
Abstract
Background:
The shape and size of the meniscus are closely related to the stability of the knee joint and the anterior cruciate ligament (ACL) injury. Studies have confirmed the correlation between meniscal morphology and isolated ACL injury.
Purpose:
To investigate meniscal parameters, including morphological changes, in participants with isolated ACL injury.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This retrospective study, conducted from January to December 2021, compared 70 patients with isolated ACL injury with 70 patients with intact ACL. The meniscal slopes and posterior meniscal angles were measured using magnetic resonance imaging. The meniscal slopes include the slope of the anterior horn of the medial meniscus (SAHMM), slope of the posterior horn of the medial meniscus (SPHMM), slope of the anterior horn of the lateral meniscus (SAHLM), and slope of the posterior horn of the lateral meniscus (SPHLM). The posterior meniscal angles include the posterior base angle of the medial meniscus (PBAMM) and the posterior base angle of the lateral meniscus (PBALM). The receiver operating characteristic (ROC) curve was used to analyze the value of meniscal morphological parameters in judging ACL injury.
Results:
The SPHMM in participants with ACL injury was greater (mean, 23.24° ± 3.42°) than that in participants without (mean, 21.88° ± 3.35°) (P = .019). The PBAMM of participants with ACL injury was significantly higher than that in participants with intact ACL (mean, 73.78° ± 6.32° vs 67.82° ± 5.88°) (P < .001). The ROC cutoff value for SPHMM was 20.65°, and values greater than this had 81.4% sensitivity and 45.7% specificity for ACL injury. The ROC cutoff value for PBAMM was 73.55°, and values greater than this had 54.3% sensitivity and 84.3% specificity.
Conclusion:
The authors found a strong association between morphological changes in the SPHMM and ACL injury. Therefore, morphological changes in the meniscus can indicate ACL injury.
The anterior cruciate ligament (ACL) is the main structure providing anterior stability to the knee joint by limiting movement of the tibia. 18 The meniscus also helps to maintain knee stability and prevent tibial migration, 12 meaning there is a synergistic effect between the ACL and meniscus. In the evaluation of ACL injury, magnetic resonance imaging (MRI) indirectly showed that tibial migration, posterior cruciate ligament tortuosity, lateral meniscus displacement, and medial meniscus posterior horn injury could indicate a weakening or loss of biomechanical ACL function.2,4,9,13,14,17 However, these indirect findings have low sensitivity and high specificity. 7 Studies have confirmed that the slope of the anterior horn of the medial meniscus (SAHMM) and slope of the anterior horn of the lateral meniscus (SAHLM) in patients with ACL injury are significantly reduced.11,18 However, the association between meniscus-related geometric features and ACL injury has not been clarified.1,10
The purpose of this study was to define and measure the morphological parameters of the meniscus, and to analyze the relationship between these parameters and ACL injury.
Methods
This retrospective study was approved by the research ethics board of our hospital (IRB00006761-M2023314). Included in this study were patients who were admitted to our hospital between January and December 2021 for standardized knee MRI examination. The inclusion criteria were (1) age 18 to 60 years, (2) MRI of the knee joint showing intact meniscus, and (3) isolated ACL injury confirmed by arthroscopy. Exclusion criteria included patients whose injury was combined with (1) multiple ligament injury, (2) secondary and above articular cartilage injury, (3) meniscal injury, and (4) direct contact injury.
We collected information on the age, sex, and knee joint side of patients with ACL and patients in the control group. This study included the same number of people without pathological changes of the knee joint as a matched control group according to age and sex characteristics. The clinical manifestations of these patients were knee joint discomfort or pain, and MRI scans did not show abnormal lesions.
MRI scanning equipment came from GE, Siemens, and United Imaging, and the field strengths of the equipment were 1.5 and 3.0 T. All MRI scans were performed in the radiology department of our center. All imaging parameters were measured independently by 2 musculoskeletal professional radiologists (Q.W. and Y.Z., 5 and 10 years of imaging diagnostic experience, respectively). The 2 doctors were unaware of the participants and measured the knee joint images of the patients and volunteers, respectively.
The meniscal slopes (MSs) were measured in the sagittal image (Figure 1, A and B) by drawing a straight line along both the upper and lower surfaces of the anterior and posterior horns. The angle between the 2 straight lines was the MS. The MSs studied were the SAHMM, slope of the posterior horn of the medial meniscus (SPHMM), SAHLM, and slope of the posterior horn of the lateral meniscus (SPHLM).

Measurement of meniscal parameters. (A) The sagittal image was determined and measured by the midpoint position of the tibial plateau in the coronal image (orange line determines the sagittal section). (B) Measurement of the posterior horns of the medial meniscus between the line L1 passing through the femoral border of the meniscus and the line L2 passing through the tibial border of the meniscus in the sagittal section’s posterior horn of the medial meniscus. The measurement method of the anterior angle of the medial meniscus and the angle of the lateral meniscus is the same as above. (C) The sagittal image was determined and measured by the midpoint position of the tibial plateau in the coronal image (orange line determines the sagittal section). (D) Measurement of the posterior base angle of the medial meniscus between the line L3 passing through the posterior border of the meniscus and the line L4 passing through the tibial border of the meniscus in the sagittal section’s posterior horn of the medial meniscus. The measurement method of the angle of the lateral meniscus is the same as above.
The posterior base angle of the meniscus (PBAM) was measured in the sagittal image (Figure 1, C and D). Because of the high variability of the anterior base angle of the meniscus and the influence of the transverse ligament of the knee, it is difficult to measure this angle, and the measurement error is large. Therefore, this study only measured the PBAM. First, the median coronal image is determined, and the midpoint position of the medial and lateral tibial plateaus is determined. The sagittal image through this point is the target image. In this sagittal image, a straight line is drawn along the bottom edge of the posterior horn and the posterior edge of the meniscus. The angle between the 2 straight lines is the meniscal base angle, which is recorded as the posterior base angle of the medial meniscus (PBAMM) and posterior base angle of the lateral meniscus (PBALM).
Statistical Analysis
SPSS (Version 24.0; IBM Corp; https://www.ibm.com/spss) was used to perform statistical analysis. According to the previous literature and clinical experience, the sample size ratio of the experimental group and the control group was set to 1:1, and the sample sizes of the experimental group and control group were calculated to be 46 and 46 cases, respectively, for a total of 92 cases. The histogram was used to test the normal distribution, and the F test was used to test the homogeneity of variance. For the continuous variables, mean ± standard deviation was used to investigate normally distributed variables, and median (interquartile range) was used for other variables. An independent-sample t test was performed to compare groups of normally distributed continuous variables, and a Mann-Whitney U test was carried out to compare groups comprising other continuous variables. The receiver operating characteristic (ROC) curve was used to analyze the value of meniscal morphological parameters in judging ACL injury. A statistically significance threshold of .05 was used.
Results
All parameters across both groups were normally distributed. Data were first assessed for each reviewer and subsequently compared between groups, and the consistency between groups was good.
Our study included 70 patients with ACL injury (52 male) and 70 control cases (52 male). The age of patients with ACL injury was 18 to 46 years (mean, 28.13 ± 6.13 years); the control group was aged 18 to 45 years (mean, 28.11 ± 6.09 years).
The MSs of both groups are shown in Table 1. In the ACL injury group, SPHMM was higher than that in the ACL-intact group (mean, 23.24° ± 3.42° vs 21.88° ± 3.35°; P = .019) (Figure 2). There was no significant difference in SAHMM, SAHLM, and SPHLM between the ACL injury group and the ACL-intact group.
Comparison of Meniscal Parameters of Patients With ACL Injury and ACL Intact a
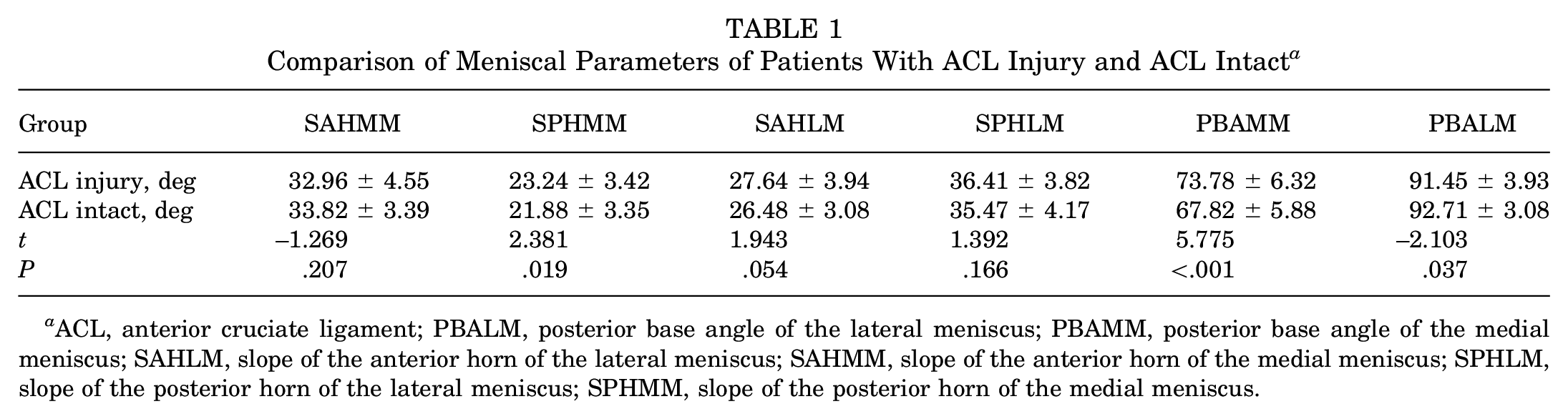
ACL, anterior cruciate ligament; PBALM, posterior base angle of the lateral meniscus; PBAMM, posterior base angle of the medial meniscus; SAHLM, slope of the anterior horn of the lateral meniscus; SAHMM, slope of the anterior horn of the medial meniscus; SPHLM, slope of the posterior horn of the lateral meniscus; SPHMM, slope of the posterior horn of the medial meniscus.

The slope of the posterior horn of the medial meniscus in (A) patients with ACL injury and (B) patients with ACL intact. Comparing the images, we found that the slope of the posterior horn of the medial meniscus in patients with ACL injury was larger.
In the ACL injury group, PBAMM was larger than that in the ACL-intact group (mean, 73.78° ± 6.32° vs 67.82° ± 5.88°; P = <.001) (Figures 3 and 4). The PBALM in the ACL injury group was smaller than that for patients with intact ACL (mean, 91.45° ± 3.93° vs 92.71° ± 3.08°; P = .037) (Figures 3 and 4). All PBAMM and PBALM values are shown in Table 1.

The posterior base angle of the medial meniscus in (A) patients with ACL injury and (B) patients with ACL intact. Comparing the images, we found that the posterior base angle of the medial meniscus in patients with ACL injury was larger.

The posterior base angle of the lateral meniscus in (A) patients with ACL injury and (B) patients with ACL intact. Comparing the images, we found that the posterior base angle of the lateral meniscus in patients with ACL intact was larger.
Multivariate logistic regression analysis showed that SPHMM and PBAMM were independent influencing factors of ACL injury (Table 2).
Logistic Regression Analysis Showing the Influencing Factors of ACL Injury a

ACL, anterior cruciate ligament; PBALM, posterior base angle of the lateral meniscus; PBAMM, posterior base angle of the medial meniscus; SPHMM, slope of the posterior horn of the medial meniscus.
In the ROC curve analysis for ACL injury, the best cutoff value of SPHMM was 20.65°, and values greater than this showed 81.4% sensitivity and 45.7% specificity (Table 3). The best cutoff value of PBAMM was 73.55°, and values greater than this showed 54.3% sensitivity and 84.3% specificity. The best cutoff value of PBALM was 91.15°, and higher values showed 45.7% sensitivity and 74.3% specificity.
AUC of Meniscal Parameters a

AUC, area under the curve; PBALM, posterior base angle of the lateral meniscus; PBAMM, posterior base angle of the medial meniscus; SPHMM, slope of the posterior horn of the medial meniscus.
Discussion
The most significant feature of this study was the ability to explore the relationship between meniscal morphological parameters and ACL injury. Patients with injured ACL had significantly higher SPHMM and PBAMM than participants with intact ACL, which revealed new indirect MRI findings in ACL injury.
During internal rotation and axial shift of the knee joint, the meniscus and ACL work synergistically to prevent excessive internal rotation and axial shift of the knee joint.6,8,18 When the ACL is damaged or broken, its synergistic effect becomes weaker, and the force from internal rotation and axial displacement of the knee joint will be more distributed to the meniscus. 15 This, in turn, causes morphological changes in the meniscus. In ACL injury, internal rotation of the knee joint and anterior displacement of the tibia often persist, meaning the meniscus will continue to be stressed. By measuring morphological parameters of the meniscus, ACL injury can be indirectly indicated.
After ACL injury, the medial meniscus undergoes greater external force than the lateral meniscus, and the resulting deformation is greater. The outer edge of the medial meniscus connects with the medial collateral ligament and activity is small, while the outer edge of the lateral meniscus has no attachment structure and the activity is relatively large. 16 Therefore, the medial meniscus is subjected to a greater external force than the lateral meniscus. Consequently, morphological changes are greater. 18 The results of our study confirmed the anatomic features and also confirmed this point. Our study found that the angle change of the medial meniscus is larger than that in the lateral meniscus, and this change is mainly concentrated in the posterior corner of the meniscus. This phenomenon is also consistent with the biomechanical changes of intra-articular rotation and tibial advancement after ACL injury.
After ACL injury, the knee joint is internally rotated and the tibia is moved forward. The internal rotation (femur relative to the tibia) of the knee joint will stress the anterior horn of the lateral meniscus and the posterior horn of the medial meniscus and produce corresponding deformation. The force is largest on the posterior horn of the medial meniscus, and morphological changes are the most obvious. Guess and Razu 5 conducted finite element analysis on a model constructed in patients with ACL injury and volunteers and found that the contact force and circumferential tension increased in the posterior horn of the medial meniscus, while the anterior horn did not change significantly. The authors concluded that the posterior horn of the medial meniscus acts as a physical barrier to limit the forward movement of the tibia. The incidence of posterior horn injury in the medial meniscus is higher in patients with ACL injury. This also indirectly shows the importance of the posterior horn of the medial meniscus during internal rotation of the knee joint and anterior displacement of the tibia.10,16
The measurement of meniscal parameters can be carried out independently from the other structures in our study. Elmansori et al 3 compared the inclination angles of the medial and lateral menisci in patients with a torn ACL with those of noninjured participants. The MS increased in patients with a torn ACL. The MS was taken as the highest point of the anterior and posterior angles, which included not only the slope of the meniscus but also the angle of the tibia. In our study, the independent measurement of meniscal parameters is not affected by other structural measurement parameters and can provide ACL injury factors more accurately.
The clinical significance of our study is not completely clear, but the purpose of our study was to explore the morphological changes of the meniscus after ACL injury. At the same time, we believe that there is a relationship between the morphological changes of the meniscus and the biomechanical changes after ACL injury, which need to be further confirmed by future studies. Our study explored the association between ACL injury and meniscal morphology. The morphology will change after ACL injury, mainly in the posterior horn of the medial meniscus. At the same time, the results of multivariate logistic regression analysis showed that SPHMM and PBAMM were independent indicators of ACL injury. The increase of SPHMM and PBAMM indicates that the posterior horn of the meniscus plays a key role in preventing the anterior displacement of the tibia after ACL injury. However, it should be noted that the logical relationship between the morphological changes of the meniscal posterior horn and the time of ACL injury needs to be clarified. These investigations constitute pivotal research anchors to further clarify the correlation between ACL injury, meniscal morphological changes, and biomechanical changes after ACL injury. In addition, we speculate that the ratio of the meniscus (the common slope of the anterior and posterior angles), the shape of the intercondylar notch, and the posterior tibial slope may be related to ACL injury. The relationship between these parameters and ACL injury will be presented in our future research.
Limitations
There were some limitations in our study. First, our study only used age and sex as labels for case matching and did not include the patient’s height, weight, or body mass index. The meniscal parameters may be related to these. A second limitation is the lack of evaluation of the time between the ACL injury and the MRI study. Because this study is a retrospective study, we believe that it is difficult to control the time of MRI examination. Finally, the 2 doctors in our study were unaware of the data of patients with ACL injury and the control group. However, ACL injury may be observed inadvertently during the measurement process, which may cause errors in the measurement results.
Conclusion
This study strongly indicates association between morphological changes of the posterior horn of the meniscus and ACL injury. The increase of SPHMM and PBAMM (above 20.65° and 73.55°, respectively) can indicate ACL injury.
Footnotes
Acknowledgements
The authors would like to thank everyone at the Department of Radiology, Peking University Third Hospital for their invaluable help with this study.
Final revision submitted August 27, 2024; accepted October 4, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the National Natural Science Foundation of China and Natural Science Foundation of Beijing. AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Peking University Third Hospital (reference No. IRB00006761-M2023314).