
Abstract
Background:
Recurrent anterior shoulder instability is frequently associated with Hill-Sachs and Bankart lesions, which compromise joint stability. While arthroscopic Bankart repair remains a widely accepted treatment for anterior shoulder instability, combining it with remplissage, with or without anterior subscapularis augmentation (ASA), has been proposed to enhance outcomes in these cases.
Purpose:
To compare the clinical and functional outcomes of arthroscopic Bankart repair with remplissage, with or without ASA, in patients with recurrent anterior shoulder instability and subcritical glenoid bone loss (GBL) (<15%).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This retrospective cohort study analyzed 56 patients with recurrent anterior shoulder instability who underwent surgery at a single tertiary university hospital between 2018 and 2022. Patients were grouped into 2 categories based on the surgical approach: Bankart repair with remplissage (group A) and Bankart repair with both remplissage and ASA (group B). Functional outcomes were evaluated using the Rowe score and the modified Constant-Murley (CM) score, while external rotation (ER) deficits were measured in adduction (ER1) and at 90° abduction (ER2). In addition, recurrence rates and postoperative clinical scores were systematically analyzed to assess the efficacy of these techniques.
Results:
The recurrence rates were 5.1% in group A and 0% in group B. Both groups demonstrated significant postoperative improvements in clinical outcomes. In group A, the mean Rowe score improved from 37.8 ± 4.5 to 93.1 ± 5.3 and the CM score from 69.8 ± 7.2 to 96.5 ± 2.5 (P < .0001). In group B, the Rowe score increased from 37.5 ± 6.4 to 94.7 ± 1.2 and the CM score from 71.2 ± 8.3 to 95.4 ± 0.9 (P < .0001). No statistically significant differences were observed between groups in postoperative Rowe (P = .23) or CM scores (P = .08). However, when postoperative range of motion was analyzed, the addition of ASA was associated with greater ER deficits compared with remplissage, both in ER1 (−12.5°± 9.19° vs −18.33°± 2.46°; P = .013) and ER2 (−14.2°± 7.67° vs −18.83°± 1.94°; P = .017).
Conclusion:
This study demonstrates that adding ASA to arthroscopic Bankart repair with remplissage significantly reduces ER while maintaining excellent clinical outcomes and low recurrence rates. The combination of these techniques provides a viable option for managing recurrent anterior instability, particularly in cases with poor tissue quality and GBL <15%.
Keywords
The estimated incidence rate of shoulder dislocations in the United States is 23.9 per 100,000 person-years. 20 Recurrent shoulder dislocations are associated with a higher prevalence of Hill-Sachs and Bankart lesions. Hill-Sachs lesions occur in approximately 71% of first-time dislocations (range, 58%-83%) but rise to nearly 85% in recurrent cases (range, 70%-95%). Although Bankart lesions are reported in almost 100% of cases in many arthroscopic studies, meta-analysis demonstrates substantial heterogeneity, with reported prevalences of 59% in first-time and 66% in recurrent anterior shoulder dislocations. 15
Arthroscopic Bankart repair has demonstrated significantly lower rates of total recurrent instability (9.7%) compared with nonoperative treatment (67.4%). 4 The combination of arthroscopic Bankart repair and remplissage has demonstrated superior outcomes, including lower rates of recurrent shoulder instability, higher rates of return to sports, and comparable final follow-up range of motion (ROM) when compared with Bankart repair alone.3,7,8,16
Managing shoulder instability with poor anterior soft tissue quality is particularly challenging, as intraoperative findings may reveal a thinned or attenuated labrum and/or degenerative changes of the anterior capsule, which can compromise fixation strength and healing after standard arthroscopic Bankart repair. The arthroscopic subscapularis augmentation (ASA) using the subscapularis tendon is a valuable method for reinforcing the anterior capsulolabral complex. It may be used as an adjunct to arthroscopic Bankart repair and remplissage, even in cases with anterior glenoid bone loss (GBL).9,10,13,16 The ASA procedure has a stabilizing effect during external rotation (ER) and abduction, with some trade-offs, including a reduction in maximum ER.
The primary objective is to compare postoperative shoulder stability, measured by dislocation events, between patients treated with remplissage alone and those treated with remplissage combined with ASA. The secondary objectives were to assess differences in functional outcomes—Rowe and modified Constant-Murley scores (CM)—and ROM, particularly ER deficits in adduction (ER1) and at 90° abduction (ER2).
It was hypothesized that adding ASA to Bankart repair with remplissage would improve shoulder stability and reduce recurrence rates compared with remplissage alone, at the cost of greater loss of ER.
Methods
This study was designed as a retrospective cohort analysis conducted at a single tertiary care university hospital. A total of 56 patients with recurrent anterior shoulder instability and GBL <15% who underwent arthroscopic Bankart repair with remplissage or arthroscopic Bankart repair combined with ASA and remplissage between January 2018 and January 2022 were included.
Inclusion Criteria
Patients with a history of traumatic recurrent anterior shoulder instability were eligible if they presented with a glenoid bone defect of less <15%, as confirmed by computed tomography (CT), and off-track Hill-Sachs lesions. Additionally, patients had to complete a standard rehabilitation program and have a minimum of 2 years of follow-up. Patients were excluded if they had nonanterior shoulder dislocations, habitual dislocations, multidirectional instability, or rotator cuff injuries. Further exclusion criteria included GBL exceeding 15%, humeral avulsion of the glenohumeral ligament (HAGL) or reverse HAGL lesions, epilepsy or psychiatric disorders requiring treatment, and revision cases of Bankart repair with or without remplissage.
Preoperative Evaluation
Each patient underwent a thorough physical examination by a senior shoulder surgeon (M.H.), with functional assessments recorded using the Rowe and modified CM scores. CT imaging with 3-dimensional reconstruction was used to evaluate glenoid bone defects, using either the best-fit circle method or the en face view, as described by Sugaya. 17 The on-track or off-track status of Hill-Sachs lesions was assessed using the Yamamoto criteria. 19 Patients with off-track lesions were included in the study and treated with either Bankart repair and remplissage or Bankart repair, remplissage plus ASA. The ASA technique was performed selectively for patients in whom intraoperative assessment revealed poor anterior capsulolabral tissue quality, such as a thinned or attenuated labrum or degenerative changes of the anterior capsule.
Surgical Technique
All surgeries were conducted by a senior surgeon under general anesthesia, a scalene block, or both. All patients were positioned in the sloppy lateral decubitus position with the arm in approximately 30° of abduction, 20° of forward flexion, and neutral rotation, maintained under 3 kg of balanced traction to allow optimal visualization of both the anterior and posterior aspects of the glenohumeral joint.
After sterile preparation, diagnostic arthroscopy was initiated via a posterior portal, and the labral lesion, glenoid bone defect, and Hill-Sachs lesion were assessed.
For the remplissage procedure, a posterolateral portal was established under needle guidance for proper placement over the Hill-Sachs lesion. The lesion surface was prepared with a rasp and bur, and 1 or 2 double-loaded 3.5-mm anchors with nonabsorbable sutures were inserted at the lesion's medial margin. Suture passage through the infraspinatus tendon was performed with the arm maintained in a neutral rotation position. Using a bird-beak passer, the sutures were placed through the central to the inferior fibers of the infraspinatus. The knots were tied after completion of the labral repair, with the arm kept in the same neutral position.
Bankart repairs involved mobilizing the labrum and preparing the glenoid margin. Bioabsorbable or PEEK double-loaded anchors with nonabsorbable sutures (range, 3-5) were inserted based on the extent of the lesion. In cases requiring ASA, one of the anchors was utilized for subscapularis tenodesis. For the ASA technique, the sutures were passed through the upper third of the subscapularis tendon together with the remnant anterior capsule and labrum using a Spectrum suture passer. The arm was held in the same neutral rotation under the same traction during both suture passage and knot tying.
Postoperative Rehabilitation
Postoperatively, the shoulder was immobilized in a sling for 3 weeks, with passive mobilization initiated on the first day. ER was initially limited to approximately 20° to 30° at the side for the first 6 weeks. Active mobilization began at 4 weeks and continued for 12 weeks. Resistance band exercises were introduced at 13 weeks, with terminal stretching added by 16 weeks. Patients were allowed to return to sports between 8 and 10 months, contingent on achieving a satisfactory ROM and shoulder strength, as confirmed by the therapist.
Follow-up and Outcome Measures
Patients were evaluated at 3, 6, and 12 weeks postoperatively, followed by assessments at 6 and 12 months and annually thereafter. Although ROM was monitored at each follow-up visit, only the final follow-up measurements were included in the statistical analysis. Functional outcomes were assessed at a minimum of 2 years postoperatively using the modified CM score and the Rowe score. Magnetic resonance imaging scans were performed to verify remplissage integrity.
ROM was measured using a goniometer to assess ER at the side (ER1) and in 90° abduction (ER2) for both shoulders. Treatment failure was defined as any episode of redislocation or subluxation. Participation in specific sports was not systematically recorded.
Patients were categorized into 2 groups for functional outcome analysis:
Group A: Bankart repair with remplissage.
Group B: Bankart repair with remplissage and ASA.
Statistical Analysis
In this study, descriptive statistics were used to summarize patient characteristics and recurrence rates; the Shapiro-Wilk test assessed data normality; paired t tests evaluated pre- and postoperative changes within groups; independent t tests compared continuous variables between groups; and the Fisher exact test compared recurrence rates. Statistical significance was set at P < .05.
A power analysis was not performed. Statistical analyses were conducted using SPSS Statistics Version 25 (IBM Corp).
Results
A total of 56 patients were included in the analysis: 39 in group A (Bankart repair with remplissage) and 17 in group B (Bankart repair with remplissage plus ASA). The mean follow-up duration was 50.8 ± 22.1 months in group A and 49.5 ± 13.3 months in group B, with no significant difference between groups (P = .82).
Significant differences were observed between groups with respect to the number of dislocations before surgery, which was higher in group B (5.7 ± 2.3) compared with group A (3.9 ± 2) (P = .004), and the number of anchors used for Bankart repair, which was greater in group B (4.1 ± 0.3) than in group A (3.2 ± 0.4) (P = .0001). No significant differences were found for any other surgical or demographic variables—including the number of anchors used for the remplissage procedure (P = .26).
Baseline demographic characteristics were comparable between groups—including age, sex distribution, laterality, dominant side involvement, and mean GBL (group A: 10.5% ± 3% vs group B: 11.3 ± 2.2%; P = .54). None of the patients were high-level athletes, and most reported only recreational gym-based weight training (Table 1).
Descriptive and Surgical Data of Patients in the 2 Groups a

Data are presented as mean ± SD. Bold P values indicate statistical significance. ASA, anterior subscapularis augmentation; GBL, glenoid bone loss.
The recurrence rate was 5.1% (2/39) in group A and 0% (0/17) in group B (2-sided ≥.999). In group A, 1 patient experienced a dislocation at 16 months after a fall during a football (soccer) game and subsequently had 10 additional dislocations. The other patient in Group A had a dislocation during weightlifting 6 years after the procedure; no further dislocations occurred thereafter.
Both surgical techniques demonstrated a statistically significant improvement in clinical scores (Table 2). Comparison of functional outcomes showed no significant differences in the Rowe scores between the 2 groups (P = .23). Similarly, no significant difference was observed in the Constant score (P = .08).
Functional Outcomes Pre- and Postoperatively in the 2 Groups a
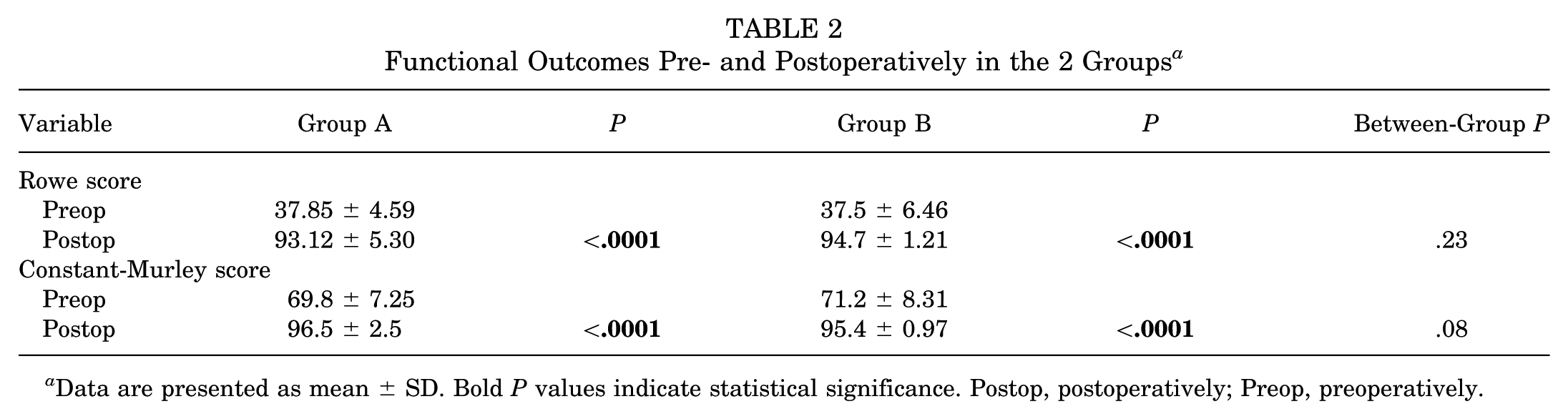
Data are presented as mean ± SD. Bold P values indicate statistical significance. Postop, postoperatively; Preop, preoperatively.
When comparing the groups regarding loss of ER, the addition of the ASA technique significantly affected motion. The mean ER1 was −12.5°± 9.19° in group A and −18.33°± 2.46° in group B (P = .013), while the mean ER2 was −14.2°± 7.67° versus −18.83°± 1.94°, respectively (P = .017) (Table 3).
Pre- and Postoperative External Rotation ER1 and ER2 in the 2 Groups a
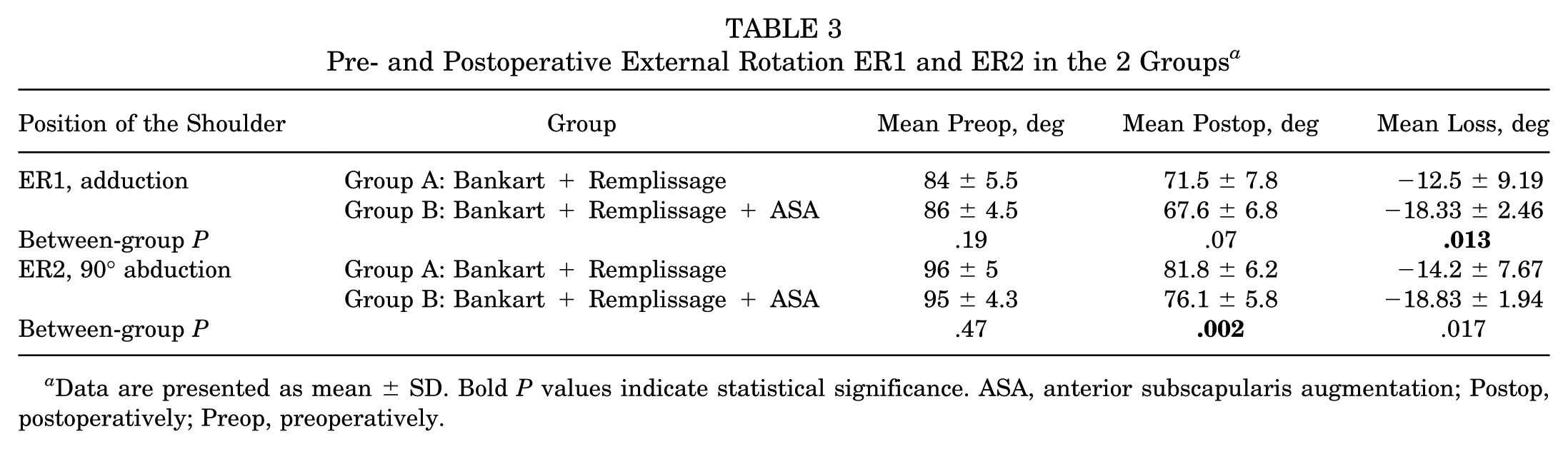
Data are presented as mean ± SD. Bold P values indicate statistical significance. ASA, anterior subscapularis augmentation; Postop, postoperatively; Preop, preoperatively.
Discussion
The primary finding of this study is that both surgical techniques—Bankart repair with remplissage and Bankart repair with remplissage plus ASA—achieved excellent outcomes for shoulder stability, with very low recurrence rates (5.1% and 0%, respectively). A secondary but clinically relevant outcome was that the addition of ASA, although providing comparable functional scores, was associated with greater ER deficits than remplissage alone. This highlights the trade-off between maximizing joint stability and preserving ROM, an important consideration for surgical decision-making.
Maiotti et al 10 have highlighted the efficacy of augmenting Bankart repair with remplissage using the ASA technique in achieving joint stability. This approach has been shown to produce clinical outcomes comparable to those of the Latarjet procedure in patients with recurrent anterior shoulder dislocations, particularly those with GBL <15% and an Instability Severity Index (ISI) score >3. In our study, the redislocation rate was 5.1% in the remplissage group and 0% in the ASA group, which closely mirrors the outcomes reported in their research for the remplissage group. Specifically, their study noted a redislocation rate of 6.1% in the remplissage cohort and 7% in the ASA group. Another study by Maiotti et al 11 suggests that arthroscopic Bankart repair plus ASA may be a viable surgical option for managing anterior shoulder instability in athletes participating in collision and contact sports. In their study, the dislocation rates after this procedure were 1.6% for atraumatic redislocations and 2.2% for posttraumatic redislocations at final follow-up. The mean functional deficit in ER was reported as 15°, with the arm in ER1 position and 10° in ER2 position. In comparison, our patients exhibited a slightly greater deficit, with mean ER1 and ER2 deficits of 18.33° and 18.83°, respectively.
Our findings are comparable to those of Brilakis et al, 1 who reported a 5.8% recurrence rate and significant functional improvement after ASA combined with classic Bankart repair without remplissage, with only minimal impact on return to sports despite some ER loss. In our series, ASA likewise provided excellent stability (0% recurrence) but was associated with an ER deficit when combined with remplissage. The excellent postoperative stability observed in the ASA group is particularly noteworthy, given that these patients presented with a greater number of preoperative dislocations (5.7 ± 2.3 vs 3.9 ± 2; P = .004) and poorer capsulolabral tissue quality, both factors typically associated with a higher recurrence risk. The postoperative improvements in functional outcomes were clinically meaningful, as the mean increases in Rowe and modified CM scores far exceeded the reported minimal clinically important difference values—9.7 points for the Rowe score and 12 and 10.4 points for the CM score established for rotator cuff repair.6,12 These findings indicate that the observed postoperative gains were not only statistically significant but also clinically important and that the addition of ASA may help offset the negative prognostic effect of advanced soft-tissue damage and recurrent instability.
In the present study, the indication for performing ASA was determined intraoperatively based on the surgeon's assessment of anterior capsulolabral tissue quality. ASA was added when the labrum appeared thinned, frayed, or degenerative, or when the anterior capsule demonstrated poor resistance to traction or suture passage. This selective approach aligns with published indications, where ASA is recommended for patients with recurrent anterior instability and compromised soft-tissue integrity or subcritical GBL up to 23%, as reported by Russo et al. 14 Although patient factors such as younger age, higher activity level, and a greater number of previous dislocations were considered, the final decision was guided primarily by intraoperative findings of poor tissue quality rather than preoperative imaging or demographic variables.
Hurley et al 5 reported a recurrence rate of 3.2% for arthroscopic Bankart repair combined with remplissage. In our cohort, the recurrence rate for this procedure was 5.1%, which is slightly higher than their findings. Although Buza et al, 2 in their analysis of 6 studies involving 167 patients who underwent arthroscopic Bankart repair plus remplissage, reported a recurrence rate of 5.4%. Buza et al 2 reported that the combination of Bankart repair and remplissage results in a mean loss of 2.6° of ER. In contrast, in our study, the deficit was greater at 12.5°. Villareal-Espinosa et al 18 highlighted that the Bankart repair alone is associated with a significantly higher risk of recurrent dislocation, with an odds ratio of 4.22 compared with the combined Bankart repair and remplissage procedure.
An additional consideration concerns the role of ASA in patients with poor tissue quality. In such cases, Bankart repair combined with remplissage and ASA may offer a valuable option for reinforcing the anterior capsulolabral complex, thereby enhancing stability even in the presence of compromised soft tissues. The trade-off, however, is a loss of ER, which, while generally well tolerated, may predispose to degenerative changes or arthritis in the long term. In addition, ER deficits may have functional consequences for overhead athletes, in whom even small losses in motion can affect performance. Our study, with its relatively short follow-up period, cannot address this concern. Therefore, the decision to incorporate ASA should be individualized, taking into account tissue quality, bone defects, and patient-specific functional demands, with the understanding that the surgeon must balance stability against the risk of ROM deficit.
Historical open stabilization procedures involving subscapularis shortening or tenodesis, such as the Putti-Platt procedure, achieved satisfactory short-term stability but demonstrated concerning long-term outcomes. In one series performed between 1964 and 1974, with a mean follow-up of 27.1 years, moderate to severe glenohumeral arthrosis developed in 5 of the 20 evaluated shoulders, with 2 progressing to advanced degenerative changes. 21 These findings illustrate that excessive anterior soft-tissue tensioning can predispose to degenerative joint disease over time, underscoring the need to balance stability with preservation of motion.
This study has several limitations. First, the retrospective design introduces potential biases—including variability in patient selection and follow-up assessments. Second, the study population was relatively small, particularly in the ASA groups, limiting the generalizability of the findings. Third, while a single experienced surgeon performed all procedures, the lack of blinding or randomization may have influenced outcomes. Fourth, none of the included patients were high-level athletes, which restricts the applicability of our findings to this subgroup. Fifth, the relatively short follow-up period does not allow conclusions regarding potential long-term complications.
Conclusion
This study demonstrates that adding ASA to arthroscopic Bankart repair with remplissage significantly reduces ER while maintaining excellent clinical outcomes and low recurrence rates. The combination of these techniques provides a viable option for managing recurrent anterior instability, particularly in cases with poor tissue quality and GBL <15%.
Footnotes
Final revision submitted December 24, 2025; accepted January 2, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: The research is conducted in the operating framework of the University of Thessaly Innovation, Technology Transfer Unit and Entrepreneurship Center “One Planet Thessaly”, under the “University of Thessaly Grants for Scientific Publication Support” action and is funded by the Special Account of Research Grants of the University of Thessaly. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Scientific Committee of the University General Hospital of Larissa (reference number: 2958).