
Abstract
Objective
The objective of this study was to determine whether there are significant differences in terms of indications, techniques, patient variables, and objective and subjective outcome scores as a function of the geographic locale of published studies of knee articular cartilage surgery.
Methods
An electronic database search was performed of clinical studies evaluating knee articular cartilage procedures from 2000 to 2021. Studies were separated into global regions (Europe, Asia, North America, and South America) based on the study country. All cartilage-based treatments in each region were recorded. Patient age and sex, mechanism of injury, cartilage lesion size and location, follow-up time, failure rate, and knee outcome scores utilized were summarized and compared by region.
Results
A total of 2,923 studies were analyzed. Eighty level 1 and 2 studies met the inclusion criteria. The majority were from Europe (n = 60), followed by Asia (n = 11), North America (n = 7), and South America (n = 2). The majority of procedures in European and North American studies were cell-based and marrow-stimulation procedures. In Asian studies, the most common procedures were marrow-stimulation, experimental, and biologic procedures as defined by the authors. Asian countries had a higher proportion of females (P < 0.001) and an overall older patient population (P < 0.001). Regional variation was also seen in terms of lesion location, mechanism of injury, and failure rate.
Conclusion
Most high-level evidence for articular cartilage-based procedures of the knee comes from European countries. These studies vary by patient age and sex, anatomic location, and mechanism of injury. Global variation should be taken into consideration when interpreting and applying studies of knee articular cartilage surgery.
Keywords
Introduction
Articular cartilage injuries are present in 60% to 66% of knees undergoing arthroscopy.1-4 Focal full-thickness chondral defects have a prevalence of 4.2% to 6.2% among all patients undergoing knee arthroscopy and up to 36% in athletes.1-4 Focal articular cartilage defects can negatively affect the lives of patients and have been shown to impair quality of life as much as patients with severe osteoarthritis. 5 Articular cartilage injuries have limited regenerative capacity in adults, and thus, have been implied as a potential risk factor for the development of osteoarthritis.6-9 Given the limited capacity of articular cartilage defects to heal, there has been considerable research dedicated to the development of the optimal method to surgically treat these lesions.8,10
Several surgical and non-surgical techniques have been shown to be beneficial in treating articular cartilage injuries, and their success has led to an increase in the utilization of these techniques over the last 20 years.10,11 Variables that may influence how articular cartilage defects are treated include patient age, activity level, lesion size, concomitant pathology, mechanical alignment, and comorbidities.10-12 These variables have led to debate in the literature over the optimal method to treat these injuries, which has led to an evolution in how these lesions are managed.13,14
A variety of societal factors, particularly cultural and economic, may influence how articular cartilage lesions are treated in different parts of the world. Prior studies have evaluated surgical trends for management of articular cartilage injuries within specific countries.10,15,16 However, to our knowledge, no study has assessed the management of these injuries as a function of global region.11,13,14 It is important to understand regional differences as they may be an important source of selection bias in clinical studies evaluating the treatment of articular cartilage defects. Economic factors may preclude certain techniques that are more costly in favor of less expensive options. Surgeon training and experience in some parts of the world may also limit the number times a specific surgical technique is utilized irrespective of the perceived success of the procedure. Finally, cultural mores or religious restrictions may prevent the use of allograft tissue that is unique to certain populations worldwide.13,17 Therefore, the purpose of this systematic review was to determine whether differences exist in the preferred techniques used to surgically treat articular cartilage defects of the knee across different regions around the globe and secondarily if there are regional differences in patient demographics, mechanism of injury, cartilage defect anatomical location, outcome scores utilized, and failure rates of cartilage-based procedures. It was our hypothesis that global variation would exist as exemplified by the published literature from different regions.
Methods
A systematic review was performed following best practices as established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 18 An electronic search was performed on April 1, 2021, by a medical librarian using a combination of keywords and controlled vocabulary in Embase.com, Ovid Medline, Scopus, Cochrane Central Register of Controlled Trials (CENTRAL), and Clinicaltrials.gov. Search terms included “articular cartilage,” “chondral injury,” “osteochondral,” “osteochondral allograft,” “osteochondral autograft,” “autologous chondrocyte implantation,” “matrix-associated chondrocyte implantation,” “microfracture,” “chondroplasty,” “stem cells,” “platelet rich plasma,” and “bone marrow aspirate concentrate.”
Only human clinical studies published between 2000 and 2021 were considered irrespective of the primary language of the publication. A total of 2,923 results were found. Forty-seven duplicate records were deleted after using the de-duplication processes described in “De-duplication of database search results for systematic reviews in EndNote,” 4 resulting in a total of 2,876 unique citations included in the project library.
Inclusion criteria included published clinical studies with level 1 and 2 evidence for the surgical and non-surgical treatment of focal articular cartilage injuries of the knee diagnosed by either magnetic resonance imaging (MRI) or arthroscopy of all languages. Level 1 studies were high-quality randomized, prospective trials with greater than 80% follow-up. 19 Level 2 studies included lower-quality randomized, prospective trials (i.e., less than 80% follow-up) and non-randomized prospective cohort studies. 19 Level 3 to 5 studies, abstracts, case reports, studies investigating osteoarthritis, animal studies, basic science studies, studies evaluating post-operative rehabilitation protocols, and studies reporting techniques without meaningful data were excluded (Figure 1). Anatomic location of the chondral lesions, when reported, were categorized as either “femoral condyle,” which included the medial femoral condyle (MFC) and lateral femoral condyle (LFC), “patellofemoral,” which included the trochlea and patella, and “tibial plateau,” which included the medial tibial plateau (MTP) and lateral tibial plateau (LTP). Abstracts of the 2,876 articles were reviewed by 2 authors (RGS and JJG) for inclusion in the systematic review; 80 articles were found to satisfy the inclusion and exclusion criteria.
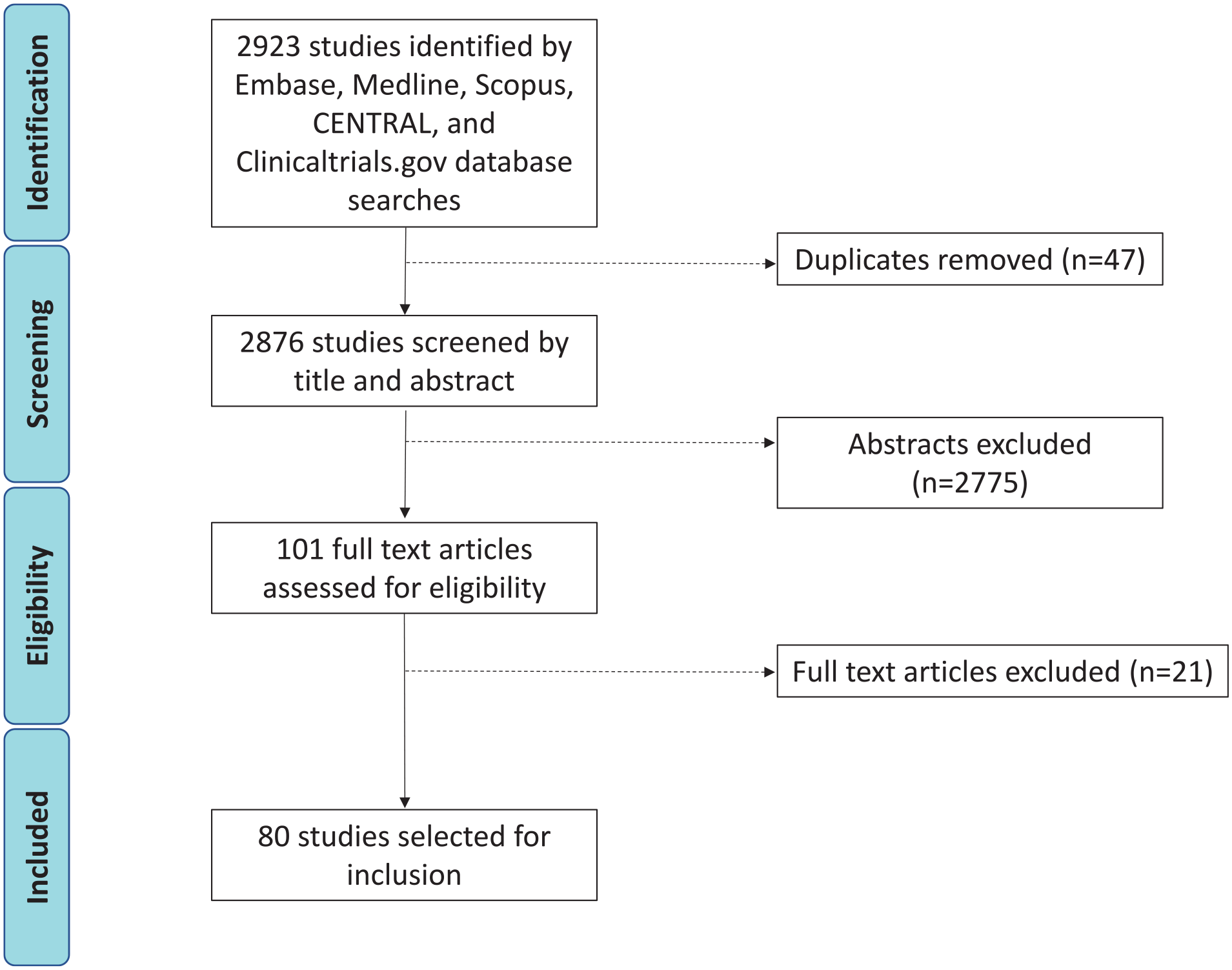
Flow diagram of article review.
Statistical Analysis
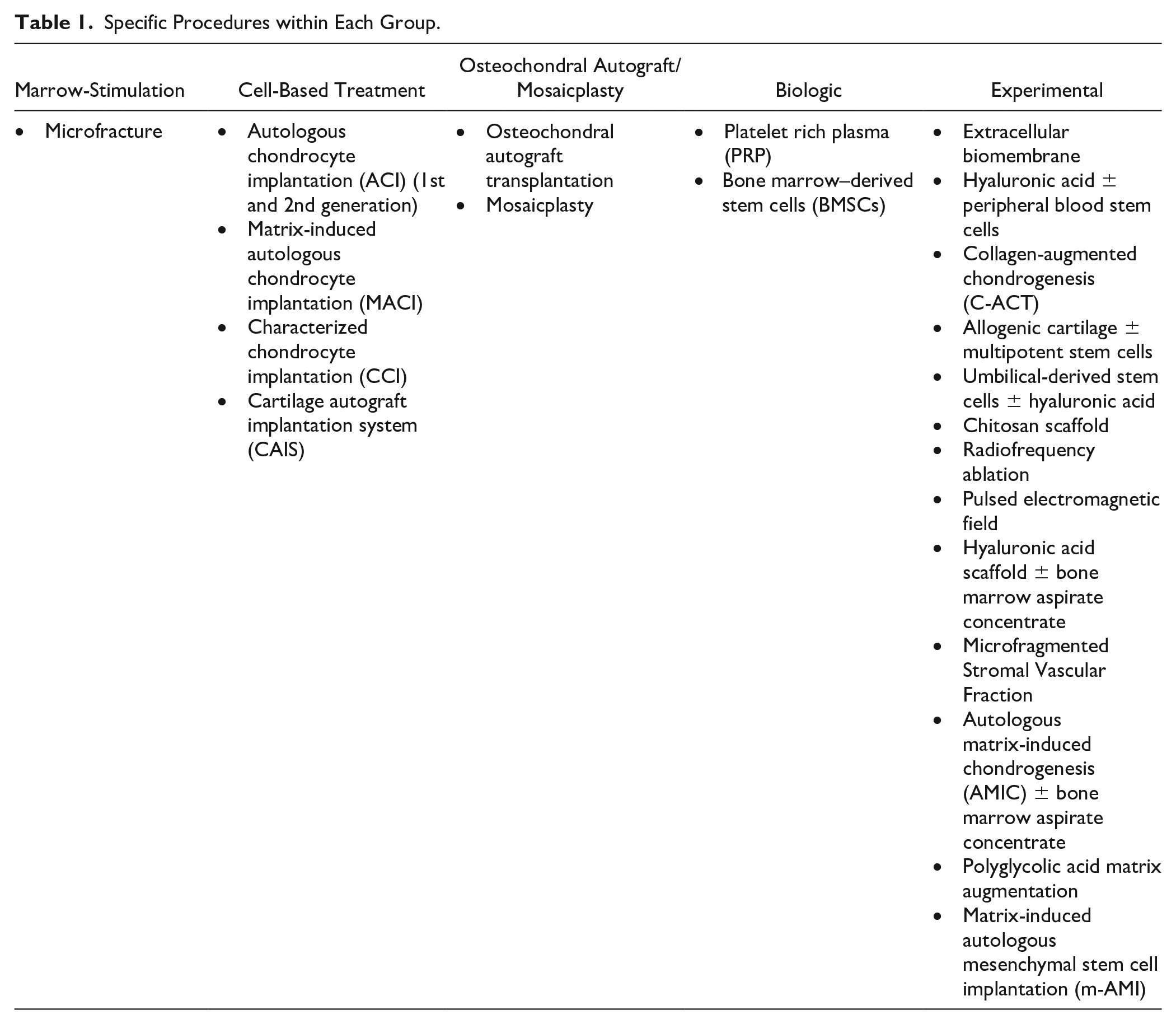
Each manuscript was evaluated and a summation of results was performed based on the country of origin. Data were extracted by 2 authors (RGS and JJG) and verified by the first author, and any discrepancies were resolved by a third author (RHB). The countries in which the studies were performed were documented, and the studies were classified into 4 regions: Europe, Asia, North America, and South America. Each specific procedure was categorized as either “cell based,” “marrow stimulation,” “osteochondral autograft/mosaicplasty,” “biologic,” and “other/experimental” ( Table 1 ). Age, duration of follow-up, body mass index (BMI), and lesion size summary statistics were all evaluated with 1-way analysis of variance. Intergroup differences in age were evaluated with the Student t test. Overall and intergroup differences in sex, mechanism of injury, and location of the lesion(s) were evaluated with the chi-square test. All statistical analyses were performed with Microsoft Excel software (Microsoft, United States).
Specific Procedures within Each Group.
Results
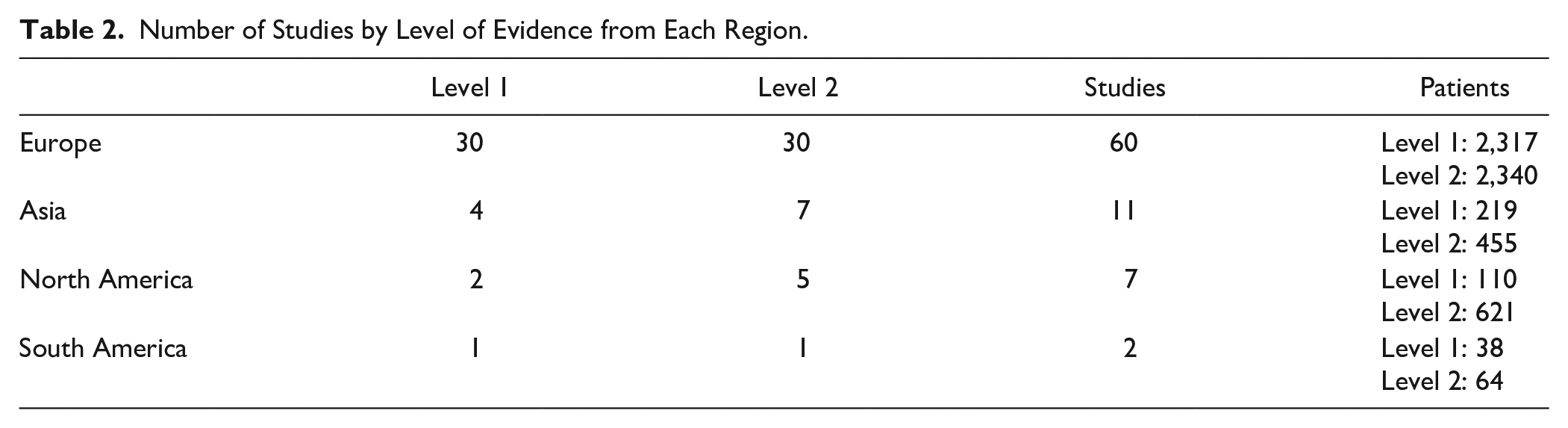
Eighty studies were included in this systematic review (Suppl. Table S1). The majority of the studies were from Europe, followed by Asia, North America, and South America ( Table 2 ). There were similar numbers of level 1 and 2 studies, with slightly more level 2 studies, overall. The number of patients included in studies from each respective region is shown in Table 2 .
Number of Studies by Level of Evidence from Each Region.
Procedures by Region
The specific types of procedures varied by global region ( Table 3 ). The 2 most common procedures evaluated in European countries were cell based (66.7% of studies) and marrow stimulation (56.7% of studies). In Asian countries, the 3 most common procedures evaluated were marrow stimulation (81.8% of studies), experimental (63.6% of studies), biologic (36.4% of studies). In North America, cell-based procedures (85.7% of studies) and marrow stimulation (42.9%) were the 2 most common treatment forms evaluated. In South America, which included only 2 total studies, there was an equivalent number of cell-based (50% of studies), marrow-stimulation (50% of studies), osteochondral autograft/mosaicplasty (50% of studies), and biologic procedures (50% of studies).
Procedures by Region.
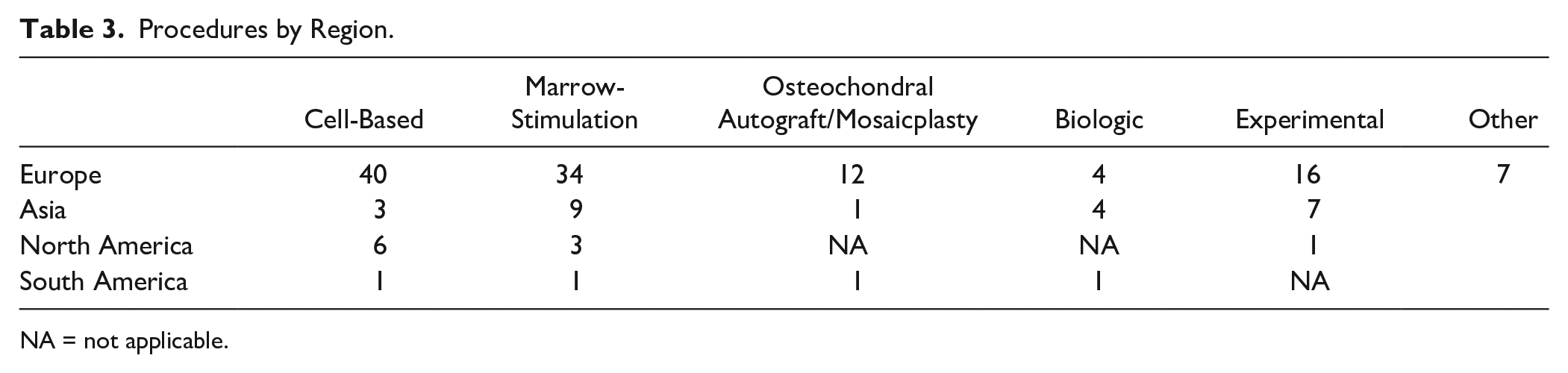
NA = not applicable.
Demographics by Region
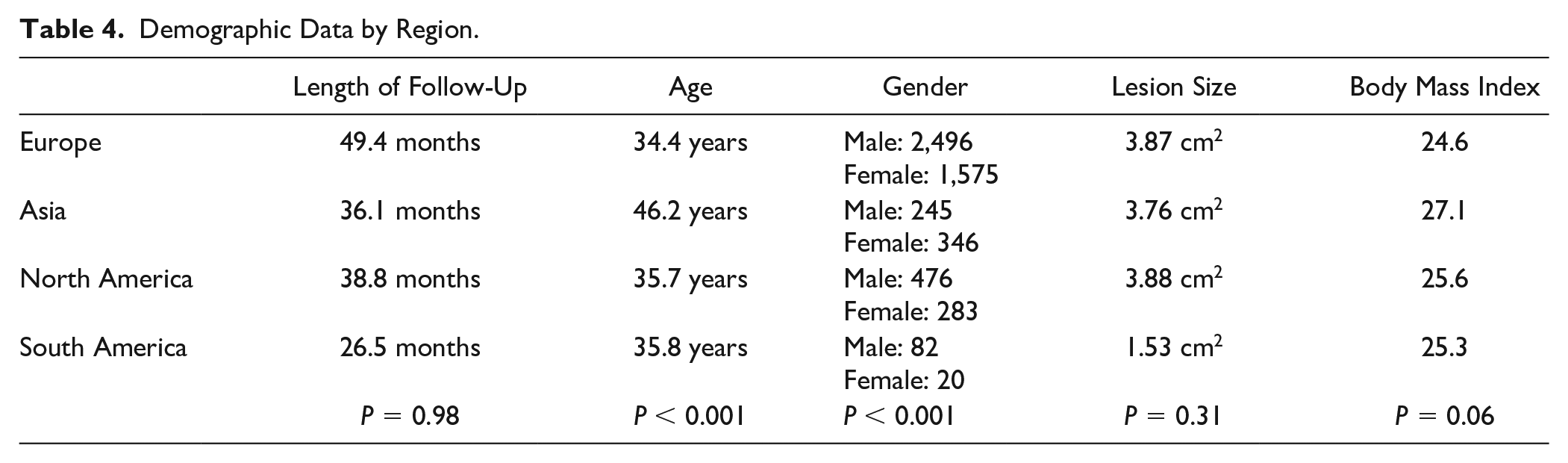
Males were more commonly evaluated in all global regions except in the Asian countries (P < 0.001) ( Table 4 ). Mean patient age in all studies was similar with no differences in European (34.4 years), North American (35.7 years), and South American (35.8 years) studies; however, studies from Asian countries had a significantly older patient population with an average age of 46.2 years (P < 0.001) ( Table 4 ). Follow-up time, BMI, and lesion size were similar between regions ( Table 4 ).
Demographic Data by Region.
Anatomic Location of Chondral Defect by Region
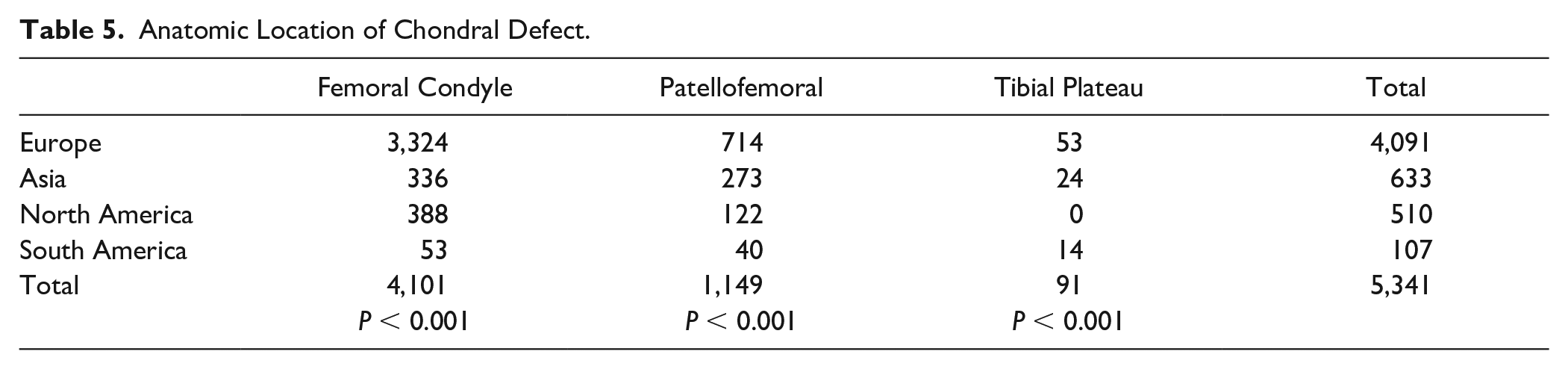
Specific lesion location was reported in 83% of the European studies, 63.6% of the Asian studies, 85.7% of the North American studies, and 100% of the South American studies. The most common anatomic locations evaluated were femoral condyle (medial and lateral), followed by patellofemoral (trochlea and patella) and tibial plateau (medial and lateral) ( Table 5 ). Interestingly, there was significant overall and intergroup differences in lesion location between all global regions (P < .05). For example, Asian studies show a higher percentage of patellofemoral lesions when compared with European, North American, and South American studies. In addition, multiple anatomic locations of chondral defects were noted in 20% of European studies, 28.6% of Asian studies, 66.7% of North American studies, and 50% of South American studies.
Anatomic Location of Chondral Defect.
Mechanism of Chondral Lesion by Region
Reporting of the mechanism of cartilage injury was poor among all 4 global regions and was provided by 55% of European studies, 54.5% of Asian studies, 57.1% of North American studies, and 0% of South American studies. In those studies that reported mechanism of cartilage injury, both European and North American countries listed more traumatic mechanisms (71% and 58.1%, respectively) than Asian countries (10.3%). Asian studies reported a much higher percentage of degenerative lesions (89.7%) than European and North American studies (16.7% and 41.9%, respectively). Intergroup analysis showed significant differences between each group analyzed in regard to the mechanism of cartilage injury ( Table 6 ). Osteochondritis dissecans (OCD) was only evaluated in studies from European countries.
Mechanism of Chondral Injury.

Outcome Scores Utilized by Region
The most common subjective and objective outcome measures used in the European and Asian countries were the International Knee Documentation Committee (IKDC) score (40% and 63.6%, respectively), Knee Injury and Osteoarthritis Outcome Score (KOOS) (40% and 55%, respectively), visual analog scale (VAS) (30% and 45.5%, respectively), Tegner activity scale (30% and 27.3%, respectively), and Lysholm knee scores (26.7% and 45.5%, respectively). South American countries most commonly used the IKDC (100%), VAS (50%), Tegner activity scale (50%), and Lysholm knee scores (50%). North American countries varied the most in outcome scores used, which included the SF-36 (71.4%), Modified Cincinnati Knee Rating System (42.9%), KOOS (42.9%), IKDC (42.9%), and Western Ontario and McMaster Universities Arthritis Index (WOMAC) (28.6%). When evaluating the top 5 most commonly used outcome scores listed for each country, the only one that was significantly different in terms of utilization between the 4 global regions was the SF-36 (P < .001).
Failures of Cartilage Procedures by Region
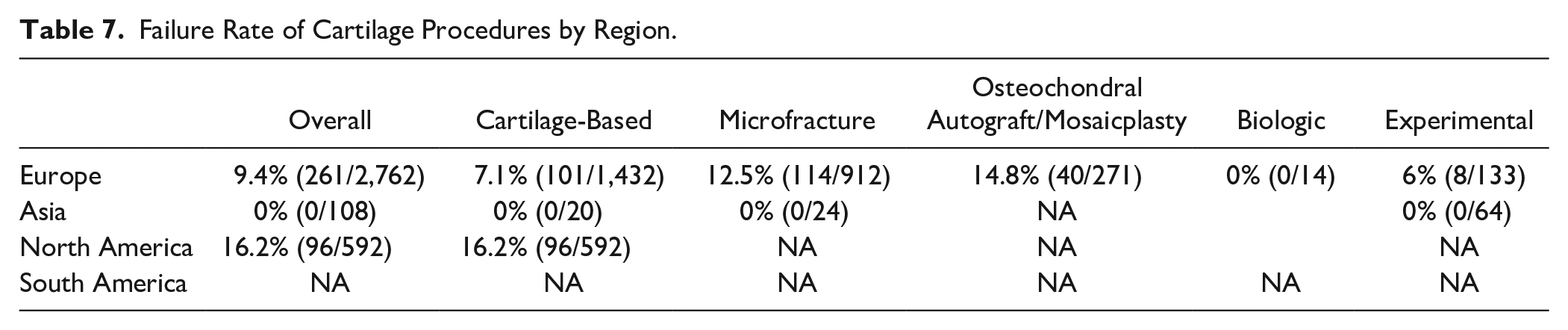
Clinical failures in our systematic review were determined by the criteria for each respective study, and this was reported in 70% of European, 27% of Asian, 57% of North American, and 0% of South American studies. The overall failure rate and failure rate among specific procedural groups are shown in Table 7 , with North American countries showing the highest failure rate among the 3 global regions (16.2%).
Failure Rate of Cartilage Procedures by Region.
Discussion
Articular cartilage injuries in the knee are very common, having been shown to be present in up to 66% of patients undergoing knee arthroscopy, which means they will likely be encountered by surgeons treating knee injuries.1-4 Management of these injuries continues to evolve as new technology is developed. Thus, it is not surprising that the number of articular cartilage procedures performed in the knee has grown at an annual rate of 5% from 2004 to 2011. 11 Despite the rapid evolution of surgical techniques, the vast majority of studies analyzing these procedures are of a lower level of evidence (i.e., levels 3-5).10,11,14 As a result, the optimal management of these lesions continues to be debated. The debate may be influenced by global differences in the preference of one procedure over another, which may be based on economic factors and/or lack of access to grafts, for instance, in the Asian-Pacific region, there are far fewer commercial tissue banks available as compared with North America. 17 In addition, it has been shown that non-commercial tissue banks may have “processing costs” which may be charged to patients or institutions and could potentially limit the use of allograft tissue. 17 Ethical cultural and religious factors must be taken into consideration as well as some populations are more likely to be accepting of tissue donation based on their beliefs which could influence the regional variation in cartilage injury treatment.13,17
This systematic review found that the majority of level 1 and 2 studies evaluating articular cartilage procedures of the knee have originated from European countries, with a majority of these studies evaluating cell-based therapy and marrow stimulation. Similarly, the majority of level 1 and 2 studies originating in North America predominantly involved cell-based therapies. In contrast, the majority of level 1 and 2 studies originating in Asian countries evaluated more experimental, biologic, and marrow-stimulation procedures. There was also a significant difference in the anatomic location of chondral lesions between studies across the 4 global regions. Differences were also noted in sex and age distribution, with a higher proportion of females and older patients included in studies from Asian countries. This finding should be considered when assessing potential articular cartilage treatments as both older age and female sex have been shown to negatively influence outcomes following articular cartilage surgery.15,20
Although the mechanism of chondral injury was poorly reported across all 4 global regions, a difference was found between all regions reporting them, with a higher number of degenerative cases being reported in Asian countries and while the majority of European studies reported the treatment of OCD lesions. Differences in injury mechanism may play a role in the treatment of these injuries as degenerative lesions are more likely in an older patient population whereas traumatic and OCD lesions are most commonly seen in younger patients; therefore, this information can be beneficial for physicians treating specific patient populations with cartilage injuries. For example, if treating an older patient with degenerative cartilage lesions, studies from Asian countries may be more applicable, whereas younger patients with traumatic or OCD lesions fit the patient profile of European and/or North American studies. Future studies should report the mechanism of cartilage injury as this may be important information when assessing and comparing outcomes. No differences were seen in the length of follow-up, BMI, cartilage lesion size, or location. However, overall failure rate was higher in North American countries when compared with other countries.
Although there have been no studies, to our knowledge, evaluating articular cartilage management based on geographic location, other studies have shown regional differences in various orthopedic procedures.16,21-27 Although not specifically looking at regional differences, there have been studies which evaluated trends in cartilage-based procedures in the United States.11,14,24 In the United States, microfracture and chondroplasty are the most common treatment for chondral injuries, especially in middle-aged patients, while osteochondral autograft/allograft and autologous chondrocyte implantation (ACI) are more common in younger patients. 24 Since 2003 in the United States, there has been a paradigm shift in favor of more complex articular cartilage procedures being performed compared with less complicated marrow-stimulation procedures based on the surgical practice of American Board of Orthopaedic Surgery (ABOS) Part II candidates. 14
There are limitations to this study, which should be mentioned. There was inconsistent reporting of all variables in the studies included from the 4 global regions, which could have influenced the outcomes evaluated. In addition, the number of studies from each region varied widely, which makes comparison between the regions difficult and could confound outcomes of this review. Although we included searches in all languages, it is possible that some studies could have been overlooked if they were not included in our database searches. Although the data extraction was not performed in a blinded fashion, 2 independent reviewers reviewed and extracted the data which was then verified by the first author and no discrepancies needed to be resolved by a third author. In addition, several patients in the various studies underwent concomitant procedures which was difficult to control for when evaluating the outcomes of interest; however, it is possible these concomitant procedures could affect the outcomes of cartilage-based procedures. We did not investigate the correlation between patient and/or defect characteristics and the choice of technique nor compare outcomes between reparative, such as bone marrow stimulating techniques, and restorative methods, such as cell- or tissue-based treatments. Finally, the mere fact that certain procedures were more common in each global region does not necessarily imply that those same procedures are performed preferentially by the majority of surgeons in that region. It is unclear to what extent clinical studies evaluating a particular surgical procedure from a region represent a proxy for the total number of procedures performed in that region.
This systematic review of level 1 and 2 studies evaluating articular cartilage procedures for the knee found that the majority of studies come from European countries followed by Asian countries, North American countries, and South American countries, respectively. European and North American countries included more cell-based and marrow-stimulation procedures, whereas Asian countries exhibited a higher proportion of experimental, biologic, and marrow-stimulation procedures. There were geographic differences in the anatomic location of the chondral injuries, mechanism of injury, patient age and sex distribution in the studies originating in the 4 global regions with studies from Asian countries reporting a higher proportion of older patients and female patients. While the cause of these differences is unclear, these global differences should be considered when interpreting studies of articular cartilage surgery in the knee and using them to guide treatment of specific patient populations.
Supplemental Material
sj-docx-1-car-10.1177_19476035221098169 – Supplemental material for Global Variation in Studies of Articular Cartilage Procedures of the Knee: A Systematic Review
Supplemental material, sj-docx-1-car-10.1177_19476035221098169 for Global Variation in Studies of Articular Cartilage Procedures of the Knee: A Systematic Review by R. Garrett Steinmetz, J. Jared Guth, Matthew J. Matava, Matthew V. Smith and Robert H. Brophy in CARTILAGE
Footnotes
Authors’ Note
The study was completed at the Washington University School of Medicine in St. Louis, MO.
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MJM—Speaker for Elite/Arthrex; Educational activity Elite/Arthrex; Consulting Pacira Pharmaceutical and Heron Therapeutics. MVS—Speaker for Elite/Arthrex; Consulting Flexion Therapeutics.
Ethical Approval
This study was exempt from IRB approval.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.