
Abstract
Background:
Patellar tendon ruptures are infrequent but disabling injuries. Surgical treatment is the gold standard to obtain good outcomes, and numerous techniques have been described. Biomechanical studies report better results when augmented techniques are used. However, there is a lack of consensus regarding the best standard technique.
Purpose/Hypothesis:
The purpose of this study was to assess a cohort of patients with acute patellar tendon rupture that was surgically treated and to compare the clinical outcomes of 2 groups: isolated repair and biological augmentation techniques with autograft or allograft. It was hypothesized that the biological augmentation group would have better clinical outcomes than the isolated repair group.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
All patients with acute patellar tendon rupture surgically treated in our center between 2016 and 2022 were retrospectively reviewed. Patient and rupture characteristics, surgical technique, clinical outcomes, and complications were recorded. The primary outcome was rerupture rate, and secondary outcomes were infection rate, stiffness >15° of knee flexion deficit, and extensor mechanism lag >5°.
Results:
The study included 34 patients with 36 operated knees (2 patients with bilateral rupture). The mean age was 44.9 years. Isolated repair was performed in 20 knees (55.6%), and 16 knees underwent repair and biological augmentation with autograft or allograft. Both groups were comparable in terms of their demographic characteristics. A statistically significant association was found between the type of surgery and tendon rerupture. Of the patients in the isolated repair group, 5 of 20 (25%) experienced a failure, whereas in the biological augmentation group, no reruptures were recorded (P = .031). However, no statistically significant associations were found between the type of surgery and other complications, such as the development of stiffness (P = .54), residual extension lag >5° (P = .87), or the development of infection (P = .25).
Conclusion:
In this cohort of patients, biological augmentation reduced the rate of surgical failure for acute patellar tendon rupture without being associated with a higher risk of complications such as stiffness, residual extension lag, or the development of infection.
Patellar tendon injuries are infrequent yet can be debilitating due to the loss of active knee extension. 21 The incidence of this injury has been estimated to be 0.68 out of 100,000 per year 12 and it has a marked male predominance, with men calculated to be 6 times more likely than women to experience patellar tendon injury. 50 Patellar tendon ruptures (PTRs) are typically sustained after forceful and sudden quadriceps contraction with the knee in a flexed position,26,29,46,50 commonly in a previously damaged tendon due to repetitive microtrauma, systemic comorbidity, or corticosteroid local injections.9,29,46,50 Inferior patellar pole ruptures are the most common type of PTR, followed by midsubstance and distal patellar tendon insertion at the tibial tuberosity.22,26,29
Surgical treatment has been advocated as the gold standard treatment for this kind of injury to regain knee extension and good clinical and functional outcomes. 21 In 1999, Marder and Timmerman 37 described excellent results using the classic PTR repair, which consists of 3 parallel vertical tunnels on the patella, reinforced by Krackow sutures on the patellar tendon. One problem this technique has faced is rerupture, which has been reported in 2% to 50% of cases.21,57 Many authors have proposed novel augmentation techniques to increase the load to failure and diminish the gap formation, aiming to optimize the clinical results and enabling more aggressive rehabilitation protocols.5,9,22,57 These augmentation techniques can be divided into nonbiological (cerclage wires, nonabsorbable sutures, suture tapes, or synthetic ligaments, to name a few) and biological (autografts and allografts16,52,57). Biomechanical studies have reported less gap formation with the use of an augmentation technique compared with no augmentation, and some have reported significant results regarding load to failure.5,22,29,45,48 Some recommendations have been proposed, like the ones provided by Gilmore et al 21 in their systematic review of the literature, suggesting that acute tendon repair and augmentation surgery achieve better postoperative outcomes and recommending the use of autografts in poor quality and scarred tendons. However, to date, there is a lack of consensus regarding which technique to use and when to use it14,19,29 and a paucity of clinical evidence comparing the classic transosseous PTR repair with augmentation techniques.
The objective of the present study was to present a series of acute PTR repairs in 1 level I trauma center and compare the clinical outcomes of 2 groups: classic repair versus biological augmentation with autografts or allografts. We hypothesized that the biological augmentation group would have better clinical outcomes than the isolated repair group.
Methods
A nonconcurrent cohort study was conducted on patients with acute PTR, aged ≥18 years, who were treated and underwent surgery in a level I trauma center. The patients admitted to our center use workers’ compensation insurance, and thus no patients are lost to follow-up due to causes other than death. Patients who have complications are immediately referred to our institution for inpatient or outpatient care. We retrospectively reviewed medical records of patients who underwent surgery between 2016 and 2022. The follow-up period was defined as the period between index surgery and the last outpatient clinic visit with a knee surgery fellowship–trained orthopaedic surgeon in our institution in the period defined above. The study excluded patients with total knee replacement–associated injuries, knee fractures requiring osteosynthesis, >42 days between injury and surgery, neurological injuries preventing active mobilization of the operated limb, nonbiological augmented repairs, and follow-up less than the defined minimum period of 9 months. We defined 9 months as a safe period to identify a rerupture and other complications and as a sufficient time before outpatient visits are more spaced between appointments (yearly or biyearly). All the surgeries were performed by 5 surgeons of our unit with subspecialty training (fellowship) in knee surgery (including R.O., J.I.L., N.F., and P.I.). The number of surgeries per specialist varied from 11 procedures by the 1 surgeon who performed the most surgeries to 5 interventions by the 2 surgeons who performed the least surgeries. All patients provided informed consent for the use of their data for research, and the study was approved by the ethical board in advance (internal code CEC 01/2024).
The definition of acute PTR varies in the literature; however, several studies have temporally defined it as cases in which surgical resolution is performed within 6 weeks from the date of rupture with adequate tissue remnant.1,33,42,50 This is the definition we used for the current research.
Patients were assigned to one of two treatment groups based on the surgeon's preference: (1) isolated repair, either end-to-end or reinsertion into the patella using transosseous tunnels or anchors and; (2) repair with biological augmentation (autograft or allograft) in cases where poor tendon quality with highly irregular edges and ends was observed, using any of the techniques described in the first group.
End-to-end repair was performed using Krackow sutures with high-strength Fiberwire No. 2 (Arthrex) or Ultrabraid No. 2 (Smith+Nephew). In cases of reinsertion, the procedure was conducted with high-strength Fiberwire No. 2 or Ultrabraid No. 2 sutures and Krackow-type stitches at the tendon end and 3 transosseous tunnels or with two 5.0-mm titanium Corkscrew anchors (Arthrex). The decision on the type of repair was made by each surgeon based on the location of the rupture and macroscopic tendon quality.
The augmentation was performed using an autograft (either semitendinosus or semitendinosus and/or gracilis [STG]) or allograft (posterior tibial tendon [PTT]) by passing a figure-of-8 loop through the patellar transverse tunnel and the anterior tibial tuberosity using the modified Ecker 16 technique described by Sundararajan. 52 In any of the augmentation alternatives, the loop was knotted on itself once the tendon reinsertion was completed. Patients were weightbearing with an articulated knee brace in full extension until suture removal, and then a progressive passive range of motion was initiated until full passive range was achieved at 6 weeks, followed by brace discontinuation. All patients received supervised physical therapy from a physical therapist 2 to 5 times per week according to the institutional protocol for a minimum of 20 sessions. Physical therapy involved immobilization with a brace, isometric exercises, and partial weightbearing on the limb with 2 walking aids for 3 weeks. Subsequently, a gradual increase in flexion of the operated knee was allowed, aiming to achieve 90° of flexion by 6 weeks after surgery with limb loading based on patient tolerance. After 6 weeks, full range of motion and unrestricted weightbearing were allowed.
Repair failure was defined as postoperative loss of the patient's ability to perform active knee extension associated with a radiographic image showing an increase in patellar height compared with a previous postoperative radiograph or a magnetic resonance imaging scan consistent with rerupture of the repaired tendon. Extension lag was defined as the loss of range of motion, measured in degrees, compared with the nonoperated side (or the preoperative range of motion of the unaffected extremity). Approval was obtained from the scientific ethics committee for this study.
We collected data on demographic characteristics of the patients, their injury (laterality, lesion location, time from injury to surgery), the surgery (surgical technique used, type of graft), and postoperative follow-up results (rerupture and time from index surgery, need for new surgeries and type of surgery, presence and quantification of extension lag in degrees, follow-up time).
All statistical analyses were performed using Stata 17 (StataCorp). No sample size was calculated given the nature of this study. Assessment for normality was performed with the Shapiro-Wilk test. For comparisons between continuous variables, unpaired t test was performed. We performed a chi-square test for comparison of categorical variables and a Pearson correlation test for correlation between continuous and categorical variables. We calculated odds ratios with their respective confidence intervals for measure of association. A significance level of P < .05 was set to designate statistical significance.
Results
A total of 36 patients with 38 PTRs who underwent surgery met inclusion criteria (2 patients with bilateral PTRs). After exclusion criteria were applied, 34 patients (36 PTRs) were enrolled in this study, of whom 32 were male (94.12%) (2/36 patients were excluded because they had repairs with both biological and nonbiological augmentation). The mean ± SD age was 44.9 ± 12.76 years, and the mean body mass index (BMI) was 28.2 ± 3.6 kg/m2, with 10 patients (29.4%) classified as obese (BMI ≥ 30 kg/m2). Fifteen patients (44.12%) had at least 1 comorbidity, with arterial hypertension being the most frequent in 8 patients (23.53%). In 21 knees (58.33%), the injury was on the right side, and in 15 (41.67%) it was on the left side. Mean follow-up was 25.4 ± 18.8 months (Table 1).
Patient Characteristics a

Data are expressed as mean ± SD or n (%), unless otherwise noted. Age and sex refer to the patients; the rest are data corresponding to the operated knees. Medical history refers to the patients’ morbid conditions reported at the time of each patient's admission for surgery. P values are provided for comparison between groups. BMI, body mass index.
Refers to operated knees.
The most frequently described mechanism of rupture was a ground-level fall in 10 cases, followed by motorcycle accidents and sports-related (soccer) incidents, each with 6 ruptures.
An isolated repair was performed in 20 knees, and in 16 knees, a repair with augmentation was performed. Mean follow-up was 29.9 ± 22.8 months for the isolated repair group and 20 ± 10.28 months for the repair + augmentation group. Both groups (isolated repair and repair with some form of biological augmentation) were comparable in terms of their demographic characteristics, with no statistically significant differences in any of the variables.
In the isolated repair group, 20 knees were included, consisting of 3 end-to-end tendon repairs, 15 reinsertions using transosseous suture, and 2 reinsertions using bone anchors. Two end-to-end repairs failed (both diagnosed by magnetic resonance imaging), whereas in the transosseous reinsertion subgroup, rerupture was observed in 3 reinsertions (the 3 cases were clinically diagnosed and confirmed by radiographs). Upon reviewing the causes of rerupture, we found that rerupture occurred secondary to a fall at ground level in 2 cases and direct knee contusion in a domestic accident in 1 case. In the other 2 cases, the diagnosis was made clinically during a medical follow-up, without the patient reporting a traumatic cause. Mean time from surgery to failure was 10.8 weeks (Table 2).
Isolated Repair Group a

Data are expressed as mean ± SD or n/N (%), unless otherwise noted.
In the repair with augmentation group, 16 knees were included, consisting of 7 end-to-end tendon repairs, 5 transosseous sutures reinsertions, and 4 reinsertions using bone anchors. Augmentation was performed with autologous semitendinosus tendon in 2 knees, semitendinosus and/or gracilis autografts were used in 4 knees, and posterior tibialis allograft was used in 10 knees. No failures were observed in the augmentation group (Table 3).
Repair + Biological Augmentation Group a

Data are expressed as mean ± SD or n/N (%), unless otherwise noted.
When evaluating surgery type (with or without augmentation), we found a statistically significant association with rerupture (P = .031). This association led to an odds ratio of 11.7 (95% CI, 0.59-229.8; P = .1). Although this association was significant, its odds ratio did not reach statistical significance, probably because of the design of this study. No infections occurred in the isolated repair group, while there was one episode of infection in the augmentation group. Additionally, there were four cases of stiffness in the isolated repair group compared to two in the augmentation group. No association was observed between surgery type and the development of infection (P = .25), stiffness >15° of flexion deficit (P = .54), or extension lag >5° (P = .87) (Table 4).
Results and complications of each group according to the type of repair used a
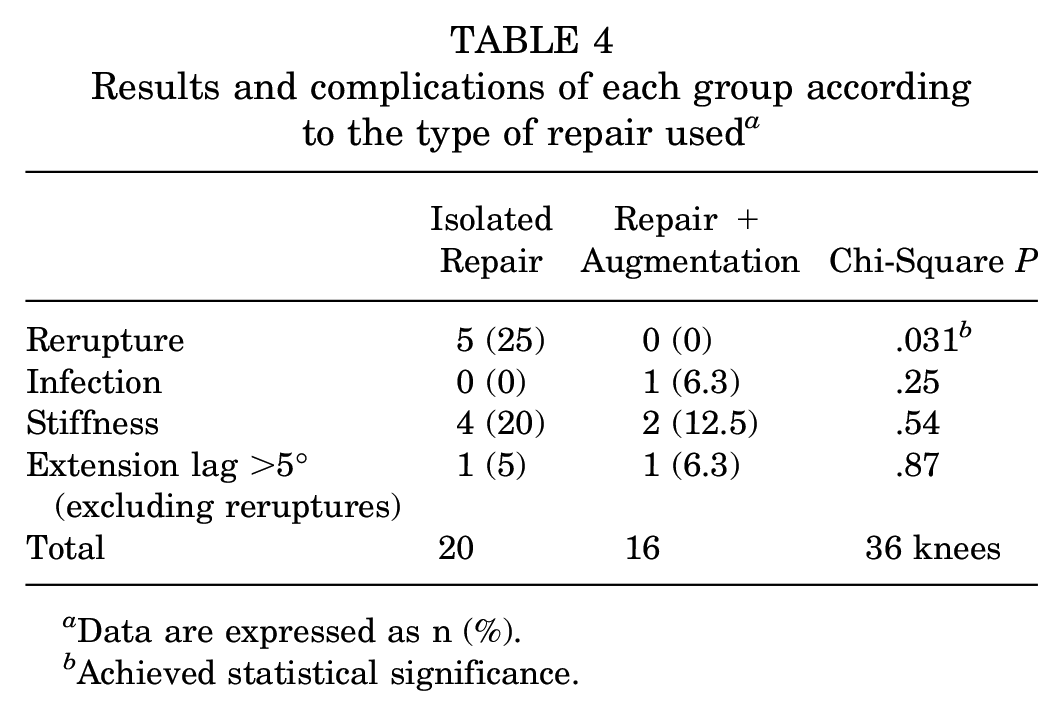
Data are expressed as n (%).
Achieved statistical significance.
Discussion
This retrospective nonconcurrent cohort study showed that acute PTR repair associated with biological augmentation using autografts or allografts was significantly associated with a reduced risk of tendon rerupture. We did not find significant differences in complications such as infection rate, residual extension lag >5°, or stiffness >15° of flexion deficit between the 2 compared groups.
Compared with previous studies,20,42 we observed a slightly higher mean age (44.9 years) in our patient cohort but with a similar male predominance (94.1%) as observed previously.12,42,46 We also found an average overweight status with a mean BMI of 28.2 kg/m2, in line with previous reports,20,23 with 30.3% of patients falling within the obesity range. Additionally, a high frequency of smokers (32.4%, 33.3%) was noted. Because these variables along with comorbidities were homogeneously distributed between groups, we did not consider them as confounders. The most frequently described mechanism in our series was fall at ground level followed by motorcycle accident, which is in line with the literature reporting that low-energy indirect trauma is the most frequent mechanism due to an eccentric contraction of the quadriceps muscle. 53 In terms of the rerupture mechanism in the group of patients with an isolated repair, we observed that it involved low-energy traumatic mechanisms.
Surgical repair of the PTR, with or without augmentation, is considered the gold standard of treatment.24,36,53 Numerous repair techniques, including different configurations of transosseous tunnels, reattachment with anchors, end-to-end repair, or various combinations of these techniques, have been described, ¶ many of them in small series or case reports.
In 1999, Marder and Timmerman 37 reported their case series of 15 patients (all athletes) surgically treated with PTR repair using transosseous tunnels and an early rehabilitation protocol. Those authors described excellent clinical and functional outcomes, with only 5° of flexion deficit, no extension lag, and 12 patients returning to their previous level of activity. In contrast, suture anchor repair has demonstrated similar or superior biomechanical properties compared with the traditional technique of transosseous repair.18,50 Bushnell et al 7 reported their experience of 13 years using anchor repair. After a mean follow-up of 29 months, those authors presented excellent results with 11 of 14 patients returning to their previous level of activities; the other 3 patients experienced rerupture (all associated with noncooperating patients).
Recent literature has compared the outcomes of these different techniques. In a large retrospective study of 374 PTR repairs (321 transosseous repairs and 53 anchor repairs), O’Dowd et al 42 stated that anchor repair of the patellar tendon led to significantly fewer reruptures in comparison with the traditional transosseous technique (0% vs 7.5%, respectively; P = .034). The infection rate was 1.6% for transosseous repair and 7.5% for anchor repair (P = .160).
Regarding augmentation techniques, numerous methods have also been reported, including the use of autografts or allografts # and synthetics. ** In 1979, Ecker et al 16 reported their augmentation technique using the gracilis and semitendinosus tendons and an encircling wire as supplementation, with all their patients returning to their preinjury level. Hsu et al 25 reported good and excellent outcomes in 85.6% of their patients, using primary repair with cerclage encircling augmentation. Others like Carlson Strother et al 9 have proposed allograft augmentation in certain situations like chronic injuries or poor tissue quality, reporting no extension lag and significantly improved International Knee Documentation Committee and Tegner activity scores.
In 2013, Sundararajan et al 52 described a novel augmentation technique using detached figure-of-8 STG autograft, reporting good International Knee Documentation Committee and excellent Lysholm and Kujala functional outcomes in all their 7 patients. In our center, we have opted for this technique (Figure 1), which is a modification of the technique originally published by Ecker et al. 16 In our cases, we have chosen to use any of these autografts or allografts (PTT), depending on tendon quality and allograft availability.

Augmentation performed using an autograft (semitendinosus) by passing a figure-of-8 loop through the patellar transverse tunnel and the anterior tibial tuberosity using the technique described by Sundararajan et al. 52
Our finding of a higher failure rate in the isolated repair group may have been influenced by the predominance of the technique using transosseous tunnels rather than anchors. As described above, in their clinical work, O’Dowd et al 42 observed a lower rerupture rate of PTR with use of anchors compared with transosseous tunnels (0% vs 7.5%, respectively). In our study, we did not observe failures in the patients who underwent isolated repair with anchors; however, because there were only 2 such patients, the sample was not sufficient to obtain any conclusive results. Biomechanical cadaveric studies comparing the use of anchors versus transosseous tunnels, such as those by Bushnell et al 6 and Ettinger et al, 18 noted significantly less gap formation in the anchor groups when subjected to cyclic loading. However, in these studies, the use of biological augmentation in tunnel repair was not included. In our case, none of the 6 cases of repair with tunnels augmented by graft presented rerupture.
Other studies have shown a decreased rate of rerupture in patients with synthetics or biologic augmentation. Kasten et al 32 described 0 failures in 29 PTRs that entailed augmentation with either a wire cerclage or 2-mm polydioxane cord. A biomechanical study by Mihalko et al 39 showed a decreased gap formation with hamstring tendon autograft augmentation at the repair site under a simulated dynamic knee motion. Roudet et al 46 reported very good long-term clinical and radiological outcomes in acute augmentations with hamstring, metal wire, or synthetic ligament. This aligns with our findings of 0 reruptures in 8 patients with end-to-end repair who underwent biological augmentation.
In terms of infections, no significant differences were observed between the groups. No events of cutaneous necrosis or operative wound dehiscence were observed in either of the 2 groups. No infections occurred in the isolated repair group, and there was 1 infection episode in the augmentation group, in a heavy smoker in whom STG autograft was used, which was observed at 35 days after surgery. This was managed with surgical debridement and subsequent superficial negative wound pressure for 7 days, with no compromise of the augmented repair observed. This low infection rate is similar to what was observed by Kasten et al 32 (1 in 29 repairs) and O’Dowd et al 42 (2.4% in their series).
Regarding development of stiffness, although there were 4 cases in the isolated repair group compared with 2 in the augmentation group, we did not find significant differences between the groups. None of the cases of stiffness development entailed bilateral PTRs. All 4 knees with isolated repair were treated using a transosseous tunnel technique, whereas in the 2 knees with stiffness in the augmentation group, 1 case involved repair with anchors and allograft (PTT) and the other case involved tunnels in conjunction with autograft (STG). Our results were similar to those observed by Marder and Timmerman, 37 who reported that 5 of 15 patients had a flexion deficit >10° in primary PTR repair, and those observed by Hantes et al, 23 who reported that 27% of patients experienced reduced knee flexion. In our study, all patients underwent postoperative physical therapy; however, these results could be partly explained by a conservative rehabilitation protocol in our center.
Excluding cases that presented rerupture, we found 1 knee in each group with extension lag >5°, with no significant differences observed between both groups, resulting in an overall rate of 5.6%6.1%. These numbers do not differ from those reported by Carlson Strother et al 9 (9.3%), Roudet et al 46 (8%), or Kasten et al 32 (9%).
All these results suggest that despite the theoretical possibility that a biological augmentation of patellar tendon repair could be more invasive and have higher surgical morbidity compared with isolated repair in acute PTRs, biological augmentation is not, in practice, associated with the development of more immediate or midterm complications.
Limitations and Strengths
We identified several limitations in our study. First is our study's retrospective, noncontrolled, single-center nature. Additionally, due to the low prevalence of the injury, the sample size was small, although similar in characteristics. Second, we lacked patient-reported outcome scores and radiological measurements, which would be desirable in this type of research. Our study also posed strengths, such as both groups being comparable in size and demographic characteristics, standardization of the compared surgical techniques, and postoperative management. Additionally, our study is the first to directly compare isolated repair techniques versus biological augmentation in acute PTRs, allowing us to determine a reduction in the failure rate without increasing adverse effects in biological augmentations.
Conclusion
Our findings suggested that biological augmentation reduced the failure rate of acute PTR repairs without being associated with increased immediate or midterm complications. Given these results, it appears necessary to conduct randomized studies to confirm these findings or help establish causality in this association.
Footnotes
Final revision submitted March 15, 2024; accepted April 8, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Equipo de Rodilla Hospital del Trabajador.