
Abstract
Background:
Addressing patella alta often involves a distalization of the tibial tubercle with an osteotomy. Yet such osteotomies have several potential complications, including nonunion, fracture, and hardware irritation. In addition, tibial tubercle osteotomies are contraindicated in children because of the presence of an open tibial tubercle apophysis.
Purpose/Hypothesis:
The primary aim of this study was to quantify the change in the Caton-Deschamps Index (CDI) and the maximum patellar tendon elongation achieved with cyclic loading with a novel transection-free patellar tendon imbrication method in cadaveric specimens. The authors hypothesized that the imbrication technique would achieve at least 1 cm of shortening and an improvement in CDI by 0.30 from pre- to postoperative imaging.
Study Design:
Controlled laboratory study.
Methods:
Ten fresh-frozen skeletally mature cadaveric knees without a history of knee surgery were used for the laboratory portion of the study. A pulley system was utilized to suspend 45 N (10 lb) from the quadriceps tendon to mimic physiological loading of the quadriceps tendon. Seven figure-of-8 high-molecular-weight polyethylene sutures were placed in the patellar tendon and tied sequentially. The patellar tendon was measured with a ruler to assess pre- and postimbrication tendon length. Computed tomography scans were obtained both before and after imbrication, and the change in CDI was calculated. To assess patellar tendon elongation, the tibia and patella were fixed to a servohydraulic load frame using custom fixtures, and the patellar tendon was dynamically loaded between 50 and 400 N at 0.5 Hz for 500 cycles. Statistical significance was determined at a P value <.05.
Results:
In the cadaveric specimens, there was a significant decrease in patellar tendon length from pre- to postimbrication (47.2 ± 7.0 mm vs 36.8 ± 7.2 mm; P < .001), with a mean patellar tendon shortening of 10.4 ± 0.97 mm. There was also a significant decrease in the CDI from pre- to postimbrication, with a mean change in CDI of 0.33 ± 0.09 (P = .014). The mean maximum patellar tendon elongation was 3.9 ± 1.7 mm after 500 cycles.
Conclusion:
The novel transection-free patellar tendon imbrication technique can be used to reduce patellar tendon length and CDI at time zero. This technique may be useful in skeletally immature patients with incompletely ossified tibial tubercle apophyses.
Clinical Relevance:
The transection-free patellar tendon imbrication technique can be used in skeletally immature patients to correct patella alta without risking potential growth arrest due to the presence of an open tibial tubercle apophysis. Moreover, this technique avoids potential complications of distalizing tibial tubercle osteotomies for the correction of patella alta in skeletally mature patients, including nonunion, fracture, and hardware irritation.
Patella alta is defined as a Caton-Deschamps Index (CDI) >1.3. Patella alta predisposes patients not only to patellar instability 8 but also to patellofemoral pain.6,10 Addressing patella alta often involves a distalization of the tibial tubercle with an osteotomy. Yet, such osteotomies have several potential complications, including nonunion, fracture, and hardware irritation. 12 In addition, tibial tubercle osteotomies (TTOs) are contraindicated in children because of the presence of an open tibial tubercle apophysis.
For skeletally immature patients, patellar tendon transfer or patellar tendon imbrication can be utilized to address patella alta. However, patellar tendon transfer can only be utilized in relatively younger patients and risks complete—and potentially catastrophic—disruption of the extensor mechanism. 1 Alternatively, patellar tendon imbrications have been performed by transecting the patellar tendon and suturing the tendon in a shortened position. 5 This technique has been shown to maintain correction of patella alta, both clinically and radiographically, at 2 years postoperatively. 11 However, this technique again risks catastrophic intraoperative or postoperative disruption of the tendon. 5 The use of a transection-free patellar tendon imbrication technique would mitigate the risk of potential disruption of the extensor mechanism. Hinkley et al 3 described a novel patellar tendon imbrication method in a technique paper published in Arthroscopy Techniques. However, no previous studies have evaluated the efficacy of this procedure, either biomechanically or clinically.
The primary aim of the present study was to quantify the amount of patellar tendon shortening and the change in the CDI achieved with a novel transection-free patellar tendon imbrication method using cadaveric specimens, with additional assessment of elongation with cyclical loading. We hypothesized that the transection-free patellar tendon imbrication method would achieve a mean of 1 cm of patellar tendon shortening, as measured by a ruler, from pre- to postimbrication in the cadaveric specimens, with minimal (<5 mm) elongation on cyclical loading. Moreover, we hypothesized that there would be an improvement in CDI by 0.30 from pre- to postoperative imaging.
Methods
Ten fresh-frozen cadaveric knees were obtained for the study. Institutional review board approval was not required, as this study used deidentified cadaveric specimens. Cadavers with a history of knee surgery were excluded. Specimens were stored at −20°C. Starting at 24 hours before the planned dissection, the cadaveric specimens were allowed to begin thawing at room temperature.
Specimen Preparation
All superficial soft tissues were removed, leaving the patellar tendon, quadriceps tendon, medial patellofemoral ligament, lateral patellofemoral ligament, retinaculae, and capsule intact. Two No. 2 Ethibond (Ethicon) sutures were used to suture proximally and distally in the quadriceps tendon in Krackow fashion and secured to a 45-N (10-lb) weight via a pulley system (Figure 1) to simulate the physiological pull of the quadriceps tendon on the patella. 14

Pulley system used to simulate physiological pull on the quadriceps tendon.
Imbrication Technique
The length and width of the patellar tendon were measured preimbrication. A standard anterior approach to the knee was performed. The paratenon was incised longitudinally. Seven figure-of-8 No. 2 high-molecular-weight polyethylene sutures were placed in the patellar tendon, per the technique described by Hinkley et al. 3 The proximal-central and distal-central sutures were tied first to try to achieve the maximum amount of shortening. The remaining sutures were then tied sequentially (Figure 2). The length and width of the patellar tendon were then measured postimbrication. The goal for shortening of the imbrication was 1 cm.

Patellar tendon imbrication technique as described by Hinkley et al. 3
CDI Calculation
For the cadaveric specimens, a computed tomography (CT) scan was obtained preimbrication and immediately postimbrication. The knees were placed in full extension for the CT scan, as a pulley system was used to mimic physiological pull of the quadriceps tendon on the patella (Figure 1). The CDI was calculated as the ratio of the distance between the anterior-most aspect of the proximal tibial articular surface and the inferior-most aspect of the patellar articular cartilage divided by the length of the patellar articular cartilage on the sagittal CT image 2 slices lateral to the anterior cruciate ligament tibial attachment.
Cyclic Loading
Cyclic loading was performed to determine if the sutures used for the imbrication would fail with loading. The tibia and patella were potted and mounted on a servohydraulic load frame using custom fixtures (Instron). The tibia and patella were fixed in 0° of flexion, and the patellar tendon was dynamically loaded between 50 and 400 N at 0.5 Hz for 500 cycles. A motion capture system was used to calculate the displacement of the tibial tubercle from the inferior pole of the patella (elongation of the patellar tendon). 13
Statistical Analysis
Data were normally distributed per the Shapiro-Wilk test. Paired t tests were used to evaluate the change in patellar tendon length and the change in CDI from pre- to postimbrication. Statistical significance was considered at a P value <.05. Statistical analysis was performed with Stata (StataCorp, LLC).
Results
The mean age of the cadaveric specimens was 51.8 years (range, 23-68 years). Eight specimens were male, and there were 9 right knees.
There was a significant amount of shortening achieved with the transection-free patellar imbrication technique, with a mean amount of patellar tendon shortening of 10.4 mm (P < .001) (Table 1, Figure 3). There was no difference in the width of the patellar tendons from pre- to postimbrication (P = .26). There was a significant decrease in CDI from pre- to postimbrication, with a mean decrease in CDI of 0.33 ± 0.09 (P = .014) (Figure 4).
PT Length and Width and CDI Values for Cadaveric Specimens Both Pre- and Postimbrication a

CDI, Caton-Deschamps Index; PT, patellar tendon.
Delta = final value − starting value.
Delta = postoperative value − preoperative value.

(Left) Cadaveric specimen preimbrication with a patellar tendon length of 45 mm. (Right) Cadaveric specimen postimbrication with a patellar tendon length of 35 mm.

Sagittal computed tomography scans demonstrating the change in Caton-Deschamps Index (CDI) from (left) preimbrication (1.53) to (right) postimbrication (1.21). Post, postimbrication; Pre, preimbrication.
The mean elongation of the patellar tendon after 500 cycles of load at 50 N was 3.9 ± 1.7 mm (Figure 5). Before cyclic loading, the mean resting length of the patellar tendon at 45 N was 36.8 mm. After 500 cycles, the mean resting length of the patellar tendon at 50 N was 40.7 mm. None of the sutures failed in any specimen after 500 cycles of loading at 50 to 400 N.
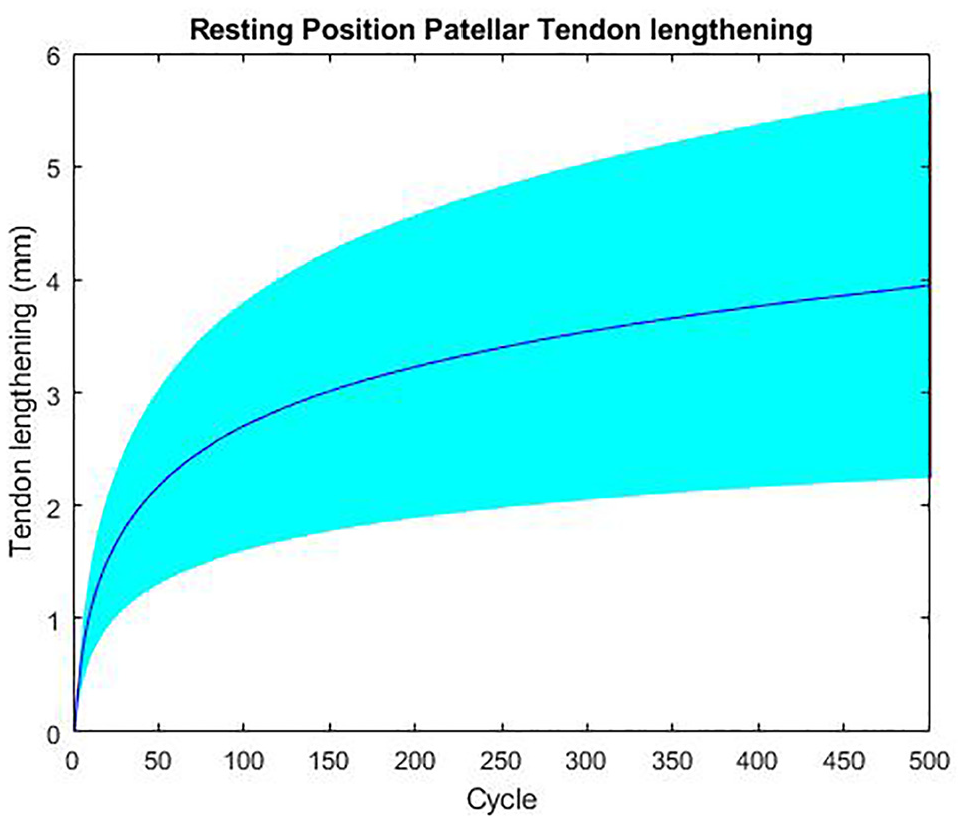
The mean and standard deviation for the translation of the patella, or elongation of the patellar tendon, at 50 N during each cycle of patellar tendon tension.
Discussion
These findings suggest that a novel, transection-free patellar tendon imbrication technique can decrease patellar tendon height by a mean of 1 cm and decrease CDI by a mean of 0.33. The resting length of the patellar tendon increased by a mean of 3.9 ± 1.7 mm after 500 cycles of load at 50 N. None of the sutures failed after 500 cycles of patellar tendon loading. As such, this technique may be used to correct patella alta in skeletally immature patients.
Patellar tendon imbrication for the correction of patella alta poses numerous advantages over TTO, including diminished risk of nonunion, fracture, and hardware irritation. 12 Moreover, patellar tendon imbrications can be performed in skeletally immature individuals, as this technique does not risk damage to the open tibial tubercle apophysis. Previously evaluated patellar tendon imbrication techniques involve tendon transection and shortening; however, the risk of intraoperative or postoperative disruption of the tendon 5 renders this method suboptimal. The transection-free imbrication technique described in this study mitigates the risk of the aforementioned complications and may be performed in pediatric patients without risk of physeal disturbance. Moreover, even if this transection-free imbrication technique fails, there will be no issue returning for TTO once the patient is skeletally mature.
Previous studies examining the efficacy of TTO in the correction of patella alta have found that TTO may be used to adequately correct patella alta, although the reoperation rate after this procedure remains high at 14.3%. 7 Our results are similar to those of Patel et al, 11 who found a mean correction of 1 cm of shortening and a change in CDI of 0.3 at 2 years postoperatively using a patellar tendon imbrication technique that involves tendon transection. In addition, Hyer et al 4 was able to achieve a correction of patella alta, measured by improvement in Koshino-Sugimoto index from 1.3 to 1.1 at 6 weeks postoperatively, using a “pants over vest” transection-free patellar tendon imbrication technique in conjunction with a distal femoral extension osteotomy in pediatric patients with cerebral palsy, knee flexion contracture, and patella alta. However, the Koshino-Sugimoto index relies on landmarks of the distal femur for evaluation of the patellar height. Given that a distal femur anterior closing-wedge osteotomy was performed in combination with the patellar tendon imbrication in the aforementioned study, the true amount of patellar tendon shortening achieved may be overestimated with the Koshino-Sugimoto index.
The total change in the length of tendon after cyclic loading is due to a combination of creep in the patellar tendon and creep in the sutures used for the imbrication. Previous biomechanical studies examining tendon elongation using a cyclic loading model have demonstrated that normal tendon creep with cyclic loading is in the 1.9- to 3.7-mm range.2,9 The mean amount of tendon elongation at 50 N in the present study, 3.9 ± 1.7 mm, is within expected limits of tendon creep with cyclic loading, although we cannot definitively say that this is due to tendon creep alone, as opposed to tendon creep plus creep from the sutures. Future biomechanical studies using intact cadaveric knees will better delineate the amount of creep from the patellar tendon itself versus creep from the sutures used for the imbrication.
Limitations
There are several limitations to the present study. First, this is a time-zero cadaveric study, and there may be changes in patellar tendon length that occur postoperatively after imbrication in an active biological environment. The results of the present study do not account for healing of the patellar tendon postimbrication, which may affect the degree of patellar shortening or biomechanical properties of the tendon with cyclic loading. Moreover, the amount of correction achieved in the cadavers is potentially greater than that which could be achieved in a living patient with muscle tone. In addition, although the cadaveric specimens used in this study did not all have patella alta, the aim of the study was to demonstrate change in patellar height.
Conclusion
Our novel transection-free patellar tendon imbrication technique can be used to reduce patellar tendon length and CDI at time zero. Additional biomechanical and larger long-term clinical studies are needed to further evaluate the efficacy of this technique.
Footnotes
Final revision submitted October 10, 2024; accepted November 14, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: H.P.G. has received support for education from Smith & Nephew. P.M.I. has received support for education from Smith & Nephew and Elite Orthopedics. S.M.S. has received consulting fees from Flexion Therapeutics, Miach Orthopaedics, Smith & Nephew, and Vericel; research support from Miach Orthopaedics, Moximed, and Vericel; hospitality payments from Bioventus, Aesculap Biologics, Zimmer Biomet Holdings, Fidia Pharma, Dynasplint Systems, Pacira Therapeutics, and Organogenesis; and honoraria from JRF Ortho and Vericel; and holds stock or stock options in Engage, Smith & Nephew, and Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.