
Abstract
Background:
Previous studies have focused on the effect of the peroneus longus tendon graft on the knee; in this study, we focused on its impact on the ankle. Injuries to the anterior cruciate ligament (ACL) are frequently observed in sports injuries. The peroneus longus tendon graft has rapidly gained a place in the literature; however, very few studies have been conducted on the foot-ankle region stability of this tendon.
Purpose:
To investigate the effect on this region of the peroneus longus tendon graft used in anterior cruciate ligament reconstruction (ACLR).
Study Design:
Case series, Level of evidence 4.
Methods:
The study included 20 out of 35 patients who met the inclusion criteria and had ACLR using a peroneus longus tendon graft at the same orthopaedics and traumatology clinic between January and December 2023.
The demographic characteristics of the patients were recorded. Ankle strength measurements were performed, and all the patients were tested with the Y test, the flamingo test, the eyes closed balance test, and the standing on tiptoes test. The Foot and Ankle Disability Index and the American Orthopedic Foot and Ankle Score were recorded.
Results:
The dynamometer measurements of the donor side and the contralateral side were compared. No statistically significant difference was determined between the 2 sides with respect to the ankle eversion and plantar flexion strength measurements (P = .096, P = .835, respectively). A significant result was obtained in the flamingo test (P = .049). No statistically significant difference was determined between the 2 sides with respect to the anterior, posterior, and lateral distances of the Y test (78.8 vs 78.6 cm, P = .973; 96.6 vs 80.4 cm, P = .053; 89.5 vs 95.0 cm, P = .357, respectively). In the examination of ankle functionality, no statistically significant difference was determined in the Foot and Ankle Disability Index and the American Orthopedic Foot and Ankle Score of the 2 sides (P = .798, P = .206, respectively).
Conclusion:
The peroneus longus tendon can be safely used as an alternative autograft in ACLR without causing donor site morbidity. There may be a deficit in balance test performance.
The anterior cruciate ligament (ACL) is one of the most frequently injured structures of the knee joint. 11 If ACL injuries are not treated surgically, they can lead to instability in the knee, meniscal injuries, and early osteoarthritic changes.8,9 The current gold standard treatment for ACL rupture in young, active patients is arthroscopic anatomic ACL reconstruction (ACLR). 3 However, graft selection remains a matter of debate. It is necessary to choose grafts that have similar biomechanics to the ACL, allow strong and safe fixation, support rapid biological integration, and cause minimal morbidity to the donor side. 15 Currently used autograft options include the hamstring tendon, bone-patellar tendon-bone, quadriceps tendon, peroneus longus, and the iliotibial band. The graft most often used in recent years is the hamstring tendon,17,18 which is also used in ACLR. Orthopaedic surgeons can use the peroneus longus tendon in deltoid ligament reconstruction and medial patellofemoral ligament reconstruction because there is a synergistic function between the peroneus longus and peroneus brevis muscles, which mitigates potential loss of strength and offers some advantage if both undergo tenodesis. The large graft diameter can be advantageous for revision surgery. Other advantages are that it does not cause pain in the knee and does not cause thigh muscle atrophy. The use of this tendon is contraindicated in patients with neurovascular deficits who have undergone foot/ankle surgery. In the search for the ideal autograft, the peroneus longus has emerged as a viable option; however, there are concerns that it may have an effect of instability in the ankle. 1 To reduce donor ankle morbidity to a minimum, some surgeons have recommended taking a partial graft (the anterior half of the tendon).4,16 To further reduce potential morbidity of donor ankle functions, routine tenodesis of the distal end of the peroneus longus to the peroneus brevis tendon has been strongly advocated.2,5
A gradual increase has been observed in the limited number of studies in the literature that have compared the peroneus longus tendon with the traditional hamstring autograft in primary ACLR. However, almost no studies have examined the effect of ankle instability when the peroneus longus is used for graft purposes.
The present study aimed to examine the clinical and functional effects of the use of the peroneus longus tendon as an autograft for ACLR on the ankle.
Methods
This retrospective cohort study included patients who underwent ACLR using the peroneus longus tendon graft between 2022 and 2023. Approval for this study was granted by the Suleyman Demirel University Health Sciences ethics committee (decision no. 26, dated 13.09.2024). Before the study, all the patients signed an informed consent form, prepared according to the standards of the clinical research ethics committee.
The patients included in the study were of both sexes, aged >18 years, with an isolated ACL injury who underwent primary anatomic ACLR using the peroneus longus tendon graft, and completed at least 1 year of follow-up. The study exclusion criteria were defined as multiple ligament injuries, a history of arthritis in the affected knee or ankle, the presence of pes planus valgus, or neuromuscular disorders with ankle deformity. Patients who could not be found in the follow-up system were also excluded. We preferred the peroneus longus tendon graft in these patients because it allows for quicker strengthening of the knee area in the postoperative period, has a larger graft diameter, and offers a smaller incision. The total number of patients operated on for the peroneus longus tendon graft was 35. A total of 20 patients who met the inclusion criteria were included in the study. The demographic and surgical data of the patients were obtained from the hospital records. The data were based on the findings from the presentation, intraoperative measurements, and follow-up examinations conducted at a minimum of 12 months postoperatively. During the follow-up, all the patients were examined clinically by a specialist surgeon (S.E.K.), and the data were carefully recorded. The ankle strength measurements of all the patients were measured with an analog hydraulic dynamometer. Balance tests—the eyes closed balance test, the standing on tiptoe test, and the flamingo test—were utilized (Figure 1). In the Y test, the foot extension distance was measured in lateral, anterior, and posterior directions (Figure 2). Ankle scoring was done according to the American Orthopaedic Foot and Ankle Society (AOFAS) and the Foot and Ankle Disability Index (FADI).
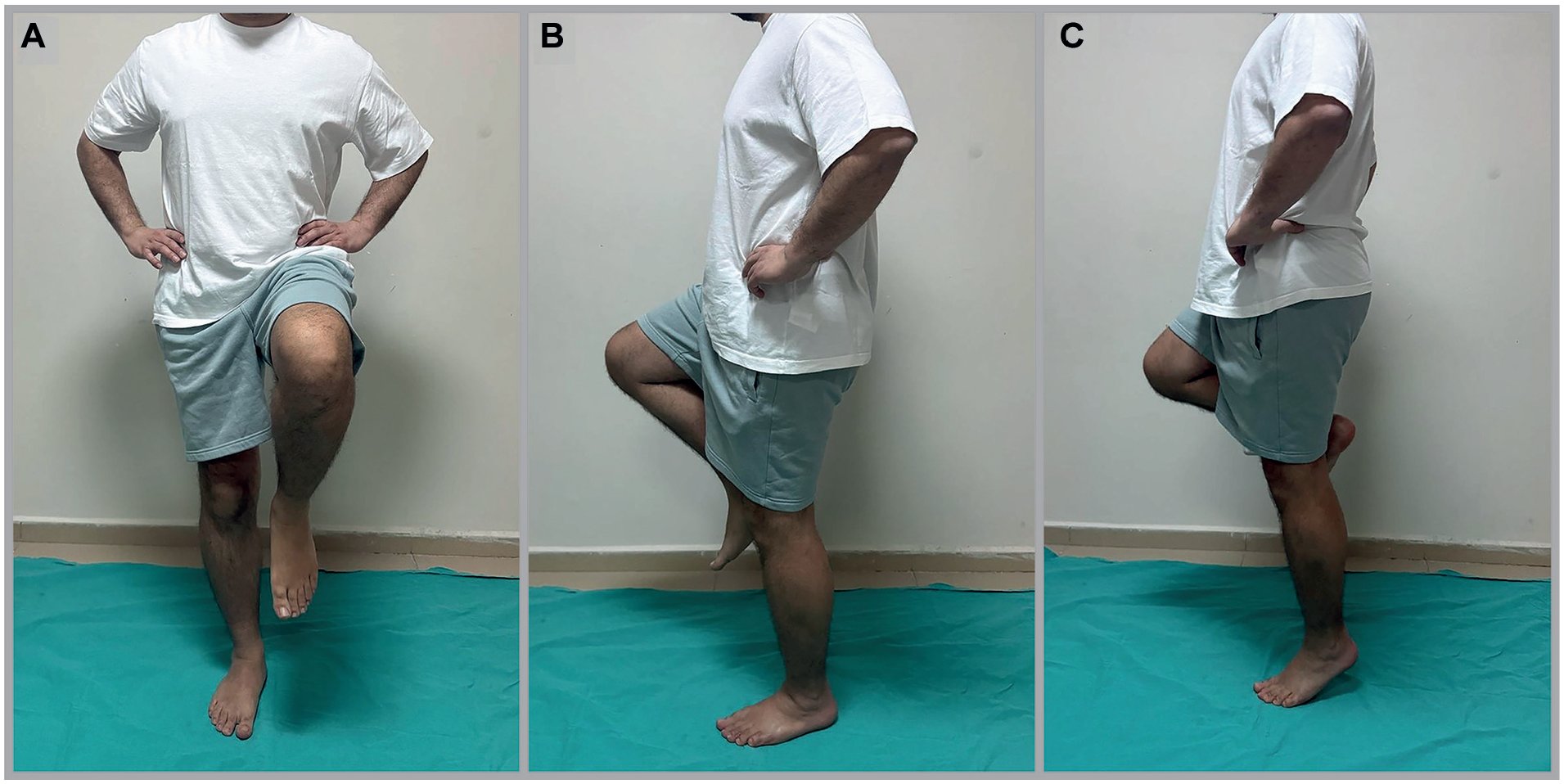
Balance tests. (A) Flamingo test. (B) Eyes closed balance test. (C) Standing on tiptoe test.
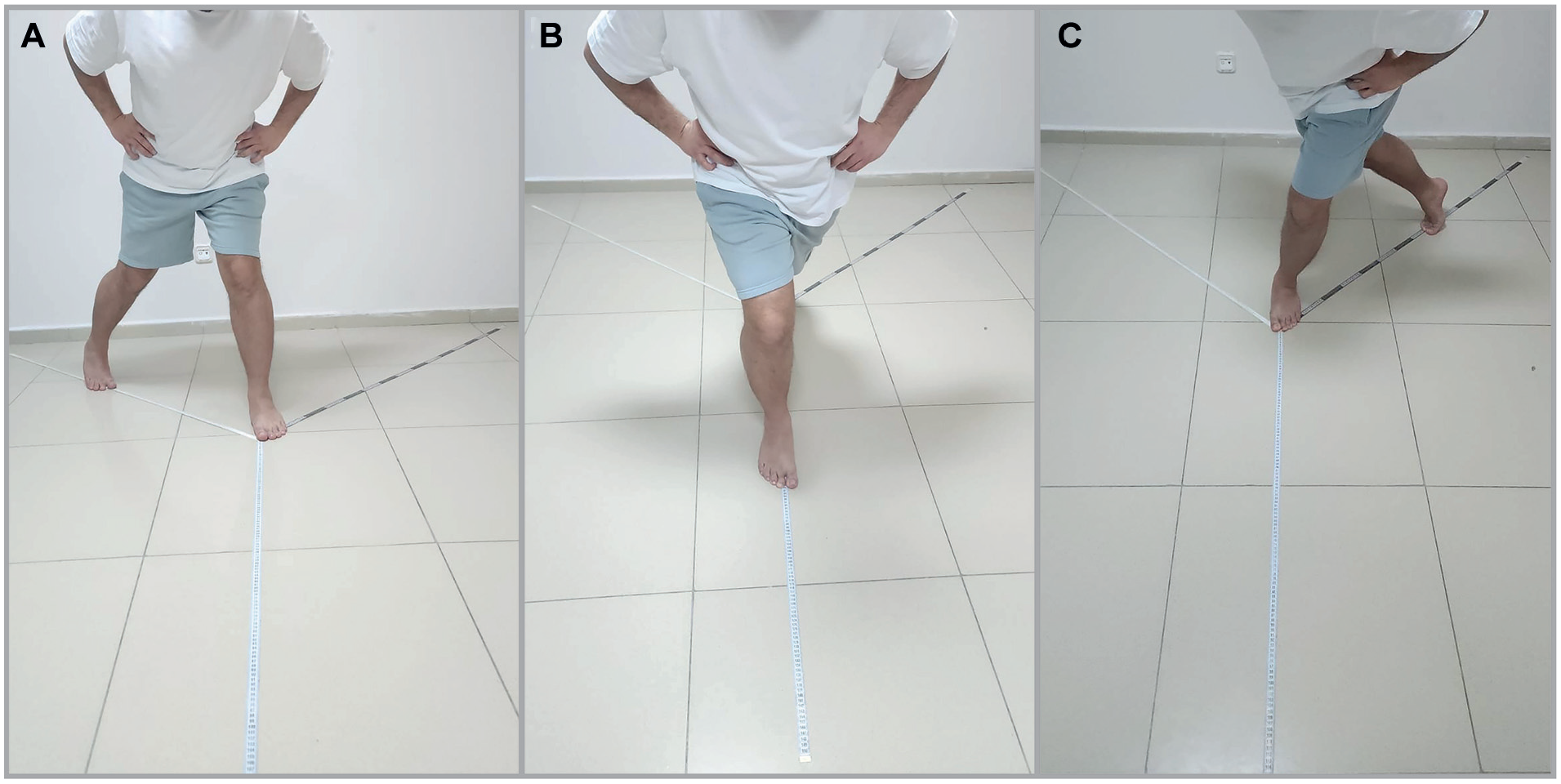
Y tests, foot extension distance. (A) Lateral. (B) Anterior. (C) Posterior.
Rehabilitation
Patients underwent an ACL rehabilitation program postoperatively. No special exercise program was applied for the foot/ankle. Patients were trained to exercise the injured leg using partial weightbearing until 3 weeks after surgery, after which they were allowed to use full weightbearing. Knee extension began immediately after surgery. Knee flexion was started from 0° to 90° (increased gradually) until 3 weeks after surgery, with subsequent full flexion. The patient was allowed to jog after 2 months. Patients were allowed to return to sports activities after passing functional outcome tests at 6 months. 13
Isokinetic Muscle Strength Test of the Ankle
The results of muscle strength tests were collected at 12 months after surgery. A Baseline analog hydraulic push-pull dynamometer was used on patients to measure isometric muscle strength. Examinations were conducted on bilateral angle eversion and first ray plantarflexion. Each muscle strength measurement was performed 3 times, and the mean strength value was recorded. The same operator (S.E.K.) conducted all muscle strength measurements to avoid any study bias.
Eversion was measured in the contralateral decubitus position. Patients were asked to make eversion movements of the ankle. The dynamometer was placed on the fifth metatarsal. The crural region of patients was gently pressed to minimize the movement of other muscles, and muscle strength was recorded from the dynamometer (Figure 3).
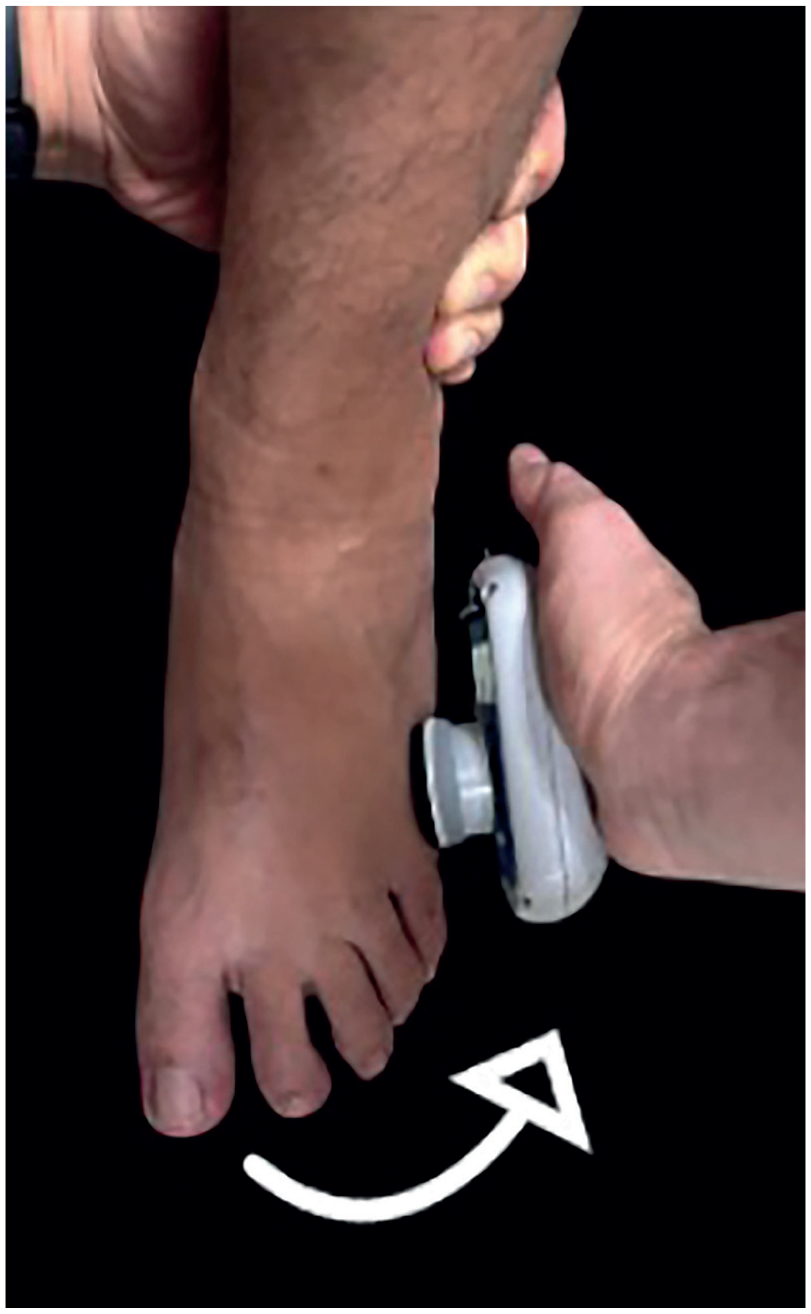
Eversion force measurement in the left ankle.
First ray plantarflexion was measured in the prone position. The ipsilateral knee joint was flexed 90°. The ipsilateral distal part of the crural region was maintained using the hands of the examiner's assistant to minimize the movement of other muscles. Patients were asked to make first ray plantarflexion movements. Muscle strength was recorded 13 from the dynamometer (Figure 4).

First ray plantarflexion force measurement in the left ankle.
Surgical Technique
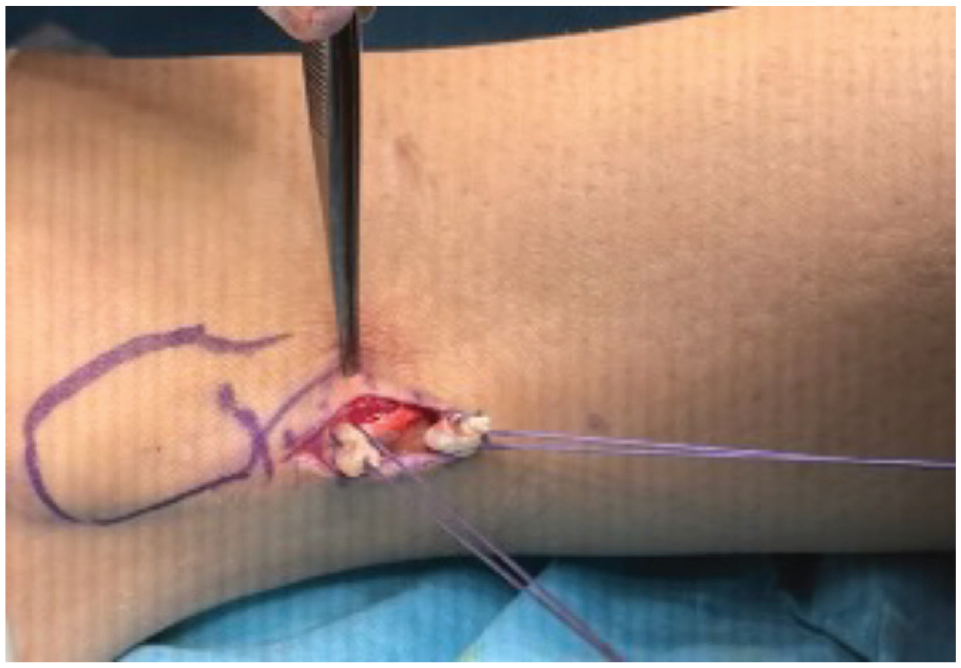
All the patients were operated on in elective conditions under spinal or general anaesthesia in a supine position with a tourniquet applied. Two specialist surgeons (S.E.K., R.D.) harvested all the grafts. For the peroneus longus tendon graft, the fibula was marked 2 cm proximal to the distal end. The incision line was defined to be approximately 2 cm and was over the tendon passing through the skin and subcutaneous tissue. The tendon fascia was opened, and then, using a clamp, the peroneus longus, which was more lateral and superficial, was raised. A primary suture (2 Vicryl sutures) (Ethicon) was applied to the distal part of the tendon, and the Krakow suture (2 Vicryl sutures) was used on the proximal part (Figure 5). We cut the peroneus longus tendon with a scalpel and divide it into 2 parts: proximal and distal. The distal part is sutured to the peroneus brevis tendon with 2 Vicryl sutures (Figure 6). By placing a finger 6 to 8 cm distal to the fibula head, it is ensured that the tendon stripper does not go further up, which is a method to prevent injury to the peroneal nerve (Figure 7). 10
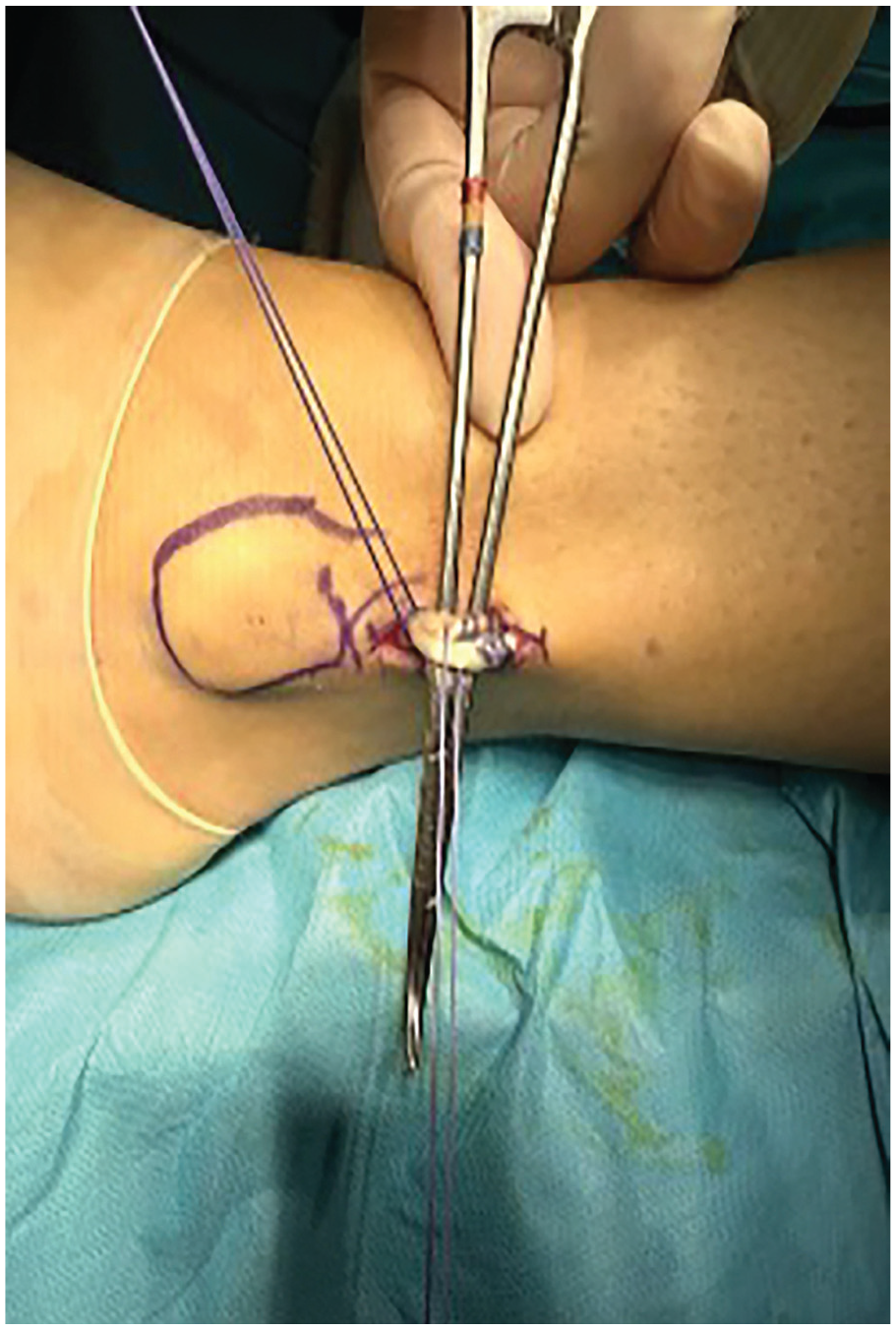
Isolation of the peroneus longus tendon for harvesting in the left ankle.
Isolation of the peroneus longus tendon (proximal and distal parts) for harvesting in the left ankle.

The peroneus longus tendon in the left ankle is stripped with a tendon stripper.
Statistical Evaluation
Data obtained in the study were analyzed statistically using Statistical Package for the Social Sciences for Windows Version 20.0 software (IBM). When comparing the data of groups separated according to the side of surgery, the median difference was examined with the Mann-Whitney U test. Conformity of the data to normal distribution was assessed with the Shapiro-Wilk test. Variables with a normal distribution were evaluated using the independent samples t test, and those not showing a normal distribution were evaluated using the Mann-Whitney U test. Statistical significance was set at P < .05. The power analysis of our study was performed, and according to the output of the G*Power program used for power analysis, when the effect size was taken as 0.8, the sample size was 20, and the power of the study was calculated as 0.80. This value demonstrates that our research is well-powered.
Results
Evaluations were done for 20 patients (18 men and 2 women), with a mean age of 28.72 ± 6.86 years (range, 18-45 years), and a mean follow-up period of 12.6 months (range, 12.5-16 months). The right knee was injured in 18 patients and the left knee in 2 patients. The mechanism of injury was a sports injury in 16 patients, a parachuting accident in 3 patients, and a traffic accident in 1 patient. The diameter of the peroneus longus tendon graft measured intraoperatively was recorded as a mean of 8.42 ± 0.82 mm (range, 7-10 mm). The length of the peroneus longus tendon graft measured intraoperatively was recorded as a mean of 24.6 cm (range, 23.8-26.4 cm) (Table 1). When evaluating ankle strength, the eversion and plantar flexion strength measurements were examined, as the peroneus longus tendon plays a particular role in these actions (Table 2).
Characteristics of the Patients and Grafts

Strength Measurements of the Ankle in Eversion and Plantar Flexion

The mean eversion strength was 85.10 ± 33.43 N on the donor side and 94.40 ± 24.69 N on the contralateral side. This difference was not statistically significant (P = .096).
The mean plantar flexion strength was 190.70 ± 31.67 N on the donor side and 187.62 ± 33.66 N on the contralateral side. This difference was not statistically significant (P = .835).
The balance test measurements were considered crucial for assessing the proprioception of the tendon graft in patients, and these measurements were taken and recorded in seconds (Table 3).
The Durations of the Balance Tests of the Patients a

The bold P value indicates statistical significance.
In the flamingo test, the mean times were 67.50 seconds on the donor side and 86 seconds on the contralateral side. This difference was statistically significant (P = .049).
In the eyes closed test, the mean times were 16.50 seconds on the donor side and 23.50 seconds on the contralateral side. This difference was not statistically significant (P = .325).
In the standing elevated on the tiptoes test, the mean times were 5.50 seconds on the donor side and 10 seconds on the contralateral side. This difference was not statistically significant (P = .111).
Although only the flamingo test showed a deficit, the measurements in the other tests are small and may be underpowered, which may represent a balance deficit.
The Y test was also regarded as important for proprioception. When performing this test, the patient stands with the 2 lower extremities in a Y shape, and while keeping one side fixed, the other side is moved forward, backward, and to the side. The maximum distance extended was also measured (in cm) (Table 4).
The Maximum Distances Extended by the Feet in Anterior, Posterior, and Lateral Positions in the Y Test

The mean anterior distance was 78.80 ± 11.52 cm on the donor side and 78.60 ± 13.96 cm on the contralateral side. This difference was not statistically significant (P = .973).
The mean posterior distances were 96.60 ± 16.14 cm on the donor side and 80.40 ± 16.09 cm on the contralateral side. This difference was not statistically significant (P = .53).
The mean lateral distances were 89.50 ± 11.84 cm on the donor side and 95 ± 14.07 cm on the contralateral side. This difference was not statistically significant (P = .357).
Functional scoring of the ankle was made according to the FADI and AOFAS scoring systems (Table 5).
FADI and AOFAS Scores a

AOFAS, American Orthopaedic Foot and Ankle Society; FADI, Foot and Ankle Disability Index.
The mean FADI scores were 98.76 ± 0.64 on the donor side and 98.96 ± 0.6 on the contralateral side. This difference was not statistically significant (P = .798).
The mean AOFAS scores were 97.80 ± 3.22 on the donor side and 98.78 ± 3 on the contralateral side. This difference was not statistically significant (P = .206).
From the total of 20 patients in the present study, hypoesthesia in the incision line was observed in 2 patients, and swelling in the incision site in 2 patients after harvesting of the peroneus longus tendon graft. All of these complications completely recovered after 6 months. After this swelling, which was observed in the early period because of the knot remaining lateral to the 2 Vicryl sutures used for tenodesis between the peroneus longus and the peroneus brevis, tenodesis was performed so that the 2 Vicryl sutures and the knot would remain more anteromedial. No other complications were observed.
To prevent peroneal nerve damage while using the tendon stripper, the other hand should be placed 6 to 8 cm distal to the fibula head so that the patient can feel the tendon stripper.
Discussion
The peroneus longus tendon graft is a viable graft option for ACLR despite concerns regarding donor site morbidity. The present study was conducted to examine the effects of peroneus longus tendon graft harvest on the donor ankle. The results of this study showed that in our sample of 20 patients undergoing ACLR using an ipsilateral peroneus longus autograft, ankle strength, stability, and functional scores were not significantly different from the contralateral side at a minimum of 12-month follow-up. The findings of Rhatomy et al 13 are in parallel with the present study results in this respect. However, in a study by Angthong et al, 1 concerns were raised about a decrease in ankle eversion strength and function. In this study, donor side morbidity was evaluated more objectively with the tests and measurements applied to the patients, and it was shown that the peroneus longus tendon graft can be used safely. However, there may be a deficit in balance. In a similar study by Vijay et al, 19 no statistically significant difference was found in ankle eversion strength on the donor side compared with the contralateral ankle eversion. No ankle instability or reduced ankle movement was reported (AOFAS mean, 96.43 ± 3.13).
The normal ACL strength 7 is 1725 ± 269 N. The peroneus longus tendon strength was defined as 1950 N by Kerimoğlu et al, 11 showing similar strength as the natural ACL. In recent literature, a graft diameter of ≥8 mm is now accepted in ACLR. It has been previously reported that the peroneus longus tendon graft is more advantageous than the hamstring in terms of diameter and tensile strength. 14 It is much more advantageous in the knee region compared with the hamstring graft, especially after ACLR. Vijay et al 20 evaluated knee functions in 140 patients and obtained better results compared with hamstring graft use in both the International Knee Documentation Committee (IKDC) and Mental Component Score scores (P = .803, P = .161, respectively). The 2-year follow-up results of patients who underwent ACLR with the peroneus longus tendon graft were reported, and excellent IKDC, mental component score, Tegner-Lysholm, AOFAS, and FADI scores were observed. A better graft diameter was obtained, along with less thigh hypotrophy, excellent ankle function results, and better results in a series of jumping tests. 12 In a systematic examination and meta-analysis of ACLR with hamstring and peroneus longus autografts in 925 patients by He et al, 10 the Lysholm and IKDC scores of the peroneus longus group were observed to have improved more than those of the hamstring group. However, there was no difference in the FADI score.
In a study of 82 patients by Cakar et al, 6 complications were observed: hypoesthesia in the distal foot in 15 patients, compartment syndrome in 2, and hyperalgesia over scar tissue in 2. The most common complication is iatrogenic damage to the distal fibres of the sural nerve. Hypoesthesia may be observed, as it provides a cutaneous branch to the skin on the lateral side of the foot. In that study, the procedure was performed with an incision from 3 different sites (fibula proximal-distal-lower end). In contrast, the method in the present study was performed with a single incision, which was considered to be sufficient and less invasive. 6 Unlike other studies, this study examined the balance status of patients to emphasize the importance of proprioception. Although significance was observed in the flamingo test (P = .049), no statistically significant results were obtained in the eyes closed balance test, the standing on tiptoe test, or the Y test. The times measured in the balance tests were shorter on the donor side, indicating the need to provide a proprioception-strengthening exercise program for all patients.
The limitations of this study are a small sample size, a short follow-up period, and a lack of comparison between pre- and postoperative results. Another shortcoming of this study was its retrospective nature. Also, the small number of participants may leave some of the comparisons underpowered.
Conclusion
There remains an insufficient number of studies on this subject in the literature. The results of the present study demonstrated that the peroneus longus tendon can be safely used as an autograft in ACLR. After graft harvesting, patients should participate in a regular rehabilitation program supported by proprioception, balance, and strengthening exercises. In addition to the comfort and practicality of graft harvesting, it can be used as an autograft in many areas. There is also the cosmetic advantage of a small incision, which is not always visible, as a sock may cover it.
Footnotes
Acknowledgements
The authors thank resident doctor Kagan Turker for his efforts in preparing the data and visuals.
Final revision submitted May 4, 2025; accepted June 5, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Suleyman Demirel University Health Sciences Ethics Committee Decisions (decision no:26, dated:13.09.2024).