
Abstract
Background:
Clinicians commonly use a clockface model to describe glenoid lesions, but variations in the usage of best fit and outer circles are often observed. Determining the compatibility of these methods is crucial, as discrepancies may affect clinical practice and the interpretation of previous research outcomes.
Hypothesis:
The best fit circle and outer circle assess the location of glenoid bone loss differently.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
This study included 231 patients with recurrent anterior shoulder instability who underwent 3-dimensional computed tomography. The authors assessed the location, orientation, and extent of glenoid defects based on clock measurements, using templates of both the outer and best fit circles. They investigated discrepancies between the 2 methods and explored factors that influenced these discrepancies.
Results:
The orientation of the linear defect showed subtle but statistically significant differences between the circles (3:02 ± 0:21 for the outer circle and 3:03 ± 0:22 for the best fit circle; P < .001). The outer circle frequently overestimated the location of the defect's center and the superior and inferior margins (differences of 0:42 ± 0:16, 0:30 ± 0:10, and 0:17 ± 0:13, respectively; all P < .001). Additionally, the anterior or posterior placement of the best fit circle's center relative to the glenoid axis was associated with all measurement discrepancies. While discrepancies in the measurements of the center, superior, and inferior margins correlated with glenoid defect size (P < .001 for all), the orientation of the defect line did not correlate with defect size (P = .456), indicating that the defect may expand while maintaining its original angle.
Conclusion:
The defect locations of the outer circle and best fit circle differed statistically. Although the mean difference was <1 hour, caution is needed when interpreting findings across studies or in surgical communication, as reference points or clockface systems may differ between them. Among these locations, the orientation of the defect line appears stable with respect to defect size in each circle, suggesting that the defect may serve as a reliable reference for describing anchor or bone block placement during surgery.
Keywords
When addressing intra-articular lesions of the shoulder joint, a clockface model is commonly used to describe their locations, such as the 3-o’clock position, which corresponds to the anterior glenoid. Since Saito et al 21 delineated glenoid bone loss with the clockface model, their research has become the cornerstone for locating bone loss in recurrent shoulder instability. That group used the outer circle of the glenoid as a reference for the clockface and found that the majority of bone loss was oriented around the 3-o’clock position. However, the best fit circle method also gained popularity and continues to be used today.11,25,26 Consequently, many studies now use either of 2 different clockface references, the outer circle or the best fit circle, for study design and result interpretation.13,27
However, the location of bone loss using the best fit circle method has not been comprehensively analyzed. 8 Furthermore, the equivalence of location determined by the outer circle and best fit circle methods remains unexplored. If discrepancies exist, identifying the circle method used becomes critical.
This study aimed to investigate the distribution of glenoid bone loss using the best fit circle method and to determine the compatibility of the outer circle and best fit circle methods in annotating the location of bone loss. We hypothesized that the best fit circle and the outer circle assess the location of glenoid bone loss differently. Additionally, factors influencing compatibility or discrepancy were also researched.
Methods
Our institutional review board approved this study and waived the requirement for patient informed consent. We retrospectively reviewed data from 312 patients with recurrent anterior shoulder instability who underwent 3-dimensional computed tomography (3D CT) between March 2018 and February 2024. The inclusion criterion was the presence of glenoid bone loss, and patients >40 of age were excluded because morphological and size changes occur with age, which could lead to potential inaccuracies in the assessment.6,22 Patients with previous surgery or those with glenoid deformity were excluded.
The radiological measurements were performed by a shoulder fellowship-trained orthopaedic surgeon (W.S.D.) and a radiologist with 3 years of experience in musculoskeletal radiology (J.W.C.). To assess inter- and intraobserver reliability, intraclass correlation coefficients (ICCs) were calculated. We assessed the location, extent, and orientation of the glenoid defect with an en face view, using templates of both the outer and best fit circles. We drew an outer circle according to the modified version of Saito et al 21 (Figure 1). The diameter of the outer circle was defined by using a line between a supraglenoid tubercle and the most inferior point of the glenoid rather than the infraglenoid tubercle because enthesopathy and anatomic variations of the infraglenoid tubercle hinder accurate localization.10,15 Furthermore, when the defect is extended to the inferior margin of the glenoid, the infraglenoid tubercle is a more difficult reference. The best fit circle was drawn using the least squares method proposed by De Wilde et al 5 and Do et al 7 to ensure high reliability. The most anteroinferior point of the glenoid defect and the most posterior point were used as reference points. Using these and 7 additional equidistant points on the inferior glenoid rim, we constructed a mathematically best fitting circle by minimizing the squared distance from each point to the circle, as described by Do et al. 7
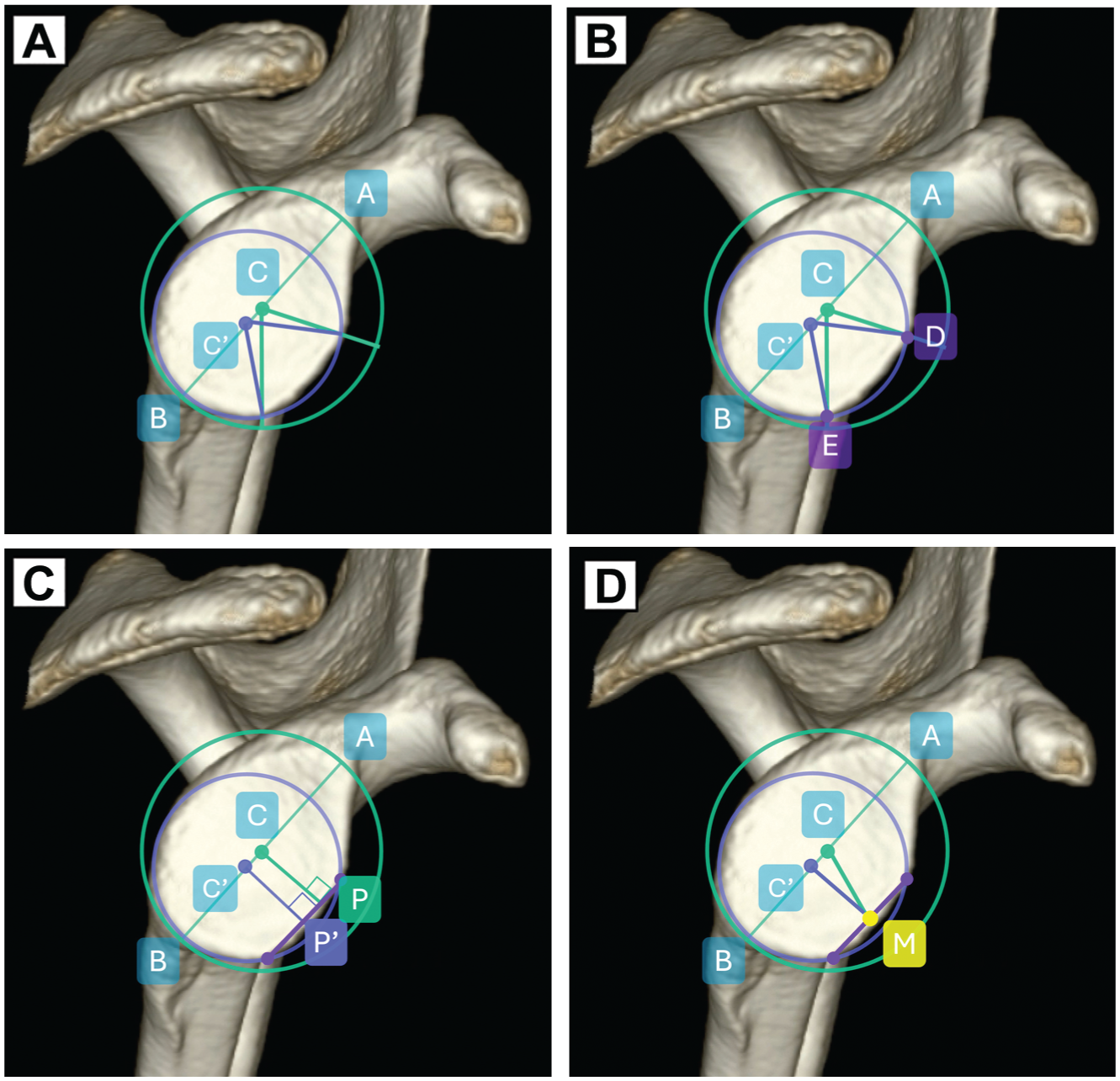
Measurement description. (A) Outer circle (green) and best fit circle (blue). The diameter of the outer circle is determined by a line connecting the supraglenoid tubercle (A) to the most inferior point of the glenoid (B). C and C′ denote the centers of the outer circle and the best fit circle, respectively. For both circles, point A is used as the reference for the 12-o’clock position. (B) Location of the superior (D) and inferior (E) margins of the glenoid bone defect. The location of the superior margin of the defect was measured by ACD for the outer circle and AC′D for the best fit circle. The location of the inferior margin of the defect was measured by ACE for the outer circle and AC′E for the best fit circle. (C) Defect line orientation. The defect line (violet line) orientation is established by a line perpendicular to the defect passing through the centers of each circle: ACP for the outer circle and ACP′ for the best fit circle. (D) Location of the defect center. The location of the defect's center (M) was gauged by the angle formed by ACM for the outer circle and AC′M for the best fit circle.
As Saito et al 21 differentiated the orientation and location of glenoid defects, we measured orientation by the angle of the defect line and location by the angles of the superior and inferior marginal points (Figure 1A). The locations of the superior and inferior margins of the defect were measured according to each circle (Figure 1B). We measured the orientation of the glenoid bone defect line according to each circle (Figure 1C). Additionally, the location of the defect center was measured for each circle (Figure 1D). The extent of the defect was quantified by the angle between the superior and inferior margins.
We assessed the differences in measurements between the 2 circles. We also investigated the effects of size of the glenoid bone defect on its orientation and location. For calculating defect size, we used the Sugaya method.7,23 Additionally, because the best fit circle differs from the outer circle in both center position (using x and y coordinates, with the y-axis defined as the glenoid axis of the outer circle and the center of the outer circle set as the origin [0, 0]) and radius size, 5 we also examined the influence of these variations on measurement discrepancies.
To enhance reliability, all measurements were automatically calculated using Python and its related libraries after manually annotating the minimal required landmarks. These landmarks included the superior tubercle, the most inferior point of the glenoid, the glenoid margin for the best fit circle, and the superior and inferior margins of the defect.
Statistical Analysis
All statistical analyses were performed using R statistical software (R Foundation for Statistical Computing) and Python. The paired t test was used to compare the mean values of measurements between the 2 circles, including the extent of the bone defect, the center, and the superior and inferior margins. The Wilcoxon signed-rank test was utilized for comparing the orientations of glenoid defects. Spearman rank correlation coefficient was used to analyze factors associated with measurements and measurement discrepancies, including the position and radius of the best fit circle, as well as the size of the glenoid defect.
Results
Of the 312 patients with recurrent shoulder instability who underwent 3D CT scans, 229 patients with 231 shoulders were included. Of these, 27 patients >40 years of age, 24 with a previous surgical history, 31 with no bone defects, and 1 with a glenoid deformity were excluded. Of the included patients, 221 were male and 8 were female. Their mean age was 23.9 ± 5.9 years. The mean size of the glenoid defect based on best fit circles was 14.0% ± 7.1% (4.0 ± 2.2 mm). The mean position of the best fit circle's center relative to the outer circle's center was 0.3 ± 1 mm on the x-axis and −4.2 ± 0.9 mm on the y-axis. Intra- and interobserver reliabilities for measurements were good to excellent, with ICCs ranging from 0.776 to 0.906 (Appendix Tables A1 and A2).
The results of the measurements are presented in Figure 2 and Table 1. Each outer circle method and best fit circle method measurement was significantly different.

Summary of results. (A) The mean orientation of the defect line and the locations of the superior and inferior defect margins. (B) The defect line orientation did not exhibit an association with defect size, suggesting that the defect may expand while maintaining its original angle.
Results of Measurements a

Max, maximum; Min, minimum.
Regarding defect size and its effects on each method's measurement, defect size was associated with the location of the defect's center and its superior and inferior margins in both outer circle and best fit circle methods (Figure 3, Table 2). In particular, the location of the defect center was inversely related to the defect size in the best fit circle method, contrary to the outer circle method. The orientation of the linear defect and the defect size did not show a significant correlation in both circle methods.

Orientation and locations related to glenoid bone defect. The graph illustrates that the orientation of the defect line does not correlate with defect size. It also reveals that positions of the inferior margin of the defect measured from the outer circle are less likely to extend beyond the 6-o’clock position due to the definition of the measurement.
Orientation and Locations Related to Glenoid Bone Defect Based on Each Circle Method and Spearman Rho a

NS, not significant.
P < .001.
P = .037.
In terms of various factors and their influence on each method's measurement discrepancy, defect size did not show an association with the orientation discrepancies of the linear defect measured by the 2 methods. These orientation discrepancies of the linear defect remained consistent regardless of defect size. In contrast, discrepancies of location identified by the best fit circle and outer circle methods varied with the defect size (Table 3, Appendix Figure A1). Both the radius of the best fit circle and the coordinates of its center were related to discrepancies of measurements between the 2 circles. Notably, the orientation of the linear defect was strongly related to the x coordinate, indicating the best fit circle's anterior or posterior positioning relative to the glenoid axis (Appendix Figure A2).
Correlating Factors of Measurement Discrepancy and Spearman Rho

Position (x) and measurement discrepancy of the defect center yielded a P value of .006. All other values yielded a P value < .001. The terms “position (x)” and “position (y)” refer to the coordinates of the center of the best fit circle, with (0, 0) representing the center of the outer circle. NS, not significant.
Discussion
The primary finding of this study was that measurements between the outer circle and best fit circle were statistically different in annotating the orientation of the glenoid bone defect line and center and the location and extent of the defect. This supports our hypothesis. However, in most cases, the discrepancies amounted to <1.5 hours. These discrepancies are contingent on the position and radius of the best fit circle as well as the size of the glenoid defect. The orientation of the linear defect did not demonstrate an association with defect size; this may have implications that the defect expands while maintaining its original angle.
Clinicians commonly use a clockface model to locate glenoid lesions. As the best fit circle gains popularity, different clinicians are using clocks with different reference points, best fit or the outer circle clocks. Often, there is no clear communication about which method was used, leading to errors and discrepancies. In addition to clinical applications, laboratory studies also utilize either the outer or best fit circles to mimic bone defects.2,9,20,27 Determining the compatibility of these methods is crucial to prevent misunderstanding in the clinic and the laboratory. If the methods are compatible, no change to the current reporting methods is necessary. The need to investigate these compatibility issues and the insufficient understanding of defect locations based on the best fit circle method were the primary motivations for this study.
According to a systematic review by Gottschalk et al, 8 the investigation of defect location has been limited; only 2 significant studies by Saito et al 21 and Ji et al 12 have been conducted. While both studies utilized the outer circle as a reference, their methodologies for determining the location of the glenoid bone defect varied. Saito et al directly measured the defect's orientation using 3D CT scans, but Ji et al inferred the defect location by comparing the morphology of shoulders with recurrent instability to that of cadaveric shoulders. Although Ji's method could potentially be refined using the contralateral glenoid as a template, we opted for Saito's approach due to its robust study design. This approach has also been utilized as a benchmark for posterior bone defect location in the research conducted by Dekker et al. 6
This research had 2 key methodological distinctions from that of Saito et al, 21 in addition to the use of the best fit circle. First, we selected the most inferior point of the glenoid as the reference for 6 o'clock, rather than the infraglenoid tubercle, due to its anatomic precision. The infraglenoid tubercle often presents as an area with anatomic variation rather than a distinct point, and its identification can be obscured when bony defects extend to the inferior glenoid.10,15 However, the most inferior point approach, while reliable, inherently restricts defect measurement to a maximum of 6 o'clock. Given these constraints, the best fit circle offers an alternative, especially when addressing defects located inferiorly.
The second methodological variation is the orientation of the defect. Saito et al 21 differentiated between the location and orientation of the glenoid defect. That research group defined location by the angular positions of the superior and inferior margins and orientation by the angle between the glenoid axis and the defect line. In practical and surgical contexts, angular positions on a clockface typically signify a point rather than a line. To align with this, we incorporated the center point of the defect, enhancing the practicality of our measurements.
Although the location of the defect's center changed with the size of the defect, the orientation of the linear defect remained consistent regardless of defect size. While this study does not track individual events of recurrent shoulder dislocation over time, the consistent orientation of linear defects may imply that, during episodes of recurrent shoulder instability, the defect's orientation remains unchanged. This may suggest that the defect maintains its original angle during expansion. This theory aligns with the findings of Saito et al 21 of a primarily anterior distribution of linear defects. This consistent orientation of the linear defect may have surgical implications, particularly in bony procedures for anterior shoulder instability, such as the bone block procedure or Latarjet procedure. These surgeries aim to restore anterior glenoid bone loss, and accurate positioning of the bone graft is critical for successful restoration.17,28 Surgeons often describe graft positions using a clockface reference, but obtaining a clear view of the glenoid and its axis to determine this position can be challenging. In such cases, identifying the linear defect intraoperatively and aligning the graft with its preserved orientation may help better replicate the original trajectory of glenoid bone loss, owing to the consistent directional pattern observed.
All other measurements that showed statistically significant differences between the 2 circles share a common factor: these measurements are influenced by the position of the best fit circle. Because all circles are mathematically similar, differences resulting from each circle method are naturally linked to their placement and size. On average, the center of the best fit circle was positioned anterior and inferior to the center of the outer circle, and the observed differences increased with more anterior and inferior best fit circle positioning. Therefore, when the center of the best fit circle is anterior and inferior to the glenoid axis, noting discrepancies in orientation is important.
Although statistical differences in measurements between the circles were noted, the defect was predominantly oriented anteriorly regardless of observation method, best fit circle or outer circle. However, several studies continue to describe anterior instability as anteroinferior instability.4,14,16 If it were to be classified as anteroinferior instability based on the glenoid axis, sometimes it should instead be termed anterosuperior instability; although rare, it occurs when the linear or pointed orientation of the defect tilts slightly upward.
Except for the center and superior margin of the bone defect, the mean differences in measurements were less than one-half hour. This variance may explain the lack of research into these differences. In most cases, the measurement differences were <1.5 hours. This may lead users of either the best fit circle or the outer circle to believe the same point is being targeted. However, the compatibility of these customary practices has not been definitively proven. Considering the growing use of the best fit circle in cases of anterior shoulder instability, caution is needed when interpreting findings across studies or in surgical communication, as reference points or clockface systems may differ between them. This study may serve as a reference for future research.
Hurley et al 11 reported that 89% of 65 experts from 14 countries recommended that the lowest anchor in Bankart repair should be placed at a position of 5:30 to 6:00. However, the study did not specify which clock reference was used. Despite the biomechanical advantages of a 6-o’clock anchor, 3 the consistency of using this position across the varying extents of Bankart lesions should be a concern. Our findings show that the inferior margin of the bony defect is typically around 4:30, suggesting that an anchor placement at 5:30 to 6:00 would require extending beyond the defect by >1 hour. Additionally, labral release often extends an additional hour beyond the anchor placement. 19 These findings raise questions about the precision and consistency of the 6-o’clock position as recommended by experts, given the variability in lesion locations and error in surgeons’ recognition of these sites.18,24 These discrepancies can partly be explained by differences in the use of clock references. Clinically, preoperative planning and postoperative evaluation are often based on an outer circle clock reference derived from the bony morphology of the glenoid. However, during surgery, the glenoid rim is covered by the labrum, with its superior part (12 o’clock) being the thickest. 1 This creates a more circular appearance compared with the bony morphology, which can influence the surgeon's clock-based perception of the glenoid. Fortunately, the linear bone defect revealed after releasing the Bankart lesion is consistently observable both in radiological imaging and in the surgical field. Therefore, utilizing the linear bone defect location on CT scans could serve as a reliable anatomic landmark in the operative field, providing a stable orientation regardless of defect size.
Limitations
This study has several limitations. First, the association between defect size and the orientation of the defect line was analyzed using cross-sectional data, not through sequential observations. Second, there is no established benchmark for determining the extent to which the measurement error differences affect clinical outcomes. Third, like previous studies on the location of bone defects, this study did not examine the relevance of these findings to clinical outcomes. Fourth, this study has clear limitations in terms of direct clinical application. In Bankart repair, anchor placement is determined primarily by intraoperative findings rather than the preoperative orientation of the glenoid defect. Therefore, the consistent orientation of the defect line, regardless of defect size, may have limited influence on actual anchor positioning. Nonetheless, its clinical value may lie in improving the accuracy of communication and documentation of anchor location, using the glenoid defect as a more reproducible intraoperative or radiological reference. Furthermore, given the lack of standardization in using outer versus best fit circles across previous studies, our findings may help promote clearer and more consistent communication in both academic and surgical settings.
Conclusion
The defect locations of the outer circle and best fit circle differed statistically. Although the mean difference was <1 hour, caution is needed when interpreting findings across studies or in surgical communication, as reference clockface systems may differ between them. Among these locations, the orientation of the defect line appears stable with respect to defect size in each circle, suggesting that the defect may serve as a reliable reference for describing anchor or bone block placement during surgery.
Footnotes
Appendix
Interobserver ICC
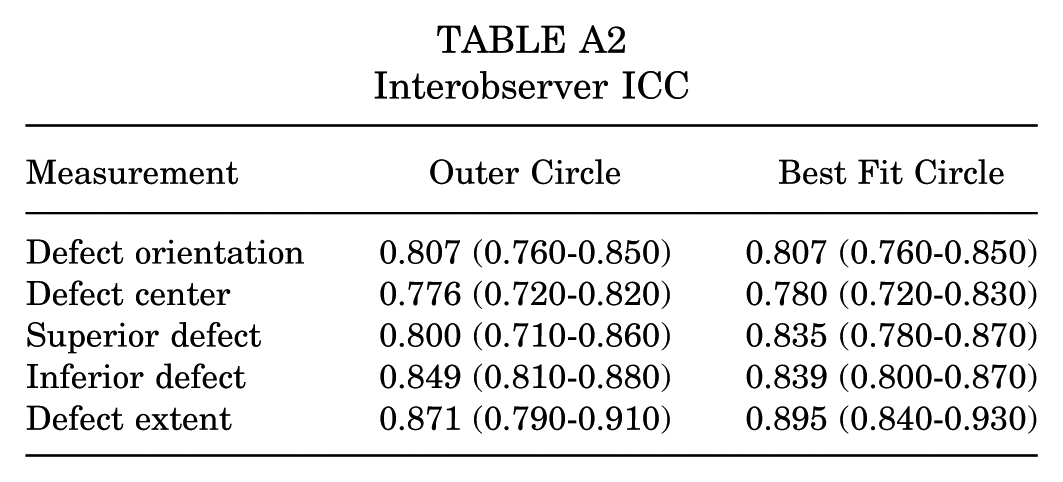
| Measurement | Outer Circle | Best Fit Circle |
|---|---|---|
| Defect orientation | 0.807 (0.760-0.850) | 0.807 (0.760-0.850) |
| Defect center | 0.776 (0.720-0.820) | 0.780 (0.720-0.830) |
| Superior defect | 0.800 (0.710-0.860) | 0.835 (0.780-0.870) |
| Inferior defect | 0.849 (0.810-0.880) | 0.839 (0.800-0.870) |
| Defect extent | 0.871 (0.790-0.910) | 0.895 (0.840-0.930) |
Acknowledgements
The authors thank C.K. Lee for the essential illustration.
Final revision submitted July 17, 2025; accepted August 1, 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Severance Hospital.