
Abstract
Background:
Multiple techniques exist to repair acute tears of the patellar tendon. Surgical repair is required to reestablish full function of the extensor mechanism of the knee, and optimal results typically occur when the tear is repaired acutely.
Purpose:
To systematically review the literature to evaluate treatment outcomes and complication rates after acute surgical repair of patellar tendon ruptures using suture anchor repair, transosseous repair, and end-to-end repair.
Study Design:
Scoping review; Level of evidence, 4.
Methods:
A systematic review was performed to analyze outcomes after patellar tendon repair in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. Potential studies were identified through searches of the Cochrane Central Register of Controlled Trials, PubMed, and Embase. Screening was completed independently by 2 authors, who sought to identify studies published from January 1980 to December 2024 that described the management of acute patellar tendon ruptures. Articles were excluded if they described chronic tears or included cases of patellar tendon ruptures in patients who previously underwent total knee arthroplasty. Clinical outcome data were recorded, including treatment outcomes and complications.
Results:
Twenty studies analyzing 1161 patients met the inclusion criteria. The most reported repair techniques were suture anchor repair, transosseous repair, and end-to-end repair. Six studies analyzed transosseous repair and found positive postoperative functional outcomes, including mean postoperative Lysholm scores ranging from 84 to 98.08 (any, n = 3). Two studies reported using suture anchors, and each stated a postoperative flexion range of motion >130°, with no complications. Five studies analyzed end-to-end acute patellar tendon rupture repair and reported mean flexion >130° (n = 3), with the most reported complication being wound infections. Eight studies compared multiple techniques for acute patellar tendon rupture repair, and 6 studies showed statistically significant improvements in functional outcome scores when comparing pre- and postoperative scoring within cohorts. Additionally, 5 studies in this group reported complications, with the most common being rerupture, reoperation, skin infections, and deep vein thrombosis.
Conclusion:
Surgical repair of acute patellar tendon rupture with suture anchor repair, transosseous repair, and end-to-end repair all achieved high healing rates. The majority of surgical options demonstrated good functional outcomes with a low risk of complications, the most common of which related to wound complications and infection.
Acute patellar tendon ruptures occur with an incidence between 0.48 and 1.09 per 100,000 person-years. These are devastating injuries that severely limit mobility and greatly affect quality of life. 4 Classically, they affect middle-aged males, younger athletes (age, 20-40 years), and patients with preexisting metabolic medical comorbidities, such as diabetes, kidney disease, or inflammatory autoimmune conditions. 29
Surgical repair is required to reestablish full function of the extensor mechanism of the knee, and optimal results typically occur when the tear is repaired acutely. 8 Repair techniques are variable but focus on returning the torn end of the tendon to its anatomic position. Midsubstance tears may be repaired via end-to-end techniques utilizing Krackow-type tendon sutures, while those tears near the proximal or distal poles of the tendon often require bony fixation through either the inferior pole of the patella or tibial tuberosity, typically accomplished with transosseous tunnels or suture anchors. 12 While studies exist comparing these techniques, the data are mixed, and no clearly superior technique has been defined owing to the paucity of high-quality comparative studies.11,26
Each technique has benefits and pitfalls. However, the impact that these considerations may have on outcomes is unclear. Suture anchor repair may utilize a smaller incision with strong initial fixation; yet, it carries risks, such as anchor pullout, bone resorption, and inflammatory responses. Transosseous repair provides better tendon fixation, promoting tendon-to-bone healing without foreign implants, although it typically requires a larger incision and violation of the quadriceps for knot tying. In end-to-end repair, torn tendon ends are sutured directly together, preserving native tissue and restoring natural biomechanics, but precise tensioning is crucial to avoid laxity or excessive tightness, and adhesion formation is a notable complication.
Beyond just the repair technique, surgeons may elect to use either biologic or cerclage augmentation to strengthen the repair and maintain proper tension of the tendon. 12 This typically involves passing the augmentation material around the proximal border of the patella and through a tunnel drilled into the tibia. The most common augmentation materials are cerclage wire and nonabsorbable suture. 12
Given the multitude of repair techniques and augmentation materials that may be used in patellar tendon repairs, the purpose of this study was to systematically review and qualitatively analyze the available data on outcomes after acute repair of patellar tendon rupture. Areas of attention were given to 3 key considerations: location of tear, type of repair, and use of augmentation.
Methods
Article Identification
A systematic review of the literature evaluating outcomes and complications after surgical repair of patellar tendon rupture was performed through 2024 using the Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials (1980-2024), PubMed (1980-2024), MEDLINE (1980-2024), and Embase (1980-2024). The following search terms were included and combined with the Boolean operators AND/OR: “patellar tendon,”“patella tendon,”“patellofemoral ligament,”“rupture,”“injury,”“repair,”“operative,”“surgery.”
The search results were compiled, and duplicates were removed. The inclusion criteria were as follows: studies that examined outcomes and/or complications after acute surgical repair of patellar tendon ruptures (acute repair was defined as surgery <4 weeks from the injury), English language, >5 patients, minimum 2-year follow up, and human subjects. Exclusion criteria included review articles, cadaveric studies, failure to stratify outcomes by chronicity of tear, and patellar tendon ruptures in patients who previously underwent total knee arthroplasty. Two authors (H.S.F., C.M.) screened the articles first by title, then by abstract, and then by full text. If a discrepancy arose between reviewers, the principal investigator decided upon article inclusion or exclusion.
Data Collection
This systematic review was completed following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. 24 The same 2 authors (G.D. and H.S.F.) reviewed each article and extracted data into a predetermined form. Variables for analysis included patient demographics, injury characteristics such as location of rupture and chronicity of tear, length of follow-up, surgical technique, complications, revisions, and patient-reported clinical outcomes. Means, standard deviations, and 95% confidence intervals were collected. The level of evidence for each study was assigned by the classification proposed by Wright et al. 34 Additionally, study quality and risk of bias were assessed by the same 2 reviewers using MINORS (Methodological Index for Non-randomized Studies), a validated tool designed to quantify the methodological quality of nonrandomized studies. 32 A meta-analysis was unable to be performed owing to significant heterogeneity in reporting, outcome measurements, and repair type. All articles were thus reviewed qualitatively.
Results
Study Selection
The search identified a total of 1202 records that were eligible for review after removal of duplicates. Of the 1202 records, 1161 studies were removed per the exclusion criteria, and the remaining 41 studies were considered for full-text analysis (Figure 1). At the completion of the full-text analysis, a further 21 studies were removed for a lack of relevance or inconsistent reporting of patient data. Finally, 20 articles remained and were eligible for qualitative analysis.

Flow chart of the article inclusion and exclusion conducted under Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines.
Overall Study Characteristics
Overall, there were 1 level 2, 5 level 3, and 14 level 4 studies that analyzed a total of 1161 patients. Of these, there were 1020 males and 72 females (Bushnell et al, 5 Kasten et al, 15 McGowan et al, 22 Shelbourne et al, 30 and West et al 33 did not provide sex/gender demographic information). The mean age of patients ranged from 30 to 54.6 years.6,14 Mean follow-up ranged from 22.4 to 123 months.19,25 Surgical repair technique and timeline were heterogeneous across studies. Overall, 18 studies evaluated acute treatment of patellar tendon ruptures (n = 1132), and 2 studies included acute and chronic treatment. For these latter 2 studies, only the acute cases were included in this review (n = 29).
Additionally, the mean MINORS grade was 8.7 ± 2.25. Characteristics of the studies are displayed in Table 1.
Characteristics of Included Studies a

Dashes indicate data not reported. BTB, bone-tendon-bone; LOE, level of evidence; MINORS, Methodological Index for Non-randomized Studies; PDS, polydioxanone.
Surgical technique or augmentation used in specific study.
Some patients received bilateral repair.
Acute Tears: Transosseous
Six articles analyzed exclusively transosseous repair of acute patellar tendon ruptures (Table 2). Each of the 6 articles used a form of augmentation, including cerclage, relaxing suture, or hamstring tendon. None of the studies indicated any instance of rerupture. Across the 6 studies, a range of outcome measures was used with few commonalities. Although this restricts a comprehensive assessment, all studies reported positive outcomes, a low risk of complications, and generally favorable conclusions.
Surgical Treatment and Outcomes of Acute Patellar Tendon Ruptures Using the Transosseous Repair Technique a
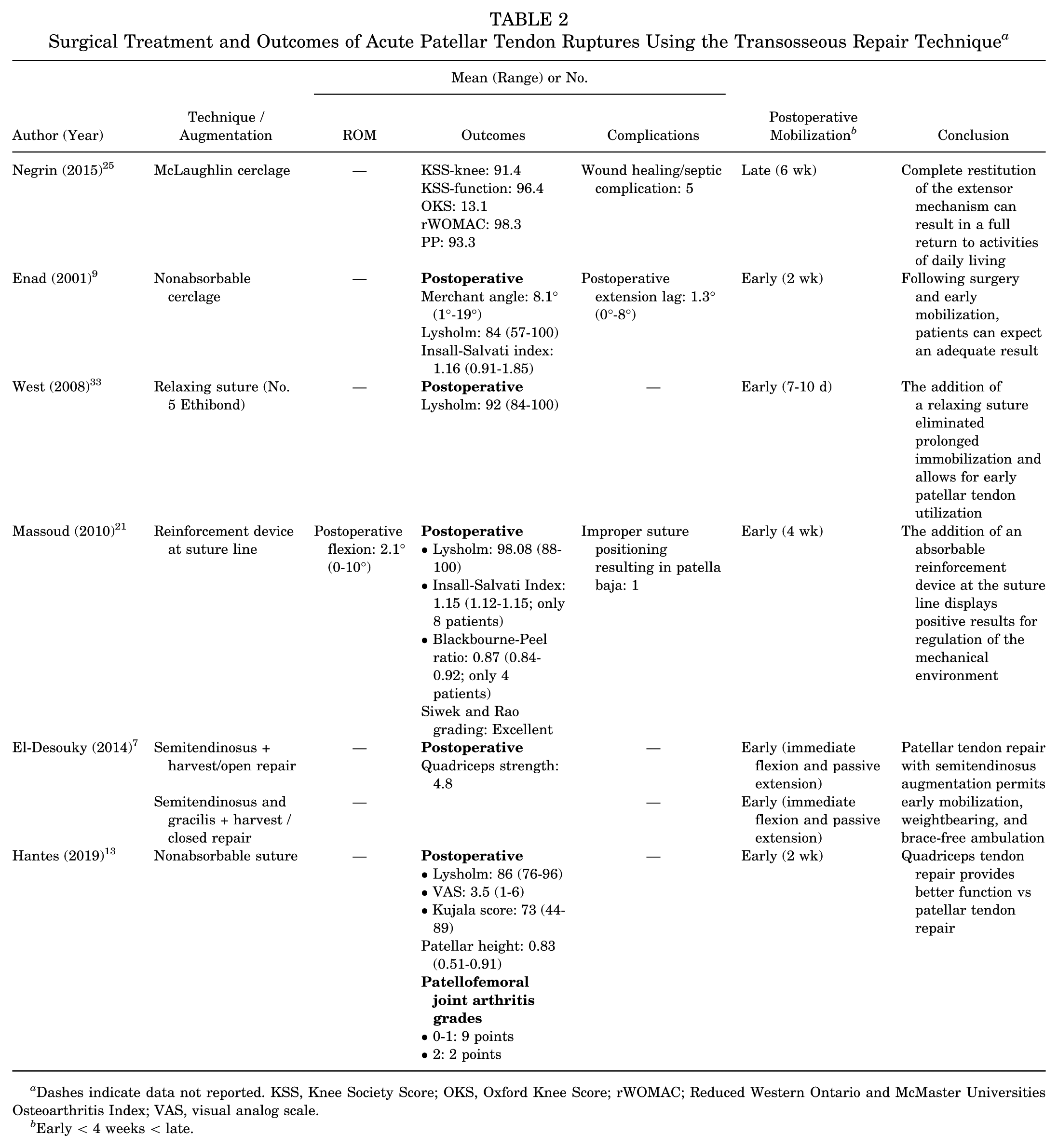
Dashes indicate data not reported. KSS, Knee Society Score; OKS, Oxford Knee Score; rWOMAC; Reduced Western Ontario and McMaster Universities Osteoarthritis Index; VAS, visual analog scale.
Early < 4 weeks < late.
Acute Tears: Suture Anchor Repair
Two studies analyzed suture anchor repair for acute patellar tendon ruptures (Table 3). Neither article used any form of augmentation. Neither study indicated any instance of rerupture. Both studies reported positive outcomes, a low risk of complications, and generally favorable conclusions.
Surgical Treatment and Outcomes of Acute Patellar Tendon Ruptures Using the Suture Anchor Repair Technique a

Dashes indicate data not reported. ROM, range of motion.
Early < 4 weeks < late.
Acute Tears: End-to-End Repair
Five studies analyzed the end-to-end technique for acute patellar tendon repair (Table 4). Each article used a form of augmentation, including wire cerclage, polydioxanone cord, Dall-Miles cable, and Mersilene tape. None of the studies indicated any instance of rerupture. Across the 5 studies, all reported positive outcomes, a low risk of complications, and generally favorable conclusions.
Surgical Treatment and Outcomes of Acute Patellar Tendon Ruptures Using the End-to-End Repair Technique a

Dashes indicate data not reported. DVT, deep vein thrombosis; HSS, Hospital for Special Surgery; PDS, polydioxanone; ROM, range of motion.
Early < 4 weeks < late.
Mixed Techniques
The remaining 7 studies used multiple repair techniques and did not stratify results by procedure type (Table 5). Two studies included patients from 3 technique groups, and 5 studies included patients from 2 technique groups. All but 1 study combined patient data, with O’Dowd et al 26 choosing to separate only complications. All but 1 article used a form of augmentation technique, such as graft, suture, metal wire, synthetic ligament, and cerclage. Three studies cited instances of rerupture among 10 (2.97%), 1 (2.63%), and 24 (7.5%) patients. Across the 7 studies, all reported positive outcomes, a low risk of complications, and generally favorable conclusions.
Surgical Treatment and Outcomes of Acute Patellar Tendon Ruptures Using >1 Technique a

Dashes indicate data not reported. ADL, activities of daily living; DVT, deep vein thrombosis; EQ-VAS, EuroQol visual analog scale; KSS, Knee Society Score; ROM, range of motion; VAS, visual analog scale; VISA, Victorian Institute of Sport Assessment.
Early < 4 weeks < late.
Surgical technique or augmentation used in that specific study.
Postoperative Mobilization
The 20 studies included different postoperative protocols for patients: 9 implemented late mobilization, 9 early mobilization, and 2 did not report any postoperative mobilization protocol. The use of early mobilization (<4 weeks) was seen more in the transosseous and end-to-end forms of repair. The studies that utilized early mobilization showed positive functional results and no change in rerupture rate as compared with the late mobilization protocols.
Discussion
To our knowledge, this the largest and most comprehensive systematic review of acute patellar tendon ruptures, with 20 articles. Various repairs were represented, such as anchor fixation, transosseous, and end-to-end techniques, all with or without augmentation, which yielded Lysholm scores >90 and return to function in most patients. After inclusion of all surgical techniques for acute patellar tendon repair, the overall rerupture rate after primary patellar repair or reconstruction was low. Suture configuration and amount/style of suture used in transosseous and suture anchor repair were heterogenous and variably reported. Only 1 study noted cerclage wire breakage as a complication. 3 No other studies indicated an instance of similar failure. These general trends help to support multiple techniques with good outcomes, revealing that there is no gold standard technique for repair of acute patellar tendon ruptures. The ultimate decision for repair can be a combination of surgeon experience and joint decision making with the patient.
Most patellar tendon ruptures occur at the junction of the proximal tendon and the inferior pole of the patella. For these avulsion tears, transosseous tunnel fixation was long considered the gold standard; however, several recent biomechanical studies found suture anchor repair to have comparable if not improved biomechanical profiles, including significantly less gap formation and higher ultimate failure loads.4,10,18,31 O’Dowd et al 26 retrospectively analyzed 374 knees repaired with transosseous tunnel fixation (n = 321) or suture anchor (n = 53) and found a significantly lower rerupture rate in the suture anchor cohort (0% vs 8%; P = .034). The remainder of the studies that examined transosseous repair utilized some form of augmentation in addition to the tunnel fixation, with no reruptures in any study and postoperative mean Lysholm scores ranging from 84 to 98. Biomechanically, it has been shown that reinforcement with hamstring tendon, suture, and metal (McLaughlin) cerclage results in better suture and reinsertion traction resistance as compared with simple transosseous fixation.23,27 Given the biomechanical evidence and the results of the studies within this review, we recommend consideration of augmentation of any transosseous repair with 1 of the aforementioned modalities.
While immobilization in terminal knee extension for 6 to 8 weeks protects the repair and has historically been the mainstay for postoperative management, this can result in knee stiffness, pain, and a lengthier time to return to sport. Earlier mobilization has therefore been a topic of interest to those surgeons who wish to return their patients to activity and decrease risk of these complications. Enad and Loomis 8 divided 10 patients into 2 cohorts: a delayed mobilization group confined to casting in extension with isometric lower extremity exercises for 6 weeks before beginning active flexion and extension and an early mobilization group permitted to flex and extend the knee in an adjustable brace within 2 weeks of surgery. They found similar results between the cohorts in terms of clinical and functional results, and no patient exhibited an active flexion or extension deficit ≥5° as compared with the opposite knee. West et al 33 published the results of their early motion protocol in a cohort of 30 patellar tendon ruptures and concluded that repairs protected by a relaxing suture were strong enough to safely permit early motion, weightbearing, and brace-free ambulation while producing good and excellent results. In the current review, Shelbourne et al 30 and Bhargava et al 3 augmented their repairs with a Dall-Miles cable and wire cerclage, respectively, and reported excellent results after implementing an early mobilization rehabilitation protocol. Further study is needed directly comparing early and late mobilization among the varying repair techniques to determine if an optimal technique exists. For end-to-end suture repair of acute patellar tendon ruptures, each study utilized a form of augmentation with either cerclage or suture. It was noted that the addition of augmentation allowed for earlier mobilization and range of motion postoperatively.3,19,30 It also provided stability to the tension that was experienced at the repair site. 30
Strengths of this study include a large sample of operations (n = 1250) being analyzed with a variety of repair techniques. The collection of knees and techniques evaluated in this study allows for a broad inquiry of data on a specific injury that can be implemented by surgeons utilizing different forms of repair. Limitations of this study include the retrospective nature of the articles involved. There were few studies with a high level of evidence available for analysis. This limitation has the potential to introduce inherent methodological bias if the studies are inappropriately combined. The attempted aggregation of patients across studies would compound limitations of each study and ultimately present largely heterogenous studies as representative of a population, when in reality they are not. This could lead to skewed results and inaccurate conclusions. As such, the decision was made to omit meta-analysis to preserve authenticity of the presentation of data. While this lessens the conclusions that can be made, the consensus of the study remains largely encouraging.
Conclusion
Surgical repair of acute patellar tendon rupture with suture anchor, transosseous, and end-to-end repair achieved high healing rates. En masse, all the surgical options demonstrated good functional outcomes with a low risk of complications, the most common of which related to wound complications and infection.
Footnotes
Final revision submitted May 1, 2025; accepted June 26, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.B.F. has received consulting fees from Ferring Pharmaceuticals, Innocoll Inc, and Liberty Surgical and a grant from Vericel Corporation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.