
Abstract
Background:
Management of chondral injury can be difficult due to the avascularity of articular cartilage and the limited ability to proliferate and promote repair. Untreated lesions can lead to early development of arthritis and the need for joint replacement. For intermediate-sized lesions, osteochondral autograft transfer and autologous cell-based cartilage treatment have been accepted as the most effective treatment options.
Purpose:
To investigate the rates of complications within 2 years of initial surgery in patients who undergo primary autologous cell-based cartilage treatment and osteochondral autograft.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective cohort study was performed on July 17, 2024, using a commercially available insurance claims database to investigate 2-year orthopaedic complication rates in 1298 patients after primary osteochondral autograft and autologous cell-based cartilage treatment for chondral injuries of the knee. Patient cohorts were propensity score matched with a caliper set to 0.2 at a ratio of 1 to 1 on the following variables: age, sex, diabetes, and tobacco use. Rates of surgical complications were compared using multivariable logistic regression, adjusted for age, sex, diabetes, obesity, and tobacco use. Odds ratios (ORs) with corresponding 95% CIs were calculated for each comparison.
Results:
A total of 1298 patients were included in this retrospective analysis. Patients who underwent autologous cell-based cartilage treatment were significantly more likely to need revision cartilage restoration surgery compared with those who underwent osteochondral autograft treatment (11.1% vs 7.4%; OR, 1.58 [95% CI, 1.08-2.34]). There was no significant difference in the rate of progression to osteoarthritis (11.4% vs 10.6%; OR, 1.15; [95% CI, 0.80-1.65]) or subsequent knee arthroplasty (0.5% vs 1.1%; OR, 0.54 [95% CI, 0.11-2.06]) within 2 years of initial procedure between the treatment cohorts.
Conclusion:
This study highlights the increased risk of revision for patients who underwent autologous cell-based cartilage treatment compared with those who underwent osteochondral autograft treatment. However, no significant difference was identified in progression to osteoarthritis or subsequent knee arthroplasty within 2 years after the initial procedure. Further studies that evaluate long-term outcomes and the progression of symptoms are needed.
Keywords
Cartilage injuries to the knee are common and are usually caused by trauma to the knee, osteoarthritis, osteonecrosis, knee instability, or malalignment. 9 The literature shows that up to 63% of knees have chondral lesions when examined via arthroscopy. 6 Cartilage injuries can lead to significant immediate symptoms such as pain, swelling, stiffness, locking, and catching sensations in the joint.15,22 Treatment for these lesions depends on various factors, including patient age, activity level, cause of the injury, and size of the chondral defect. 24 Management of chondral injury can be difficult because of the avascularity of articular cartilage and the limited ability to proliferate and promote repair. 34 Appropriate intervention with chondral defects is often performed to prevent early development of arthritis and the need for joint replacement.17,25,32
There are 3 categories of treatment options for symptomatic focal cartilage defects of the knee: (1) Mesenchymal stem cell stimulation, which includes microfracture, drilling, and abrasion chondroplasty; (2) substitution options, including osteochondral autograft transfer and osteochondral allograft; and (3) biologic replacement options, such as autologous cell-based cartilage treatment, stem cell therapy, and tissue engineering.19,31 Treatment options depend on several factors, one of the most important being the size of the chondral lesion. For small lesions (<2 cm2), chondroplasty, microfracture, osteochondral allograft, and osteochondral autograft constitute the most appropriate treatment options and have been shown to have acceptable outcomes. 21 For intermediate and large lesions (>2 cm2), osteochondral autograft and autologous cell-based cartilage treatment have been accepted as effective treatment options.3,14,30 Osteochondral autograft involves harvesting osteochondral plugs from donor sites—usually nonweightbearing areas of articular cartilage, which can lead to donor site morbidity—and it is a single-stage procedure. In autologous cell-based cartilage treatment, chondrocytes are harvested in a first-stage procedure and expanded in vitro before being reintroduced into the joint in the second-stage procedure. While it avoids the donor site morbidity associated with osteochondral autograft, it is a 2-stage procedure requiring the use of more resources and higher costs for the patient and the health care system.27,36 The literature comparing outcomes after these procedures is limited by small patient cohorts, and there does not appear to be a current consensus.11,16,20,26,35
The present study aimed to (1) compare the rates of complications within 2 years from initial surgery, and (2) compare these rates in the context of cost differences reported in the literature between autologous cell-based cartilage treatment and osteochondral autograft. It is hypothesized that patients who undergo autologous cell-based cartilage treatment would have lower rates of joint complications than patients who undergo osteochondral autograft, and that autologous cell-based cartilage treatment would be associated with higher surgical costs than osteochondral autograft.
Methods
Data Source and Study Design
Patient records were queried from the PearlDiver Mariner database (PearlDiver Inc), a commercially available administrative claims database that contains de-identified patient data from the inpatient and outpatient settings. The database contains the medical records of patients across the United States between 2010 and the third quarter of 2022, which are derived from billable claims accepted and paid out through clearinghouses used by insurance payors. This study utilized the “M165Ortho” data set within PearlDiver, which contains 165 million patients. All health insurance payors are represented, including commercial, private, and government plans. Researchers extract data using Current Procedural Terminology (CPT) and International Classification of Diseases, Ninth and Tenth revision (ICD-9/ICD-10) codes. Institutional review board exemption was granted as provided data were de-identified and compliant with the Health Insurance Portability and Accountability Act (Study 2024-1096). No outside funding was received for this study.
A retrospective cohort study was performed on July 17, 2024, to investigate patient outcomes after various treatment methods for chondral injuries of the knee. Only patients who had continuous enrollment in the database during the study period were included in the study. Patients were identified using CPT codes and sorted into osteochondral autograft or autologous cell-based cartilage treatment cohorts. To avoid falsely elevated numbers of reoperations for the autologous cell-based cartilage treatment cohort, only CPT-27412, the code for the second stage of the procedure, was used to create the autologous cell-based cartilage treatment cohort. In addition, to avoid heterogeneity in the autologous cell-based cartilage treatment cohort, patients included in this study were limited to those who underwent the initial procedure between December 2016 and October 2022. The rates of complications, such as diagnosis of knee osteoarthritis, knee stiffness (defined by ICD-10-D-M25661 or ICD-10-D-M25662, indicating ‘stiffness of right or left knee, not elsewhere classified’), knee revision cartilage restoration, knee arthroplasty (includes unicompartmental and total knee arthroplasty), manipulation under anesthesia, lysis of adhesions, irrigation and debridement, meniscectomy, ligamentous procedures (includes anterior cruciate ligament, posterior cruciate ligament, and collateral ligaments), arthroscopic cleanup (includes lysis of adhesions, synovectomy, and loose body removal), and the mean time to osteoarthritis diagnosis, and revision cartilage restoration procedures were compared in patients who underwent either primary osteochondral autograft or autologous cell-based cartilage treatment. Cartilage injury of the knee was defined with ICD-10 diagnosis codes. Revision cartilage restoration (includes chondroplasty, microfracture, osteochondral autograft, autologous cell-based cartilage treatment, and osteochondral allograft), knee osteoarthritis, knee arthroplasty, manipulation under anesthesia, irrigation and debridement, meniscectomy, ligamentous procedures, and arthroscopic cleanup were defined with CPT/ICD-10 codes. All ages were included. Patients were filtered to exclude instances of previous diagnosis of knee osteoarthritis, previous cartilage repair procedures, including microfracture, osteochondral autograft, and autologous cell-based cartilage treatment, and previous total knee arthroplasty. All codes used to define all relevant diagnoses and procedures are provided in Appendix Table A1.
Descriptive and Clinical Characteristics
Baseline descriptive data were obtained for all patient cohorts, including age and sex (Table 1). Clinical characteristics obtained included the prevalence of diabetes mellitus, obesity (defined by ICD diagnosis codes indicating body mass index of ≥30 kg/m2), tobacco use, hypertension, chronic obstructive pulmonary disease, chronic kidney disease, congestive heart disease, coronary artery disease, rheumatoid arthritis, and Elixhauser Comorbidity Index. Codes used to define clinical characteristics are provided in Appendix Table A1.
Descriptive Data for Patients Undergoing Osteochondral Autograft or Autologous Cell-Based Cartilage Treatment a

BMI, body mass index; COPD, chronic obstructive pulmonary disease; ECI, Elixhauser comorbidity index.
Outcomes
Outcome parameters investigated were as follows: the frequency with which patients were diagnosed with knee stiffness; osteoarthritis; revision cartilage restoration procedures; manipulation under anesthesia/arthroscopic cleanup; meniscal/ligamentous procedures; total knee arthroplasty; unicompartmental knee arthroplasty; time to revision surgery; time to osteoarthritis diagnosis; and time to reoperation within 2 years of initial surgical management of knee cartilage injury.
Statistical Analysis
Statistical analyses were performed using the R statistical software Version 4.1.0 (R Project for Statistical Computing) integrated within the PearlDiver software with an α level set to .05. Patient cohorts were propensity score matched with a caliper set to 0.2 at a ratio of 1 to 1 on the following variables: age, sex, diabetes, and tobacco use. Categorical variables were compared with a chi-square test, and continuous variables were compared with the Welch t test or the Mann-Whitney U test. Rates of surgical complications were compared using multivariable logistic regression, adjusted for age, sex, diabetes, obesity, and tobacco use. Odds ratios (ORs) with corresponding 95% CIs were calculated for each comparison.
Results
Before applying the exclusion criteria, 3393 patients underwent autologous cell-based cartilage treatment, and 6151 patients underwent osteochondral autograft. After filtering for patients who were continuously enrolled in the database for the entire study period of 2 years (3 months before their first instance of CPT codes for the relevant procedure to 2 years after the relevant procedure), there were 882 in the autologous cell-based cartilage treatment cohort and 1603 in the osteochondral autograft cohort. After applying the exclusion criteria outlined above, there were 649 patients in the autologous cell-based treatment cohort and 1337 patients in the osteochondral autograft cohort. After matching at a 1 to 1 ratio, the final study groups consisted of 649 patients in each cohort for a total of 1298 patients included in this analysis.
Patients who underwent autologous cell-based cartilage treatment had a significantly higher risk of revision cartilage procedures within 2 years compared with patients who underwent osteochondral autograft (11.1% vs 7.4%; OR, 1.58 [95% CI, 1.08-2.34]) (Table 2). Patients who underwent autologous cell-based cartilage treatment also had a significantly higher risk of all reoperations within 2 years compared with patients who underwent osteochondral autograft (15.1% vs 11.4%; OR, 1.39 [95% CI, 1-1.92]). These patients had no significant difference in likelihood of diagnosis of osteoarthritis within 2 years compared with patients who underwent osteochondral autograft (11.4% vs 10.6%; OR, 1.15 [95% CI, 0.80-1.65]). No significant difference was observed in the risk of knee stiffness diagnosis within 2 years (15.3% vs 12.9%; OR, 1.20 [95% CI, 0.88-1.65]). No significant difference was found in the risk of irrigation and debridement within 2 years between treatment cohorts (0.3% vs 0.8%; OR, 0.37 [95% CI, 0.05-1.75]). No significant difference was found in the likelihood of knee cleanup within 2 years in the autologous cell-based cartilage treatment cohort compared with patients who underwent osteochondral autograft (6.2% vs 4.3%; OR, 1.43 [95% CI, 0.87-2.37]). Patients who underwent autologous cell-based cartilage treatment demonstrated no significant differences in the likelihood of meniscal/ligamentous procedures within 2 years compared with patients who underwent osteochondral autograft (2% vs 2.8%; OR, 0.71 [95% CI, 0.34-1.46]). Patients who underwent autologous cell-based cartilage treatment had no significant difference in the likelihood of unicompartmental knee arthroplasty/total knee arthroplasty within 2 years compared with patients who underwent osteochondral autograft (0.5% vs 1.1%; OR, 0.54 [95% CI, 0.11-2.06]).
Rates of Complications Within 2 Years of Osteochondral Autograft Versus Autologous Cell-Based Cartilage Treatment a

OR, odds ratio; Ref, reference.
There was no significant difference in the mean time to osteoarthritis diagnosis compared with patients treated with osteochondral autograft (318 days vs 287 days; P = .4126) (Table 3). There was no significant difference in the mean time to revision cartilage procedures compared with patients treated with osteochondral autograft (314 days vs 297 days; P = .6042), nor was there any significant difference in the mean time to reoperation compared with patients treated with osteochondral autograft (288 days vs 244 days; P = .1268).
The Mean Time to Complications After Osteochondral Autograft and Autologous Cell-Based Cartilage Treatment a

Data are presented as mean ± SD. Ref, reference.
The frequency with which patients received concomitant meniscal surgery was 17.3% versus 4.8% for osteochondral autograft and autologous cell-based cartilage treatments, respectively. The proportion of patients who underwent concomitant ligamentous procedures was 60.9% in the osteochondral autograft cohort versus 17.6% in the autologous cell-based cartilage treatment cohort. The rate of concomitant osteotomy procedures was 8.2% for the osteochondral autograft cohort versus 21.1% for the autologous cell-based cartilage treatment cohort.
Discussion
The major findings of this study demonstrated a 58% higher rate of ipsilateral knee revision cartilage restoration procedures in patients who underwent autologous cell-based cartilage restoration procedures compared with those who underwent osteochondral autograft treatment (11.1% vs 7.4%; OR, 1.58 [95% CI, 1.08-2.34]). No significant differences were observed in other complications within 2 years, including diagnosis of osteoarthritis (11.4% vs 10.6%; OR, 1.15 [95% CI, 0.80-1.65]), knee stiffness (15.3% vs 12.9%; OR, 1.20 [95% CI, 0.88-1.65]), or subsequent procedures, such as irrigation and debridement (0.3% vs 0.8%; OR, 0.37 [95% CI, 0.05-1.75), arthroscopic cleanup (6.2% vs 4.3%; OR, 1.43 [95% CI, 0.87-2.37]), meniscal/ligamentous procedures (2% vs 2.8%; OR, 0.71 [95% CI, 0.34-1.46]), or arthroplasty (0.5% vs 1.1%; OR,0.54 [95% CI, 0.11-2.06]). No significant differences were observed in the time from the initial procedure to revision cartilage restoration procedures (314 days vs 297 days; P = .6042).
This study aimed to investigate the complication rates of 2 different surgical treatment options for chondral lesions of the knee and compare these rates in the context of the costs associated with these procedures. Since the size and specific location of chondral lesions within the knee joint cannot be discerned in the present study, the treatment cohorts investigated cannot be assumed to be equal in severity of injury. This study does not intend to suggest superiority of one technique over the other for a specific size or location of cartilage injury, but rather to globally assess the rates of complications for these procedures.
The results of this study demonstrate a 58% higher rate of ipsilateral knee revision cartilage restoration procedures in patients who underwent autologous cell-based cartilage treatment compared with those who received osteochondral autograft treatment. This difference could be attributed to differences in the biological incorporation of these graft types into the area of cartilage lesion. Autologous cell-based cartilage treatment requires injection of chondrocytes or placement of a chondrocyte-rich matrix into the chondral lesion on top of the subchondral bone, which is then sealed with suture or fibrin glue. 18 osteochondral autograft, however, uses a full-thickness plug with mature hyaline cartilage attached to subchondral bone to fill in the chondral defect, and it has been shown to provide more rapid integration at the defect site. 7 This study found no significant difference in the mean time to revision between treatment cohorts. This may indicate that although patients who undergo autologous cell-based cartilage treatment have an increased likelihood of requiring additional cartilage restoration surgery compared with patients who undergo osteochondral autograft, the temporality of failure between index procedures remains similar. This could be due to a similar mechanism for graft failure, including a lack of proper incorporation of the graft into the surrounding articular cartilage, leading to persistence of the incongruent articular surface.10,12 Another possible explanation for these findings is the size limitations between the procedures. Most studies 4,23,28 suggest the upper limit for osteochondral autograft to be approximately 4 to 6 cm2, while the typical minimum lesion size indicated for autologous cell-based cartilage treatments is 3 cm2 with an upper limit of 10+ cm2.
Although this study found a significantly higher incidence of revision cartilage restoration procedures after autologous cell-based cartilage treatment compared with osteochondral autograft, there were no detectable differences within 2 years in rates of other complications investigated, including diagnosis of osteoarthritis, knee stiffness, knee irrigation and debridement, knee cleanup procedures, meniscal/ligamentous procedures, and knee arthroplasty. There was a 20% higher likelihood of developing postoperative knee stiffness and a 43% increased likelihood of undergoing manipulation under anesthesia/lysis of adhesions/synovectomy/removal of loose body after autologous cell-based cartilage treatment compared with osteochondral autograft; nonetheless, these outcomes were not significant (P > .05). This could potentially be caused by a higher incidence of graft hypertrophy and periosteal extrusion in early generations of autologous cell-based cartilage treatment compared with osteochondral autograft. 13
The mean cost of surgery for autologous cell-based cartilage treatment is estimated2,5,8,33,37 to be approximately $10,195 to $16,000, while the cost of osteochondral autograft ranges between $3823 and $7187. The cost of autologous cell-based cartilage treatment can be drastically higher (up to $66,939) when the price of transport, storage, isolation, and expansion of chondrocytes, as well as the need for 2 procedures, is factored in. 29 It is important to consider appropriate resource allocation in addition to patient clinical outcomes data when deciding between treatment options for patients with symptomatic articular cartilage lesions.
This study should be interpreted in the context of its limitations. By only evaluating complications within 2 years, this analysis is limited to outcomes within this timeframe. Furthermore, because continuous database enrollment for 2 years after the index procedure was required for inclusion, patients who changed insurance carriers or lost insurance coverage within 2 years after surgery were excluded. In addition, the possibility of coding errors is inherent in any analysis of administrative claims data. However, such instances 1 are rare and made up only 0.9% of Medicare and Medicaid payments in 2023. A causal relationship cannot be established between autologous cell-based cartilage treatment/osteochondral autograft and the risk of postoperative complications, given the retrospective nature of this study. Another limitation of this database study is the inability to establish and analyze the effect of cartilage lesion size in our patient cohorts. As the database only allows examination of diagnosis and procedure codes, the present study is not capable of analyzing outcomes of these procedures based on lesion size. Also, the results of this study may be affected by the variable outcomes of different generations of autologous cell-based cartilage treatment, which have evolved and improved rapidly over recent years. To mitigate this, the patient cohorts included in this study were limited to those who underwent the initial procedure between 2016 and 2022. In addition, although matching and multivariable regression were used, differences in terms of rates of cohort comorbidities or other confounders not controlled for in the regressions could have influenced the results.
Conclusion
This study highlights the increased risk of revision for patients who underwent autologous cell-based cartilage treatment compared with those who underwent osteochondral autograft. However, no significant difference was identified in progression to osteoarthritis or subsequent knee arthroplasty within 2 years after the initial procedure. Further studies that evaluate long-term outcomes and the progression of symptoms are needed.
Footnotes
Appendix
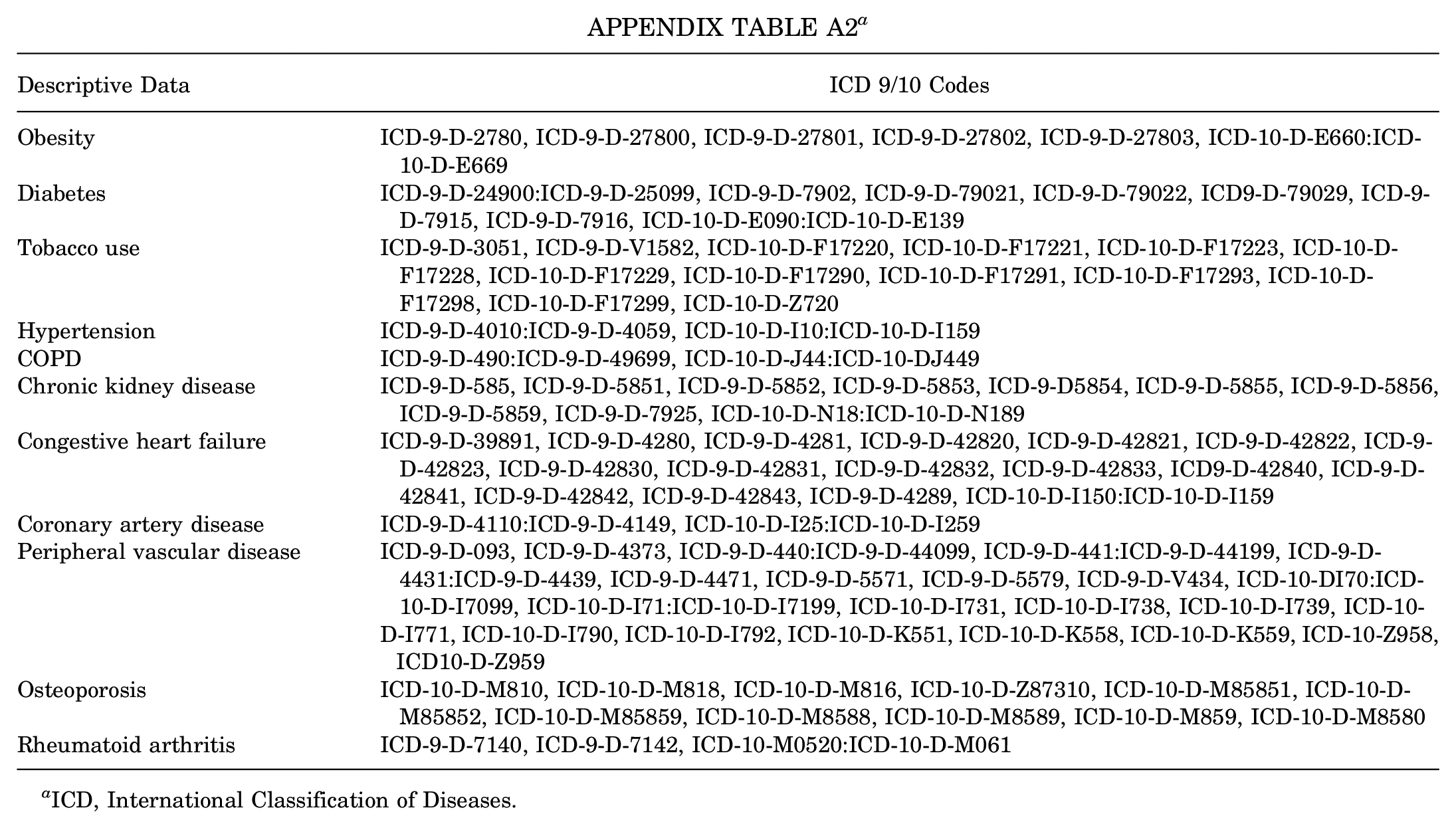
| Descriptive Data | ICD 9/10 Codes |
|---|---|
| Obesity | ICD-9-D-2780, ICD-9-D-27800, ICD-9-D-27801, ICD-9-D-27802, ICD-9-D-27803, ICD-10-D-E660:ICD-10-D-E669 |
| Diabetes | ICD-9-D-24900:ICD-9-D-25099, ICD-9-D-7902, ICD-9-D-79021, ICD-9-D-79022, ICD9-D-79029, ICD-9-D-7915, ICD-9-D-7916, ICD-10-D-E090:ICD-10-D-E139 |
| Tobacco use | ICD-9-D-3051, ICD-9-D-V1582, ICD-10-D-F17220, ICD-10-D-F17221, ICD-10-D-F17223, ICD-10-D-F17228, ICD-10-D-F17229, ICD-10-D-F17290, ICD-10-D-F17291, ICD-10-D-F17293, ICD-10-D-F17298, ICD-10-D-F17299, ICD-10-D-Z720 |
| Hypertension | ICD-9-D-4010:ICD-9-D-4059, ICD-10-D-I10:ICD-10-D-I159 |
| COPD | ICD-9-D-490:ICD-9-D-49699, ICD-10-D-J44:ICD-10-DJ449 |
| Chronic kidney disease | ICD-9-D-585, ICD-9-D-5851, ICD-9-D-5852, ICD-9-D-5853, ICD-9-D5854, ICD-9-D-5855, ICD-9-D-5856, ICD-9-D-5859, ICD-9-D-7925, ICD-10-D-N18:ICD-10-D-N189 |
| Congestive heart failure | ICD-9-D-39891, ICD-9-D-4280, ICD-9-D-4281, ICD-9-D-42820, ICD-9-D-42821, ICD-9-D-42822, ICD-9-D-42823, ICD-9-D-42830, ICD-9-D-42831, ICD-9-D-42832, ICD-9-D-42833, ICD9-D-42840, ICD-9-D-42841, ICD-9-D-42842, ICD-9-D-42843, ICD-9-D-4289, ICD-10-D-I150:ICD-10-D-I159 |
| Coronary artery disease | ICD-9-D-4110:ICD-9-D-4149, ICD-10-D-I25:ICD-10-D-I259 |
| Peripheral vascular disease | ICD-9-D-093, ICD-9-D-4373, ICD-9-D-440:ICD-9-D-44099, ICD-9-D-441:ICD-9-D-44199, ICD-9-D-4431:ICD-9-D-4439, ICD-9-D-4471, ICD-9-D-5571, ICD-9-D-5579, ICD-9-D-V434, ICD-10-DI70:ICD-10-D-I7099, ICD-10-D-I71:ICD-10-D-I7199, ICD-10-D-I731, ICD-10-D-I738, ICD-10-D-I739, ICD-10- D-I771, ICD-10-D-I790, ICD-10-D-I792, ICD-10-D-K551, ICD-10-D-K558, ICD-10-D-K559, ICD-10-Z958, ICD10-D-Z959 |
| Osteoporosis | ICD-10-D-M810, ICD-10-D-M818, ICD-10-D-M816, ICD-10-D-Z87310, ICD-10-D-M85851, ICD-10-D-M85852, ICD-10-D-M85859, ICD-10-D-M8588, ICD-10-D-M8589, ICD-10-D-M859, ICD-10-D-M8580 |
| Rheumatoid arthritis | ICD-9-D-7140, ICD-9-D-7142, ICD-10-M0520:ICD-10-D-M061 |
ICD, International Classification of Diseases.
Final revision submitted March 9, 2025; accepted March 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: W.M.H. has received consulting fees from Smith & Nephew and Vericel; travel and lodging from Smith & Nephew; and food and beverage from Smith & Nephew and Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.