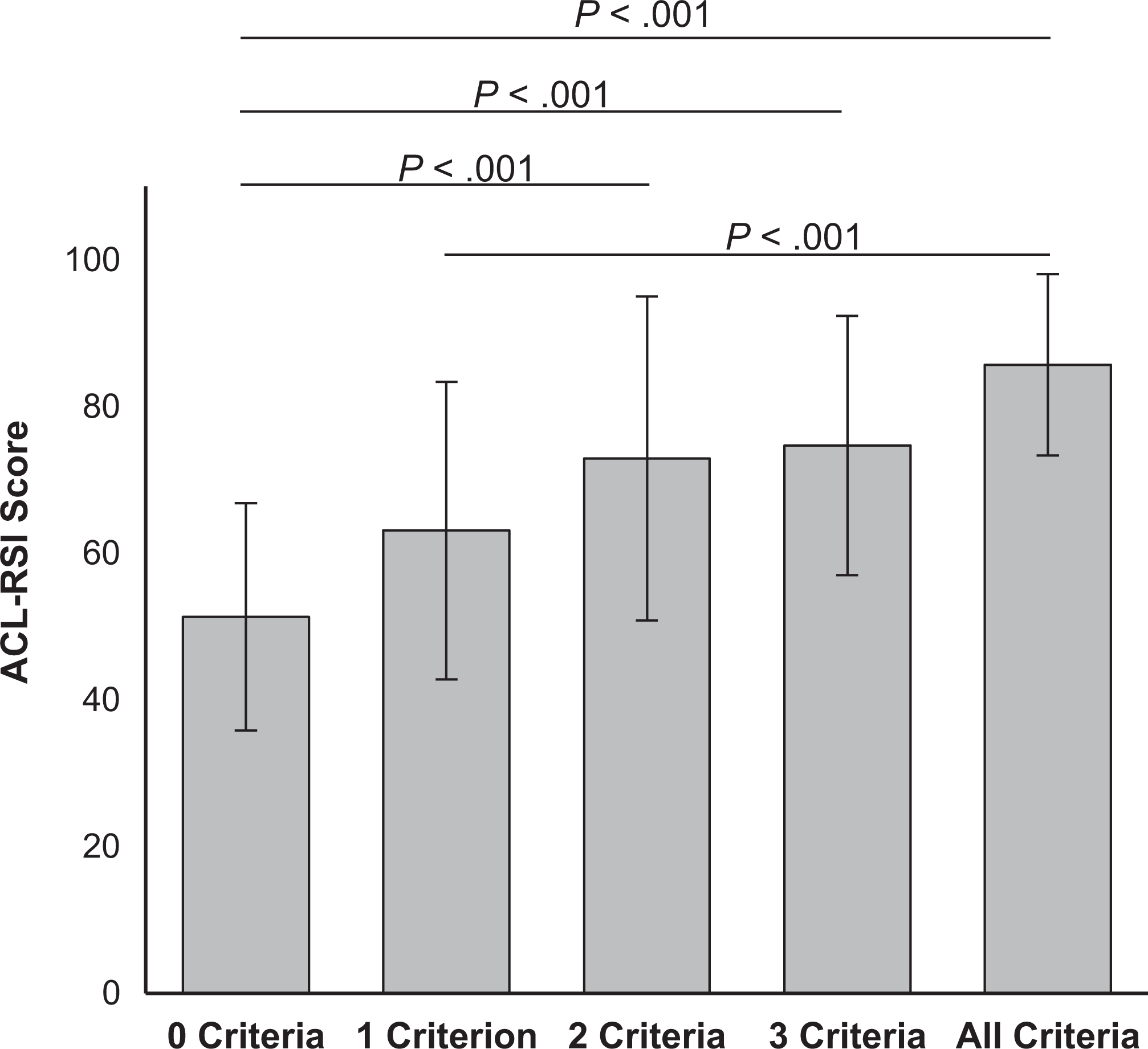
Comparison of Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scores according to the number of return-to-sport criteria met.
Discussion
In the present study, patients who returned to their original sport level had higher knee function and ACL-RSI scores compared with those who did not (P < .001). This study also demonstrated that meeting each return-to-sport criterion, except quadriceps strength, was positively associated with the ACL-RSI score (P < .01 for all). In addition, patients who met multiple criteria for return to sport had a higher ACL-RSI score than did those who did not meet any of the criteria (P < .001 for all), and the score tended to be higher as the number of criteria met increased (P < .001).
Recent studies have investigated factors associated with the ACL-RSI score. Webster et al 33 investigated the factors that contribute to the ACL-RSI score in athletes at an average of 12 months (range, 11-24 months) after ACL reconstruction using a hamstring tendon autograft. They revealed that self-reported symptoms and function, as measured using the IKDC subjective form, had the most significant associations with the ACL-RSI score. Additionally, Aizawa et al 1 showed that the LSI of the lateral single-leg hop distance was independently associated with the ACL-RSI score at 6 months after ACL reconstruction in athletes who participated in cutting, pivoting, and jump-landing sports. The current study also found that meeting each criterion for hamstring strength, single-leg hop distance, and IKDC subjective score was independently associated with the ACL-RSI score at 12 months after ACL reconstruction. The study findings suggest that objective knee function test results and subjective knee function outcomes are related to the ACL-RSI score.
In the present study, meeting the criterion for quadriceps strength was not associated with the ACL-RSI score. O’Connor et al 26 reported that the ACL-RSI score at 9 months after ACL reconstruction had no significant relationship with quadriceps strength and the height of a single-leg countermovement jump and a single-leg drop jump in male athletes. Similarly, quadriceps strength was not associated with the ACL-RSI score in a study by Aizawa et al. 1 Contrarily, Lepley et al 20 reported that maximum voluntary isometric contraction of the injured limb for quadriceps strength at the time of return-to-sport activities (28.3 ± 2.9 weeks after ACL reconstruction) was significantly related to the ACL-RSI score. Because a wide variation in patient activity levels, timing, and methods of measurement exists among previous reports, further research is needed to investigate whether quadriceps strength affects the ACL-RSI score at the time of return to sport.
Regarding the association between meeting multiple return-to-sport criteria and the ACL-RSI score, the results showed that patients who met multiple criteria (2-4) for return to sport had a higher ACL-RSI score than did those who did not meet any of the criteria, and the score tended to be higher as the number of met criteria increased. In a previous study, Beischer et al 6 divided participants into 2 groups, recovered and nonrecovered, according to whether LSIs of 5 lower limb muscle function tests (knee extension and flexion strength, unilateral vertical hop, single-leg hop for distance, and side hop) were ≥90%. They compared the ACL-RSI score between the 2 groups at 8 months and 12 months after ACL reconstruction and reported no significant difference between the groups. The discrepancy in these results may be because of differences in the classification of the participants. In the study of Beischer et al, patients who met none to 4 of 5 criteria were included in the nonrecovered group. Therefore, it is possible that the average score in the nonrecovered group became high because of relatively higher scores in patients who met multiple criteria, such as 3 and 4 criteria, and the difference was not significant. Despite the difference, our results at least suggested that meeting multiple criteria could be associated with better psychological readiness after ACL reconstruction.
Several studies have reported that meeting return-to-sport criteria was associated with an increased rate of return to preinjury sport after ACL reconstruction. 23,24,29,34 A recent systematic review and meta-analysis suggested that meeting return-to-sport criteria could significantly reduce the risk of ACL reruptures. 32 Meanwhile, there is limited evidence that shows that psychological interventions improve the return-to-sport rate and reduce the reinjury rate. 8 In the present study, meeting return-to-sport criteria was positively associated with psychological readiness. Therefore, meeting as many return-to-sport criteria as possible, which can be associated with better psychological readiness, would be the primary strategy for returning to preinjury sport. However, further research is required to address this question.
Limitations
There were some limitations to this study. First, this was a single-center, cross-sectional study. Thus, the generalizability and causality of the results should be examined via additional multicenter and longitudinal studies. Second, we could not assess whether specific combinations of the functional criteria used in this study might have differing effects on the ACL-RSI score because of an insufficient number of patients. Therefore, it is unclear which combination of muscle strength, single-leg hop distance, and IKDC subjective score is more associated with the ACL-RSI score. Third, other indicators for returning to sport used in previous studies, 10,11,29,34 such as the crossover hop, single-leg triple hop, the Landing Error Scoring System score, and the global rating scale score of perceived function, were not measured in this study. However, this study measured muscle strength, single-leg hop performance, and patient self-reported function, which were examined by numerous previous studies 7 and provided useful information. Fourth, because there was variability among the surgeons with respect to allowing return to sport, there may have been bias in decision making. In addition, we used LSIs of knee muscle strength as part of our own criteria for allowing return to sport. Therefore, the significantly lower values for these return-to-sport criteria in the NRTS group were a natural result of our screening process. Finally, this study did not examine the relationship of the return-to-sport criteria or the ACL-RSI score with ACL reinjuries.
Conclusion
In the current study, patients who met multiple return-to-sport criteria had higher psychological readiness according to the ACL-RSI score compared with patients who did not meet any of the criteria, and the ACL-RSI score was higher as the number of met criteria increased.
Footnotes
Acknowledgment
Final revision submitted January 11, 2022; accepted February 17, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from the Japan Sports Medicine Foundation (2020). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Kobe University Graduate School of Medicine (No. B190055).