
Abstract
Background:
There is an increasing rate of procedures being performed for concomitant injuries during anterior cruciate ligament (ACL) surgery. Few studies have examined risk factors for these associated injuries in young patients.
Hypothesis:
There are patient-related factors predictive of concomitant knee pathology that differ between age-based cohorts.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Natural language processing was used to extract clinical variables from available notes of patients undergoing ACL surgery between 2000 and 2020 at a single institution (5174 ACL surgeries; mean age, 17 ± 4 years; 53.1% female; accuracy, >98%). Patients were stratified to pediatric (5-13 years), adolescent (14-19 years), and young adult (20-35 years) cohorts. Logistic regression was used to determine predictors of concomitant injury to the menisci, medial collateral ligament (MCL), posterolateral corner (PLC), and posterior cruciate ligament (PCL).
Results:
Between 2000 and 2020, 54% of pediatric, 71% of adolescent, and 70% of adult patients had ≥1 concomitant soft tissue injury. In children and adolescents, increased age was consistently predictive of sustaining a concomitant injury (P < .02). Female children had increased odds of concomitant medial meniscal injury, while female adults had decreased odds (P≤ .046). Adolescent and adult female patients had decreased odds of concomitant lateral meniscal injury (P≤ .027). Female children had increased odds of injury to the MCL (P = .015), whereas female children and adolescents had decreased odds of PCL injury (P≤ .044). Adolescents undergoing revision ACL surgery had increased odds of meniscal injury (P≤ .001) and decreased odds of concomitant MCL injury (P = .028). Increased body mass index (BMI) was associated with increased odds of concomitant medial meniscal injury in all cohorts (P≤ .041), lateral meniscal injury in adults (P = .045), and PLC injury in children (P = .016). Contact injuries were associated with increased odds of MCL injury in adolescents (P = .017) and PLC injury in adolescents and adults (P < .014).
Conclusion:
These findings support the hypothesis, as there were multiple factors that significantly affected the risk of concomitant injuries that differed between cohorts. Increased age, BMI, and contact injury history were generally associated with increased odds of sustaining a concomitant injury, whereas female sex and revision ACL surgery had mixed effects. Further studies are essential to investigate the sex-based differences in risk for concomitant injuries and to develop tailored treatment plans that minimize the risk of secondary ACL injury.
There is a growing incidence of anterior cruciate ligament (ACL) injuries in pediatric and adolescent populations, which is outpacing other pediatric orthopaedic injuries, as well as ACL injuries in adult populations.5,6,13,50,55 Timely reconstruction is recommended in these younger patients to minimize further intra-articular damage and facilitate a prompt return to activity.2,14,40 Concurrent with the increasing ACL injury rate, there is an increase in the number of concomitant injuries and related procedures. 55 These concomitant injuries can occur at the time of initial insult or due to progressive damage in the setting of altered joint mechanics and intra-articular derangement when surgical intervention is delayed.1,14,19,28 Concomitant injury patterns involving the menisci,3,9,14,17,38,52,55 collateral ligaments,29,43 posterolateral corner (PLC),11,24 and posterior cruciate ligament (PCL)15,16,53 have been described in the literature.
In younger cohorts, increasing age has been associated with concomitant injury to the menisci, 38 collateral ligaments, 29 and PCL. 24 The effect of patient sex on concomitant injuries is poorly characterized, with mixed effects observed within the literature.9,17,25,39 Studies report that increased body mass index (BMI) is associated with concomitant injury to the menisci,3,9,38 but not other soft tissue structures within the knee, 29 and also that obesity may be a risk factor for concomitant injury in adolescents but not pediatric patients. 33 However, there is a paucity of large-cohort studies that report on other patient-level risk factors for these associated injuries and their incidence, which remain poorly characterized.
Therefore, the purpose of this study was to use a large database of pediatric, adolescent, and young adult ACL surgeries to describe the incidence of common concomitant soft tissue injuries and evaluate, in comparative fashion, the risk factors associated with these injuries. By understanding the prevalence of these concomitant injuries as well as their risk factors, we seek to gain valuable insight to provide evidence-based care for this population. We hypothesized that there are patient-related factors predictive of concomitant knee pathology that differ between the 3 age-based cohorts.
Methods
Participants
After institutional review board approval, a custom natural language processing (NLP) pipeline 47 was used to identify all patients treated surgically at a single institution for an ACL tear between January 1, 2000, and December 31, 2020, and extract pertinent clinical and operative data from the available unstructured electronic clinical notes to develop an institutional ACL surgery registry. Details on the NLP pipeline used along with model performance metrics and validation have been previously published.47,48 Briefly, we developed an NLP model to identify ACL surgery cases from operative notes (accuracy, 1.00; sensitivity, 0.99; specificity, 1.00). 48 We then extracted relevant injury and surgical details from the unstructured clinical notes of the identified cases using NLP (accuracy, 0.98 ± 0.01; sensitivity, 0.97 ± 0.03; specificity, 0.98 ± 0.02). 47 The models were trained and tested on ground-truth labels extracted by a human examiner with adequate medical knowledge on ACL injuries on a subset of patients. During manual review, positive cases were labeled when the notes detailed an acute meniscal tear or an acute sprain or tear of the medial collateral ligament (MCL), PLC, or PCL. A concomitant PLC injury was defined as injury to the fibular/lateral collateral ligament, popliteofibular ligament, or popliteal tendon. This initial extraction created a registry including 5638 ACL surgeries. From this registry, only patients with sufficient preoperative documentation, including imaging interpretation, were included in this study.
Mechanism of injury (ie, contact vs noncontact), ipsilateral ACL injury history, sports participation, and concomitant injuries to the menisci, MCL, PLC, and PCL were extracted from clinical notes using NLP, to be used as predictors for the outcomes of interest. The outcomes of interest were also extracted from preoperative notes. Laterality was extracted from the operative reports. Age, sex, BMI, race, and insurance status were retrieved from the structured medical record.
Patients were grouped by age, with the pediatric cohort composed of patients between 5 and 13 years of age, the adolescent cohort composed of patients between 14 and 19 years of age, and the young adult cohort composed of patients between 20 and 35 years of age, which is the maximum age allowable for surgery performed at the study institution. Patients were also grouped by their level of athletic participation according to the level 1 to 3 classification proposed by Hefti et al 20 and adapted by Moksnes and Risberg. 32 In this classification, level 1 activities include frequent jumping, cutting, and pivoting (eg, soccer and basketball); level 2 activities involve lateral movements with less pivoting (eg, racket sports and gymnastics); and level 3 activities include straight-ahead activities without jumping or pivoting (eg, running and weightlifting). 32
The information for the 3 cohorts is summarized in Table 1. All surgeries were performed by 1 of 8 different sports medicine fellowship-trained orthopaedic sports medicine specialists, 4 of whom also completed general pediatric orthopaedic surgery fellowships (B.E.H., M.S.K., M.D.M., D.E.K., M.A.C., Y.M.Y., L.J.M., M.M.M.).
Cohort Characteristics a
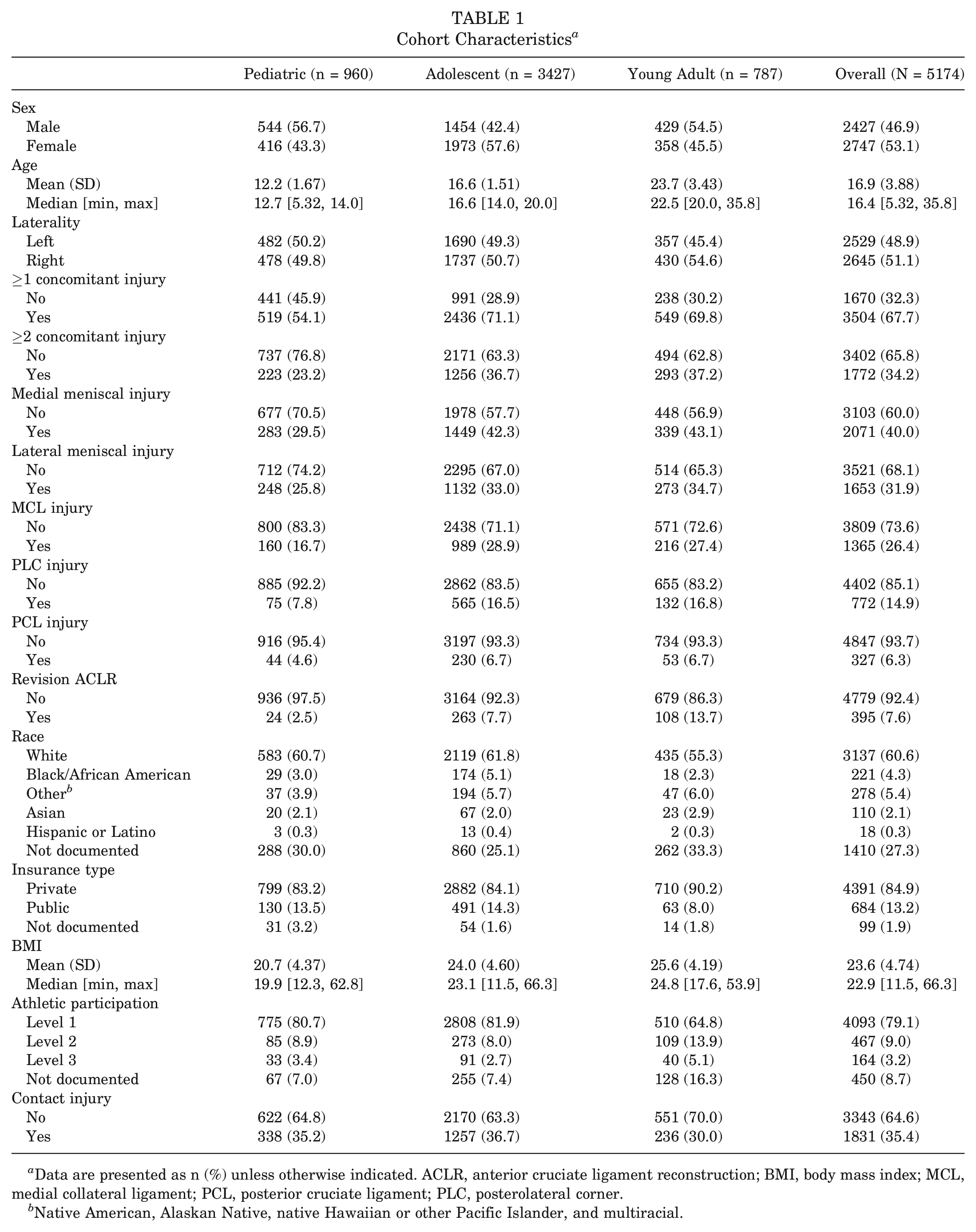
Data are presented as n (%) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; MCL, medial collateral ligament; PCL, posterior cruciate ligament; PLC, posterolateral corner.
Native American, Alaskan Native, native Hawaiian or other Pacific Islander, and multiracial.
Statistical Analysis
Patient characteristics were summarized by standard descriptive summaries (eg, means and standard deviations for continuous variables such as age and percentages for categorical variables such as sex). Logistic regression was used to evaluate potential predictors of concomitant injury. Age (continuous), sex (dichotomous), race (categorical), insurance status (dichotomous), BMI (continuous), sports level (categorical), injury mechanism (dichotomous), laterality (dichotomous), and revision ACL surgery (dichotomous) were used as predictors of concomitant injuries. Male sex, index ACL surgery, level 3 sports participation, private insurance, White race, noncontact injury, and left knee injury were used as baselines for comparison, and thus do not have associated odds ratios. Separate models were developed for (1) concomitant medial meniscal injury, (2) concomitant lateral meniscal injury, (3) concomitant MCL injury, (4) concomitant PLC injury, and (5) concomitant PCL injury for the 3 cohorts, yielding 15 unique models. Within each cohort, the lowest age (5, 14, or 20 years) was used as the reference, whereby each additional year of age led to an increase or decrease in the odds of concomitant injury based on the observed odds ratio. Adjusted odds ratios (aORs) and corresponding 95% CIs were calculated and considered significant at P < .05. The logistic regression models were developed using RStudio (Posit).
Results
The NLP pipeline identified 5174 ACL surgeries performed on patients who met the inclusion and exclusion criteria. The mean age of patients at the time of surgery was 16.9 ± 3.9 years (range, 5.32-35.8 years), and the sample included 2747 (53.1%) female patients. Within the study population, 3504 (67.7%) patients had ≥1 concomitant soft tissue injury, and 1772 (34.2%) patients had ≥2 concomitant injuries. These concomitant injuries included 2071 (40%) medial meniscal injuries, 1653 (31.9%) lateral meniscal injuries, 1365 (26.4%) MCL injuries, 772 (14.9%) PLC injuries, and 327 (6.3%) PCL injuries (Table 1).
Predictors of Medial Meniscal Injury
The aORs and associated 95% CIs and P values for predictors of concomitant medial meniscal injury are presented in Table 2. In the pediatric cohort, age (aOR, 1.21; P = .002), female sex (aOR, 1.48; P = .023), and increased BMI (aOR, 1.06; P = .001) were associated with increased odds of being evaluated with a concomitant medial meniscal injury. Additionally, pediatric patients with right knee injuries (aOR, 1.4; P = .043) were more likely to have medial meniscal injuries than those with left knee injuries.
Predictors of Concomitant Medial Meniscal Injury in Pediatric, Adolescent, and Adult Cohorts a
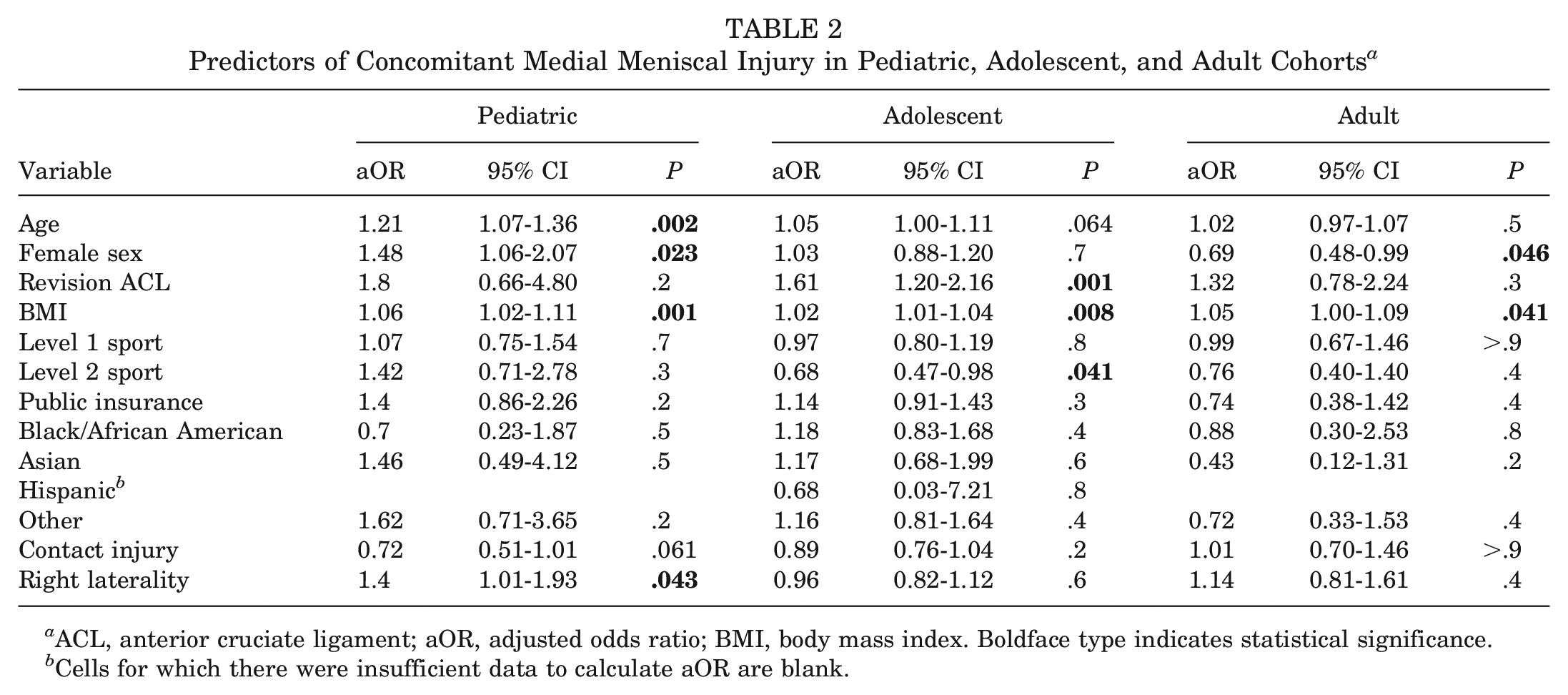
ACL, anterior cruciate ligament; aOR, adjusted odds ratio; BMI, body mass index. Boldface type indicates statistical significance.
Cells for which there were insufficient data to calculate aOR are blank.
In the adolescent subcohort, revision ACL surgery (aOR, 1.61; P = .001) and increased BMI (aOR, 1.02; P = .008) were associated with increased odds of having a concomitant injury to the medial meniscus. Additionally, level 2 sports participation was associated with decreased odds of being evaluated with a concomitant medial meniscal injury (aOR, 0.68; P = .041).
In the adult subcohort, increased BMI was associated with increased odds of being evaluated with a concomitant medial meniscal injury (aOR, 1.05; P = .041). Additionally, female sex was associated with decreased odds of concomitant medial meniscal injury (aOR, 0.69; P = .046).
Predictors of Lateral Meniscal Injury
The aORs and associated 95% CIs and P values for predictors of concomitant lateral meniscal injury are presented in Table 3. In the pediatric subcohort, increased age (aOR, 1.17; P = .008) was associated with increased odds of concomitant lateral meniscal injury.
Predictors of Concomitant Lateral Meniscal Injury in Pediatric, Adolescent, and Adult Cohorts a
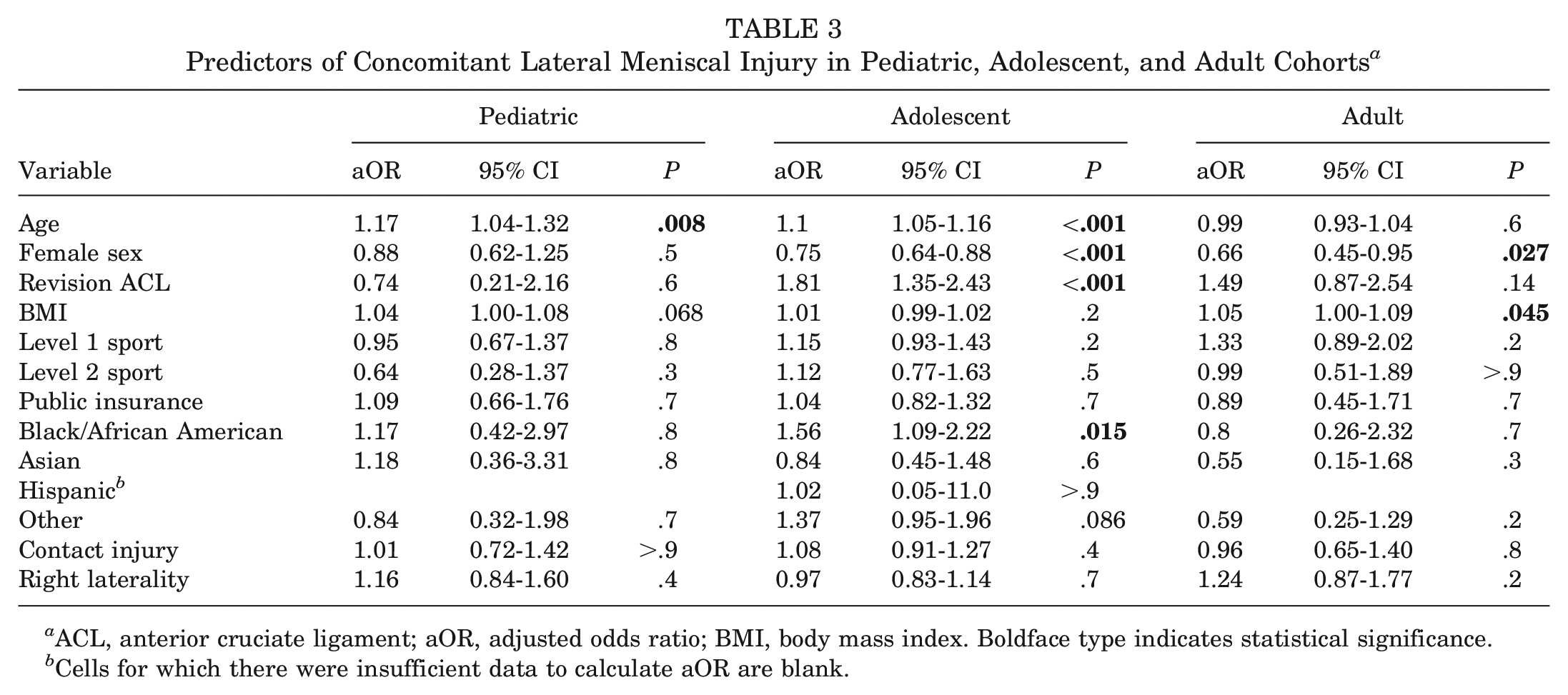
ACL, anterior cruciate ligament; aOR, adjusted odds ratio; BMI, body mass index. Boldface type indicates statistical significance.
Cells for which there were insufficient data to calculate aOR are blank.
In the adolescent cohort, increased age (aOR, 1.1; P < .001), revision ACL surgery (aOR, 1.81; P < .001), and Black/African American race (aOR, 1.56; P = .015) were associated with increased odds of concomitant lateral meniscal injury. Additionally, female sex (aOR, 0.75; P < .001) was associated with decreased odds of being evaluated with a lateral meniscal injury.
In the adult cohort, increased BMI (aOR, 1.05; P = .045) was associated with increased odds of being evaluated with a concomitant lateral meniscal injury. Additionally, female sex (aOR, 0.66; P = .027) was associated with decreased odds of concomitant lateral meniscal injury.
Predictors of MCL Injury
The aORs and associated 95% CIs and P values for predictors of concomitant MCL injury are presented in Table 4. In the pediatric subcohort, increased age (aOR, 1.18; P = .017) and female sex (aOR, 1.64; P = .015) were associated with increased odds of concomitant MCL injury.
Predictors of Concomitant Medial Collateral Ligament Injury in Pediatric, Adolescent, and Adult Cohorts a
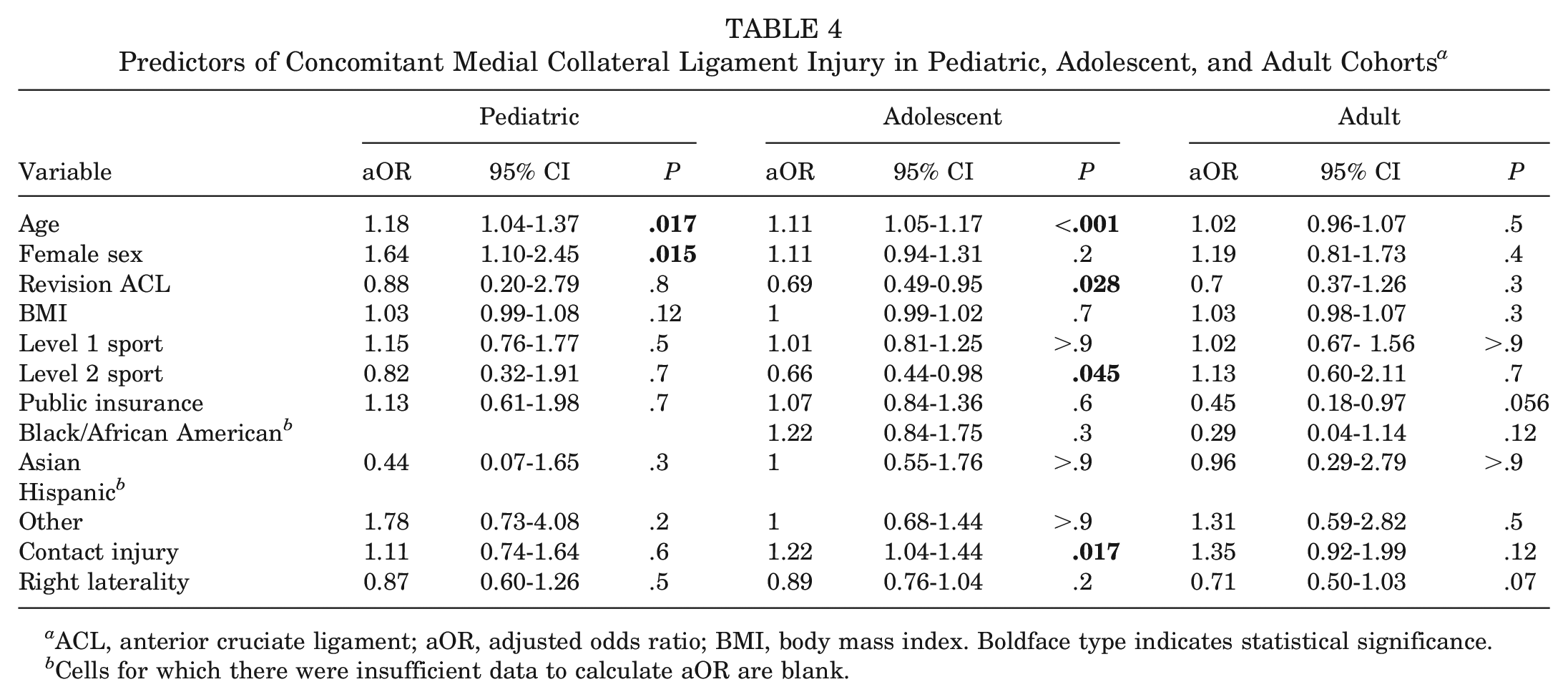
ACL, anterior cruciate ligament; aOR, adjusted odds ratio; BMI, body mass index. Boldface type indicates statistical significance.
Cells for which there were insufficient data to calculate aOR are blank.
In the adolescent subcohort, increased age (aOR, 1.11; P < .001) and contact injury mechanism (aOR, 1.22; P = .017) were associated with increased odds of being evaluated with a concomitant MCL injury. Additionally, revision ACL surgery (aOR, 0.69; P = .028) and level 2 sports participation (aOR, 0.66; P = .045) were associated with decreased odds of concomitant MCL injury.
There were no significant associations observed within the adult subcohort.
Predictors of PLC Injury
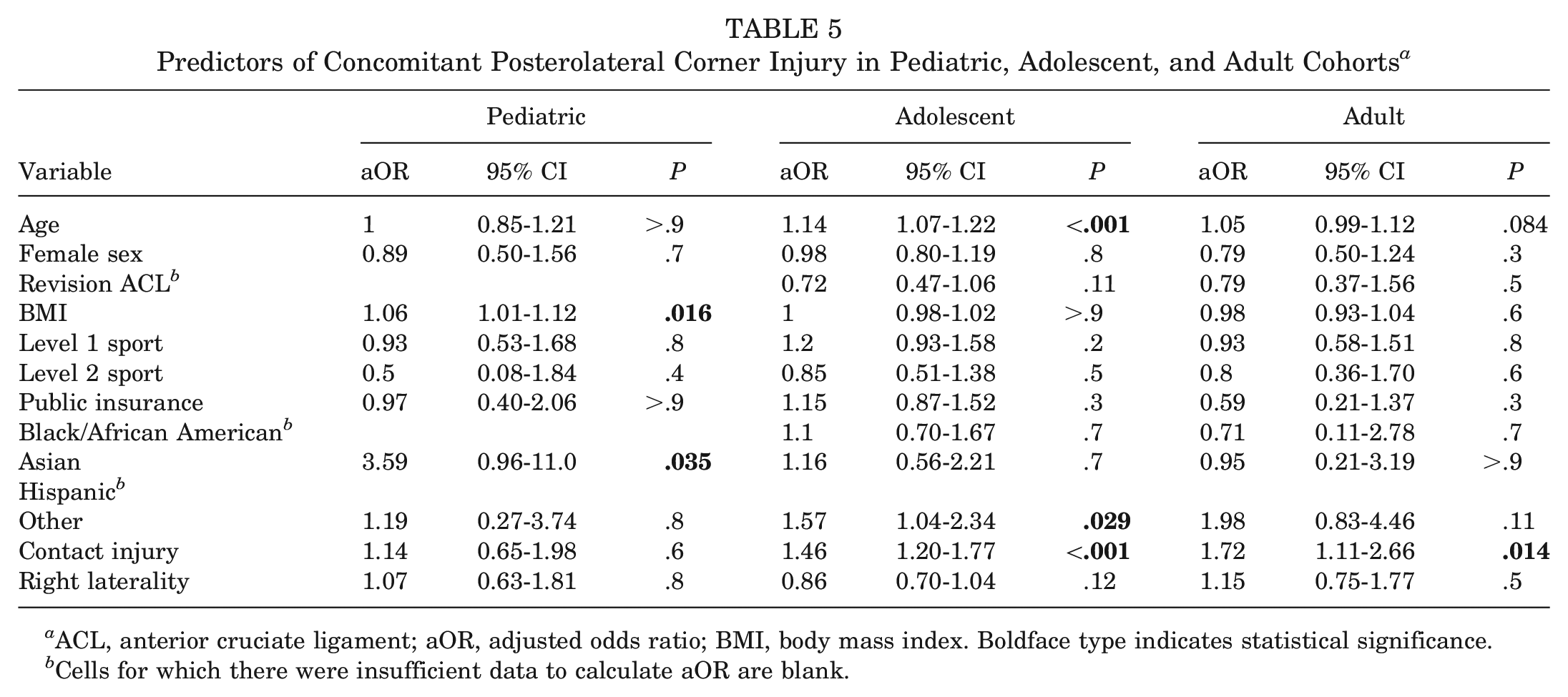
The aORs and associated 95% CIs and P values for predictors of concomitant PLC injury are presented in Table 5. In the pediatric subcohort, increased BMI (aOR, 1.06; P = .016) and Asian background (aOR, 3.59; P = .035) were associated with increased odds of being evaluated with a concomitant PLC injury.
Predictors of Concomitant Posterolateral Corner Injury in Pediatric, Adolescent, and Adult Cohorts a
ACL, anterior cruciate ligament; aOR, adjusted odds ratio; BMI, body mass index. Boldface type indicates statistical significance.
Cells for which there were insufficient data to calculate aOR are blank.
In the adolescent subcohort, increased age (aOR, 1.14; P < .001), race classification as “other” (aOR, 1.57; P = .029), and contact injury mechanism (aOR, 1.46; P < .001) were associated with increased odds of being evaluated with a concomitant PLC injury.
In the adult patients, contact injury mechanism (aOR, 1.72; P = .014) was associated with increased odds of being evaluated with a concomitant PLC injury.
Predictors of PCL Injury
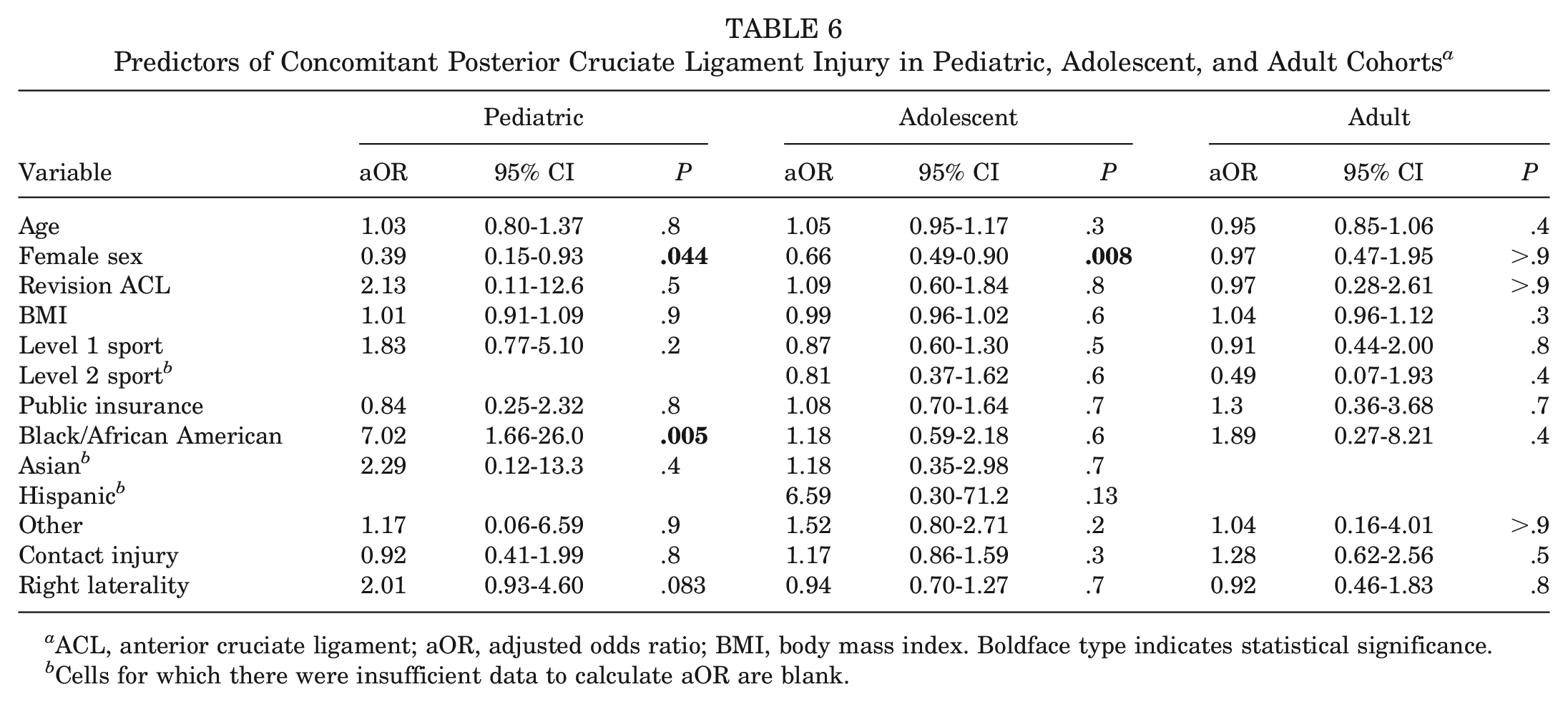
The aORs and associated 95% CIs and P values for predictors of concomitant PCL injury are presented in Table 6. In the pediatric subcohort, only Black/African American race (aOR, 7.02; P = .005) was associated with increased odds of concomitant PCL injury. Female patients had decreased odds of being evaluated with a concomitant PCL injury (aOR, 0.39; P = .044).
Predictors of Concomitant Posterior Cruciate Ligament Injury in Pediatric, Adolescent, and Adult Cohorts a
ACL, anterior cruciate ligament; aOR, adjusted odds ratio; BMI, body mass index. Boldface type indicates statistical significance.
Cells for which there were insufficient data to calculate aOR are blank.
In the adolescent subcohort, female sex was associated with decreased odds of being evaluated with a concomitant PCL injury (aOR, 0.66; P = .008).
There were no significant risk factors for concomitant PCL injury in the adult subcohort.
Discussion
This large-scale single-center study shows that in patients undergoing ACL surgery between 2000 and 2020, 67.7% of patients had ≥1 concomitant soft tissue injury, with the highest rates observed in the adolescent cohort (71%). Notably, this rate is higher than other rates reported in the pediatric and adolescent sports medicine literature, adding additional concerns and complexities to the clinical care of pediatric and adolescent patients with ACL tears. In general, increased age, increased BMI, and contact injury history were associated with increased odds of concomitant injury, whereas female sex and revision ACL surgery had mixed effects.
The current study findings demonstrated that a majority of patients evaluated with an ACL tear had ≥1 concomitant soft tissue injury with rates of 54%, 71%, and 70% observed in the pediatric, adolescent, and adult subcohorts, respectively. In their study including 208 pediatric and adolescent patients, Vavken et al 52 reported that 56% of their patients had ≥1 concurrent injury, with 32% having a medial meniscal tear and 35% evaluated with a lateral meniscal tear. However, the authors strictly included meniscal and chondral injuries in their reported concomitant injury rate, which differs from the current study's focus on meniscal and ligamentous injuries. Their group reported similar meniscal injury rates, however, as prevalence rates of 42% medial meniscal tears and 33% lateral meniscal tears were observed in the adolescent cohort of the current study. In their study of 508 pediatric and adolescent patients, Lee et al 29 reported concomitant MCL injuries in 18% of patients with ACL tears and LCL injuries in 2% of their cohort. Similarly, in the current study, there were MCL injuries in 17% of the pediatric and 29% of the adolescent cohorts. However, when considering the entire PLC, concomitant PLC injuries were observed in 8% of pediatric patients and 17% of adolescent patients. Of note, Kinsella et al 24 reported that the popliteofibular ligament (10%) and popliteus (4%) were more common than LCL tears (2%) in their pediatric and adolescent cohort. The rates reported in the current study are more consistent with the 5% to 20% rates reported in the adult literature.12,27,34,49 Notably, these rates all arise from relatively small cohorts, and large amounts of data for many injury patterns (particularly the PCL) remain scarce, highlighting the need for future large-scale prospective studies to better characterize the incidence of these concomitant injuries.
It is well described in the literature that the incidence of ACL tears is increasing in younger patients,5,21,54 highlighting the importance of considering age as a covariate in analyzing patients evaluated with an ACL injury. In the pediatric cohort, each additional year of age was associated with increased odds of injury to the medial meniscus, lateral meniscus, and MCL. In adolescents, each additional year of age was associated with increased odds of injury to the lateral meniscus, MCL, and PLC. In their study including 453 pediatric and adolescent patients, Perkins et al 38 also reported that increased age was associated with increased odds of medial and lateral meniscal tears. Dumont et al 14 also reported that increased age was independently associated with increased odds of medial meniscal tears in their study of concomitant injuries in young patients. Regarding the other soft tissue structures within the knee, Lee et al 29 observed that older age was associated with greater odds of having a collateral ligament injury, and Kinsella et al 24 reported similar findings in their study of concomitant PLC injuries in young patients. Notably, the current results only suggest an association between age and medial meniscal injuries in pediatric patients; however, the association in adolescents approached significance. The findings from the current large-cohort study strengthen the current body of pediatric and sports medicine literature, highlighting the importance of considering age when characterizing the risk profile of young, athletic patients.
Sex has been well studied as a risk factor/modifier in the incidence of ACL injury, specifically as it interacts with age.5,21,37 In the current pediatric cohort, female sex was associated with increased odds of medial meniscal and MCL injury and decreased odds of PCL injury. Adolescent female patients in this current study had decreased odds of lateral meniscal and PCL injury. Adult female patients in the current study also had decreased odds of PCL injury but uniquely had decreased odds of medial meniscal injury, differing from the pediatric cohort. In their prospective study of 541 patients (mean age, 26 years), Kluczynski et al 25 reported that male sex was a risk factor for concomitant medial and lateral meniscal tears. Similarly, in their study including 221 young athletes, Piasecki et al 39 concluded that female athletes were at lower risk of concomitant meniscal and chondral injuries. This finding was significant even without differences in mechanism of injury, including similar rates of noncontact and jumping injuries between the sexes. The authors proposed an array of potential explanations, such as differences in strength, weight, muscle recruitment, and joint alignment. In contrast to their studies, Jackson et al 23 reported in a case series including 880 pediatric patients that male patients were more likely to have lateral meniscal tears, whereas medial meniscal tears were more common in female patients. The current findings regarding the medial meniscus are more reflective of the study by Jackson et al. These studies,23,25,39 as well as the current study, are in accordance with recent literature studying lateral meniscal injuries in adult populations, with odds ratios between 2.3 and 7.4 being reported for the effect of male sex on concomitant lateral meniscal tears.9,17 There are limited data available regarding concomitant MCL and PCL injuries in the setting of ACL injury. In isolation, there are conflicting data regarding the effect of sex as a risk factor for MCL injury,41,46 and cadaveric impact simulations showed no sex difference in MCL strain during a simulated athletic task. 44 For the PCL, male patients are reported to make up between 60% and 84% of isolated and combined PCL injuries,10,15,30,36,45 and sex-related differences in PCL injury patterns have been reported. 35 The exact mechanism of these differences, if true, is unclear, highlighting a potential area of future study.
Increased weight and BMI have been well-established as risk factors for ACL injury.22,26,51 To understand the effect of body habitus on the risk of concomitant soft tissue injuries, BMI was included as a potential predictor in all models. In the current study, each 1-point increase in BMI was associated with increased odds of concomitant medial meniscal injury in all cohorts, lateral meniscal injury in adults, and PLC injury in pediatric patients. Notably, these findings are not directly in line with the recent literature regarding the effect of BMI on concomitant soft tissue injuries. While Vavken et al 52 found that increased BMI led to greater odds of concomitant medial meniscal injury in their adolescent cohort, Perkins et al 38 only observed increased odds of lateral meniscal injury when considering 2-point increases in BMI. Additionally, Dumont et al 14 observed that weight >65 kg was independently associated with increased odds of both medial and lateral meniscal tears in pediatric and adolescent cohorts. In their young adult cohort, Brambilla et al 9 reported increased odds of medial, but not lateral, meniscal tears with increased BMI. When considering the other soft tissue structures of the knee, the current study suggests that BMI has minimal effect on MCL or PCL injury risk and is associated with increased odds of PLC injury in the pediatric subcohort. In contrast, Lee et al 29 did not report any significant associations between BMI and concomitant collateral injury risk in their young cohort. The limited, somewhat conflicting data available for comparison again demonstrate the need for future large-scale collaborative efforts to understand the effect of this generally modifiable risk factor on the injury patterns and long-term joint health of young, adolescent populations.
Level 1 sports such as basketball, soccer, football, and lacrosse are known to increase the risk of ACL injury when compared with other sports,4,18 and in general these injuries tend to be noncontact.7,8 However, high-energy contact mechanisms are often a cause of other ligamentous injuries in these athletic cohorts. 31 In the current study, contact injury history was associated with increased odds of injury to the MCL in adolescents and to the PLC in the adolescent and adult cohorts. These findings support those of Lee et al, 29 who observed a 120% increase in odds of concomitant collateral ligament injury in pediatric and adolescent patients who sustained a contact injury. Similarly, Salem et al 42 reported a significant increase in the incidence of grade 3 collateral ligament damage in adults sustaining contact ACL injuries. This constellation of findings, in accordance with the recent sports medicine literature, reinforces the importance of sports participation/level as a variable when classifying ACL and concomitant injury risk, as well as in patient-specific counseling and management for these high-risk cohorts.
This study is not without limitations. Primarily, this was a single-center study. Accordingly, it is unclear to what extent these findings are generalizable to other populations. However, the results presented stem from 20 years of treating patients at a large, regional academic referral center, which is believed to sufficiently represent a substantial portion of the general pediatric population. Additionally, this study only identified patients with ACL injuries who underwent surgery at our institution. Therefore, this registry may be missing clinical data about patients who had index or revision procedures at another institution. Also, patients with ACL tears managed nonsurgically who had concomitant injuries may not have been included. However, as surgical management is generally recommended to young patients with ACL deficiency, the effects of this limitation are minimal. Finally, the current study is susceptible to selection bias because of its retrospective design.
Conclusion
Based on analysis of 5174 ACL reconstruction procedures at a single academic medical center between 2000 and 2020, >67% of patients undergoing ACLR had ≥1 concomitant soft tissue injury, with injuries to the medial and lateral menisci being the most prevalent. Increased age, increased BMI, and contact injury history were associated with increased risk of multiple concomitant injuries, whereas female sex and revision ACL surgery demonstrated mixed effects. There were no significant associations between body habitus and concomitant soft tissue injuries. Given the implications of concomitant injuries on overall prognosis and arthritis risk in this young, active subpopulation, these data underscore the importance of future studies investigating prevention strategies and the vigilance ACL surgeons must apply in the detection and treatment of these common additional injuries.
Authors
James A. Pruneski, MD, Benton E. Heyworth, MD, Mininder S. Kocher, MD, Nazgol Tavabi, PhD, Matthew D. Milewski, MD, Dennis E. Kramer, MD, Melissa A. Christino, MD, Yi-Meng Yen, MD, PhD, Lyle J. Micheli, MD, Martha M. Murray, MD, Leah Gilreath, Alexander Kim, Joseph Murray, and Ata M. Kiapour, PhD (Department of Orthopedic Surgery and Sports Medicine, Boston Children's Hospital, Harvard Medical School, Boston, Massachusetts, USA).
Footnotes
Acknowledgements
The authors thank Dr. Amir Kimia, Mr. Assaf Landschaft, and Ms. Lanna Feldman for assisting with this study.
Submitted April 28, 2023; accepted August 29, 2023.
Presented as a poster at the annual meeting of the AOSSM, Washington, DC, July 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study received funding support from the Children's Hospital Orthopedic Surgery Foundation and Boston Children's Hospital Faculty Council. B.E.H. has received education payments from Arthrex, Kairos Surgical, and Pylant and is a consultant and stock owner for Imagen Technologies. M.S.K. has received consulting fees and royalties from OrthoPediatrics and Ossur; royalties from Elsevier and Wolters Kluwer; speaking fees from Smith & Nephew; and support for education from Kairos Surgical Inc. D.E.K. is a paid consultant for Miach Orthopaedics and DePuy Synthes and receives education support from Kairos Surgical. M.D.M. has received royalties from Saunders/Mosby-Elsevier. Y.-M.Y. has received consulting fees from OrthoPediatrics and Smith & Nephew. L.M. is an unpaid consultant for Carticel. M.M.M. owns stock and has received consulting fees from Miach Orthopaedics and has received royalties from Springer. A.M.K. is a paid consultant of Miach Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.