
Abstract
Background:
Severe osteoarthritis (OA) has been identified as a risk factor for inferior outcomes following high tibial osteotomy (HTO).
Purpose:
To investigate the effectiveness of HTO in patients with advanced OA, particularly those with Kellgren-Lawrence (KL) grade 4 (KL4), and to compare clinical outcomes based on OA severity and the effect of postoperative alignment in each group.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective review was conducted on patients who underwent biplanar medial opening-wedge HTO from 2010 to 2022, with a follow-up period of 2 to 5 years. Patients were divided into 2 groups based on preoperative KL grades: non-KL4 and KL4. Clinical outcomes were compared using patient-reported outcome (PRO) measures: pain visual analog scale (VAS), Lysholm Knee Score, and Knee injury and Osteoarthritis Outcome Score (KOOS) between the groups. Subgroup analyses were conducted to ascertain whether outcomes differed based on postoperative weightbearing line (WBL) ratio within each group.
Results:
Out of 324 patients, 141 were eligible: 110 in the non-KL4 group and 31 in the KL4 group, with a mean follow-up of 37.5 months (overall mean age, 56.9 years; mean body mass index, 26.9 kg/m2). Baseline demographics were similar between the groups. The KL4 group had more severe preoperative conditions (larger defect size and more varus). However, both groups showed significant improvements in PROs (P < .001), with no significant differences between them. In the KL4 group, patients with a postoperative WBL ratio ≥62.5% showed better scores in certain PRO measures, while other PRO data showed no significant differences (VAS: 17.1 ± 19.1 vs 33.9 ± 18.3, P = .03; KOOS Activities of Daily Living subscale: 78.7 ± 9.9 vs 69.3 ± 13.8, P = .04). In contrast, the non-KL4 group showed no difference in PROs based on WBL ratio. In the KL4 group, the final VAS was most correlated with the WBL ratio (r = −0.545; P = .002). A WBL ratio of 62.2% to 67.3% was the cutoff value to predict the achievement of low residual pain (VAS < 18; median of KL4 group) in KL4 patients.
Conclusion:
HTO can yield comparable clinical outcomes in KL4 OA patients to those with lower-grade OA. However, achieving sufficient valgus alignment (WBL ratio > 62.2%-67.3%) correlates with less residual pain in the short- to midterm follow-up in high-grade OA patients.
Keywords
High tibial osteotomy (HTO) is an established treatment option for young and active patients with medial compartment osteoarthritis (OA) and varus deformity, showing good short- to long-term outcomes.19,35,38 However, as with most of orthopaedic surgeries, achieving satisfactory outcomes for all patients is not always possible, and certain risk factors are associated with poor postoperative results.3,4 Clinical outcomes after HTO can vary based on the baseline severity of OA.5,24,34,42 In patients with severe OA, intra-articular deformity and soft tissue laxity, represented by increased joint line convergence angle (JLCA), may result in inconsistent coronal alignment corrections, leading to suboptimal results.27,30,32,37 Additionally, the severe OA itself, including complex lesions such as meniscal degenerative tears and diffuse cartilage defects, is associated with inferior outcomes5,24,34,42 and decreased long-term survival.4,44 Several studies have reported that patients with preoperative severe OA, particularly evaluated as Kellgren-Lawrence (KL) grade 4 (KL4), 21 tend to have low satisfaction scores 42 and decreased survival after HTO. 24
However, the results from previous studies are based on outcomes achieved through corrections toward specific, consistent targetalignments set for a group of patients by an individual surgeon.5,24,34,42 The optimal targetalignment for HTO remains debatable. 18 The classic targetalignment is set at the Fujisawa point, 8 which corresponds to 62.5% of the weightbearing line (WBL) ratio, or approximately 3° to 5° of valgus. 2 In contrast, near-neutral or less valgus alignment has also been recommended recently based on laboratory and short-term clinical study results.1,27,29 There is also a perspective that targetalignment should be adjusted based on the severity of OA or cartilage defects.7,12 Some studies empirically suggested adjusting targetalignment according to the depth of medial cartilage defects 12 or individual targetalignment based on various conditions, including severity of OA or meniscal status.7,39 However, this approach still lacks sufficient evidence.
This study aims to analyze how clinical outcomes differ based on the severity of OA, specifically KL4 OA. Additionally, we seek to determine whether the effect of postoperative alignment on clinical outcomes differs based on the severity of OA. Our hypothesis is that patients with KL4 OA will have generally inferior outcomes compared with non-KL4 patients and that postoperative alignment will significantly influence outcomes more in KL4 patients than in non-KL4 patients.
Methods
This retrospective study included patients who underwent medial open-wedge HTO (MOWHTO) between March 2010 and April 2022 at 2 centers by a single senior surgeon (S.-H.K.). The inclusion criteria were as follows: patients who underwent unilateral MOWHTO for medial compartment OA without concomitant femoral osteotomy, with a minimum follow-up of 2 to 5 years. Because the main purpose of this study was to determine whether clinical outcomes differ depending on the severity of OA, patients with factors that could affect clinical outcomes, except for the severity of OA, were excluded. The exclusion criteria included (1) varus coronal alignment 1 year after the MOWHTO on whole lower-extremity radiographs (WBL ratio < 50%), 6 (2) excessively valgus-corrected coronal alignment (WBL ratio ≥ 75%), 23 (3) previous knee ligament surgery or injuries, (4) previous surgical history in the ipsilateral limb, (5) complications after MOWHTO (eg, saphenous nerve injury, nonunion after hinge fracture), (6) severe ipsilateral limb pain due to other pathology that renders accurate assessment of the patient-reported outcomes (PROs) (eg, lumbar radiculopathy), and (7) no follow-up PROs after >2 years. Indications for MOWHTO were as follows: (1) relatively young age (<65 years) and active patients with medial knee pain refractory to nonoperative treatment for ≥3 months, (2) medial compartment OA with varus deformity (mechanical tibiofemoral angle [mTFA] > 5°), and (3) a relatively good range of motion (arc of motion > 100° and flexion contracture < 15°) without joint instability.
Included patients were divided into 2 groups based on the KL grade: non-KL4 group and KL4 group.Comparative analysis was performed between the 2 groups (Figure 1). This study was approved by the institutional review board of our institution. Due to the retrospective nature of the study and the minimal risk involved, patient consent was waived by the institutional review board.

Patient flow diagram. ACL, anterior cruciate ligament; KL, Kellgren-Lawrence grade; MCL, medial collateral ligament; PCL, posterior cruciate ligament; WBL, weightbearing line.
Surgical Procedure and Postoperative Rehabilitation
All surgical procedures of biplanar MOWHTO were performed by a single senior orthopaedic surgeon. Diagnostic arthroscopy was conducted before MOWHTO. The meniscal lesions were evaluated, and combined procedures were performed if necessary or planned (partial meniscectomy, subtotal meniscectomy, meniscus posterior root repair). Meniscus posterior root repair combined with HTO was performed over a short period (November 2019 to June 2020). The size, grade, and extent of the cartilage lesions were evaluated. Combined cartilage procedures were considered for focal cartilage defects, assessed as contained lesions with vertical shoulders on the cartilage edges.17,31,40 For uncontained, extensive arthritic cartilage lesions, isolated HTO without cartilage procedures was generally preferred. However, cartilage procedures were performed in select cases at the patient’s request. Following the arthroscopic evaluation and procedures, biplanar MOWHTO was performed. The target point of correction was 62.5% (Fujisawa point). 28 The required correction angle was planned using the Miniaci method on whole lower extremity standing anteroposterior (AP) radiographs. 41 A longitudinal skin incision of approximately 6 to 8 cm was made midway between the tibial tuberosity and the posteromedial border of the proximal tibia, starting approximately 2 cm below the joint line and extending to the pes anserinus area. The proximal attachment of the pes anserinus tendon was partially detached and distally retracted by a temporary suture during surgery. The superficial medial collateral ligament was released or transected using previously described methods. 14 For the transverse osteotomy, 2 parallel guidewires were inserted from the anteromedial cortex approximately 40 mm below the joint line, advancing obliquely toward the fibular tip. 15 The transverse osteotomy plane was directed to the upper one-third of the distance between the fibular tip and the circumferential line of the fibular head, which was identified as a safe zone in previous studies. 33 The transverse osteotomy was performed with an oscillating saw. Complete osteotomy of the tibial posterior cortex to the hinge point was performed with caution to avoid an externally rotated hinge axis and to minimize increasing of the posterior tibial slope. 15 Vertical osteotomy was performed to the tibial tuberosity for the proximally oriented biplanar osteotomy, angled 110° from the transverse osteotomy. 15 After the osteotomy, medial opening was achieved with an adjustable spreader. Once the desired gap opening was achieved, a TomoFix plate (Synthes) and screws were used to rigidly fix the osteotomy site. When a correction of ≥10° was performed, an allogenous chip bone graft was applied to the osteotomy gap.
Routine rehabilitation protocols after MOWHTO were as follows: patients were instructed to begin crutch-assisted ambulation with partial weightbearing after surgery. Passive range of motion exercises began 2 days postoperatively with a hinged knee brace, starting at 60° and increasing by 30° every 2 weeks. After 6 weeks, patients discontinued crutches and the knee brace. For those with a combined cartilage repair procedure or meniscus root repair, weightbearing was initially more restricted. Weightbearing was restricted for 4 weeks with crutches, followed by partial weightbearing for an additional 6 weeks. Passive range of motion exercise was emphasized using a continuous passive motion machine to promote early cartilage healing. At the 1-year follow-up visit, bony union was confirmed via radiographs, and plate removal was performed approximately between 1 year and 1.5 years postoperatively, considering symptoms of irritation from the plate and the potential for future arthroplasty conversion. 25 During plate removal, second-look arthroscopy was conducted, with patient consent, to assess the overall condition of the knee after MOWHTO.
Clinical and Radiographic Assessment
Clinical outcomes were assessed using several prospectively collected PRO measures: a 100-point pain visual analog scale (VAS), Lysholm Knee Score, and Knee injury and Osteoarthritis Outcome Score (KOOS). Preoperative PROs and PROs at the final follow-up, ranging from 2 to 5 years, were retrospectively reviewed. The minimal clinically important differences (MCIDs) for each PRO were based on previous related studies: VAS, 27 13 ; Lysholm score 10.1 13 ; KOOS Pain, 15.4; KOOS Symptoms, 15.1; KOOS Activities of Daily Living, 17; KOOS Sport/Recreation, 11.2; and KOOS Quality of Life, 16.5. 11 The MCID achievement rate for each PRO was evaluated. 13
Preoperative KL grade was assessed using standing AP and Rosenberg view knee radiographs, with the worse radiograph between the 2 being used for grading. Preoperative and postoperative medial proximal tibia angle (mPTA), JLCA, and joint line obliquity (JLO) angle were evaluated on standing whole lower extremity AP radiographs taken preoperatively and at 1 year postoperatively by previously described methods.16,46 Lateral opening was denoted as a positive value for JLCA, and lateral inclination of the joint line was denoted as a positive value for JLO. Preoperative and postoperative mechanical alignment was also evaluated using the mTFA and the WBL ratio measurement (medial edge of tibial plateau, 0%) on standing whole lower extremity AP radiographs taken preoperatively and at 1 year postoperatively.16,36 Varus was denoted as a negative value for mTFA. All radiographic parameters were measured by 2 orthopaedic surgeons (S.-H.J. and H.J.) twice, with ≥3-week intervals between measurements, using a picture archiving and communication system (Centricity PACS Viewer; GE Healthcare Co).
Statistical Analysis
All statistical analyses were performed using SPSS Version 26.0 (IBM), with statistical significance set at P < .05. Continuous variables were presented as mean ± SD, and categorical variables as number (percentage) unless otherwise indicated. The primary purpose of this study was to compare the PROs between the non-KL4 and KL4 groups.Comparisons between the groups were performed using an independent t test or Mann-Whitney U test, depending on the results of the normality test (Shapiro-Wilk test). Categorical variables from the 2 groups were compared using chi-square tests. Pearson correlation tests were conducted to analyze the correlation between each PRO and the WBL ratio in each group.For subgroup analysis, the non-KL4 and KL4 groups were further divided into groups with WBL ratios above and below 62.5%. The PROs of the subgroups with WBL ratios above or below 62.5% were compared between the groups. Logistic regression analysis was performed to identify the factors affecting the rates of achievement of favorable PROs. Receiver operating characteristic curve analysis was utilized to determine the cutoff value for the WBL ratio to ensure low residual pain. Intraclass correlation coefficients were used for intra- and interobserver reliabilities of the measurements for radiographic parameters. Post hoc power analysis was conducted using G*Power (Version 3.1.9.4; Universität Düsseldorf) to calculate the statistical power of the study’s significant results.
Results
A total of 324 patients were retrospectively reviewed in this study. On the basis of inclusion and exclusion criteria, 141 patients were selected and divided into 2 groups: non-KL4 (110 patients) and KL4 group (31 patients). The mean follow-up period was 37.5 months and did not differ between the groups. Baseline demographic characteristics were not different between the groups (Table 1). On baseline evaluations, the KL4 group had significantly larger medial femoral condyle cartilage defects, higher preoperative JLCA, and more preoperative varus (P < .001; P < .001; P = .007). Postoperatively, JLCA and mPTA showed differences between the groups (P = .002; P = .006); however, postoperative alignment did not show a significant difference (Table 1). Intraobserver reliability for WBL ratio was 0.994 (95% CI, 0.984-0.998), and 0.856-0.948 for other radiographic measurements (mTFA, JLCA, mPTA, and JLO). Interobserver reliability for WBL ratio was 0.989 (95% CI, 0.969-0.996) and 0.796-0.899 for other radiographic measurements, showing good to excellent intra- and interobserver reliability.
Demographic and Baseline Characteristics of the 2 Groups a

Values are presented as mean ± SD or n (%). Boldface values indicate statistical significance (P < .05). JLCA, joint line convergence angle; JLO, joint line obliquity; KL, Kellgren-Lawrence; MFC, medial femoral condyle; mPTA, medial proximal tibial angle; mTFA, mechanical tibiofemoral angle; WBL ratio, weightbearing line ratio.
Varus angle was denoted as a negative value.
Lateral opening was denoted as a positive value for JLCA.
Lateral inclination of the joint line was denoted as a positive value for JLO.
Both groups showed significant improvement in PROs at the final follow-up compared with preoperative PROs (all PROs, P < .001). The KL4 group demonstrated no significant difference in PROs or improved PROs compared with the non-KL4 group (Table 2). The MCID achievement rates for each PRO also did not differ between the groups. None of the included patients underwent total knee arthroplasty conversion.
Final and Improved Patient-Reported Outcomes and Comparison Between the Non-KL4 and KL4 Group a
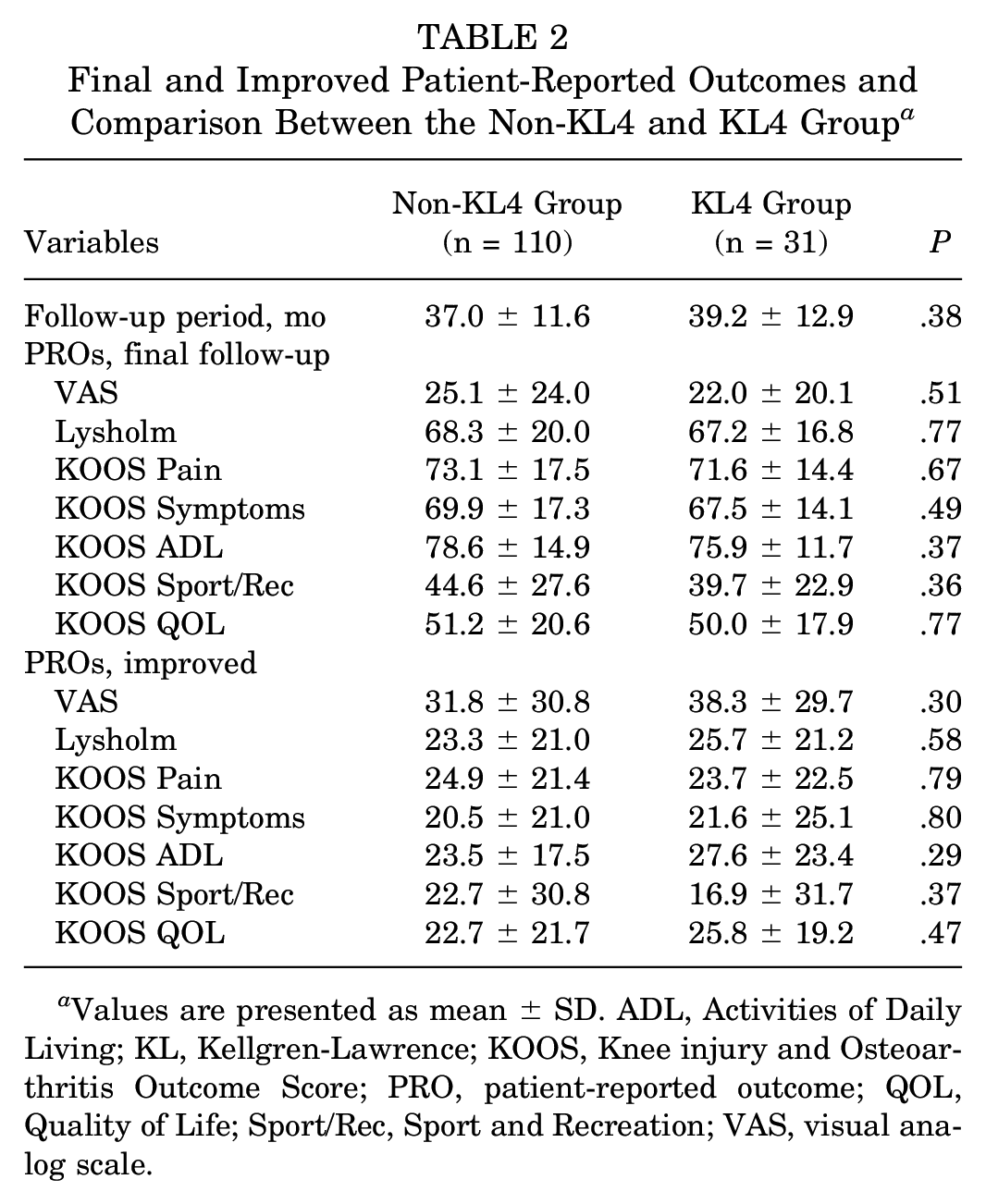
Values are presented as mean ± SD. ADL, Activities of Daily Living; KL, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QOL, Quality of Life; Sport/Rec, Sport and Recreation; VAS, visual analog scale.
Subgroup Analysis of KL4 Group
In the KL4 group, patients were divided into 2 subgroups based on a WBL ratio of 62.5%, with 10 patients in the <62.5% group and 21 in the ≥62.5% group.Follow-up period did not differ between these subgroups (36.8 ± 12.0 vs 40.1 ± 13.3 months; P = .52) (Figure 2). There were no significant differences in age, body mass index (BMI), or preoperative WBL ratio between the subgroups (age: 58.2 ± 12.5 vs 55.6 ± 4.5 years, P = .55; BMI, 25.9 ± 3.1 vs 26.9 ± 5.0 kg/m2, P = .56; preoperative WBL ratio: 17.8% ± 11.2% vs 11.3% ± 12.4%, P = .19). However, the postoperative WBL ratio differed significantly (P < .001), with means of 58.5% ± 3.7% for the <62.5% group and 68.3% ± 3.5% for the ≥62.5% group, respectively. In the KL4 group, patients who achieved postoperative WBL ratio ≥62.5% demonstrated better VAS and KOOS ADL scores compared with those with a WBL ratio <62.5%, while no significant differences were found in the other PROs (VAS: 17.1 ± 19.1 vs 33.9 ± 18.3, P = .03; KOOS ADL: 78.7 ± 9.9 vs 69.3 ± 13.8, P = .04) (Figure 2). MCID achievement rate for KOOS QOL was significantly higher when WBL ratio was ≥62.5% than when WBL ratio was <62.5% in the KL4 group (P = .02). However, in the non-KL 4 group, PROs did not differ based on the WBL ratio (Figure 2). Statistical power for significant results ranged from 0.81 to 0.84, with the highest power observed in the comparison of VAS between WBL ratio ≥62.5% and <62.5% groups in the KL4 group.

(A) PROs based on a WBL ratio ≥62.5% or <62.5% in KL4 patients at final follow-up.The KL4 group included 10 patients in the <62.5% group and 21 in the ≥62.5% group, with follow-up periods of 36.8 ± 12.0 and 40.1 ± 13.3 months, respectively. (B) PROs based on WBL ratio in non-KL4 patients at final follow-up.The non-KL4 group included 39 patients in the <62.5% group and 71 in the ≥62.5% group, with follow-up periods of 36.1 ± 12.4 and 37.5 ± 11.2 months, respectively. In the KL4 group, patients with a postoperative WBL ratio ≥62.5% demonstrated better VAS and KOOS ADL scores compared with those with a WBL ratio <62.5%, but no significant differences were observed in the other PROs. However, PROs did not differ based on the WBL ratio in the non-KL4 group.ADL, Activities of Daily Living; Imp, improved; KL, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; QOL, Quality of Life; VAS, visual analog scale; WBL, weightbearing line. Asterisk indicates statistical significance.
In Pearson correlation tests, correlations between some PROs and the WBL ratio were higher in the KL4 group, showing a coefficient r value of 0.358 to 0.545 in the KL4 group, compared with 0.195 to 0.210 in the non-KL4 group (Table 3). In the KL4 group, the final postoperative VAS (residual pain) was the most correlated PRO with the WBL ratio (r = −0.545; P = .002). The statistical power of the Pearson correlation test between the VAS and WBL ratio was calculated to be 0.95. Receiver operating characteristic curve analysis revealed that a WBL ratio of 62.2% to 67.3% was the cutoff value that best predicted the achievement of low residual pain (VAS < 18; median of KL4 group) in KL grade 4 patients (area under curve, 0.796) (Figure 3).
Correlation Between the Postoperative Weightbearing Line Ratio and Patient-Reported Outcomes (PROs) at Final Follow-up in Each Group (Non-KL4 Group and KL4 Group) a

Boldface values indicate statistical significance (P < .05). ADL, Activities of Daily Living; KL, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; Sport/Rec, Sport and Recreation; VAS, visual analog scale.
The most correlated.
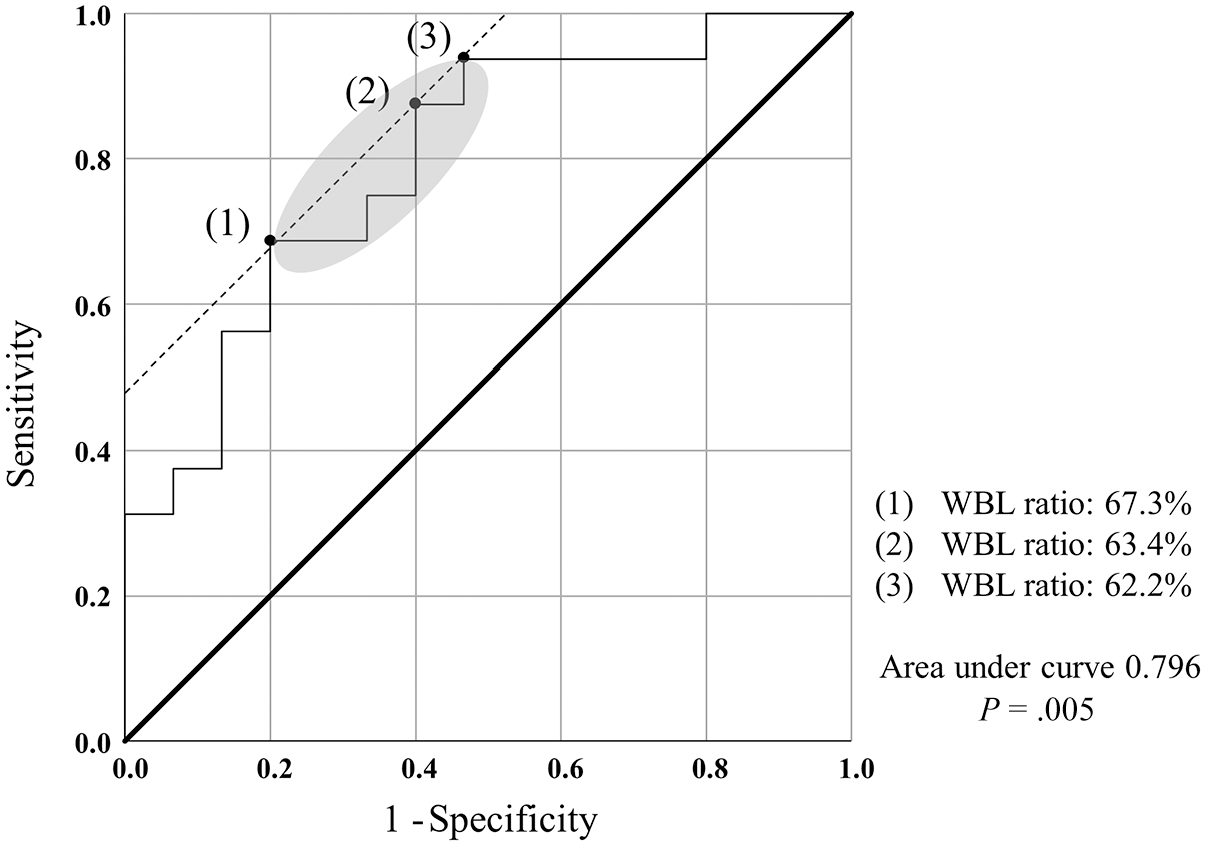
Receiver operating characteristic curve analysis of weightbearing line (WBL) ratio to predict residual pain lower than 18 in KL4 patients (n = 31). Three points were identified as showing similar Youden index (sensitivity + specificity − 1): (1) 67.3% (2) 63.4% (3) 62.2%. A WBL ratio of 62.2%-67.3% was determined to be the cutoff value to predict the achievement of low residual pain in KL grade 4 patients (area under curve, 0.796; P = .005).
Discussion
The principal finding of this study is that the KL4 group did not exhibit significantly inferior outcomes in the mid- to short-term follow-up compared with the non-KL4 group.This suggests that HTO can be an effective treatment even for patients with KL4. However, when analyzing the relationship between postoperative alignment, represented by the WBL ratio, and clinical outcomes within each group, a stronger correlation was found in the KL4 group.In the KL4 group, the WBL ratio was most closely associated with the final VAS score for residual pain. A postoperative WBL ratio between 62.2% and 67.3% predicted a low residual pain VAS of ≤18.
The relationship between OA severity and clinical outcomes after HTO has been frequently studied in previous research.3-5,24,34,42-44 Preoperative severity of OA is reported to be associated with clinical outcomes and long-term survival,4,5,34,43,44 with the most severe form, KL4 OA, identified as a significant risk factor.24,42 However, our study results indicate that KL4 patients did not exhibit inferior outcomes compared with patients with less severe OA in short- to midterm follow-up.This contrast with previous studies could be explained by one of our principal findings: the correlation between the WBL ratio and clinical outcomes in the KL4 group.In this study cohort, a large portion of patients in both the KL4 (70.9%) and the non-KL4 (67.2%) groups achieved a postoperative WBL ratio above the classic alignment target of 62.5%. Within the KL4 group, patients with a WBL ratio >62.5% demonstrated significantly higher PROs compared with those with a WBL ratio <62.5%. This suggests that relatively more valgus alignment may have contributed to the noninferior outcomes observed in KL4 patients. If the target had been set to near-neutral or less valgus alignment, as recently suggested,1,29 the KL4 group might have shown inferior clinical outcomes, showing a similar trend to previous studies.24,42
There is still no consensus on the optimal targetalignment for HTO. Traditionally, Fujisawa etal 8 reported favorable results when the postoperative WBL passed through 30% to 40% of the lateral tibial plateau from the center, and this target region later became the origin of the most commonly utilized classic target point, known as the Fujisawa point (WBL ratio, 62.5%).18,28 Coventry etal 2 and Hernigou etal 10 also proposed 3° to 5° of valgus as an appropriate targetalignment, based on excellent long-term outcomes. However, more recently, there has been a shift toward favoring less valgus alignment, closer to neutral alignment, as the optimal target.1,27,29 Martay etal, 29 in their finite element model study, suggested that a WBL ratio of 62.5% excessively increases pressure in the lateral compartment, proposing 55% WBL ratio as the optimal target within a safe zone of a 50% to 60% WBL ratio. Atkinson etal 1 performed HTO in 34 patients to a near-neutral alignment (0.6°± 3.0° valgus) and demonstrated improvement in cartilage composition using 3-T magnetic resonance imaging T2 mapping, suggesting less valgus alignment as a sufficient alignment to improve cartilage. Clinically, Lee etal 26 reported that while overcorrection leads to inferior outcomes, undercorrection (WBL < 57%) and acceptable alignment result in similar clinical outcomes. Despite these studies’ results, some studies still report inferior outcomes with undercorrection and support the validity of classic alignment targets.23,45 Overall, while there is emerging support for near-neutral alignment, the debate continues, and further high-quality evidence is needed to establish the optimal targetalignment for HTO.
Another perspective suggests setting different targetalignments for each patient. This idea was initially proposed in the literature by Jakob and Jacobi, 12 who recommended adjusting the WBL ratio based on the depth of medial cartilage loss: 55% to 57.5% for one-third loss, 60%to 62.5% for two-thirds loss, and 65% to 67.5% for complete loss. Feucht etal 7 also reviewed various HTO indications nonsystematically and proposed individualized targetalignments for each indication. However, this individualized approach lacks clear evidence. 12 In the present study, although various conditions throughout HTO were not covered, a different targetalignment for severe OA patients was proposed. Clinical outcomes in KL4 patients were found to be more significantly influenced by the WBL ratio compared with other patients, and achieving a WBL ratio of 62.2% to 67.3% or higher was recommended for KL4. This approach aligns with strategies setting different targetalignments based on the degree of OA considered in previous studies7,12 but is supported by our statistical analysis, providing some scientific evidence. In this study, the clinical outcomes for the non-KL4 group did not differ whether the WBL ratio was above or below 62.5%, showing low correlations between the WBL ratio and the clinical outcomes. However, this does not imply that achieving a neutral or less valgus alignment is sufficient for patients with KL3 or less. HTO is typically performed on young, active patients, and the surgery should ensure long-term clinical outcomes.3,35 Studies that favor near-neutral alignment are mostly laboratory studies or short-term studies, which do not consider long-term varus recurrence and survival.1,20,27,29 Therefore, the durability of near-neutral alignment requires further long-term investigation.
The cutoff range of 62.2% to 67.3% derived in this study does not represent the optimal targetalignment for KL4 patients. Rather, it indicates that residual pain is reduced at WBL ratios above this range. This raises the question of whether a higher degree of valgus >67.3% would result in better outcomes. Furthermore, in this study’s subgroup analysis of the KL4 group, a WBL ratio of ≥62.5% showed statistically significant differences in only a few PROs, while most did not show significant differences. Additionally, in the correlation analysis, only the VAS demonstrated a moderate correlation. Therefore, targeting more valgus alignment should be approached with caution. Excessive overcorrection has been linked to reduced cosmetic satisfaction 9 and accelerated patellofemoral arthritis progression after HTO. 47 Theoretically, more valgus correction increases mechanical loading on the lateral compartment, which can accelerate lateral degeneration. 23 Some studies have reported that lateral compartment degeneration after HTO is associated with long-term clinical outcomes. 22 Therefore, based on the results of this study and previous reports, achieving sufficient valgus alignment for short-term relief while avoiding unnecessary overcorrection is advisable. Thus, the 62.2% to 67.3% range suggested as cutoff by this study appears to be an appropriate targetalignment in KL4 patients.
Patients with a WBL ratio <50% or >75% in this study were excluded to avoid confounding factors related to excessive under- or overcorrection, which might independently lead to inferior outcomes.6,23 These thresholds (50% and 75%) were not defined as criteria for overcorrection or undercorrection but were established to excessive over- or undercorrection that could affect outcomes. Kuriyama etal, 23 in a computer simulation study, analyzed HTO models corrected to WBL ratios of 40%, 50%, 60%, 62.5%, 70%, and 80%. They found that corrections ≤70% were acceptable, but at 80%, excessive lateral loading and abnormal contact between the medial femoral condyle and medial intercondylar eminence occurred during knee extension. This study adopted a 75% (between 70% and 80%) upper limit for excessive overcorrection based on their findings and the authors’ empirical experience. El-Azab etal 6 reported significantly inferior outcomes for WBL ratios <50%, supporting this study’s threshold for excessive undercorrection.
Based on the results of this study, HTO appears to be an effective procedure even for patients with KL4 OA. However, for KL4 OA patients, achieving postoperative valgus alignment beyond the classic targetalignment is necessary to expect low residual pain levels in short- to midterm follow-up.The strength of the present study is its uniqueness in suggesting an appropriate targetalignment range for patients with severe OA.
Limitations
This study has several limitations. First, as a retrospective study, there are inherent biases such as selection bias. Second, in studies comparing the outcomes of HTO as a treatment for OA, there are many potential confounding factors that could influence the outcomes. This study included HTO patients over an extended period, some of whom underwent additional cartilage procedures or meniscus root repairs. The heterogeneity of the cohort may have introduced confounding factors. Third, the relatively small sample size of the KL4 group poses a risk of selection bias and increases the likelihood of being underpowered. Post hoc power analysis in this study indicated some degree of underpower. Fourth, this study selected patients with a postoperative WBL ratio between 50% and 75%. Although this range was chosen based on previous studies, 23 the cutoff values for undercorrection and overcorrection that lead to inferior outcomes have not been definitively established, and there is some arbitrariness in this choice. Last, this study analyzed clinical outcomes based on a follow-up period of 2 to 5 years. The conclusions of this study will need to be confirmed through long-term studies for more definitive conclusions.
Conclusion
HTO can yield comparable clinical outcomes in KL4 OA patients to those with lower-grade OA. However, achieving sufficient valgus alignment (WBL ratio > 62.2%-67.3%) correlates with less residual pain in the short- to midterm follow-up in high-grade OA patients.
Footnotes
Final revision submitted December 16, 2024; accepted January 10, 2025.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Gangnam Severance Institutional Review Board (IRB No. 3-2024-0179).