
Abstract
Background:
Knee injection therapy is less effective for severe osteoarthritis (OA), specifically Kellgren-Lawrence (KL) grade 4. Patient selection for knee injection trials has historically been based on extension anteroposterior (AP) radiographic evaluation; however, emerging evidence suggests that KL grading using a flexion posteroanterior (PA) radiograph more accurately and reproducibly predicts disease severity. The impact of radiographic view on patient selection and outcome after knee injection therapy remains unknown.
Hypothesis:
A 45° flexion PA radiograph will reveal more advanced knee OA in certain patients. These patients will report worse pre- and postinjection outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Four raters independently graded extension AP and flexion PA radiographs from 91 patients previously enrolled in a knee injection trial. Patients determined to have KL grade 4 OA by any rater on extension AP radiographs were excluded. Among included patients, those upgraded to KL grade 4 on flexion PA radiographs by at least 2 raters constituted group 2, while all remaining patients constituted group 1. Demographic data and patient-reported outcome scores before injection and at 6 weeks, 3 months, 6 months, and 12 months postinjection were compared between groups.
Results:
Overall, 64 patients met the inclusion criteria, of which 19 patients (30%) constituted group 2. Compared with group 1, patients in group 2 were older (58.7 vs 52.3 years, P = .02), had worse visual analog scale pain scores before (6.6 vs 5.3, P = .03) and 6 months after injection (5.3 vs 3.5, P = .01), had less improvement in both Lysholm (8.5 vs 20.5, P = .02) and Short Form–12 physical component (–2.2 vs 1.7, P = .03) scores from preinjection to 6 months postinjection, and had less improvement in both Lysholm (1.6 vs 13.1, P = .03) and Knee injury and Osteoarthritis Outcome Score sport subscale (–2.1 vs 16, P = .01) scores from preinjection to 12 months postinjection.
Conclusion:
One in 3 patients considered to have mild to moderate knee OA on extension AP radiography is upgraded to severe knee OA (KL grade 4) on flexion PA radiography. These patients report worse preinjection outcomes, worse pain scores at short-term follow-up, and decreased improvement in knee function scores between 6 months and 1 year postinjection.
Symptomatic knee osteoarthritis (OA) affects nearly one-fifth of Americans daily. 9,14 Of the treatments offered at mild to moderate stages of disease, knee injection therapy with corticosteroids, hyaluronic acid (HA), platelet-rich plasma (PRP), and bone marrow aspirate concentrate are common options. 21 Eligibility for knee injection therapy is often guided by radiographic evidence of osteoarthritis, most often using the scoring system developed by Kellgren and Lawrence 17 (Table 1). In utilizing Kellgren-Lawrence (KL) grade, the vast majority of clinical trials pertaining to knee injection therapy have demonstrated maximal therapeutic response in mild disease, with diminishing response in advanced (KL grade 3 or 4) disease. 2,3,13,15,20 No single injection therapy has been shown to elicit superior outcomes in advanced OA. 1 As such, current trials typically exclude patients with KL grade 4 or bone-on-bone osteoarthritis. 4,10,35,37
Kellgren-Lawrence (KL) Grading for Knee Osteoarthritis

Historically, indication for knee injection therapy using KL grade has been based on an extension anteroposterior (AP) radiograph. However, recent evidence suggests that flexion posteroanterior (PA) views confer greater sensitivity and specificity in identifying advanced chondral disease. 7,12,29,32,38 The reasons for this are 2-fold: (1) arthroscopic evaluation has demonstrated that cartilage destruction tends to occur more posteriorly on the femoral condyles than is shown by the conventional extension AP view of the knee 24 and (2) biomechanical studies have shown that the greatest contact stresses in femorotibial articulation occur when the knee is partially flexed. 23 Despite this emerging evidence, it remains unknown whether knee injection outcomes can be influenced by preinjection radiographic technique. In the present study, we sought to determine how use of a 45° flexion PA view influences (1) patient selection for knee injection therapy and (2) patient-reported outcomes (PROs) after knee injection therapy. The authors hypothesized that flexion PA radiographs would reveal more advanced knee OA in certain patients, and that these patients would report worse pre- and postinjection outcomes.
Methods
After obtaining institutional review board approval, clinical records were reviewed from 91 consecutive patients with atraumatic, progressive knee pain. All patients had previously been enrolled in a prospective, randomized controlled trial comparing HA with PRP across all stages of OA (including KL grade 4). All patients had completed a preinjection clinical evaluation, a 5-view radiograph of the symptomatic knee, including weightbearing extension AP and flexion PA views, and validated PRO measures (Lysholm, International Knee Documentation Committee [IKDC] form, Knee injury and Osteoarthritis Outcome Score [KOOS], Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC], visual analog scale [VAS], Short Form-12 [SF-12]).
Part A
All preinjection extension AP radiographs were scrambled and graded independently using the KL scale by 1 musculoskeletal radiology fellow, 1 orthopaedic surgery resident, and 2 fellowship-trained orthopaedic surgeons. Varying levels of training across the 2 specialties were included to track interrater reliability between raters of different training levels (resident and fellow vs attending surgeons) and different training experiences (musculoskeletal radiologist vs attending surgeons). Patients were included in the present study if they received a KL grade <4 on extension AP view by all 4 raters.
Part B
If patients met the inclusion criteria, a 45° flexion PA view of the symptomatic knee was obtained and then scrambled, reviewed, and graded independently by the same 4 observers. Interrater reliability between all raters was determined by intraclass correlation coefficient (SPSS; IBM Corp) using a 2-way mixed model and was repeated for subgroup analysis between different levels of medical training. The highest (worst) grade was selected in the event of discrepancy between the 4 raters regarding KL grade. Patients who were upgraded to KL grade 4 on flexion PA view by 2 or more raters (at least 1 being an attending orthopaedic surgeon) constituted group 2, while all other patients constituted group 1. All patients were followed for a minimum of 6 months. Age, sex, body mass index (BMI), and PRO scores before injection and at 6 weeks, 3 months, 6 months, and 1 year after injection were compared between groups using unpaired Student t tests and chi-square tests.
Results
Part A
Utilizing the extension AP view, 27 of 91 patients were given a KL grade of 4 by at least 1 rater and were consequently excluded from the study. Of these 27 excluded patients, all but 1 also received a KL grade of 4 on flexion PA view by at least 2 graders. Of the remaining 64 patients who met the criteria for inclusion in this study, 35 were male and 29 were female (mean age, 54.2 years; mean BMI, 27.2 kg/m2). A total of 33 left knees and 31 right knees were evaluated. In all, 31 patients received HA injection while 33 patients received PRP injection. There were no significant differences in pre- or postinjection PROs between the 2 injection types. The mean follow-up across the entire cohort was 11.2 months.
Part B
After review of the flexion PA radiograph for the 64 patients included in the study, 19 patients (30%) were upgraded to KL grade 4, constituting group 2. This group included 10 patients who received an HA injection and 9 patients who received a PRP injection. The proportion of HA and PRP recipients did not differ between groups (P = .66). Demographic differences between groups 1 and 2 are presented in Table 2. Patients in group 2 were significantly older than those in group 1, with a mean age of 58.7 years compared with 52.3 years, respectively (P = .02). There were no statistically significant differences regarding sex or BMI between groups, nor were there any significant differences in outcomes based on injection type. PROs both before and 6 months after injection therapy are presented for both groups in Table 3.
Demographic Comparison Between Groups a

a BMI, body mass index; HA, hyaluronic acid; PRP, platelet-rich plasma.
b Boldfaced P value indicates statistical significance.
Patient-Reported Outcome Scores at Different Stages of Knee Injection Therapy for Groups 1 and 2 a

a Group 1, n = 45; group 2, n = 19. ADL, activities of daily living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, quality of life; SF-12, Short Form–12; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index; VAS, visual analog scale.
b Boldfaced P values indicate statistical significance (P ≤ .05).
VAS
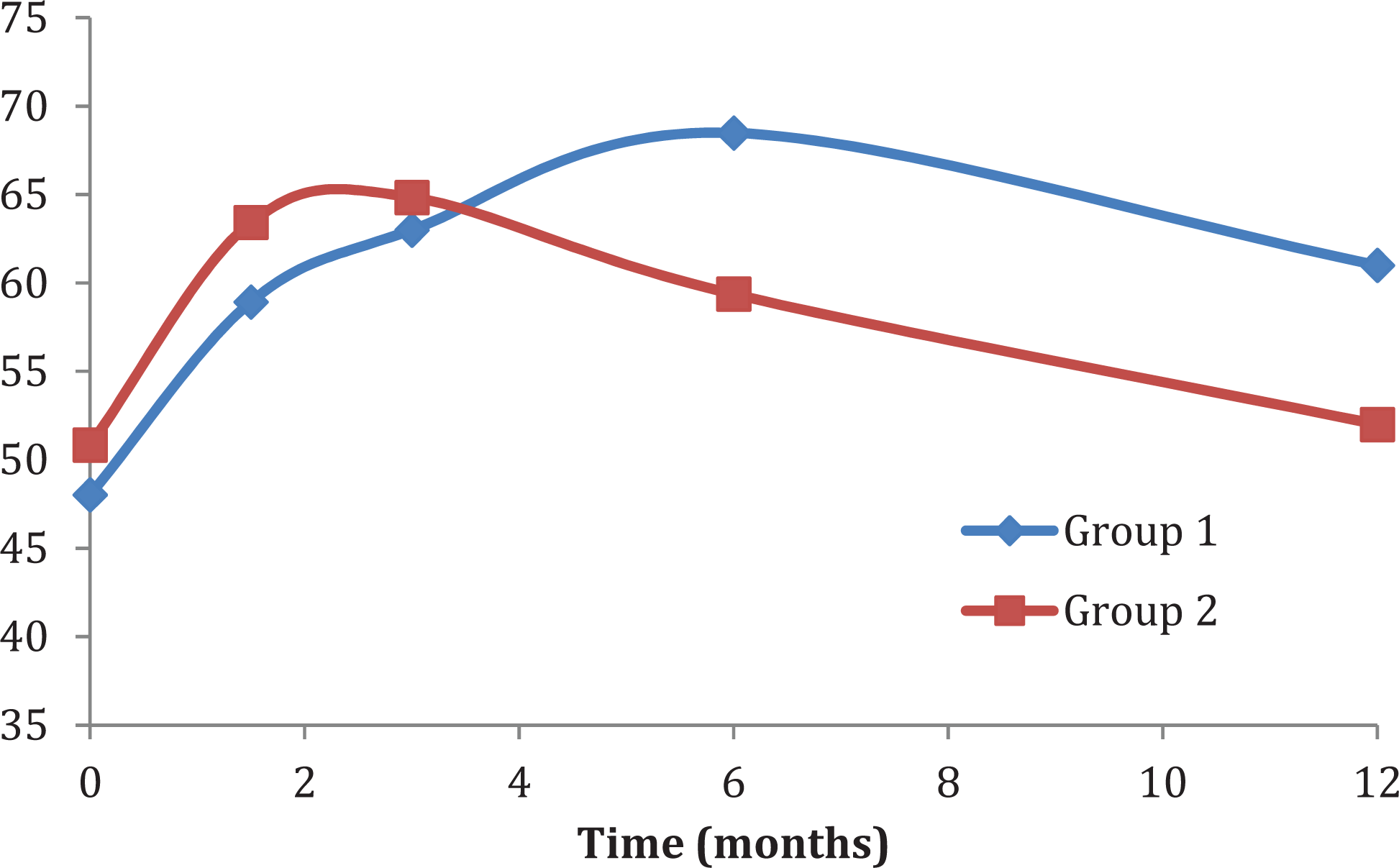
Group 1 had significantly lower (better) preinjection VAS pain scores than group 2 (5.3 ± 1.9 vs 6.6 ± 2.3; P = .03) (Figure 1). Group 1 had significantly less improvement in VAS pain scores than group 2 at 3 months postinjection (1.0 ± 2.4 vs 2.6 ± 2.7; P = .03), but still reported lower pain overall (4.3 ± 2.7 vs 4.7 ± 2.1; P = .77). Group 1 continued to report significantly lower VAS pain scores at 6 months postinjection (3.5 ± 2.3 vs 5.3 ± 2.5; P = .01) and a nonstatistically significant trend toward lower pain at 11.2 months postinjection (4.9 ± 3.2 vs 6.5 ± 3.3; P = .06). There were no significant improvements within either group compared with baseline at 6 months or beyond with regard to VAS pain.

Comparison of visual analog scale (VAS) scores between groups 1 and 2 over 12 months after knee injection therapy. Note that a higher VAS score corresponds with worse pain control. Asterisk denotes statistically significant differences between groups.
Lysholm
There were no statistically significant differences between groups 1 and 2 at any time point, although group 1 showed a trend toward higher (better) Lysholm scores at 6 months postinjection (68.5 ± 17.7 vs 59.4 ± 16.8; P = .06). When compared with group 2, group 1 had a significantly larger improvement between preinjection and 6 months postinjection (20.5 ± 16.8 vs 8.5 ± 19.8; P = .02) and between preinjection and 11.2 months postinjection (13.1 ± 19.2 vs 1.6 ± 18.4; P = .03) (Figure 2).
Comparison of Lysholm scores between groups 1 and 2 over 12 months after knee injection therapy.
KOOS
Group 1 reported significantly worse preinjection KOOS quality of life scores compared with group 2 (31 ± 20 vs 42 ± 21; P = .04). There were no differences in any other KOOS subscores between groups 1 and 2 at any additional time point. However, the improvement in subscores between preinjection and 11.2 months postinjection was significantly higher for group 1 compared with group 2 for KOOS sport subscale scores (16 ± 22 vs −2.1 ± 24; P = .01).
SF-12
There were no statistically significant differences between groups 1 and 2 at any time point, although group 1 showed a trend toward higher (better) SF-12 physical component scores at 6 months postinjection (40.7 ± 5.6 vs 37.4 ± 6.7; P = .052). When compared with group 2, group 1 had a significantly smaller improvement in SF-12 mental component scores between preinjection and 6 weeks postinjection (−3.9 ± 14 vs 4.9 ± 17.7; P = .04) and a significantly larger improvement in SF-12 physical scores between preinjection and 6 months postinjection (1.7 ± 5.8 vs −2.2 ± 7.1; P = .03).
IKDC
There were no statistically significant differences between groups 1 and 2, although group 1 showed a trend toward higher (better) IKDC scores at 1 year postinjection (50.6 ± 23.7 vs 39.0 ± 15.9; P = .06).
WOMAC
There were no statistically significant differences between WOMAC scores of groups 1 and 2 at any time point.
Interrater reliability was calculated to be 0.821 (95% CI, 0.729-0.886) for extension AP films. Flexion PA views yielded an intraclass correlation coefficient of 0.914 (95% CI, 0.872-0.945). Both of these values correspond to excellent reliability. 33 Subgroup analysis was conducted between varying levels of training, as the mean KL grade determined by the resident and radiology fellows was compared with the mean score determined by the 2 attending orthopaedic surgeons for every patient. On extension AP view, the mean resident and radiologist grades and mean attending grades had an intraclass correlation coefficient of 0.873 (95% CI, 0.787-0.924). Again, reliability between the 2 groups increased on flexion PA view to 0.923 (95% CI, 0.873-0.953).
Discussion
Radiographic view has significant influence on patient selection and patient-reported outcomes for knee injection therapy to manage knee OA. Specifically, we found that 1 in 3 patients with mild to moderate knee OA (KL grade <4) on an extension AP radiograph showed severe knee OA (KL grade 4) on a flexion PA radiograph (Figure 3). Perhaps most significant, we found that among patients with severe knee OA (KL grade 4), as determined using a flexion PA radiograph, outcomes were significantly worse after knee injection therapy as compared with the remaining cohort. Ultimately, our findings suggest that clinicians who use flexion PA radiography can improve patient selection for knee injection therapy, but more important, patient expectations and outcomes after knee injection therapy.

Three different patient extension anteroposterior (AP) radiographs with corresponding flexion posteroanterior (PA) radiographs directly below. Mean Kellgren-Lawrence (KL) grades for each radiograph were determined as follows: extension AP #1 (image A), 1; flexion PA #1 (image D), 3.5; image B, 1.75; image D, 4; image C, 2.25; image F, 4. In this study, flexion PA films were found to better illustrate tibial osteophytic lipping (D), femoral osteophytes (E), obliteration of the joint space (E and F), subchondral sclerosis (F), and deformation of bony ends (E and F).
Analysis of the timing of outcomes after knee injection yields several important findings. Before injection, patients in group 2 reported significantly worse pain scores, which we believe reflects their advanced chondral disease, which is best detected using flexion PA views. Interestingly, these patients also had significantly higher preinjection KOOS quality of life scores, which we speculate may reflect the older age of this group and their likely lower expectations with regard to knee function and quality of life. At short-term follow-up after injection, patients in group 2 reported significantly worse pain and functional outcomes across multiple validated surveys, with differences becoming most apparent around the 6-month postinjection period. Of note, the reported discrepancies between groups in VAS pain scores exceed published values for the minimal mean clinically important difference of 1.1 cm in knee osteoarthritis, meaning that patients in group 2 have noticeably worse pain. 16 This difference in short-term outcomes is critical, as the literature strongly suggests that injection therapy provides only short-term symptomatic relief and does not alter the natural history of disease. 22,36 A lack of significant long-term differences between groups is therefore not surprising, as benefits of injection therapy subside and patients equal out with respect to pain and function. Failure of injection therapy to maximize short-term outcomes in group 2, however, suggests that patients with radiographic evidence of advanced chondral disease should be counseled and appropriately educated regarding expectations of knee pain and function. Aside from the significant clinical ramifications of using suboptimal imaging, physicians using only extension AP views may be exposing these patients to unnecessary risks of injection therapy and delays in definitive management.
Our results demonstrate that knee injection treatment of OA can be influenced by radiograph choice, which is a significant finding given the relative infrequency of radiographic reporting across current randomized controlled trials pertaining to knee injection therapy. In fact, of the 10 prospective, randomized, controlled knee injection trials conducted in the past 5 years, only 4 studies specify using AP and/or lateral views, while the remaining 6 do not describe their radiographic methodology. 3,4,6,10,11,25 –27,30,35 There is currently no literature exploring knee injection outcomes based on specific radiographic views, yet incorporation of flexion PA views that better identify advanced chondral disease into routine practice would likely lead to improved patient selection for injection therapy and consequently improved patient outcomes. Given that one-third of this cohort would have been precluded from knee injection therapy if staged with a 45° flexion PA radiograph, and that this same group reported worse preinjection and short-term outcomes, it is worth considering how a flexion PA view could have changed the enrollment for and the outcomes of previous knee injection trials.
While a number of flexion PA radiograph views have been reported and utilized in the literature, 8,24,28,31 the Rosenberg PA view at 45° of flexion has consistently yielded improved diagnosis of both moderate and severe knee OA when compared with extension AP views. One 2014 multicenter cohort analysis of 632 patients revealed that 45° PA flexion weightbearing radiographs yielded greater interobserver reliability and correlation with arthroscopic findings of chondral disease compared with AP radiographs. 38 A 2001 prospective cohort study of 152 patients undergoing knee arthroscopy revealed that the flexion 45° PA view had greater sensitivity (83% vs 42%) in correctly detecting severe lateral compartment chondropathy. 7 The findings of our study further support the notion that flexion PA radiographs have greater interrater reliability than extension AP radiographs. However, they are unique in that excellent reliability was maintained across 2 specialties and across various levels of medical training. This serves to improve collaboration among surgeons and radiologists across various levels of training, as any single physician’s KL grade on flexion PA view may reliably indicate or rule out a patient for injection therapy.
Our study is most limited by the utilization of the KL classification system that grades the degree of OA based on preinjection radiographs. Specifically, the KL system has been criticized for its reliance on the presence of osteophytes, which some argue may be a product of normal aging and may not reliably predict future development of cartilage degeneration within the tibiofemoral joint. 5,19,34 Patients with other radiographic features of OA, such as joint space narrowing, subchondral sclerosis, or subchondral cysts, may therefore receive artificially low KL grades if they lack pronounced osteophytes. 18 Additionally, we were unable to correlate our KL grade to the current gold standard for OA diagnosis: arthroscopy. Our study is also limited by its retrospective design, its lack of a control group, and the fact that 2 types of injections were used. However, subgroup analysis revealed no significant differences in outcomes based on injection type. Finally, given that this study only tracked outcomes after HA and PRP injections, future prospective studies of other injection treatment modalities, such as corticosteroids, bone marrow aspirate concentrate, and placebo injections, are needed to generalize our results to all knee injections.
Conclusion
Approximately 1 in 3 patients considered to have mild to moderate knee OA (KL grade <4) based on an extension AP radiography had severe knee OA (KL grade 4) on flexion PA radiography. After knee injection therapy, patients determined to have severe knee OA on a flexion PA radiograph had significantly more pain at baseline, reported worse pain scores at short-term follow-up, and showed decreased improvement in knee function scores between 6 months and 1 year postinjection. These findings suggest that patient selection for injection therapy is influenced by radiographic degree of OA and that use of a PA flexion radiograph could influence patient selection in future injection trials based on a more accurate diagnosis of severe OA. Going forward, there is a need for studies pertaining to knee injection therapy to not only report their methods for indicating patients for treatment, including radiographic views, but to also utilize the optimal radiographic view for assessing chondral pathology, which we believe to be the 45° flexion PA view. Finally, we strongly encourage clinicians to utilize the 45° flexion PA view to improve not only patient selection for knee injection therapy but also patient expectations and outcomes after knee injection therapy.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.Y. receives research support from Arthrex and NuTech. B.J.C. receives research support from Aesculap/B.Braun, Arthrex, Cytori, Medipost, Ossur, Smith & Nephew, Tornier, and Zimmer; is a paid consultant for Arthrex, Regentis, and Zimmer; receives royalties from Arthrex, DJ Orthopaedics, Elsevier, Saunders/Mosby-Elsevier, and SLACK Inc; and has stock/stock options in Carticept and Regentis.
Ethical approval for this study was obtained from Rush University Medical Center (ORA Number: 10012103-IRB01).