
Abstract
Background:
Anterior cruciate ligament (ACL) injuries commonly occur in athletes, and ACL reconstruction (ACLR) after ACL injury can predictably allow athletes to return to sports (RTS). However, the time to RTS can be variable and dependent on a variety of patient and surgical factors.
Purpose:
To evaluate the associations between hamstring tendon (HT), quadriceps tendon (QT), and bone-patellar tendon-bone (BPTB) autograft choice and RTS data for athletes after primary ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Recreational and competitive athletes aged between 13 and 24 years, undergoing primary ACLR at an academic tertiary institution located in the central United States from 2010 to 2022, were included in the study. RTS outcome variables, including time from procedure to RTS clearance, return to previous level, return to competition, and reinjury (ACL retear and meniscus tear), if found to be significantly associated with autograft type, were subsequently assessed using Wilcoxon rank-sum tests with Bonferroni correction and logistic regression, with the HT autograft as the reference, to investigate the relationship between different autograft types and patients' recovery and clearance status. Graft failure was based on clinical history of reinjury, physical examination, magnetic resonance imaging, and/or revision surgery.
Results:
A total of 200 patients who had ACLR were included in this study. Athletes with hamstring tendon autografts were cleared at 25.4 weeks postoperatively, while those treated with BPTB and QT autografts were cleared at 41.1 and 37.6 weeks, respectively (P < .001). Of 55 athletes treated with the HT, 53 (96.4%) returned to competition. Also, 43 of 43 (100%) of athletes treated with BPTB autografts, and 22 of 22 (100%) athletes treated with QT autografts returned to competition. Moreover, 34 of 88 (38.6%) of HT autografts, 8 of 83 (9.6%) BPTB autografts, and 3 of 28 (10.7%) QT autografts had a subsequent ACL graft failure (P < .001). After adjusting for sports level, QT and BPTB autografts continued to have reduced rates of reinjury and subsequent meniscal tear when compared with HT autografts.
Conclusion:
HT autograft patients, on average, were cleared sooner and more likely to suffer an ACL graft tear compared with BPTB or QT patients. However, all 3 graft choices demonstrated similar RTS rates. This study is important for shared decision-making between orthopaedic surgeons and athletes when determining the optimal, patient-specific graft for ACLR.
Anterior cruciate ligament (ACL) tears are relatively common and result in 100,000 to 300,000 reconstructions being performed in the United States per year. 17 ACL reconstruction (ACLR) is typically performed in athletes looking to resume cutting and pivoting in sports. 26
Bone-patellar tendon-bone (BPTB), hamstring tendon (HT), and quadriceps tendon (QT) grafts are the most common autograft options for ACLR. BPTB autografts may lead to faster biologic incorporation, while HT autografts may have fewer donor site morbidity issues. 17 While BPTB remains the gold standard autograft choice from a historical perspective for high-level athletes, QT utilization is recently increasing because of improved donor site morbidity and optimistic early clinical outcomes.7,11 A pediatric study found that QT autografts had larger diameters and resulted in fewer retears when compared with HT autografts. 22 A systematic review and meta-analysis concluded that QT was similar to BPTB and HT autografts. Still, it resulted in decreased anterior knee pain compared with BPTB and improved function compared with HT. 21 Less information is available regarding the effect of graft choice on recovery, especially the quadriceps muscle function, which is impacted after ACLR.23,26 Studies have shown that 82% of patients returned to any level, and 63% returned to the previous level of play. 2
Information is lacking regarding the effect of graft choice on return to sports (RTS) rates. Understanding the influence of graft type on variables such as RTS capabilities and the likelihood of second ACL injury is necessary for determining the optimal graft choice for the athlete. This study aimed to determine the relationship between graft choice and RTS rates, clearance timing, and reinjury rates. We hypothesized that patients with QT autografts would RTS more quickly when compared with patients with HT and BPTB autografts.
Methods
Study Design
An institutional review board (IRB)-approved, retrospective review was conducted on patients who underwent ACLR by 1 of 7 surgeons (including R.W. and B.R.W.) at a single academic medical center between January 2010 and February 2022 (Figure 1). Recreational and competitive athletes, identified as participating in a sport via chart review, aged between 13 and 24 years, who injured their ACL were eligible. The study included primary reconstructions using QT, BPTB, and HT autografts. Participants were excluded if they had a follow-up time of <1 year.

Flow chart of the inclusion and exclusion criteria for the study.
Data Collection
Study data were collected and managed using REDCap (Research Electronic Data Capture) electronic data capture tools hosted at the University of Iowa.9,10 REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources.
Date cleared by the physician to RTS, return to previous level of play, return to competition, and reinjury rates were collected. ACL retear was determined by clinical history of reinjury, physical examination, magnetic resonance imaging, and/or confirmation during revision surgery. The last follow-up date was also collected. Return to competition was defined as returning to a game or meet-type situation, and return to previous level was defined as college athletes returning to the college level and recreational athletes returning to recreational sports. Clearance to RTS was determined by physician judgment and/or passing RTS testing. Additionally, meniscus cartilage treatment data were collected. They included medial meniscal repair, lateral meniscal repair, medial meniscal debridement, lateral meniscal debridement, medial meniscal transplant, lateral meniscal transplant, chondroplasty, microfracture, and osteochondral autologous transplantation.
Statistical Analysis
Primary outcome variables included time from procedure to RTS clearance, return to previous level, return to competition, and reinjury (ACL retear and meniscus tear). Moreover, the meniscus cartilage treatment was assessed.
Data are presented as median (first quartile [Q1] - Q3) for continuous variables and as number (%) for categorical variables. Outcomes were first compared among 3 autograft types using the Kruskal-Wallis test for continuous variables and the chi-square test for categorical variables.
Continuous variables found to be significantly different among autograft groups were examined using pairwise Wilcoxon rank sum tests with Bonferroni correction, with the HT as the reference. Categorical outcomes significantly associated with autograft type were assessed using logistic regression to investigate the relationships between different autograft types and patients' recoveries and clearance statuses. Regarding potential confounders, we examined age, sex, and sports level for their associations with the autograft type and outcome variables. Those variables found to be statistically significant and with a substantial influence on the effect size were included in the final models of outcomes with autograft type (reference group, HT).
All statistical analyses were performed using R Version 4.3.3 (R Foundation for Statistical Computing). P < .05 was considered statistically significant.
Results
Descriptive Statistics
A total of 200 athletes who underwent primary ACLR were included in this study, with a median age of 17 years. There were 99 (49.5%) women and 101 (50.5%) men. There were 65 (32.5%) collegiate athletes, 70 (35%) high school athletes, 10 (5%) other athletes, and 55 (27.5%) athletes without a known level. Other athletes could consist of recreational, intramural, club, national, professional, and international athletes. Among them, 28 (14%) had QT autografts, 83 (41.5%) had BPTB autografts, and 89 (44.5%) had HT autografts (Table 1).
Participant Characteristics (N = 200) a

Data are presented as median (Q1- Q3) for continuous variables and n (%) for categorical variables. ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; HT, hamstring tendon; NA, not applicable; Q, quartile; QT, quadriceps tendon; RTS, return to sports.
Comparison Among Autograft Types
The median follow-up times were 1.4 years for QT, 1.5 years for BPTB, and 2.6 years for HT patients.
Age, sports level, meniscus cartilage treatment (yes or no), any reinjury (yes or no), ACL retear (yes or no), and subsequent meniscal tear (yes or no) were found to be significantly different among the 3 autograft types (P < .05). No significant difference was found in sex distribution among autograft types (P = .14).
The Kruskal-Wallis test revealed significant differences in time from the procedure to RTS clearance among the 3 autograft groups (P < .001). The median time from procedure to clearance was 37.6 (33.2-41.2) weeks for QT patients, 41.1 (29.1-52.1) weeks for BPTB patients, and 25.4 (23.3-28) weeks for HT patients (Table 2 and Figure 2). Subsequent pairwise comparisons revealed significant differences in clearance time between QT and HT (P < .001) patients, as well as between BPTB and HT patients (P < .001), indicating that patients undergoing QT and BPTB procedures had longer clearance times compared with patients undergoing HT procedures. No substantial difference was detected between QT and BPTB patients in clearance time (P = .86). There was no significant difference among the levels of sports participation.
Participant Characteristics by Autograft Type a

Data are presented as median (Q1- Q3) for continuous variables and n (%) for categorical variables. The Kruskal-Wallis test was conducted for continuous variables, and the chi-square test was performed for categorical variables. The bold P values indicate statistical significance (P < .05).
ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; HT, hamstring tendon; NA, not applicable; Q, quartile; QT, quadriceps tendon; RTS, return to sports.
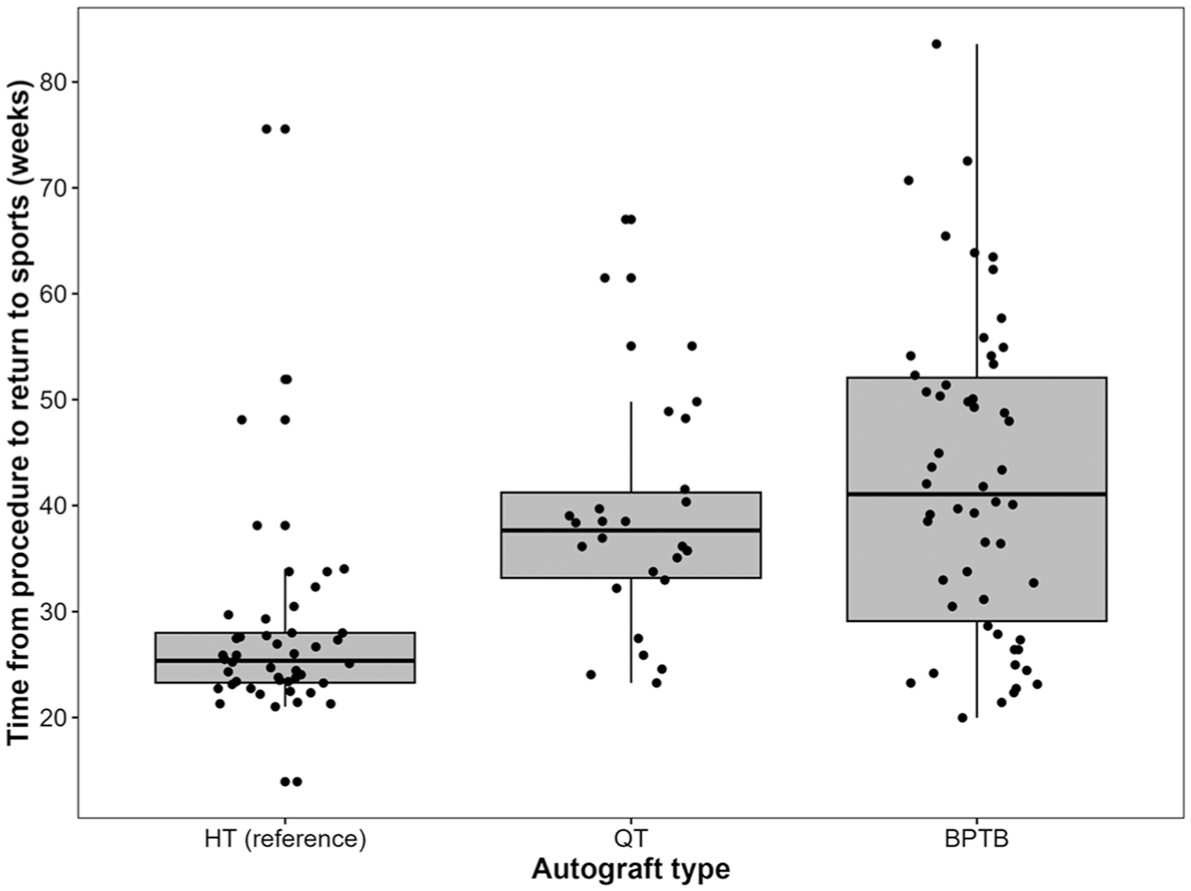
Comparison of time from procedure to RTS clearance by autograft type. RTS, return to sports.
Association Analyses of Outcomes With Autograft Type
The potential confounders (age, sex, and sports level) were tested in the relationships between dichotomous outcomes and graft type.
No significant relationship was detected between the potential confounders (age, sex, and sports level) and meniscus cartilage treatment; thus, none of these variables were added to the model.
Logistic regression indicated that the BPTB group exhibited 2.34 times higher odds of concurrent meniscus cartilage treatment compared with the HT group (P = .013) (Table 3). There was no statistically significant difference in the concurrent meniscus cartilage treatment rate between QT and HT procedures (P = .31).
Associations Between Concurrent Meniscus Cartilage Treatment and Autograft Type (Reference, HT) a

Bold P values indicate statistical significance (P < .05). BPTB, bone-patellar tendon-bone; HT, hamstring tendon; OR, odds ratio; QT, quadriceps tendon.
Wald P value.
Univariate logistic analyses revealed significant associations between sports level and reinjury; therefore, it was included in the final model.
Adjusting for sports level, athletes who underwent QT procedures showed a statistically significant 0.1 times lower odds of reinjury compared with those who underwent HT (P < .001) (Table 4). Athletes who underwent BPTB procedures showed a statistically significant 0.24 times lower odds of reinjury compared with those who underwent HT (P < .001). Reinjury information collected included medial collateral ligament (MCL) tear, MCL sprain/strain, ACL tear, ACL sprain/strain, meniscal tear, cyclops/scar tissue debridement, and other.
Associations Between Reinjury and Autograft Type (Reference, HT) a

Bold P values indicate statistical significance (P < .05). BPTB, bone-patellar tendon-bone; HT, hamstring tendon; OR, odds ratio; QT, quadriceps tendon.
Wald P value, a adjusted for sports level.
No significant association was found between the potential confounders and ACL retear; therefore, none of them was added to the model.
Patients who received QT autografts had 0.19 times lower odds of ACL retear compared with those who had HT autografts (P = .01) (Table 5). The BPTB group had a statistically significant 0.17 times lower odds of retear compared with the HT group (P < .001).
Associations Between ACL Retear and Autograft Type (Reference, HT) a

Bold P values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; HT, hamstring tendon; OR, odds ratio; QT, quadriceps tendon.
Wald P value.
Univariate logistic analyses revealed marginally significant associations between sports level and meniscal tear, and including it in the model would substantially change the beta of the autograft type variable by >20%. Thus, it was included in the final model as a confounder.
Adjusting for sports level, participants who underwent QT procedures showed a statistically significant 0.22 times lower odds of meniscal tears compared with those who underwent HT procedures (P = .004) (Table 6). Participants who underwent BPTB procedures showed a statistically significant 0.24 times lower odds of meniscal tears compared with those who underwent HT procedures (P < .001).
Associations Between Subsequent Meniscal Tear and Autograft Type (Reference, HT) a

Bold P values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; BPTB, bone-patellar tendon-bone; HT, hamstring tendon; OR, odds ratio; QT, quadriceps tendon.
Wald P value, a adjusted for sports level.
Discussion
This retrospective study reviewed RTS rates for athletes after ACLR among QT, HT, and BPTB autografts. Our goal in this study was to determine which graft type was associated with better RTS outcomes by analyzing return to competition, time to clearance to RTS, and reinjury rates. HT autograft athletes appear to RTS significantly more quickly, according to our results. This earlier return could be due to their greater quadriceps strength and ability to pass the RTS testing sooner. QT autografts have also been shown to have inferior quadriceps strength after reconstruction when compared with HT autografts. 14 Return to competition was similar among all graft types, which were not amenable to statistical testing due to smaller sample sizes. ACL retears and other reinjuries were significantly more likely in HT athletes as well. In the literature, HT autograft failure was reported in 6.9% (2/29) of those returning to play by Jeffers et al, 13 15% (42/275) by Barber-Westin and Noyes, 3 0% (0/49) in 24 months by Ebert et al, 6 9% (19/210) by Blucher et al, 4 10% (85/862) within 5 years by Manara et al, 19 13.3% (4/30) by Britt et al, 5 in 17% at 15 years by Leys et al, 16 and 14/84 (17%) by Maheshwer et al. 18 These sources demonstrate that HT retear rates are variable.
A pediatric meta-analysis concluded that QT autografts were comparable with BPTB and HT autografts in athletes. They found a 2.5% graft failure rate among QT autografts. 27 Our ACL retear rates were higher than those found in the meta-analysis, which could be caused by our smaller sample size or an increased activity level in the population studied. The most critical factors influencing graft retear of autograft ACLRs are younger age and higher activity level. This was a highly active group of athletes wishing to RTS, made up of predominantly teenage populations. In addition, Johnston et al 14 found that QT grafts were not quicker to recover than HT grafts. We found that HT grafts recovered significantly quicker than BPTB and QT autografts.
In addition, concurrent meniscus and/or cartilage treatment can act as a confounder during recovery from ACLR and for subsequent reinjury rates. A study by Mesnard et al 20 provided evidence that repair to both menisci had an impact on hamstring muscle strength but did not affect muscle recovery when only repairing a single meniscus in combination with ACLR. 20 Time to RTS was found to take longer for ACLR combined with meniscal repair than for meniscal repair alone by Vanderhave et al. 25 Adhitya et al 1 found that patients undergoing ACLR who also had meniscal injury were more likely to suffer a reinjury at 12 and 24 months.
A study evaluating BPTB and HT autografts showed that HT autograft patients passed RTS testing in 8 months as opposed to 11 months in BPTB autografts, with the BPTB group having less quadriceps strength than the HT patients. 24 Reinjury rates can be decreased by recovering for more extended periods before returning to sports; the shorter RTS time in our HT group may be the reason for the increased rate of ACL retears. A study by Grindem et al 8 showed a 51% decrease in reinjury for each month of delay in RTS from 6 to 9 months. Passing RTS testing and comparable quadriceps strength can also decrease the risk of reinjury.8,12
The results of this study are important for shared decision-making between athletes facing ACLR and their physicians. While HT autografts may lead to faster recovery, they also pose a higher risk of reinjury than BPTB and QT autografts. However, if an athlete would like to RTS sooner, an HT autograft may be an option. Furthermore, many of these HT autograft ACLRs were cleared at a standard 6 months in the earlier period of the dataset, which limits the comparability of time to RTS clearance between the 3 graft types. QT autografts show comparability to the BPTB gold-standard graft. Our study can add to the limited literature surrounding QT autografts and their comparison with BPTB autografts. These results additionally represent a more generalizable population of young people, with both recreational and competitive athletes included.
Strengths
A strength of this study is its duration. Data were collected on patients from 2010 to 2022 and included 200 patients at various levels.
Limitations
A limitation of this study is its retrospective nature and lack of consistent follow-up. This limitation in follow-up made gathering return to competition and return to previous level of play data difficult, leading to a substantial reduction in our sample size. At the same time, retrospective study designs only allow demonstration of association and not causation. In addition, the number of surgeons involved in the study led to variability in RTS clearance decisions. However, the surgeons used the same physical therapy group for RTS assessments and used data from those physical therapists, along with shared decision-making between the athlete and family, for RTS decisions. Likewise, the reinjury rate in this study may be influenced by several factors—including the athletes' level of participation (both recreational and competitive), the type of sport played (which was not analyzed), and the athletes' adherence to follow-up after clearance. Moreover, athletes who do well may not follow up, while those who meet the follow-up criteria may experience more problems. Similarly, the longer follow-up observed in the HT autograft group increases the risk of rerupture. Most collegiate athletes were preferentially treated with BPTB, given that it is the gold standard graft for high-risk athletes, which may have influenced retear rates between patients based on graft types. In addition, all patients were included when analyzing reinjury rates. Also, outcomes of articular cartilage and meniscus surgery during ACLR have different outcome trajectories and are not always generalizable to the entire ACL population. The timing of this study may introduce bias, as earlier in the study period, more patients were treated with HT autografts and cleared at 6 months, while later in the study, more BPTB and QT autografts were used, and a formal RTS protocol was implemented. The small sample size of QT autografts may also make the results of this study less reliable; however, model fitness for dichotomous outcomes in Tables 3 to 6 was checked univariately and multivariately. The uneven distribution of graft types, including the smaller QT sample size, did not lead to any issues with logistic regression convergence, suggesting that there was a sufficient sample size in the QT group for modeling. Furthermore, due to the length of this study and the sample size, we could not control for fixation method (interference screw vs button), which may have changed over time. This study was also conducted at a single institution.
Conclusion
HT athletes returned to sports more quickly and saw higher rates of ACL retears and reinjuries than BPTB and QT autograft patients.
Footnotes
Acknowledgements
Thank you to Shannon Ortiz and Armand John Gentile for their work on this project, including the database and IRB.
Final revision submitted April 23, 2025; accepted June 4, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: This project was funded by the Department of Orthopaedics and Rehabilitation at the University of Iowa. Research conducted for this manuscript was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under grant number UL1TR002537. This manuscript does not speak to the attitudes of the National Institutes of Health. This manuscript is under the authority of the authors. B.R.W. received royalties and consulting fees from Conmed and is a member of the Board of Directors of the American Orthopaedic Society for Sports Medicine, Association of Clinical Elbow and Shoulder Surgeons (ACESS), the American Board of Orthopaedic Surgery, and the Mid-America Orthopaedic Association. R.W. is a consultant for Smith & Nephew, Conmed, and Responsive Arthroscopy; has received research support from Smith & Nephew (R2018120186) and the Department of Defense (W81XWH-18-PRORP-CTRA); is an editorial board member of Arthroscopy Journal and The American Journal of Sports Medicine; and is a committee member of the American Orthopaedic Society for Sports Medicine (AOSSM), ISHA -The Hip Preservation Society, and the Arthroscopy Association of North America. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Iowa, Iowa City, Iowa, USA.