
Abstract
Background:
Long-term follow-up for anterior cruciate ligament reconstruction (ACLR) is limited due to heterogeneity in the number of techniques utilized, the number of surgeons included, and attrition bias.
Purpose:
To analyze a single surgeon's 35-year experience with ACLR using the transtibial technique, with an emphasis on temporal trends in graft selection and subanalyses on rates of revision surgery, contralateral ACLR, and nonrevision reoperation among different demographic cohorts of patients.
Study Design:
Case series; Level of evidence, 4.
Methods:
All patients who underwent arthroscopically assisted single-bundle ACLR between 1986 and 2021 were identified from a prospectively maintained single-surgeon registry. Outcomes of interest included revision, reoperation, and contralateral rupture rates.
Results:
A total of 2915 ACLRs were performed during the senior surgeon's career. The mean age for primary ACLR was 29.4 ± 14.8 years. During primary ACLR, 98.4% of patients received a central-third bone-patellar tendon-bone (BPTB) graft. Increasing patient age was associated with increasing allograft usage (P < .01), with a significant temporal increase in allograft usage over the senior surgeon's career (P < .01). There was a higher revision rate among younger patients (P < .01), female patients aged 21 to 25 years (P = .01), and patients who received an allograft during the primary procedure (P = .04). The contralateral rupture rate showed no difference between sexes (P = .34); however, patients who underwent ACLR with autograft had a greater rate of contralateral injury compared with those with allograft (P < .01). The contralateral rupture rate was greater than the revision rate (P < .01). The most common causes of nonrevision reoperation were failed meniscal repair, new meniscal tears, arthrofibrosis, and painful hardware removal.
Conclusion:
The findings of this single-surgeon registry reveal temporal trends in ACLR over a 35-year career. There was a trend toward increasing BPTB allograft use in ACLR, especially in older patients and revision cases. A greater revision rate was observed among younger patients, female patients, and those receiving allografts during primary surgery. Contralateral ACLR was more common than revision surgery.
Keywords
Anterior cruciate ligament (ACL) reconstruction (ACLR) has changed drastically over the last 40 years, starting with the introduction of an arthroscopically assisted technique in the 1980s. 19 The evolution of the 2-incision technique followed by the utilization of a transtibial (TT) reconstruction allowed for improvement in patient outcomes, cosmetic benefits, and more anatomic reconstruction compared with previous techniques. 16 More recently, the paradigm shift to using an independent anteromedial (AM) portal for femoral tunnel drilling has been adopted to overcome potential shortcomings of the TT method, such as femoral tunnel depth, angulation, and ultimately impact on the graft bending angle during ACLR.25,26,46 Graft utilization has also evolved during this period. Despite the risks for patellar fracture and residual anterior knee pain, bone-patellar tendon-bone (BPTB) autograft remains the most commonly used tissue in younger athletic individuals because of its long-term outcomes, low failure rates, and a high return-to-sports rates.17,22,31,48
The impact of femoral tunnel location during ACLR with the AM and TT approaches has been an area of prolific research.2,14,41 While some clinical studies have shown higher ACLR failure rates due to a vertically oriented femoral tunnel and a higher rate of posttraumatic osteoarthritis with the TT technique,8,30 several large-scale international registries have demonstrated a greater revision rate with AM tunnel drilling.13,36,44 Various modifications to the TT technique have been investigated to improve outcomes, including utilizing a proximal starting point and drilling the tibial tunnel in a more oblique trajectory. The goals of technical changes such as these are to allow for more anatomic femoral tunnel placement and improve rotational stability, in addition to the already excellent anteroposterior stability provided by the traditional TT technique. 33
Prior cohorts of this registry have been published over 25-year and 30-year intervals.5,38 However, the last 5 years of the senior surgeon's (B.R.B.) career were not previously published. The purpose of this study was to describe and holistically analyze a single surgeon's 35-year experience with ACLR utilizing predominantly a TT approach, with an emphasis on understanding revision, reoperation, and graft usage rates over time. We hypothesized that within the last 5 years of the senior author's (B.R.B.) career, there would be (1) a continued temporal rise in BPTB allograft usage given the increased graft availability, (2) an older cohort of patients continuing to seek ACLR surgery from the senior author, and (3) maintenance of between-group trends in revision rates, contralateral rupture rates, and nonrevision reoperation rates from the 25-year and 30-year analyses despite the former 2 hypotheses.
Methods
This study was an institutional review board–approved retrospective review of a prospectively maintained computerized surgical registry of the senior author's practice at a single, high-volume institution. All patients within this database undergoing primary or revision ACLR between September 1986 and December 2021 were included in this study. Patients who underwent primary ACL repair and those who had multiligamentous reconstructions, knee dislocations, ACL tibial eminence fractures, or concurrent osteotomies were excluded from this study. Variables extracted included patient age, sex, laterality, graft used, incidence of revision surgery, incidence of nonrevision reoperation, and time to subsequent procedures. No in-person follow-up was conducted specifically for this study. Revision, re-revision, or subsequent reoperation rates were calculated for patients returning to the senior author's practice for subsequent care after index ACL surgery. Patients not returning for subsequent care were assumed to have had a successful surgical outcome. Cohorts of this data set have previously been reported at 25-year and 30-year follow-ups.5,38
Surgical Technique
All ACLR procedures were performed using an arthroscopically assisted, single-bundle technique. Between 1986 and October 1991, a 2-incision technique was used (involving independent outside-in femoral tunnel drilling), and since October 1991, a TT technique was used. The specifics of the surgical technique have been published in multiple journals and textbooks.20,34,51 The central one-third of a BPTB autograft or allograft was utilized almost exclusively, as it has been shown to be biomechanically superior to the medial and lateral portions of the BPTB graft. 50 An accessory inferolateral portal was utilized through the patellar tendon to facilitate the insertion of a variable tibial aimer guide for the creation of the tibial tunnel. This modification allowed for more rotational flexibility of the aiming device and a more distal starting point on the tibia, thus reducing the potential for graft tunnel mismatch, and obviated the more vertical orientation that can occur if the aiming device is inserted through a standard inferomedial portal. Metal interference screws were exclusively used for graft fixation. Final graft fixation was achieved with the knee in complete extension or hyperextension. An accelerated postoperative rehabilitation program with full range of motion and full weightbearing has been used since 1990, whereas before this, weightbearing was delayed and the knee was maintained in terminal extension until 6 weeks postoperatively.
Statistical Analysis
Data were extracted from the database and analyzed by an independent statistician. Descriptive statistics were used to describe the cohort undergoing primary and revision ACLR. After confirmation of normality using Shapiro-Wilk test, the Student t test and analysis of variance were used for inferential statistics regarding continuous data. Fisher exact and chi-square tests were used for inferential statistics regarding categorical data (patient sex, graft choice, rate of revision ACLR, and rate of reoperation). An alpha level of .05 was determined to be of statistical significance. All descriptive statistics were performed in Excel (Microsoft Corporation). Inferential statistics were performed using R (RStudio Version 2021.09.1+372 “Ghost Orchid” release for macOS).
Results
Between September 1986 and December 2021, the senior author performed 2915 ACLRs, of which 2616 (89.7%) were primary procedures, 270 (9.3%) were revision procedures, and 29 (1.0%) were re-revision procedures. Demographic data for patients undergoing primary, revision, and re-revision ACLR are shown in Table 1. There were significantly more male than female patients in the primary ACLR (P < .01) cohort but not in the revision (P = .26) or re-revision (P = .69) cohorts. The mean age for patients at the time of primary ACLR was 29.4 ± 14.8 years, which did not differ significantly from patient age at the time of revision reconstruction (29.4 ± 9.3 years) or at the time of re-revision reconstruction (28.0 ± 7.2 years) (P = .87).
Demographic Data for Patients Undergoing Primary, Revision, and Re-revision ACLR a

ACLR, anterior cruciate ligament reconstruction.
Graft Selection
Graft selection for primary ACLR is shown in Table 2. Of 2616 patients undergoing primary ACLR, 2573 (98.4%) received a central-third BPTB autograft or allograft, the senior author's preferred graft choice. It should be noted that 65% of the cohort received autograft BPTB grafts and 33% received allograft BPTB grafts. The ages of these 2 cohorts were significantly different (P < .01). Hamstring autograft or allograft was utilized in select primary cases and was typically reserved for skeletally immature patients who were significantly younger than the BPTB cohort at the time of surgery (P < .01).
Graft Use for Primary ACLR a

ACLR, anterior cruciate ligament reconstruction; BPTB, bone-patellar tendon-bone; HS, hamstring; Quad, quadriceps tendon.
Patients undergoing allograft reconstruction were significantly older than those undergoing autograft reconstruction (P < .01). There was a direct association between the rate of allograft use in primary ACLRs and patient age at surgery (P < .01) (Figure 1). Additionally, the senior author's practice showed a greater use of allograft tissue in primary ACLR over time (P < .01). Figure 2 depicts the 5-year trends in allograft use for primary ACLR. Whereas only 1.4% of primary reconstructions between 1986 and 1991 used allograft tissue, 54.3% of primary cases used allograft tissue between 2017 and 2021. Of these allograft reconstructions, 119 (13.7%) patients had a nonirradiated allograft (before September 2003) and 749 (86.3%) patients had allografts that were processed and sterilized with low-dose (1.2 Mrad) irradiation (September 2003 and beyond) from a single American Association of Tissue Banks–certified tissue bank (AlloSource).

Percentage of allografts used for primary anterior cruciate ligament reconstruction in each age cohort.
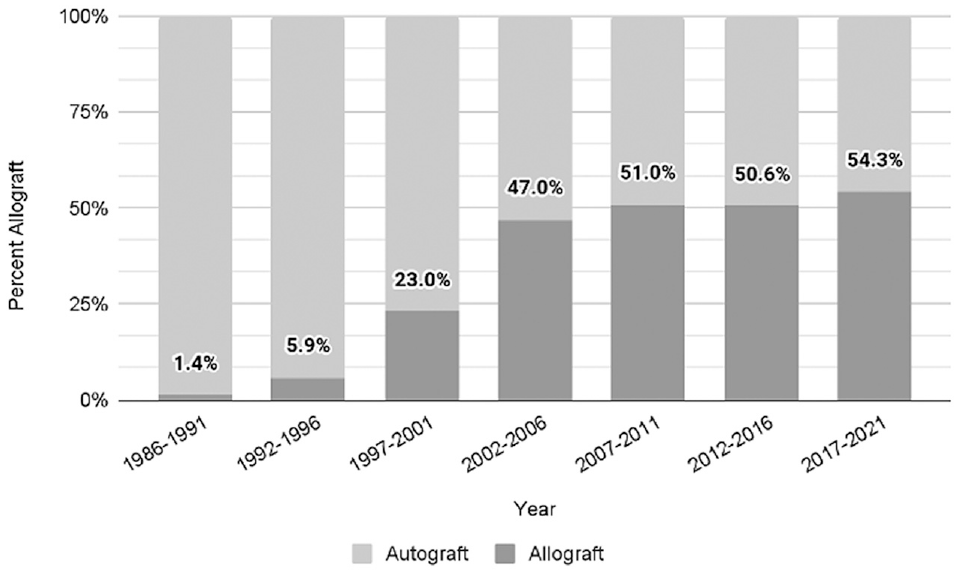
Trends in anterior cruciate ligament allograft use by year in surgeon's practice.
Revision Surgery
There were 270 revision ACLRs performed within the data set. Of these, 53 revision surgeries were personal revisions (ie, patients undergoing primary and subsequent revision ACLR with the senior author), imparting an overall personal revision rate of 2.0% (53/2616). The personal revision rate for patients undergoing a 2-incision approach was 3.1% versus 1.9% for patients undergoing a TT approach; however, this difference did not reach statistical significance (P = .24). There was a significantly lower revision rate among older patients compared with younger patients (P < .01). Figure 3A depicts the revision rates as a function of age and sex. The revision rate among female patients was 2.8% versus 1.4% among male patients, representing a significant difference (P = .01). This difference was most pronounced among younger patients and became less pronounced among older patients. Figure 3B depicts the rate of revision as a function of age and graft type (ie, autograft vs allograft). The revision rate was 1.6% among autograft primary ACLRs and 2.8% among allograft primary ACLRs, representing a significant difference (P = .04). This difference was most pronounced among patients aged 21 to 25 years (P < .01). It should be noted that there were specific reasons that allografts were used in this younger cohort (eg, patient request, concerns about rehabilitation compliance, or lower activity demands). Figure 3C demonstrates the time to revision ACLR as a function of graft type. The most common timeframe for graft rupture in the autograft and allograft groups was 1 to 3 years after primary reconstruction. There was no difference in primary ACLR failure rates among patients receiving a BPTB autograft (13.8%) versus BPTB allograft (12.5%) within the first postoperative year (P = .89).

Rate of revision of primary anterior cruciate ligament reconstruction as a function of (A) age and sex and (B) age and graft type. (C) Time to revision anterior cruciate ligament reconstruction as a function of graft type. s/p, status post.
Graft selection for revision ACLR is shown in Table 3. Among patients undergoing revision ACLR, the preferred graft choice was BPTB allograft, accounting for 199 (73.7%) revision reconstructions. In revision cases using BPTB autograft, 61 (92.4%) cases harvested the patellar tendon from the ipsilateral knee, whereas 5 (7.6%) cases harvested the patellar tendon from the contralateral knee (in cases of previous ipsilateral BPTB graft harvest during primary reconstruction or patellar tendon insufficiency).
Graft Use for Revision ACLR a

ACLR, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; HS, hamstring; Quad, quadriceps tendon.
Contralateral Surgery
There were 149 contralateral ACL injuries requiring ACLR within the data set, indicating an overall rate of 6.0%. The rate of contralateral surgery was significantly higher than the rate of personal revisions (P < .01). The mean time to contralateral injury was 52.2 months. The rate of contralateral injury was 5.6% among male patients versus 6.6% among female patients; however, this difference did not reach statistical significance (P = .34). Table 4 describes the contralateral ACL rupture rate between autograft and allograft ipsilateral ACLRs. Patients undergoing autograft ACLR had a significantly higher rate of contralateral injury than those undergoing allograft ACLR (P < .01). However, there was no significant difference in the duration to contralateral injury based on graft type (P = .42).
Contralateral ACL Rupture Rate as a Function of Primary Reconstruction Graft Type a
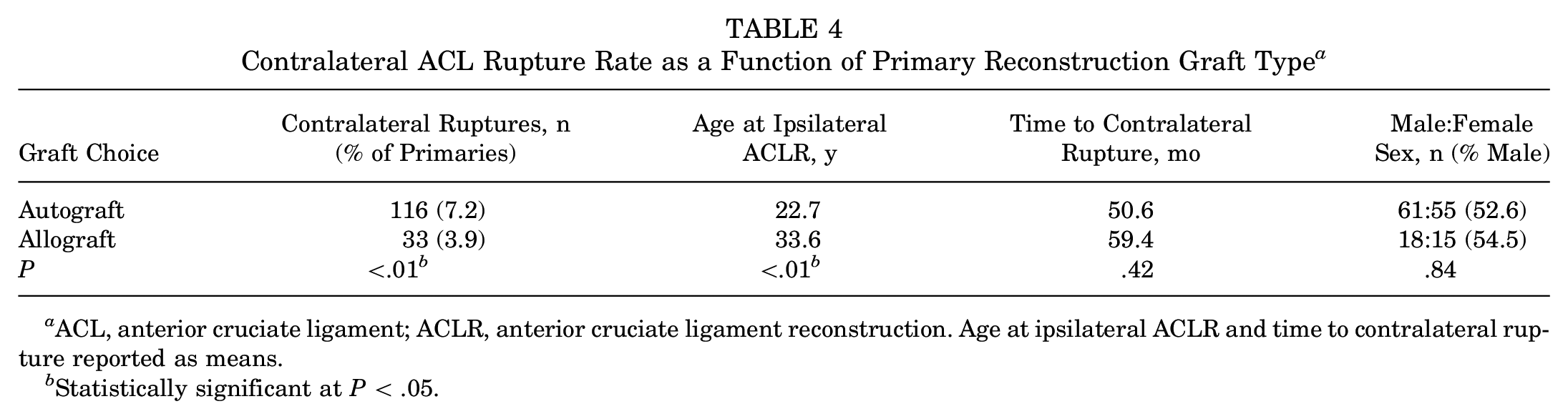
ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction. Age at ipsilateral ACLR and time to contralateral rupture reported as means.
Statistically significant at P < .05.
Other Reoperations
The overall rate of nonrevision reoperation after primary ACLR was 12.9% (n = 337). The nonrevision reoperation was 12.9% after autograft reconstruction versus 12.7% after allograft reconstruction (P = .22). The mean time to reoperation was 51.3 months (range, 0.5-316 months). Figure 4 describes the frequency of nonrevision reoperations after primary ACLR as a function of graft type (ie, autograft vs allograft). The most common causes of reoperation by percentage were failed meniscal repairs (n = 79, 3.0%), new meniscal tears (n = 92, 3.5%), arthrofibrosis requiring lysis of adhesions (n = 86, 3.3%), and painful hardware requiring removal (n = 22, 0.8%).

Incidences of subsequent nonrevision reoperation as a function of graft type. DJD, degenerative joint disease; HFPS, hypertrophic fat pad syndrome; HTO, high tibial osteotomy; I&D, irrigation and debridement; IPT, infrapatellar tendon; LOA, lysis of adhesions; MCL, medial collateral ligament; PLC, posterolateral corner; ROH, removal of hardware.
Discussion
The present investigation provides the longitudinal experience of a sports medicine surgeon over a period of rapid change in the treatment of ACL injuries, allowing for an understanding of the trends in reconstruction during this time. The salient findings are the following: (1) the mean age for primary ACLR (29.4 ± 14.8 years) was not significantly different for revisions (29.4 ± 9.3 years) or repeat revisions (28.0 ± 7.2 years); (2) 98.4% of primary ACLRs received a central-third BPTB graft and the mean ages for autografts and allografts were 21.6 and 37.7 years, respectively; (3) increasing allograft use was associated with increasing patient age in the senior surgeon's practice; (4) revision ACLR cases utilized a BPTB allograft the most (73.7%); (5) a significantly higher revision rate was observed in younger patients, female patients (most pronounced at ages 21-25 years), and those who underwent allograft during the primary procedure; (6) the personal revision rate for patients with primary autograft (1.6%) was significantly lower than that for patients with primary allograft (2.8%); (7) the personal revision rate for male patients (1.4%) was significantly lower than that for female patients (2.8%); (8) the personal revision rate for the TT approach (1.9%) was lower than that for the 2-incision approach (3.1%), although this difference was not significant; (9) the overall contralateral rupture rate was 6.0%, with no difference between sexes, although autografts resulted in higher contralateral injury than allografts; and (10) the most common causes of nonrevision reoperation were failed meniscal repair, new meniscal tear, arthrofibrosis, and painful hardware removal. Previous cohorts of this data set have been published at 25 and 30 years of follow-up; the present investigation provides a greater sample size of data—particularly for allograft ACLR—as well as a novel subanalysis on 2-incision versus TT ACLR outcomes.5,38
Temporal trends have shown a national and global shift from the traditional TT technique to the independent AM femoral tunnel drilling technique over the last 20 years. 45 Some argue that independent femoral tunnel drilling allows for more anatomic graft placement, which better resists rotational stress. 3 This is contrary to a more vertical tunnel, which primarily can only resist anterior translational force. However, while potentially more technically demanding than AM drilling, the results of the current study suggest that the TT technique can achieve long-term graft survivorship, potentially suggesting satisfactory tunnel placement. Several cadaveric studies have sought to refine the TT approach in order to optimize femoral tunnel placement. Bhatia et al 3 found that using a 10-mm half-fluted reamer led to a tibial tunnel 4.35 mm more anterior relative to one drilled with a full-fluted reamer. As a more posterior tunnel results in more vertical graft placement, utilization of a half-fluted reamer may assist in obtaining a more horizontal femoral tunnel placement with the TT technique. 3 Piasecki et al 33 assessed the effect of tibial tunnel starting point location and orientation on femoral tunnel positioning using 8 cadaveric specimens and computer-assisted navigation. When comparing starting positions of 15.9 mm and 33.0 mm distal to the joint line, the more proximal position resulted in significantly greater tibial footprint overlap (97.9% vs 71.1%) as well as greater femoral overlap (87.9% vs 59.6%). The authors concluded that a highly anatomic tunnel can be achieved using a modified TT approach, where the tibial starting point is more proximal than with traditional techniques. In the current study, the senior author's technique has allowed for an obliquely oriented tibial tunnel, which results in a lower femoral tunnel position on the lateral wall of the intercondylar notch. 20 The senior author utilized an accessory inferior portal through the patellar tendon for oblique orientation of the tibial aiming device. 38 The results of the aforementioned cadaveric studies and those of the current study demonstrate that a successful and durable TT ACLR can be achieved but requires a meticulous approach to each step during tunnel drilling.
A modified TT technique has been adopted throughout the world for its benefits, which include allowing for anatomic reconstruction without the need for hyperflexion of the knee, minimizing graft bending angles, and ultimately decreasing strain on the graft during healing.10,27,43,48 Those in favor of an AM approach note the greater ease of achieving anatomic femoral tunnel placement, as well as the option to hyperflex or maintain more natural knee flexion during femoral drilling by using a flexible reaming system with comparable outcomes.15,29 Yet, the possibility of damaging the medial femoral condyle while crossing the notch, decreased load to failure and graft tunnel mismatch due to a shorter femoral tunnel (<25 mm), and risk of posterior wall blowout have all been reported shortcomings of the AM technique.1,6,7,18
The personal revision rate after primary ACLR was 2.0%, with significantly higher rates of revision among females (2.8% vs 1.4%), younger patients, and those who received allografts during the index procedure. These findings are consistent with several studies evaluating BPTB revision and contralateral rupture rates in comparison with other autograft choices.9,21,24,35,37,39 Samuelsen et al 39 performed a meta-analysis of 47,613 patients comparing graft rupture rates between BPTB and hamstring autograft ACLR. They found that at a mean follow-up of 68 months, the BPTB and hamstring rupture rates were each 2.8%, with no significant differences in postoperative residual laxity or positive Lachman between cohorts. Conversely, a 2020 prospective study comparing BPTB and hamstring autograft use in high school and college-aged athletes found a 2.1 times greater rate of revision at a 6-year follow-up with hamstring autograft, suggesting the superiority of BPTB grafts in a younger, high-demand patient population. 40
The contralateral rupture rate in the current study was 6.0%, with no significant differences between male and female patients. Interestingly, patients who received autograft had a higher contralateral rupture rate than those who received allograft (P < .01). This may be explained by the differences in populations, with patients who received an autograft being younger and more active than those who received allograft. These contralateral rupture rates are lower than the pooled contralateral rupture rate (11.8%; range, 8.2%-16.0%) found in a systematic review evaluating prospective level 1 and 2 studies utilizing BPTB and hamstring autograft. 49 It is important to note that revision rates and contralateral rupture rates from the literature must be analyzed in the context of potential risk factors. Several studies have found that female sex,4,32 younger age (<25 years),9,11 generalized joint laxity, 24 and the decision to use autograft or allograft9,23,28,42 all contribute to revision and contralateral rupture.
In the senior author's practice, the increasing trend of allograft usage over time and with patients >30 years of age is due to an overall older patient cohort in the surgeon's practice, observed successes, low morbidity rates, patient subjective satisfaction, and comfort with performing BPTB allograft ACLR. 12 The higher rate of revision with allograft in a younger population is consistent with the existing literature. 47 However, the disparity in failure rates between autograft and allograft in the current study was found to have a significant decrease after patients reached the age of 25 years and became only about 1% after age 30. Furthermore, the (nonsignificantly) lower nonrevision reoperation rate for patients who received allografts, in combination with reduced surgical morbidity, supports the use of allografts in an older patient population.
The data within this study were derived from a prospectively maintained, single-surgeon registry of ACLRs conducted at a single, high-volume institution. However, the use of registry data is inherently limited because of the lack of follow-up for the vast majority of patients. The data, specifically reoperation and revision rates, presented in the current paper reflect patients who returned to the senior author's practice for further care. It is not possible to assess the cohort of patients who either did not need further care or sought care elsewhere for subsequent injury after the initial ACLR. This attrition bias leads to an underestimate of the true reoperation, revision, and contralateral rupture rates in this cohort of patients. Furthermore, while we assume that the attrition bias is likely uniform within our practice, some groups of patients may be more likely than others to return for subsequent care, thus potentially limiting the strength of our between-group comparisons as well. Another consideration is that the surgeon and patient demographic factors may be specific to the senior surgeon's practice and may not be as broadly applicable to the general population undergoing ACLR. Furthermore, the database used for this study is largely focused on operative and demographic information. As a result, we were unable to provide further information on the mechanism of injury, patient-reported outcomes, and activity level.
Conclusion
The findings of this single-surgeon registry reveal temporal trends in ACLR over a 35-year career. There was a trend toward increasing BPTB allograft use in ACLR, especially in older patients and revision cases. A greater revision rate was observed among younger patients, female patients, and those receiving allografts during primary surgery. Contralateral ACLR was more common than revision surgery.
Footnotes
Final revision submitted January 28, 2024; accepted February 23, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.J.R. has received education payments from Medwest Associates, Arthrex, and Crossroads Orthopedics LLC; consulting fees from Vericel; and hospitality payments from Wright Medical Tech and Stryker. J.C. has received education payments from Medwest Associates, Arthrex, and Smith+Nephew; consulting fees from RTI Surgical, Smith+Nephew, Vericel, Arthrex, and DePuy Synthes Products; nonconsulting fees from Smith+Nephew and Arthrex; compensation for serving as faculty or as a speaker for a nonaccredited and noncertified continuing education program from Linvatec; a grant from Arthrex; and hospitality payments from Medical Device Business Services, Medwest Associates, and Stryker. B.R.B. has received consulting fees from OsteoCentric Tech; hospitality payments from OsteoCentric Tech; and honoraria from NovoPedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (ref No. 13051304-IRB01).