
Abstract
Background:
Successful return to sport after anterior cruciate ligament (ACL) reconstruction (ACLR) can be affected by a patient’s physical and psychological state throughout the rehabilitation process.
Purpose:
To prospectively compare differences in patients at 6 months after primary ACLR with the ACL–Return to Sport after Injury (ACL-RSI), International Knee Documentation Committee (IKDC) or pediatric (Pedi)-IKDC, Hospital for Special Surgery Pediatric Functional Activity Brief Scale (Pedi-FABS), and Patient-Reported Outcomes Measurement Information System–Psychological Stress Experiences (PROMIS-PSE) scores.
Study Design:
Prospective cohort study; Level of evidence, 2.
Methods:
Patients enrolled were 8 to 35 years old who underwent primary ACLR and had their 6-month follow-up appointments between December 2018 and March 2020. Patients were divided into 3 age groups as follows: (1) preadolescents (10-14 years); (2) adolescents (15-18 years); and (3) adults (>18 years). Outcomes on the ACL-RSI, IKDC/Pedi-IKDC, Pedi-FABS, and PROMIS-PSE were compared according to age group, graft type (hamstring, patellar tendon, quadriceps, or iliotibial band autograft), and sex.
Results:
A total of 176 patients (69 male, 107 female), with a mean age of 17.1 ± 3.1 years were included in the study. The mean ACL-RSI scores were significantly different among age groups (preadolescents, 75 ± 18.9; adolescents, 61.5 ± 20.4; and adults, 52.5 ± 19.8 [P < .001]) and graft types (P = .024). The IKDC and PROMIS-PSE scores were also significantly different among age groups (P < .001 and P = .044, respectively) and graft types (P = .034 and P < .001, respectively), with the iliotibial graft and the younger age group performing the best. There was no significant difference in the Pedi-FABS either by age group (P = .127) or graft type (P = .198). Female patients had lower ACL-RSI scores and higher (worse) scores on PROMIS-PSE than their male counterparts (P = .019 and P < .001, respectively), with no sex-based differences on IKDC or Pedi-FABS scores. The ACL-RSI and IKDC were positively correlated (Spearman r = 0.57; P < .001), while the ACL-RSI and PROMIS-PSE were negatively correlated (Pearson r = –0.34; P < .001).
Conclusion:
This study suggests that psychological profiles and subjective perceptions of knee function 6 months after ACLR may vary in patients of different ages and between the sexes. Preadolescent patients had better scores on a majority of patient-reported outcomes compared with adolescent and adult patients.
Anterior cruciate ligament (ACL) tear is one of the most common orthopaedic sports injuries and the number of ACL reconstructions (ACLRs) has increased significantly over the past 15 years. 33,44 While the overall incidence of ACLRs has increased by 43% across all age groups, it has increased by 74% in patients aged <25 years. 44 One study found that the number of ACLRs performed on patients aged <15 years had increased 10,11,38 by 924% between 1994 and 2006.
Reinjury continues to be a major concern after ACLR. Younger patients have a reinjury risk between 18% to 23%, while adult populations have a lower risk of reinjury. 5,41,43 Return to preinjury level of sports and activities after ACLR has varied in the literature from 44% to 80%. 3,5,7,21,23,24 The rate is highest in younger patients, 7 with 80% returning to prior activity level. However, this comes with a higher rate of reinjury at around 20%. Patients seem to be most at risk of ACL reinjury during the first 1 to 2 years after ACLR with the risk of injury within the first year reported 15 to be as high as 50%. Fear of reinjury has been identified as a major factor in decision making for return to sports (RTS) after ACLR. 24
RTS is commonly used as a measure of the success of ACLR and is often essential to patients and their families. A variety of factors have been identified to guide RTS decision, including time from surgery, strength testing, functional testing, patient-reported outcome (PRO) scores, and psychological factors. 16 As the understanding of psychological readiness after ACLR has improved, previous studies have identified that younger age positively affects psychological readiness. 42 However, it is unknown how other factors such as sex or graft type affect psychological readiness. Even though there are different graft types used for different age groups, it is of interest to observe how the PRO scores vary across the graft types and age groups separately.
The purpose of this study was to assess the level of psychological readiness and psychological stress in young athletes and compare it with other commonly utilized PROs. We hypothesized that there would be an inverse relationship between psychological stress and psychological readiness and that PRO scores would not differ significantly with age, sex, or graft types at 6 months after ACLR.
Methods
In this prospective cohort study, we identified patients between the ages of 8 and 35 years who underwent primary ACLR between December 2018 and March 2020. Patients were included if they had a primary ACLR and completed PRO measures between 5 to 8 months postoperatively at their clinical visit closest to 6 months postoperatively. ACLR was performed by 1 of 6 orthopaedic surgeons (M.D.M., D.E.K., M.S.K., L.J.M., Y.M.Y, M.A.C.) at a single tertiary-referral pediatric hospital/sports medicine center. Patients who had meniscal repair, partial meniscectomy, lateral extra-articular tenodesis, or anterolateral ligament reconstruction were included. Exclusion criteria included a history of prior ipsilateral knee surgery, revision ACLR, incomplete PROs, and multiligamentous knee surgery. The graft type selected was based on the preferences of the orthopaedic surgeon and the patient/family considering the patient’s skeletal age and physeal status. Patients received either a hamstring, bone–patellar tendon–bone (BTB), quadriceps, or iliotibial band (ITB) autograft. Demographic and clinical data collected included sex, age, primary sport, time to RTS, and presence of concomitant meniscal pathology.
Patients were divided into 1 of 3 following groups based on their chronological age at the time of their surgery: (1) preadolescents (10-14 years); (2) adolescents (15-18 years); or (3) adults (19-30 years). Although the adult group spanned a large range of ages, it had a mean age of 21.4 years and only 6 patients were aged >23 years; thus, for analysis purposes, it was not further stratified. Postoperative rehabilitation protocols were similar across all orthopaedic surgeons. Patients who received only an ACLR were allowed weightbearing as tolerated immediately after surgery and patients who had both ACLR and a meniscal repair were instructed to have limited weightbearing for the first 6 weeks. All patients were to gradually increase their strength and range of motion over 6 to 12 weeks. The patients were to begin light running and plyometrics if capable approximately 4 months after surgery. RTS testing was done at 6 months after surgery, with the goal in most cases being to have the patient RTS around 9 months after surgery. The results of testing at 6 months allowed for the rehabilitation protocol to be altered for the final stages of rehabilitation if necessary.
Patients completed an electronic or paper version of a questionnaire at their 6-month follow-up appointment. The electronic questionnaire was constructed and administered via a REDCap version 12.0.28 database and was a compilation of 4 PRO measures. The Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) is a measure of psychological readiness to RTS after ACLR, which combines scores across 3 categories of emotion, confidence, and risk appraisal to yield a total score, with a higher score indicating a greater, more positive psychological readiness to RTS. 40 The International Knee Documentation Committee (IKDC) (for patients aged >18 years), and pediatric (Pedi)–IKDC (for patients aged 10-18 years) subjective forms were used to assess knee symptoms and function in activities of daily living. 14,17 Previous studies have not found any clinically significant difference between pediatric and adult IKDC scores. 29,35 Given this, pediatric and adult IKDC scores were directly compared and not converted in our study. The Hospital for Special Surgery Pediatric Functional Activity Brief Scale (Pedi-FABS) quantifies the activity level of athletes. 12 The Patient-Reported Outcomes Measurement Information System Psychological Stress Experiences (PROMIS-PSE) is a validated tool that assesses a patient’s cognitive perception of disruption, controllability, manageability, anger, and fear, with higher T scores indicating higher levels of stress. 6
Statistical Analysis
Continuous variables were summarized using means ± SDs and ranges as needed. Categorical variables were summarized using numbers and percentages. Comparisons between groups were performed with the Fisher exact test for categorical variables and with the independent t test, analysis of variance F test, Wilcoxon rank-sum test, and Kruskal-Wallis test for continuous variables as appropriate. Pearson/Spearman correlation analyses were performed to evaluate the association between outcome measures. Post hoc pairwise comparison testing among the age and graft type groups was performed with Tukey-Kramer adjustments. All tests were 2-sided, and P < .05 was considered statistically significant. SAS Version 9.4 (SAS Institute) software was used.
Results
A total of 176 patients were included in the final patient cohort (Figure 1). The mean age was 17.1 ± 3.1 years (range, 10-30 years). The study included 69 (39.2%) male and 107 (60.8%) female patients. The patients were divided into the following age groups: 29 (16.5%) preadolescents; 105 (59.7%) adolescents, and 42 (23.9%) adults. Graft type distribution was 128 (72.7%) hamstring autografts, 31 (17.6%) BTB autografts, 13 (7.4%) ITB autografts, and 4 (2.3%) quadriceps autografts. Patients who received a hamstring autograft had a mean age of 17.3 years (range, 13-30 years), and those who received a BTB autograft had a mean age of 18.4 years (range, 15-27 years). Patients who received an ITB autograft had a mean age of 12.5 years (range, 10-14 years), and patients who received a quadriceps autograft had a mean age of 15.5 years (range, 14-17 years). No meniscal pathology was present in 84 patients (47.7%), while 33 patients (18.8%) underwent a partial meniscectomy and 59 patients (33.5%) underwent a meniscal repair. A total of 165 participants were most commonly injured while playing sports (93.8%). The participants’ primary sports were soccer (n = 50 [28.4%]), basketball (n = 32 [18.2%]), or lacrosse (n = 19 [10.8%]) (Table 1).

Flowchart of patient inclusion. ACL, anterior cruciate ligament; PRO, patient-reported outcome.
Patient Characteristics (N = 176) a
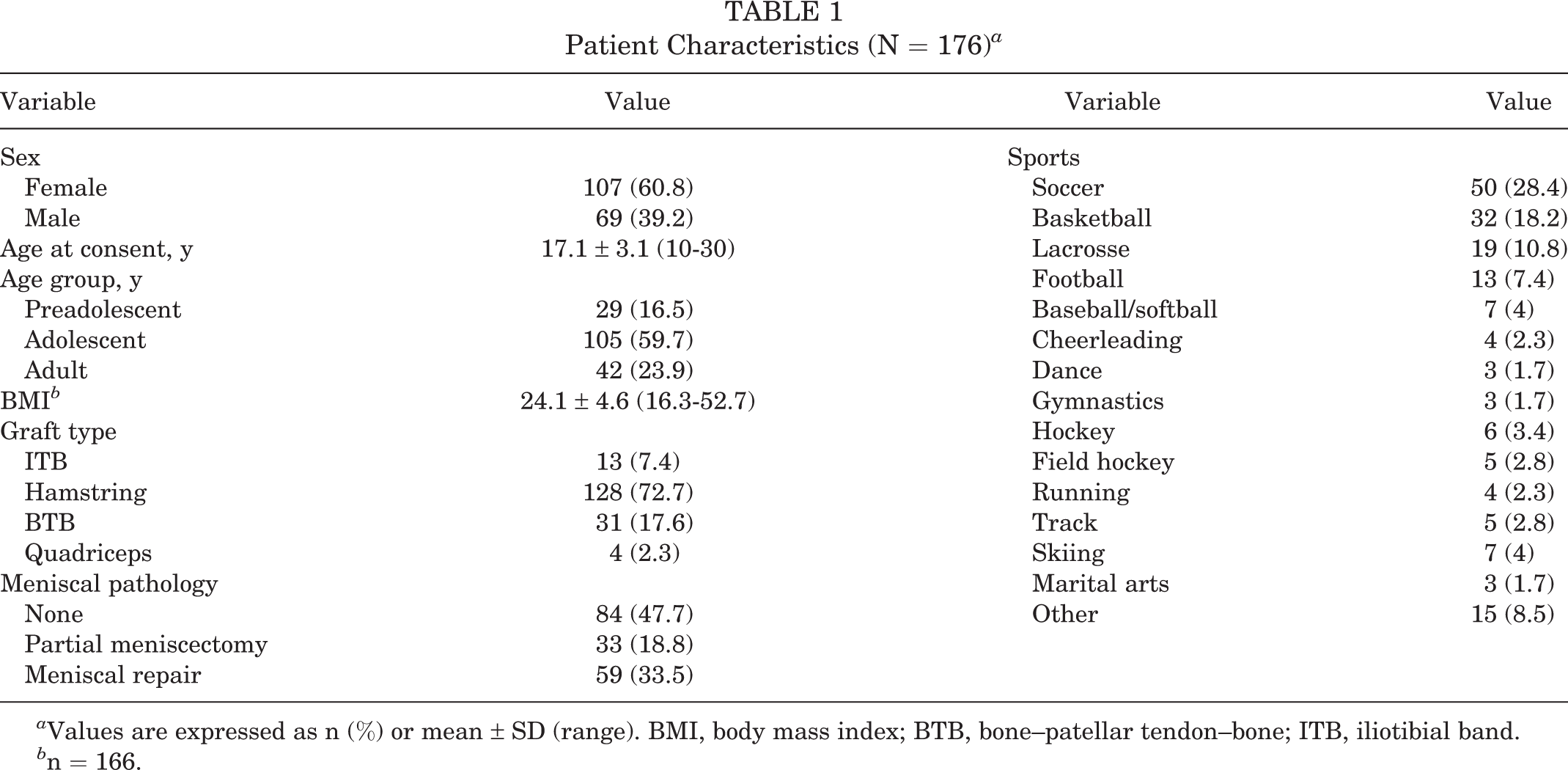
a Values are expressed as n (%) or mean ± SD (range). BMI, body mass index; BTB, bone–patellar tendon–bone; ITB, iliotibial band.
b n = 166.
Patient-Reported Outcomes
There was a significant difference in ACL-RSI scores both across age groups (P < .001) and among graft types (P = .024) (Tables 2 and 3). Younger patients reported significantly higher ACL-RSI scores than both adolescent and adult patients (preadolescents, 75 ± 18.9; adolescents, 61.5 ± 20.4; and adults, 52.5 ± 19.8; pairwise P = .004 and P < .001, respectively). The mean IKDC scores were significantly higher for both preadolescent and adolescent patients compared with adults (preadolescents, 82; adolescents, 78.1; and adults, 61.5; both pairwise P < .001). There were significant differences between IKDC scores among graft types (ITB, 81.8; hamstring, 75.1; BTB, 69.6; and quadriceps, 81.5) (P = .034). PROMIS-PSE scores were also significantly different among age groups (preadolescents, 50 ± 9.3; adolescents, 53.8 ± 8.1; and adults, 54.7 ± 7.4) (Table 2), with adult patients demonstrating more perceived stress than preadolescents (pairwise P = .048). Overall, 3 of the 4 outcome measures (ACL-RSI, IKDC, and PROMIS-PSE) demonstrated significant differences between age groups and graft types, with the younger age group and ITB autograft cohorts demonstrating better scores. There was no significant difference in reported pediatric activity levels based on Pedi-FABS scores between age groups (P = .127) or graft types (P = .198). The mean overall PRO scores were as follows: ACL-RSI, 61.5 ± 21.2 (range, 5.8-99.2); IKDC, 74.8 ± 14 (range, 42.5-100); Pedi-FABS, 22.7 ± 7.7 (range, 0-30); and PROMIS-PSE, 53.4 ± 8.2 (range, 34.2-78.5).
PRO Scores by Age Group a

a Values are expressed as mean ± SD. Bold P values indicate a statistically significant difference between groups (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sports after Injury; IKDC, International Knee Documentation Committee; Pedi-FABS, Pediatric Functional Activity Scale; PRO, patient-reported outcome; PROMIS-PSE, Patient-Reported Outcomes Measurement Information System–Psychological Stress Experience.
b Based on the analysis of variance F tests except for the Pedi-FABS, which was based on the Kruskal-Wallis test.
PRO Scores by Graft Type a

a Values are expressed as mean ± SD. Bold P values indicate a statistically significant difference between groups (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sports after Injury; BTB, bone–patellar tendon–bone; IKDC, International Knee Documentation Committee; ITB, iliotibial band; Pedi-FABS, Pediatric Functional Activity Scale; PRO, patient-reported outcome; PROMIS-PSE, Patient-Reported Outcomes Measurement Information System–Psychological Stress Experience.
b Based on t tests except for Pedi-FABS, which was based on the Wilcoxon rank-sum test.
When examining the effects of sex, female patients scored statistically lower on the ACL-RSI than their male counterparts (58.5 ± 19.2 vs 66.2 ± 23.3; P = .019) (Table 4). Female patients were also found to score higher (worse) on the PROMIS-PSE than male patients (55.1 ± 8.2 vs 50.8 ± 7.7; P < .001). There were no significant sex differences noted between the IKDC (P = .406) or Pedi-FABS (P = .916) scores.
PRO Scores by Sex a

a Values are expressed as mean ± SD. Bold P values indicate a statistically significant difference between female and male patients (P < .05). ACL-RSI, Anterior Cruciate Ligament–Return to Sports after Injury; IKDC, International Knee Documentation Committee; Pedi-FABS, Pediatric Functional Activity Scale; PRO, patient-reported outcome; PROMIS-PSE, Patient-Reported Outcomes Measurement Information System–Psychological Stress Experience.
The ACL-RSI and IKDC had a moderately positive Spearman correlation of 0.57 (P < .001). The ACL-RSI and PROMIS-PSE had a weak negative Pearson correlation of –0.34 (P < .001). There was no significant difference (P = .496) in the mean timing of RTS clearance across the age groups: preadolescents, 8.8 ± 2.1 months; adolescents, 8.3 ± 2 months; and adults, 8.1 ± 2 months.
Discussion
We hypothesized that there would be an inverse relationship between psychological stress and psychological readiness and that PRO scores would not differ significantly among different ages, sex, or graft types among this young population at 6 months after ACLR. The results of this study demonstrate differences in psychological metrics on PRO measures that vary by patient age, sex, and graft type. This is important, as improved performance on the ACL-RSI and IKDC has been shown to correlate with postoperative RTS and clinical outcomes. 4 We found that preadolescents, male patients, and those who received an ITB autograft demonstrated higher ACL-RSI scores, potentially indicating higher psychological readiness to RTS in younger patients. These same groups also demonstrated significantly lower scores on the PROMIS-PSE, in which a higher score correlates with higher levels of stress and a higher perception of disruption. This is in line with our finding of a negative Pearson correlation between the ACL-RSI and PROMIS-PSE, indicating that a patient with a higher ACL-RSI score or higher feelings of being psychologically ready to RTS also has a lower PROMIS-PSE score or lower baseline levels of stress.
The PROMIS-PSE describes the child’s cognitive-perceptual disruption as it relates to an event and is not specific to an ACL injury but rather to a specific health attribute or stressor. 6 Although the PROMIS-PSE is a validated and efficient outcome instrument for patients with ACL tears and has a high correlation with currently utilized knee PROs with no floor or ceiling effects for patients who underwent ACLR, the PROMIS-PSE has not previously been examined in this manner. 13 Our study is the first to look at PROMIS-PSE as it related to outcomes following ACL reconstruction. Patients’ PROMIS-PSE scores could be useful in determining their psychological recovery after ACLR, as mild and moderate stress exposures can enhance productivity and motivation, while high-intensity stress can lead to anxiety, depression, hopelessness, and negative self-evaluation. 20 Further studies are needed to examine the utility of preoperative understanding of patients’ psychological stress as it relates to their postoperative recovery and readiness to RTS and activities.
In the present study, we demonstrated that female patients scored lower on the ACL-RSI than male patients and had higher PROMIS-PSE scores, indicating they had lower levels of perceived psychological readiness and higher levels of stress. Tan et al 37 found that female patients had worse subjective and functional outcomes with lower rates of RTS after ACLR and suggested that this difference may be influenced by psychological factors. In their univariate analysis, Webster et al 42 have shown that female patients also had lower psychological readiness as measured by the ACL-RSI and that they were less likely to RTS. Kostyun et al 18 echoed these findings and showed that female patients had lower ACL-RSI scores at the RTS clearance, as well as at 3 and 6 months postoperatively. Christino et al 9 suggested that kinesiophobia could lead to increased psychological distress that can affect outcomes and suggested that female patients may be a particularly vulnerable population. Similarly, Sims and Mulcahey 34 found that female patients exhibit greater anxiety concerning an injury’s impact on their lives and a loss of physical self-worth while men report a greater overall loss of self-worth with injury. The authors suggested that preoperative identification of sex-specific psychological factors could contribute to an improved RTS and quality of life. It is also possible that male and female patients may respond differently to the psychological readiness outcome questions and perhaps may differ in their willingness to honestly report fear, anxiety, and concerns associated with RTS. Sex-based differences in outcome reporting have previously been documented in adolescent sports concussion data, with female patients reporting more symptoms and at a higher frequency than male patients. 1 Of note, other authors have shown no significant differences in psychological readiness by sex; thus, it is unclear whether the sex differences observed in this study are truly generalizable. 2,19,22
The effect of age on outcomes after ACLR has become particularly concerning, as it has been shown that patients who are <20 years old can be 3 to 6 times more likely to sustain a second ACL injury. 41 Given this high rate of reinjury among younger patients, many studies have sought to identify risk factors predisposing patients to reinjury. Recent evidence has identified some biomechanical and neuromuscular factors—including hip internal rotation moment, knee valgus, and asymmetric sagittal plane mechanics—during a drop vertical jump, which can predict a second ACL injury if present at the time of RTS in young athletes aged 10 to 25 years. 31 As successful RTS after ACLR can be both physically and psychologically challenging, more attention has been placed on better understanding the role of a patient’s psychological readiness to RTS in the rehabilitation phase. The literature is currently split as to whether increased fear of reinjury may be a risk factor or a protective factor for secondary injury after ACLR. 30,32 One study 30 found that patients who demonstrated higher scores of self-reported fear had an increased risk of sustaining a second injury within 2 years after RTS. However, in a matched cohort study, Piussi et al 32 showed that higher psychological readiness and knee-related self-efficacy were associated with the patients suffering a repeat ACLinjury.
Further understanding of a patient’s psychological response is important, as this is considered potentially modifiable. For patients of any age undergoing ACLR, those who demonstrate unfavorable psychological characteristics (eg, low self-efficacy, anxiety, fear of reinjury, catastrophizing coping response, and pessimism) may be more at risk for poorer outcomes and delayed RTS than those with more favorable psychological characteristics. 9 Younger adolescent athletes have been shown to experience posttraumatic stress disorder and psychological distress after an injury, as well as increased levels of preoperative mood disturbances compared with adults. 28,39 Ardern et al 4 found that patients’ preoperative and 4-month postoperative ACL-RSI scores were associated with their chances of returning to their prior level of sport at 12 months postoperatively. They also found no interaction effects from the level of sport participation and psychological responses. This is in contrast to the study by Morrey et al 27 who found that competitive adolescent athletes were more likely to demonstrate greater mood disturbance compared with recreational athletes at the time of their RTS clearance. Therefore, one could conclude that early identification of younger patients who demonstrate either low ACL-RSI scores or those who demonstrate higher levels of baseline stress—as determined by an increased score on the PROMIS-PSE in our study—may benefit from potential intervention to improve their psychological characteristics earlier in the postoperative rehabilitation process.
The results of this study demonstrated that younger patients performed better across several PRO measures. The results of this study also demonstrated a correlation between the ACL-RSI, IKDC, and PROMIS-PSE in 10- to 14-year-old patients. This patient population is steadily increasing, as 1 study 44 found that between 2000 and 2015, the annual increased incidence of ACLR for patients aged 5 to 14 years was 7.7% for boys and 8.8% for girls. Early sports specialization, higher levels of competition, more intense training, and longer sporting seasons have been suggested to explain the rise in ACL tears in these younger athletes. 11 Many injury prevention programs have been designed to address potential neuromuscular risk factors, particularly in female athletes, as female athletes are 9 times more likely than male athletes to sustain an ACL tear. 36,37 Chicorelli et al 8 found that patients aged ≤14 years were able to return to the same preinjury skill level at a rate of 96%. A previous study has identified patients aged <20 years are at increased risk of sustaining a second ACL injury if they have lower psychological readiness at 12 months. 25 One study 26 found that patients in this age group who had a second injury had a smaller change between their preoperative and 12-month ACL-RSI scores than their non-reinjured counterparts. Our study suggests that injured preadolescent patients may demonstrate different psychological responses to ACLR compared with adolescent and adult patients. Further studies are necessary to ascertain whether age and psychological differences significantly influence the outcomes and risk of reinjury in preadolescent patients.
Limitations
There were several limitations despite the prospective nature of the study. The graft type was not randomized and rather was based on preferences of the orthopaedic surgeon and patient/family, with patients who were skeletally immature receiving ITB autografts, as transphyseal techniques were not an option. Therefore, it was difficult to ascertain whether the differences in PROs were truly due to graft type or if age was a confounding variable. Even with this study’s small sample size for some graft types and age groups, differences were large enough to reflect true differences, and they were statistically significant in some cases. Power is important if statistically significant differences are not found. In that case, the lack of a statistically significant difference may be due to small sample sizes, resulting in low power (<80%). However, further studies that include larger sample sizes and potentially collect information on bone age could provide additional information. Second, we did not have baseline preoperative scores, which may have been beneficial for comparison to further put our results in context. Also, as the questionnaire involved patients completing multiple PRO instruments consecutively, one must consider the possibility of test fatigue. Last, while our psychological readiness and PRO testing was generally done after the patients had completed their strength and functional testing, we did not directly control the timing of the administration of the questionnaires. The timing of this testing in the literature is not well reported and it is possible that the timing of the functional testing and the patients’ perception of their functional status based on that testing might change their responses to the subjective outcome measures. Similarly, since these outcomes were collected 6 months after ACLR and prior to their RTS, it is possible that the patients' perception of their ability to RTS would change as they approached their later RTS clearance. Finally, our prospective cohort ended enrollment in March 2020 because of the global coronavirus disease–2019 pandemic, as this was likely to be a significant confounding factor. Further studies evaluating the timing of psychological readiness testing as it relates to physical or functional testing is warranted.
Future studies are warranted to better understand whether increased psychological readiness is protective or, conversely, a risk factor for reinjury in the younger patient. A prospective study 9 that identifies at-risk patients of different ages early in the rehabilitation process to determine the need for a potential intervention is needed. Potential interventions could include an evaluation by a mental health professional or a sports psychologist, guided-imagery therapy, and positive self-talk, which have all been shown to decrease stress levels, which could ultimately lead to decreasing the rate of reinjury.
Conclusion
The study findings suggest that psychological profiles and subjective perceptions of stress and knee function 6 months after ACLR may vary across patients of different ages and between sexes. Preadolescent patients had higher performance scores on the ACL-RSI, IKDC, and PROMIS-PSE compared with their adolescent and adult counterparts. Age- and sex-related differences in PROs should be considered when counseling patients throughout both the physical and the emotional rehabilitation process after an ACLR. Future studies are necessary to better understand the effect of age, sex, graft type, sports participation, and functional performance on psychological recovery and rehabilitation after an ACLR.
Footnotes
Final revision submitted January 5, 2023; accepted January 25, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.D.M. has received education payments from Kairos and royalties from Elsevier. J.L.T. has received education payments from Kairos, Gemini Mountain, and Smith & Nephew. D.E.K. has received education payments from Kairos and One Day and consulting fees from DePuy and Miach Orthopaedics. M.S.K. has received education payments from Kairos; consulting fees from OrthoPediatrics and Ossur; and royalties from Elsevier, OrthoPediatrics, Ossur, and Wolters Kluwer. Y.-M.Y. has received consulting fees from Smith & Nephew. M.A.C. has received hospitality payments from OrthoPediatrics and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children’s Hospital (ref No. P00013151).