
Abstract
Background:
Although medial open-wedge high tibial osteotomy (MOWHTO) is the treatment of choice for patients with mild to moderate osteoarthritis with varus malalignment, concerns about inferior outcomes in patients with preoperative radiological kissing lesion (RKL) remain.
Purpose:
To compare the mid- to long-term clinical and radiological results and survivorship after MOWHTO in patients with versus without preoperative RKL.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 122 knees in patients who underwent MOWHTO with a medial locked plate and had minimum 5-year follow-up data. The mean age at surgery was 55.9 years (range, 38-65 years), and the mean follow-up was 7.5 years (range, 5-12.8 years). All patients had undergone second-look arthroscopy around 2 years after MOWHTO. The knees were divided into an RKL group (n = 17) and no-RKL group (n = 105) based on preoperative standing radiographs. The authors compared postoperative American Knee Society (AKS) knee and function scores, range of motion, and improvements in AKS scores between groups, as well as hip-knee-ankle angle, medial proximal tibial angle, and joint-line convergence angle from preoperatively to postoperatively. Also compared were the degree of cartilage regeneration between first- and second-look arthroscopy and the survival rate after index surgery.
Results:
Preoperative AKS scores were significantly lower in the RKL group versus the no-RKL group (AKS knee, 79.6 ± 7.5 vs 83.8 ± 3.9, P = .037; AKS function, 68.8 ± 9.3 vs 76.0 ± 5.1, P = .006). Likewise, postoperative AKS scores were significantly lower in the RKL group versus the no-RKL group (AKS knee: 91.3 ± 4.2 vs 94.4 ± 1.6, respectively, P = .008; AKS function: 90.0 ± 10.0 vs 97.6 ± 4.5, respectively, P = .007). However, all patients had excellent postoperative AKS knee and function scores (>80). Moreover, there were no between-group differences in pre- to postoperative improvement in AKS scores, postoperative radiological changes, or grade of cartilage regeneration. The survival rates in the RKL and no-RKL groups were 100% and 97.1%, respectively (P ≥ .999).
Conclusion:
Although the latest clinical scores were lower in the RKL group than in the no-RKL group, comparable results in postoperative clinical improvement, cartilage regeneration, and survivorship were observed in patients with RKL at mid- to long-term follow-up.
Keywords
Medial open-wedge high tibial osteotomy (MOWHTO) has been commonly indicated for young and active patients with a mild to moderate degree of medial osteoarthritis (OA). 3,10 Furthermore, recent literature has reported that favorable results can be achieved with extended indications of MOWHTO because of advances in surgical techniques and fixation devices. 6,22,30,44,47 Additionally, younger age, lower body mass index (BMI), better physical activity, and earlier stage of OA are closely associated with successful outcomes in MOWHTO. 8,9,19,25
Meanwhile, we often encounter relatively younger and active patients with advanced grade of OA in whom we may hesitate to perform total knee arthroplasty (TKA), as it would be undesirable when comparing their physical activity and relatively longer life expectancy with the longevity of the artificial joint. 15,17,34,44,45 Thus, a joint-preserving surgery such as an osteotomy is a possible option despite the presence of advanced OA, such as Kellgren-Lawrence (K-L) grade 3 or 4. However, limited evidence remains for applying MOWHTO, specifically in younger and active patients with advanced OA, such as those with radiological kissing lesion (RKL). Only a few studies have reported MOWHTO in patients with RKL, with contradictory results. 35,46 Moreover, these contradictory results were mostly short- to midterm results, which might be too limited for comment on the success of MOWHTO. 35,44,46 In this regard, it would be reasonable to perform MOWHTO under select indications that include known positive predictors, if we choose MOWHTO for these patients. We performed MOWHTO in select patients with preoperative RKL after thoroughly assessing their physical and radiological conditions.
The purpose of the current study was to evaluate mid- to long-term clinical and radiological results and survivorship after MOWHTO in patients with preoperative RKL and to compare them with those in patients without RKL. In addition, we assessed the grade of cartilage regeneration after MOWHTO between the groups, based on 2-stage arthroscopy. We hypothesized that the results and survivorship of MOWHTO would not be inferior in select patients with preoperative RKL to those with no RKL at mid- to long-term follow-up.
Methods
Patient Selection and Study Design
We retrospectively reviewed a consecutive series of 152 knees that had MOWHTO with a medial locked-plate system between February 2008 and December 2015. Local institutional review board approval was obtained before the study, and the patients provided written informed consent to participate. The inclusion criteria for the current study were as follows: (1) a minimum follow-up of 5 years after MOWHTO; (2) second-look arthroscopy at the time of plate removal (around 2 years after the index operation); (3) general indication of MOWHTO; and (4) select indication of MOWHTO for patients with preoperative K-L grade 4. Our general indications for MOWHTO were as follows: (1) symptomatic medial OA K-L grade 2 or 3 with varus malalignment >5°, (2) age <70 years, (3) BMI <35 kg/m2, (4) range of motion (ROM) showing >100° of forward flexion and <15° of flexion contracture, and (5) no severe grade of patellofemoral or lateral compartment OA. In addition, in patients with preoperative RKL including K-L grade 4, MOWHTO was selectively performed in those with (1) age ≤60 years, (2) BMI <30 kg/m2, (3) hip-knee-ankle angle (HKAA) <−15°, (4) Tegner activity level ≥3, (5) osteophytes < grade 3 at the medial femoral condyle (MFC) and medial tibia plateau (MTP) based on the Osteoarthritis Research Society International's atlas, 2 (6) willingness to undergo joint-preserving osteotomy, and (7) agreement and understanding of the possibly lower success rate when compared with patients with general indications of MOWHTO.
Among the 152 knees, 26 from the no-RKL group were excluded because of follow-up loss and 4 (3 knees in the no-RKL group and 1 knee in the RKL group) were excluded because of absence of second-look arthroscopic data. Therefore, 122 knees were ultimately enrolled in the study; 17 were allocated to the RKL group and 105 were allocated to the no-RKL group (Figure 1).
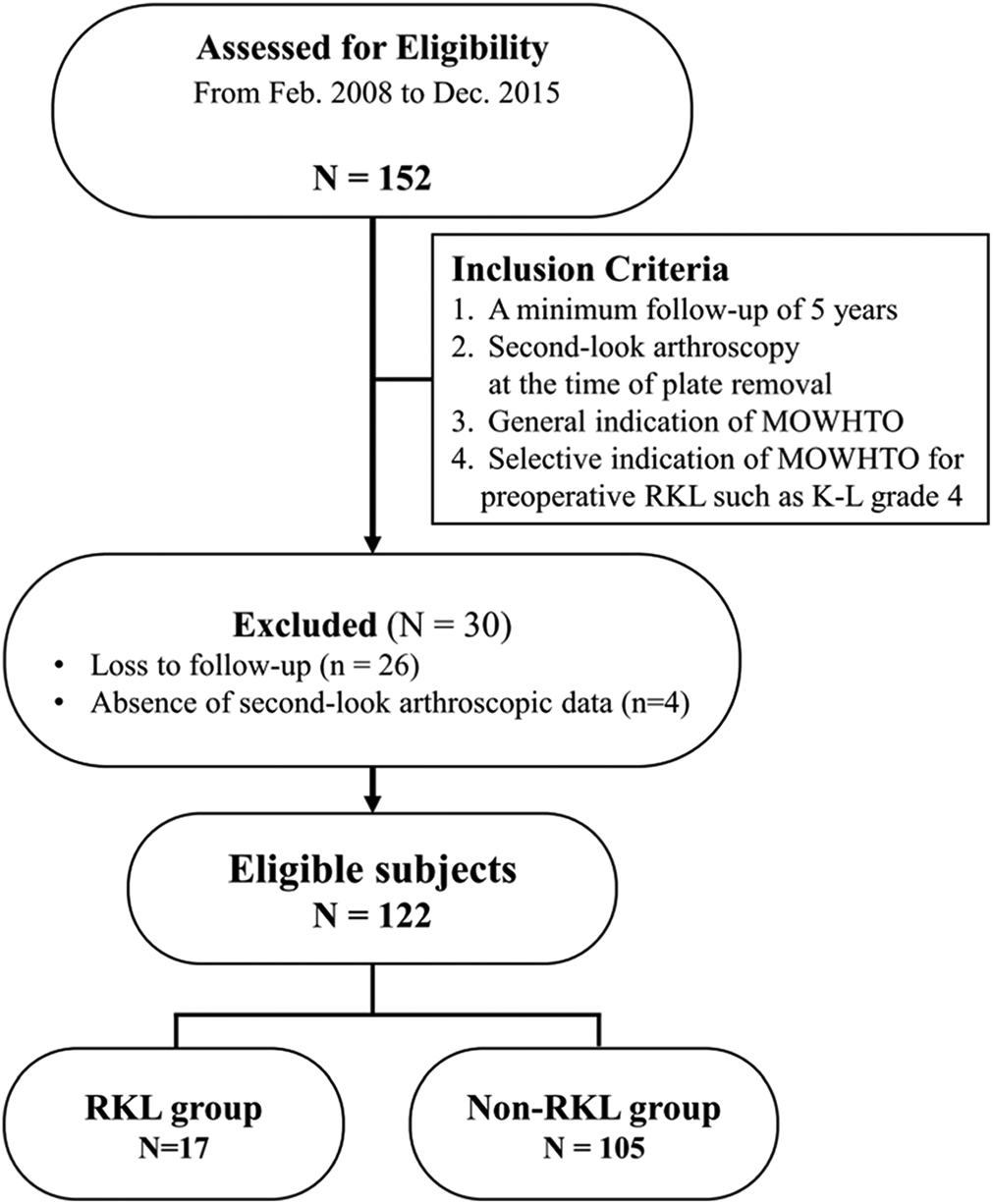
Flow diagram illustrating patient enrollment. Overall, 122 knees (80.3%) were enrolled in the current study. K-L, Kellgren-Lawrence; MOWHTO, medial open-wedge high tibial osteotomy; RKL, radiological kissing lesion.
RKL was defined as obvious bone-on-bone contact between the MFC and MTP on preoperative standing anteroposterior and lateral or Rosenberg view radiographs (Figure 2). 35,40,41,46 Defining the RKL on simple radiographs is helpful to surgeons because it is the preoperative factor for surgical indications of MOWHTO. Based on the RKL findings from radiographs, we divided the patients into RKL and no-RKL groups.
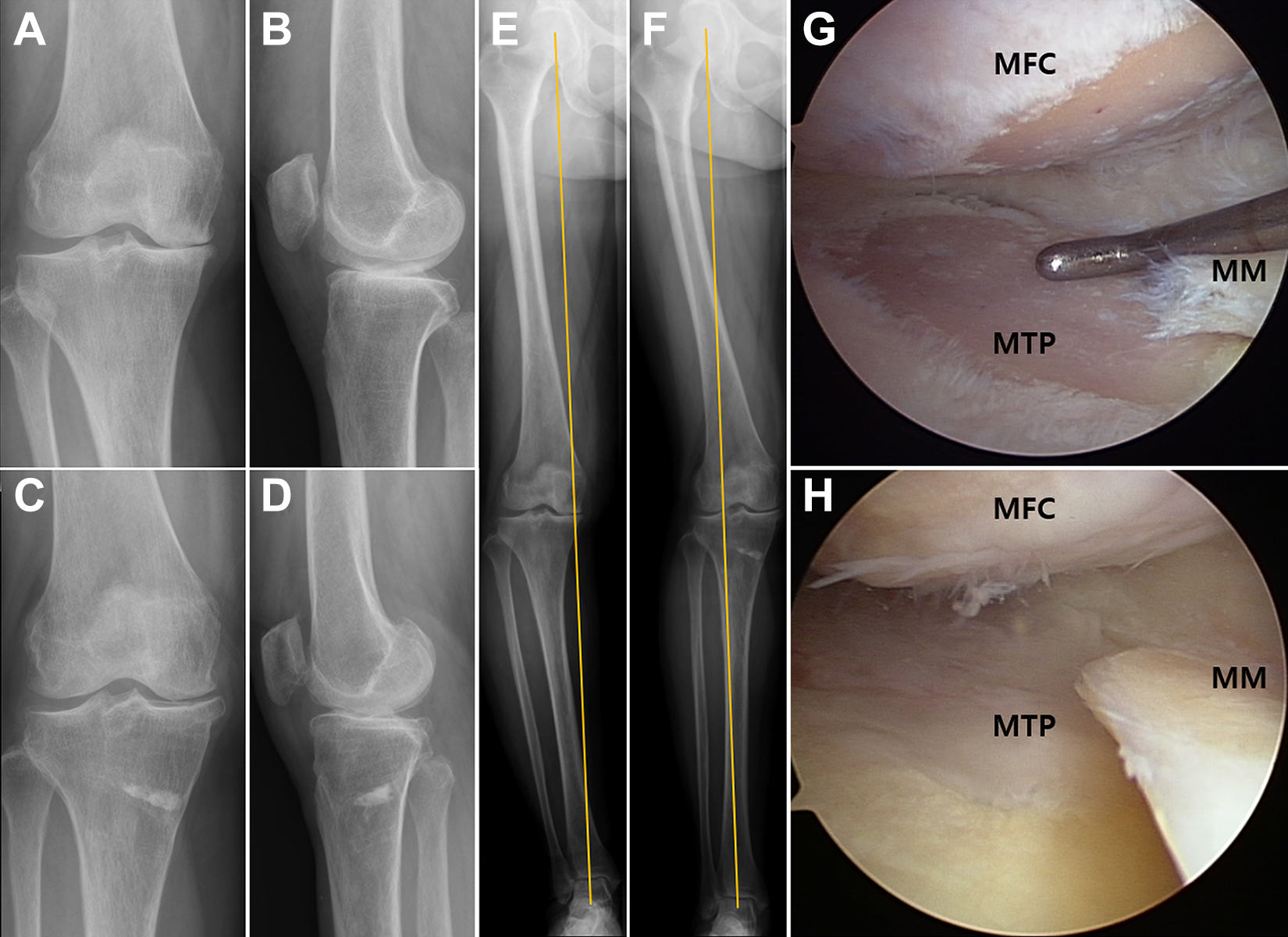
Radiological kissing lesion (RKL) in the medial compartment is shown on preoperative standing (A) anteroposterior and (B) lateral radiographs of the right knee of a 55-year-old woman. Decompressed RKL is shown on postoperative standing (C) anteroposterior and (D) lateral radiographs 7 years after medial open-wedge high tibial osteotomy (MOWHTO). (E) Preoperative varus alignment is corrected to valgus alignment and (F) maintained well 7 years after MOWHTO on lower extremity images. (G) Arthroscopic findings of cartilage status in the medial femoral condyle (MFC) and medial tibia plateau (MTP) show the exposure of subchondral bone at the time of MOWHTO. (H) Arthroscopic findings show near-total coverage of fibrous cartilage 2 years after MOWHTO without any cartilage repair procedures. MM, medial meniscus.
Surgical Technique and Rehabilitation Protocol
All the operations were performed by a senior surgeon (K.-I.K.). Arthroscopic examination was concomitantly performed at the time of MOWHTO. Cartilage status was routinely evaluated, and irrigation of debris, excision of chondral flaps without chondroplasty, and partial meniscectomy of degenerative meniscal flaps were performed. No cartilage repair procedures were performed in any of the cases. After arthroscopy, biplanar valgus osteotomy was performed using a minimally invasive technique and fixed using a medial locked plate system (TomoFix; Synthes). 30,48 Based on the arthroscopic cartilage's status, we adjusted the target to shift the mechanical axis to result in 3° to 4° valgus (weightbearing line at about 62.5% from the medial edge of the plateau) in advanced OA and to 1° to 2° valgus (weightbearing line at about 55%-60% from the medial edge of the plateau) in mild OA. 14,23,24 After fixation of the plate with locking screws, the opening gap was filled with a cancellous bone graft if the gap width exceeded 10 mm.
Passive and active ROM, quadriceps setting, straight-leg raises, and ankle pump exercises were started on the day after surgery. Partial weightbearing ambulation with crutches was initiated when the pain was tolerable. Patients were permitted to begin full weightbearing without crutches at 6 weeks postoperatively. Patients were also allowed sports activities such as jumping after 9 months according to their needs and conditions. All patients followed the same protocol.
Evaluation Criteria
Clinical assessment included recording American Knee Society (AKS) knee and function scores preoperatively and at every follow-up. 18,32 AKS knee and function scores were graded as excellent (80-100), good (70-79), fair (60-69), or poor (<60). 4,18,42 ROM was evaluated using a 30-cm plastic movable arm preoperatively and at every follow-up. 37 Preoperative and postoperative AKS scores and ROM were compared between the RKL and no-RKL groups. Improvements in the AKS scores and ROM from the preoperative value were also compared between the 2 groups. 7,49
Radiological evaluation included the HKAA (negative value indicating varus alignment), 12 medial proximal tibial angle (MPTA), 39 and joint line convergence angle (JLCA). 38 Preoperative and postoperative HKAA, MPTA, and JLCA were compared between the 2 groups. The K-L grades were assessed preoperatively and at the latest follow-up. 20
The cartilage status of the medial compartment was recorded at the first and second stages of arthroscopy based on the International Cartilage Regeneration & Joint Preservation Society grade. 31 Through 2-stage arthroscopy, the grade of cartilage regeneration after MOWHTO was classified and compared between the groups based on the macroscopic staging system by Koshino et al 27 : stage A, no regeneration; stage B, partial regeneration (such as pink fibrous tissue with or without partial coverage with white fibrocartilage); and stage C, total regeneration. Failure was defined as conversion to TKA or reoperation. Postoperative complications were also reviewed. Failures and complications were compared between the RKL and no-RKL groups. Two independent orthopaedic surgeons (J.-H.K. and S.-H.L., with 5 years' and >15 years' experience, respectively) evaluated the presence of RKL and arthroscopic findings of cartilage regeneration in a blind manner, and differences in readings were adjudicated by consensus.
Statistical Analysis
Statistical analysis was performed using SPSS software (Version 23.0; IBM Corp). Continuous data are presented as means ± SDs. All dependent variables were tested for normality of distribution and equality of variance using the Kolmogorov-Smirnov test and analyzed using parametric or nonparametric tests, as appropriate. Continuous variables were analyzed using the Student t test or Mann-Whitney U test. Categorical variables were analyzed using the chi-square or Fisher exact test. The paired t test or Wilcoxon signed-rank test was used to analyze significant changes in variables between the preoperative period and the last follow-up. Statistical significance was set at P < .05.
Intra- and interobserver reliability and reproducibility of the radiological and arthroscopic findings were assessed using the intraclass correlation coefficient (ICC), where reliability was classified as little for ICC values ≤0.25, low for 0.26-0.49, moderate for 0.50-0.69, high for 0.70-0.89, or very high for values ≥0.90. 33
Results
The mean follow-up was 7.5 years (range, 5-12.8 years). Postoperative clinical and radiological evaluations were available for 119 knees, excluding 3 knees with failure on the latest follow-up. Table 1 summarizes the overall demographic and preoperative characteristics of the patients. The ICC for the radiological and arthroscopic findings was between 0.84 and 0.96, indicating significantly high intraobserver and interobserver agreement.
Patients’ Demographic and Preoperative Characteristics a
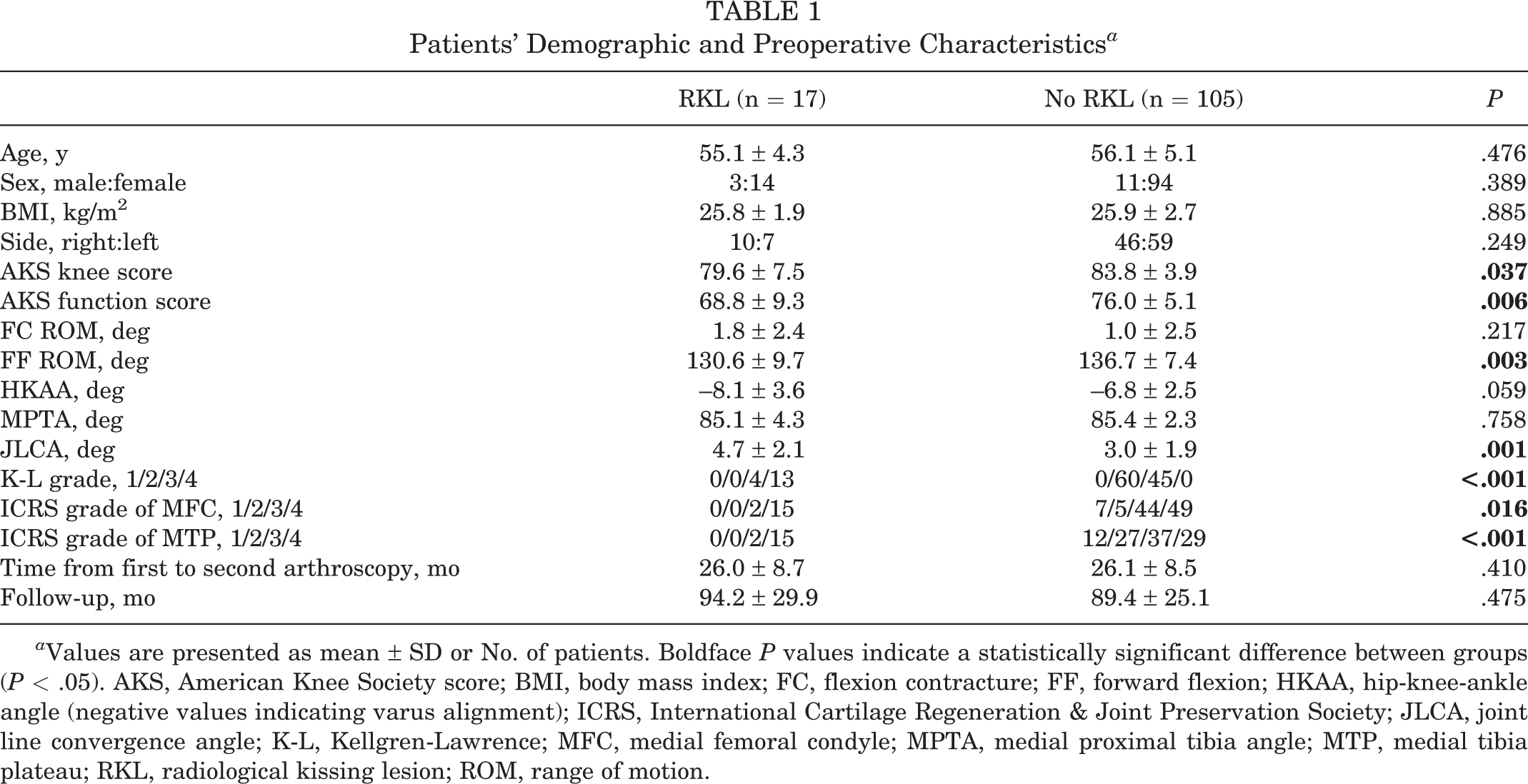
a Values are presented as mean ± SD or No. of patients. Boldface P values indicate a statistically significant difference between groups (P < .05). AKS, American Knee Society score; BMI, body mass index; FC, flexion contracture; FF, forward flexion; HKAA, hip-knee-ankle angle (negative values indicating varus alignment); ICRS, International Cartilage Regeneration & Joint Preservation Society; JLCA, joint line convergence angle; K-L, Kellgren-Lawrence; MFC, medial femoral condyle; MPTA, medial proximal tibia angle; MTP, medial tibia plateau; RKL, radiological kissing lesion; ROM, range of motion.
Outcomes
Both the RKL and no-RKL groups had significantly improved AKS scores after MOWHTO compared with their preoperative scores (P < .001). When we compared the latest AKS scores between the 2 groups, the RKL group (knee, 91.3 ± 4.2; function, 90.0 ± 10.0) had significantly lower scores than the no-RKL group (knee, 94.4 ± 1.6, P = .008; function, 97.6 ± 4.5, P = .007). However, all patients were graded “excellent” (>80) in postoperative AKS knee and function scores. Moreover, the degree of improvement in the postoperative AKS knee and function scores from the preoperative values was similar between the RKL and no-RKL groups (Table 2). No significant difference was found between the 2 groups in the postoperative ROM or the degree of change in ROM from the preoperative values. Regarding the radiological assessments, no differences were observed in postoperative HKAA, MPTA, and JLCA between the 2 groups (Table 3). The degree of cartilage regeneration by macroscopic staging assessment through 2-stage arthroscopy showed no significant difference between the RKL and no-RKL groups (Table 4).
Clinical Outcomes Between the Groups a

a Values are presented as mean ± SD or No. of patients (%) unless otherwise indicated. 3 knees of failure cases were excluded in the analysis of postoeprative outcomes. Boldface P values indicate a statistically significant difference between groups or between pre- and postoperative values (P < .05). AKS, American Knee Society score; FC, flexion contracture; FF, forward flexion; post, postoperative; pre, preoperative; RKL, radiological kissing lesion; ROM, range of motion. Dashes indicate not applicable.
Postoperative Radiological Outcomes Between the Groupsα

αValues are presented as mean ± SD unless otherwise indicated. 3 knees of failure cases were excluded in the analysis of postoeprative outcomes. Boldface P values indicate a statistically significant difference between groups or between pre- and postoperative values (P < .05). HKAA, hip-knee-ankle axis; JLCA, joint line convergence angle; K-L, Kellgren-Lawrence; MPTA, medial proximal tibial angle; post, postoperative; pre, preoperative; RKL, radiological kissing lesion.
Stage of Regeneration of Articular Cartilage Based on 2-Stage Arthroscopic Findings a

a Values are presented as No. of patients (%). RKL, radiological kissing lesion.
Survivorship and Complications
The overall survival rate was 97.5% after MOWHTO at an average of 7.5 years of follow-up. No significant difference was observed in survival rates between the 2 groups (RKL, 100%, No RKL, 97.1%; P ≥ .999). (Table 5). Failure was found in 3 knees within the no-RKL group: 2 patients underwent revision MOWHTO because of early collapse of the opening gap, and 1 patient underwent TKA conversion at 7 years postoperatively for OA progression. One patient within the no-RKL group had late hematogenous infection 15 months postoperatively after dental treatment; the patient was treated with plate removal and debridement.
Postoperative Failure and Infection Between the Groups a

a Values are presented as No. of patients (%). MOWHTO, medial open-wedge high tibial osteotomy; RKL, radiological kissing lesion.
Discussion
The principal finding of the current study is that comparable results were shown in select patients with RKL in postoperative clinical improvements, radiological outcomes, and survivorship after MOWHTO at mid- to long-term follow-up. Moreover, the degree of cartilage regeneration through 2-stage arthroscopy was also comparable between the 2 groups at the 2-year follow-up.
RKL on the standing radiograph implies bone-on-bone contact resulting from cartilage denudation in the weightbearing zone, indicating an advanced degree of medial OA. 1,20 Generally, joint replacement has been the preferred treatment for patients with RKL since unsatisfactory results from extensive cartilage loss at the weightbearing portions are expected after joint-preserving operations. 11,43 However, in relatively younger and active patients with RKL, high rates of revision and unsatisfactory performance of artificial joints have been reported, making surgeons hesitant to perform joint replacement in this cohort. 5 Therefore, joint-preserving surgery can be selectively performed in these patients considering their physical activity, life expectancy, and implant longevity. 43,44,46 Moreover, many studies have acknowledged that younger and physically active patients with lower BMI were related to successful MOWHTO. 8,9,16,21,29 Therefore, we performed MOWHTO in select patients with RKL if they met the criteria based on previous studies, 8,9,16,21,29 such as younger age (≤60 years), low BMI (<30 kg/m2), nonsevere varus deformity (HKAA <15°), and fair physical activity (Tegner score ≥3). In addition, such patients, who had a strong desire and will to preserve their joints at least a few years rather than undergo joint replacement, selectively underwent MOWHTO. On the basis of the theoretical advantages of MOWHTO, we assumed that similar satisfactory results to those seen in patients with no RKL could be obtained in patients with RKL after MOWHTO by decompressing the excessive focal stress from the collision of MFC and MTP with the achievement of postoperative valgus alignment. 35
Limited evidence and controversy still exist regarding the clinical and radiological outcomes of MOWHTO in patients with RKL. 35,46 Recent studies reported short-term clinical outcomes of MOWHTO concomitantly with microfracture in patients with preoperative RKL; however, their clinical results were contradictory. 35,46 In addition, Schuster et al 43 reported favorable mid- to long-term clinical and radiological results in patients with advanced OA after MOWHTO; however, they also performed concomitant chondral resurfacing procedures and had no control group (case series). Thus, the result of the comparative study after purely performing MOWHTO in this cohort is still questionable. We evaluated the mid- to long-term clinical and radiological results after MOWHTO without additional chondral treatments in both the RKL and the no-RKL groups. Our results showed that postoperative AKS scores were significantly lower in the RKL group than in the no-RKL group at the latest follow-up. Meanwhile, preoperative AKS scores were also significantly lower in the RKL group, which seems reasonable considering the difference in the severity of OA between the 2 groups. Therefore, the difference in postoperative AKS scores between the 2 groups could be a result of the difference in preoperative AKS scores between the groups. Moreover, the postoperative mean AKS score was more than 90 points, and all patients had excellent-grade AKS scores even in the RKL group. In addition, the postoperative improvement in AKS scores from the preoperative values showed no significant difference between the 2 groups. Accordingly, our results indicated that comparable effectiveness of MOWHTO, such as the ability to improve clinical scores from the preoperative value, could be obtained in both the RKL and the no-RKL groups. It may be postulated that a great effectiveness of MOWHTO could be applicable to patients with RKL, with such select indications. Therefore, joint-preserving MOWHTO could be a viable option for select patients with RKL to postpone or avoid joint replacement surgery.
A recent meta-analysis investigated the survivorship of MOWHTO at 5 and 10 years and found pooled survival rates of 95.1% (95% CI, 93.1%-97.1%) and 91.6% (95% CI, 88.5%-94.8%), respectively 22 . In our study, a survival rate of 97.5% was reported at the average follow-up of 7.5 years after MOWHTO in a series of 122 patients, representing excellent survivorship compared with previous studies. 22,43 A long-term study 43 reported a survival rate of 81.7% at a mean follow-up of 10 years after MOWHTO with K-L grades 3 and 4. Notably, none of the RKL groups had failure after MOWHTO in the current study. In our cohort, 2 patients in the no-RKL group had early fixation failure and subsequently underwent revision MOWHTO, and only 1 patient had a conversion to TKA at 7 years postoperatively. Based on our survivorship, we could cautiously recommend the MOWHTO to select patients with RKL to delay the need for a subsequent TKA.
Limitations
There were several limitations to this study. First, it had a retrospective design with a small number of cases in the RKL group. Moreover, different indications were applied to each cohort, which might be selection bias. However, limited evidence exists to confidently recommend MOWHTO for patients with RKL with a thorough and comprehensive explanation of possible inferior outcomes. Thus, including only a relatively small number of cases in RKL with select indications was inevitable because of a lack of evidence. We expect that the results of our study will contribute to the establishment of high-level evidence with adequate cases in the future. Second, female predominance was another limitation of our study. As the incidence of knee OA was much higher in women than in men in Asian countries, 13,26,28,50 it was not possible to avoid this predominance. Third, this study evaluated patient-reported outcome measures using only AKS knee and function scores. As this retrospective study included patients from 2008, the old version of AKS scores was only available for clinical assessment in all patients because the new version of AKS scores was published in 2012. 36 However, AKS scores have been widely used and have shown excellent reliability in the evaluation of individuals with knee OA after surgery. Additionally, this study evaluated ROM in clinical outcomes and sought to comprehensively investigate outcomes in patients with preoperative RKL, focusing not only on clinical outcomes but also on radiological and arthroscopic outcomes and survivorship. However, it would be better if this study included other patient-reported outcome measures, such as patient satisfaction, to reflect practical results.
Conclusion
Although the latest clinical scores were lower in the RKL group than in the no-RKL group, comparable results in postoperative clinical improvements, cartilage regeneration, and survivorship were observed in select patients with RKL at mid- to long-term follow-up.
Footnotes
Final revision submitted February 3, 2022; accepted March 22, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyung Hee University Hospital at Gangdong (study No. KHMC 2021-04-036).