
Abstract
Background:
The peroneus longus tendon (PLT) autograft is suggested as a promising alternative graft option for reconstructive procedures supported by a growing body of evidence indicating favorable results. However, concerns remain regarding long-term functional impairments of the foot and ankle after harvesting a full-thickness PLT.
Purpose:
To evaluate long-term donor site morbidity in patients who underwent anterior cruciate ligament reconstruction using a PLT autograft.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective review was performed to identify patients with harvested PLT autografts, and all eligible patients were invited to participate in a clinical examination at the hospital. To evaluate their range of motion, all included patients underwent a physical examination. Clinical outcomes were measured using the American Orthopaedic Foot and Ankle Society (AOFAS) score and the Activities of Daily Living and Sports subscales of the Foot and Ankle Ability Measure (FAAM-ADL and FAAM-S). To evaluate foot and ankle structural changes, the intermetatarsal angle (IMA), hallux valgus angle (HVA), arc height index (AHI), lateral talo-first metatarsal angle (LTFMA), calcaneal pitch angle (CPA), and metatarsal angle (MA) were measured in the PLT harvested side and the contralateral side.
Results:
A total of 26 patients who were available for the final follow-up were included in this study. The mean age of the patients at the final follow-up was 45.7 ± 9.5 years. The mean follow-up time was 19.5 ± 3.4 years. AOFAS scores were excellent in 92.3% of patients (n = 24) and good in 7.7% (n = 2). The mean FAAM-ADL score was 99.6 ± 1.86. The mean FAAM-S score was 98.1 ± 5.94. No statistically significant differences were observed between the PLT harvested side and the contralateral side for any of the measured parameters—including the IMA, HVA, AHI, LTFMA, CPA, and MA.
Conclusion:
This study demonstrated good to excellent long-term patient-reported outcomes and negligible radiographic changes after harvesting the full thickness PLT compared with the contralateral side. These long-term data strongly support PLT harvesting as an alternative graft choice and suggest that this method does not alter the natural history of foot and ankle structures.
The peroneus longus tendon (PLT) was described 13 as an alternative autograft option for anterior cruciate ligament (ACL) reconstruction (ACLR) in 2008. Since then, a growing body of evidence has emerged, presenting encouraging results.17,18 Recent meta-analysis showed that the PLT autograft indicated similar functional outcomes compared with the hamstring tendon autograft for ACLR.1,11 Also, clinical studies demonstrated minimal donor site morbidity with satisfactory functional outcomes after harvesting the PLT.10,19 The PLT autograft is suggested as a promising alternative option for reconstructive procedures. 11 However, concerns remain regarding functional impairments of the foot and ankle after harvesting a full-thickness PLT.6,16
The peroneal tendons evert the hindfoot and contribute to the plantarflexion, and the PLT combines these actions to stabilize the first metatarsal head on the ground. 12 The PLT also provides active and passive contributions to locking the first metatarsal against the medial cuneiform. 3 Cadaveric studies have explored the influence of the PLT on the stiffness of the foot’s medial longitudinal arch, highlighting that insufficient traction of the PLT can lead to structural foot disorders. 14 Similarly, another study has demonstrated a significant increase in medial displacement of the transverse arch after transecting the PLT. 4 Furthermore, some authors have suggested that PLT insufficiency has the potential to cause catastrophic foot complications, similar to posterior tibial tendon dysfunction. 5
Although several clinical studies have shown minimal donor site morbidity after PLT harvesting in the short term, its long-term structural effect on foot and ankle biomechanics is still unknown. 19 This study aimed to evaluate long-term outcomes of foot and ankle function in patients who underwent ACLR using a PLT autograft. We hypothesized that PLT harvesting would have a negligible effect on foot and ankle functions in the long term.
Methods
Institutional review board approval was obtained for this study, and a retrospective review was performed to identify patients with harvested PLT autografts. A total of 64 patients who underwent ACLR using a full-thickness PLT autograft performed by the same surgeon (A.U.T.) between June 2000 and February 2007 were included in this study. All eligible patients were invited to participate in a clinical examination at the hospital. A total of 26 patients who were available for the final follow-up were included in this study. A total of 38 patients were lost to follow-up—17 patients had changed their phone number and 21 could not participate in the examination because of a change of address.
All procedures were performed at the same center using the same previously well-described operative technique. 13 Two separate incisions were created—a distal incision approximately 2 to 3 cm distal to the lateral malleolus and a second incision located 10 cm proximal to the lateral malleolus. After the skin incision, meticulous blunt dissection was performed at the distal site. The PLT was meticulously identified and secured with a No. 2 nonabsorbable suture. Subsequently, the tendon was transected, then the PLT was exposed by opening the fascia through the second incision, and the tendon was pulled up and harvested without using the tendon stripper. The remaining distal PLT stump was not secured to the peroneus brevis tendon in any of the cases.
Clinical and Radiographic Evaluation
The following baseline characteristics were recorded: age at the final follow-up, sex, duration of follow-up, dominant side, laterality of the graft harvested side, and body mass index. A physical examination that measured range of motion and patient-reported outcomes was performed. The active ranges of flexion, extension, inversion, and eversion were measured with a goniometer and compared with those of the contralateral side. The primary clinical outcome measurements were the American Orthopaedic Foot and Ankle Society (AOFAS) score and the Activities of Daily Living and Sports subscales of the Foot and Ankle Ability Measure (FAAM-ADL and FAAM-S).2,15 AOFAS scores were categorized as follows: excellent (90%-100%), good (80%-89%), fair (60%-79%), and poor (<60%). The FAAM-ADL and FAAM-S were considered as separate outcomes.
All patients underwent foot and ankle anteroposterior (AP) and lateral weightbearing radiographs of both sides at the final follow-up. To evaluate the foot structural changes, the intermetatarsal angle (IMA), hallux valgus angle (HVA), arc height index (AHI), lateral talo-first metatarsal angle (LTFMA), calcaneal pitch angle (CPA), and metatarsal angle (MA) were measured in patients while weightbearing and recorded. 7 The IMA was measured as the angle between the long axes of the first and second metatarsal bones on foot AP radiographs. The HVA was measured as the angle between the long axes of the first proximal phalanx and first metatarsal on foot AP radiographs. The AHI was calculated as the ratio of the foot’s arch height at the midpoint of its length to the total foot length on lateral radiographs. The LTFMA was determined as the angle formed between the long axis of the talus and the first metatarsal on a weight-bearing lateral view. The CPA was measured as the angle between the plantar aspect of the calcaneus and plantar planes. The MA was measured as the angle between the first metatarsal and plantar plane on a lateral radiograph (Figure 1).

(A) Measurement of the IMA and the HVA on an anteroposterior radiograph. (B) The AHI is calculated as the ratio of the AH at 50% of the TFL to the TFL. (C) Measurement of the LTFMA, CPA, and MA on the lateral radiograph. AH, arch height; AHI, arch height index; CPA, calcaneal pitch angle; IMA, intermetatarsal angle; HVA, hallux valgus angle; LTFMA, lateral talo-first metatarsal angle; MA, metatarsal angle; TFL, total foot length.
Statistical Analyses
Statistical analyses were performed using IBM SPSS Statistics software Version 24.0 (IBM Corp). Descriptive statistics were presented as the mean and standard deviation for all continuous variables and are presented in tables. Normal distribution was defined by the Shapiro-Wilk test. The Mann-Whitney U test and the Kruskal-Wallis test were used to compare the clinical and radiological outcomes of the PLT harvested side compared with the contralateral side. Statistical significance was set at P < .05.
Results
A total of 26 patients (25 men, and 1 woman) were included in the study. The mean age of the patients at the final follow-up was 45.7 ± 9.5 years (range, 30-62 years). The mean follow-up time was 19.5 ± 3.44 years (range, 12-23 years). Patient characteristics are shown in Table 1.
Patient Characteristics a
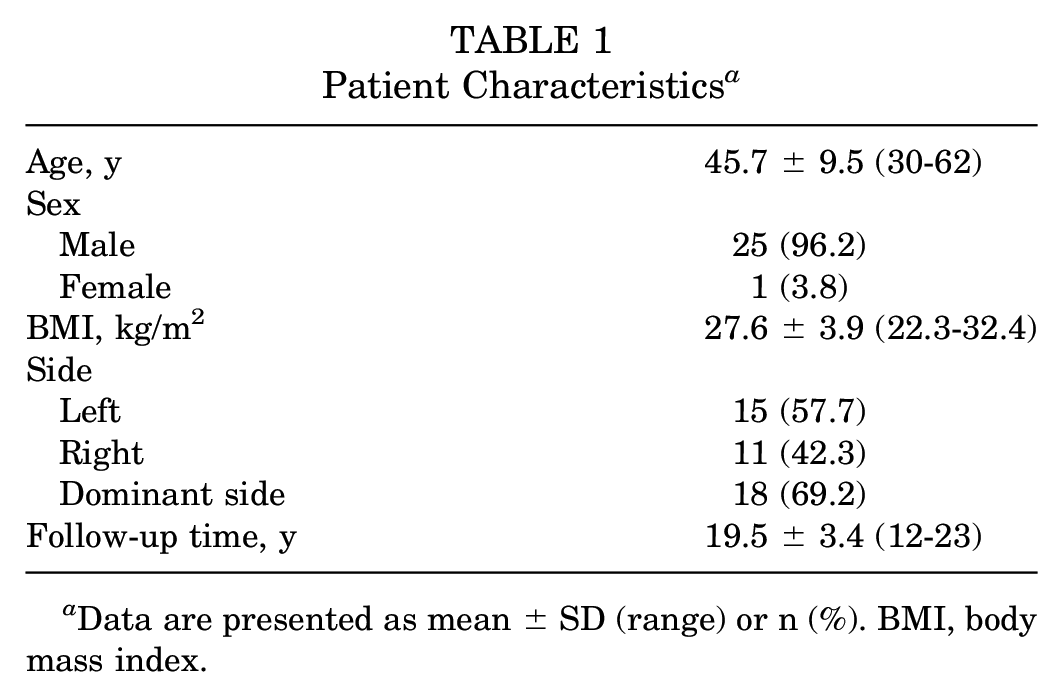
Data are presented as mean ± SD (range) or n (%). BMI, body mass index.
AOFAS scores were excellent in 92.3% of patients (n = 24) and good in 7.7% (n = 2). The mean FAAM-ADL score was 99.6 ± 1.86 (range, 90.4-100). The mean FAAM-S score was 98.1 ± 5.94 (range, 78.1-100). Clinical results are shown in Table 2. No significant differences were found in range of motion—including flexion, extension, inversion, and eversion—between the affected and healthy sides (Table 3).
Clinical Results a

Data are presented as mean ± SD (range). ADL Activities of Daily Living subscale; AOFAS, American Orthopedic Foot and Ankle Society; FAAM, Foot and Ankle Ability Measure; S, Sports subscale.
Comparison of ROM a

Data are presented as mean ± SD (range). PLT, peroneus longus tendon; ROM, range of motion.
Comparative radiographic measurements are detailed in Table 4. No statistically significant differences were observed between the affected and healthy sides for any of the measured parameters—including the IMA, HVA, AHI, LTFMA, CPA, and MA.
Radiological Results a

Data are presented as mean ± SD (range). AHI, arc-height index; CPA, calcaneal pitch angle; HVA, hallux valgus angle; IMA, intermetatarsal angle; LTFMA, lateral talo-first metatarsal angle; MA, metatarsal angle; TA, talocalcaneal angle.
Hypoesthesia was identified in 2 patients within the dermatomal distribution of the sural nerve. One patient additionally presented with radiographic evidence of stage 1 osteoarthritis in the tibiotalar joint. Notably, this patient also demonstrated stage 1 osteoarthritis in the contralateral tibiotalar joint, suggesting a preexisting condition. No other complications were observed in the remaining patients.
Discussion
The PLT autograft is increasingly used as an alternative option in primary or revision ACLR. 17 There is limited information to support the potentiality of the PLT harvesting procedure in altering the natural history of the foot structure, and the potential structural damage to the foot arch remains a concern. 16 The results of the present study address this critical gap in the literature and strongly support that PLT harvesting has a negligible effect on foot and ankle functions in the long term. After a mean follow-up period of 19.5 years, we demonstrated no significant differences between the PLT harvested side and the contralateral healthy side. These data will facilitate surgeon and patient decision-making and provide long-term data to guide expectations for clinical outcomes and foot and ankle structural survivorship.
The primary function of the PLT is plantarflexion of the foot and first metatarsal and eversion of the foot. 12 Although a decrease in active range of motion and strength parameters may be expected in the early period after harvesting the PLT, long-term neuromuscular adaptations are likely to compensate for these impairments, ultimately restoring functional capacity. 21 Our findings demonstrate this consistently with mid-term results of other studies, which demonstrated good to excellent patient-reported outcomes and range of motion. 1 On the other hand, studies investigating postoperative eversion strength yield equivocal results. Some studies reported statistically significant changes between operated and nonoperated sides, while other studies found no significant difference.19,20 Even in cases with decreased eversion torque, the remaining eversion strength is adequate for daily activities and most sports.
From a structural perspective, the PLT contributes to stabilizing and locking the first metatarsal against the medial cuneiform. In their cadaveric study, Johnson and Christensen 12 demonstrated that increasing PLT loads led to less pronounced angular changes in the sagittal and transverse planes of the medial column. They proposed that through this locking mechanism, the PLT might play a role in counteracting first-ray hypermobility, thereby restricting the development of hallux valgus deformity. Similarly, Bohne et al 4 demonstrated that in cadaveric feet, sequential soft tissue sectioning between the first and second metatarsals revealed a significant increase in IMA only upon transection of the PLT. They suggested that the PLT is a strong retaining mechanism of the first metatarsal and loss of this stabilization would lead to metatarsus primus varus. In contrast, the present study found no significant differences between the PLT harvested side and the healthy side in long-term radiographic measurements—including IMA and HVA.
This divergence in outcomes and survivorship suggests that the effect of the harvesting site of the PLT on the natural history of the foot may be most significant. In this context, Edama et al 9 described various attachment sites of the PLT insertion in their cadaveric study and proposed that these sites might contribute to stabilizing the first ray. The present findings suggest that the key stabilizing function of the PLT arises from its complex insertional structure, which extends from the cuneiform to the first and second metatarsals, and harvesting the PLT away from its insertion point may not have catastrophic consequences.
Several studies also explored the influence of the PLT on the medial longitudinal arch. Kokubo et al 14 investigated how the posterior tibialis and peroneus longus impact foot arch stiffness, finding that while the posterior tibialis significantly affects arch stiffness, the peroneus longus may not play a substantial role in maintaining the medial longitudinal arch. In their study, Dullaert et al 8 used ex vivo computed tomography scans to explore how weightbearing and PLT activation influence the first tarsometatarsal joint and foot arch. They reported that pulling the PLT resulted in a significant increase in first metatarsal rotation and a slight, nonsignificant increase in LTFMA. Our study revealed no significant variances between the PLT-harvested side and the contralateral side in lateral radiographic measurements—including AHI, LTFMA, CPA, and MA. The results of the present study align with previous studies indicating that the PLT does not function to maintain the medial longitudinal arch, and the long-term observations revealed that harvesting the PLT did not result in medial arch collapse or first ray elevation.
Limitations
This study has several limitations. One of the major limitations of this study is its retrospective design, which introduces inherent biases. Second, the sample size was not large because of the unavailability of certain patients to participate in the research. Third, the present study focused only on the long-term structural effect of harvesting the PLT. The impact of PLT harvesting on foot biomechanics is not fully understood across multiple studies, and concerns exist regarding the potential for PLT insufficiency to cause severe foot complications resembling those seen in posterior tibial tendon insufficiency.5,16 Last, the major limitation is the failure to identify any significant difference between the PLT harvested side and the healthy side, leading to the conclusion that there is no observable difference. In fact, from a philosophical standpoint, when comparing 2 groups that are inherently different, it is self-evident that there must be a difference in their outcomes. Nonetheless, we believe that these results should be encouraging to patients and surgeons that harvesting the PLT has negligible effect on foot biomechanics in the long term. Future trials with larger populations are needed to support the findings of this study as definitive conclusions.
Conclusion
This study demonstrated good to excellent long-term patient-reported outcomes and negligible radiographic changes after harvesting the full thickness PLT compared with the contralateral side. These long-term data strongly support PLT harvesting as an alternative graft choice and suggest that this method does not alter the natural history of foot and ankle structures.
Footnotes
Final revision submitted August 27, 2024; accepted October 4, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Karadeniz Technical University, School of Medicine (reference No. 24237859-340).