
Abstract
Background:
The Bankart and Latarjet procedures are the 2 most commonly performed procedures for stabilization of anterior glenohumeral instability around the world. The aim of this study was to describe actual trends in surgery for anterior instability in the United States and in France.
Hypothesis:
Glenohumeral stabilization surgery overall is becoming more frequent in France and in the United States, with an increasing number of Latarjet procedures having been performed in each country in recent years.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective review was performed using French and American databases from 2009 to 2018. Procedure codes MEMA005 and MEMC004 were pulled from the French National Health Insurance System and Current Procedural Terminology codes 23455, 29806, and 23462 were pulled from IBM MarketScan. During this period, 73,914 patients underwent anterior shoulder stabilization surgery in France and 391,521 in the United States. For each year and the global period, the estimated number of Bankart procedures in the United States was compared with the number of French procedures. The same comparison was done for Latarjet procedures. The sex ratio was compared using chi-square testing. The mean age was compared using a Student t test.
Results:
The Bankart procedure represents 98% of the shoulder stabilization procedures in the United States, but the Latarjet procedure is becoming more common in the United States, having increased by 154% during the 10-year study period. In France, the Latarjet procedure represents 75% of the surgeries, having increased by 40% during the 10-year study period. However, use of the Bankart procedure in France increased from 11.2/100,000 in 2009 to 13.4/100,000 in 2018.
Conclusion:
This study demonstrated that, overall, use of the Latarjet procedure has been increasing over the last decade in both the United States and France. However, there remains a divergence in the treatment of anterior shoulder instability between the 2 countries. The Latarjet procedure remains the preferred treatment option in France for anterior shoulder instability (75% Latarjet vs 25% Bankart), whereas the Bankart procedure is dominant within the United States (98% Bankart vs 2% Latarjet). When breaking data down by age groups, more Bankart procedures are being performed on younger patients, and in both countries the incidences of women requiring these surgeries are increasing. The authors hope this study will serve as a foundation for future prospective studies establishing evidence-based algorithms to guide the treatment of anterior instability and provide a root cause analysis on why different surgeons choose a specific procedure to treat this problem.
Stabilization of anterior glenohumeral instability is a common treatment for most shoulder surgeons around the world. Although there have been many procedures described to treat recurrent anterior instability, the Bankart and Latarjet procedures are the 2 most commonly performed procedures.8,9,32,37
The Bankart procedure was initially described in Europe by the British surgeon Arthur Bankart in 1923. 4 It is an anatomic procedure that consists of an anterior capsulolabral repair back to its native origin. With the increasing utilization of arthroscopy in recent years, the arthroscopic procedure is now performed much more frequently than the open procedure.1,6 Nonetheless, 1 systematic review has shown comparable outcomes between both the open and arthroscopic techniques, and at 5 years of follow-up, instability recurrence rates vary between 11.7% and 28.7%, while re-dislocation rates vary between 4.2% and 20.3%. 36 The overall recurrent dislocation rate appears to be time dependent, with rates reaching as high as 25% by 10 years postoperatively. 9 The Latarjet procedure was first described in 1954 by French surgeon Michel Latarjet 24 and later modified by Patte 30 and Walch. 13 It is a nonanatomic procedure that consists of a coracoid bone-block transfer to the anterior edge of the glenoid in order to fill the bony defect, 7 and it utilizes the conjoint tendon as a dynamic shoulder stabilizer. 49 At 5 years of follow-up, the instability recurrence rates vary between 8.6% and 20.9% and the re-dislocation rates between 0.3% and 5.8%. 36 However, unlike the arthroscopic Bankart procedure, the rate of clinically detectable neurological injury after a Latarjet procedure can exceed 10% with no improvement in 4% of patients.15,38,46,47 Recently, there have been technical innovations to perform the Latarjet procedure arthroscopically5,23,42 with comparable recurrence (0.3%-4.8%) and complication (8.1%-8.9%) rates.17,21,34
The decision to perform either the Bankart or Latarjet procedure is dependent on multiple factors, including glenoid and humerus bone loss, chronicity, age, activity level, prior procedures, and rate of long-term arthritis.2,36 Furthermore, epidemiological studies have shown that the treatment choices are based on many factors, including age, 25 urban versus rural population, 39 emerging surgical trends in locations with 1 predominant technique, 1 sport type,12,43 and insurance. 45 In order to help surgeons choose between the stabilization techniques, Balg and Balg 2 proposed a radioclinical score in 2007 based on patient characteristics and bone lesions—the Instability Severity Index Score. This 10-point index is made up of 6 prognostic factors scored from 0 to 2 points each, with the sum of points determining the risk of recurrent instability. 2 Finally, the long-term re-dislocation risk is important to consider, seeing that the rate has been reported to range from 13% to 16% for Bankart procedures and 1% to 3.2% for Latarjet procedures. Additionally, revision rates for both Bankart and Latarjet procedures have been noted at 17% and 1.6%, respectively.28,18,51
Despite this growing evidence to help guide surgeons, the treatment of anterior shoulder instability remains quite divergent on different continents. For example, most shoulder surgeons in the United States prefer the arthroscopic Bankart procedure for first-time dislocations without bone loss,1,10,35,41 while the arthroscopic Bankart procedure is only used as a preferential technique for 25% of the French Arthroscopy Society's members. 40 This preference seems to have a link to the history of both techniques, the surgeon's training, surgical cost, and operative time, rather than to evidence-based medicine.16,33 A systematic review by Knapik et al 20 demonstrated that the overall outcomes for the treatment of anterior instability did not appear to differ between continents. However, this study could not estimate true incidences of procedures performed. To date, there remains a paucity of studies examining recent trends in the treatment of anterior shoulder instability in different countries. Therefore, the aim of this study was to describe actual trends in surgery for anterior instability in the United States and in France. We hypothesized that glenohumeral stabilization surgery overall is becoming more frequent in France and in the United States, with an increasing number of Latarjet procedures in each country in recent years.
Methods
Data Set
A retrospective comparative epidemiological review was performed using French and American databases from 2009 to 2018. French data were collected from the national health insurance system. All surgical procedures performed in France are registered with a specific code, using a specific classification for clinical procedures. Data from the French general population were collected from the National Institute of Statistics and Economic Studies. American data were collected from IBM MarketScan databases, which are administrative claims-based databases administrated by Truven Health Analytics; they contain data on >230 million patients in the United States. An advantage specific to this database is the ability to capture numerous aspects of inpatient and outpatient care longitudinally, enabling national trends in health care utilization to be comprehensively analyzed and described. 25 Querying the databases by Current Procedural Terminology (CPT) codes allows for the capture of patients who underwent the procedures of interest if privately insured by an employer. American population data were collected from the United States Census Bureau. Data privacy agreement and institutional board review were not mandatory as no identifying information was included.
IBM Watson Health MarketScan and SPSS Statistics software (IBM Corp) provide discharge weights, which represent statistical adjustments that attempt to correct for differences in the demographics of the database compared with the actual population. These weights adjust for any bias or discrepancies that may exist in the sample data, such as over- or underrepresentation of certain demographic or clinical characteristics. This enables them to be projected to the larger population as a whole. To use these, each record in the sample data is assigned a weight factor based on the likelihood that the record represents the overall population. For example, higher weights are assumed to be more representative of the population and thus are weighted higher. The converse is also true. This allows researchers to make more accurate generalizations about the larger population based on the obtained sample data.
Patient Selection
During the study period, we considered the number of open, arthroscopic Latarjet, and arthroscopic Bankart repairs performed in France using France's procedural coding (MEMA005 and MEMC004). Since a capsulolabral repair is frequently performed in combination with Latarjet procedures, patients with both codes for a single procedure were placed in the Latarjet cohort. It was not possible to differentiate between the open and the arthroscopic technique, and other bone-block procedures such as the Bristow repair could be counted as a Latarjet procedure.
For the United States, 118,821 patients were identified using CPT codes for open and arthroscopic Bankart and Latarjet procedures (23455, 29806, and 23462)). An advantage of the IBM MarketScan database is the linking of these CPT-labeled insurance claims with detailed, deidentified patient information. National estimates were calculated using weights provided by Truven MarketScan and complex sampling functions in SPSS. These discharge weights are created by factoring in various patient characteristics, hoping to account for possible selection biases present in the IBM MarketScan sample. Only privately insured patients and those with Medicare supplemental plans are included in the database, representing only a fraction of the greater US population. Patients were further characterized by sex and age at the time of the procedure. Age was then broken down into age groups: <20 years, 20 to 30 years, and >30 years. Population characteristics are reported as mean age and sex ratio.
Statistical Analysis
For each year and the global period, the estimated number of Bankart procedures in the United States was compared with the number of French procedures. The same comparison was done for Latarjet procedures. The sex ratio was compared using chi-square testing. The mean age was compared using a Student t test. Statistical significance was described by |ρ|> 0.60 and P < .05. Statistical analysis was performed using R software (R Foundation).
Results
Patient Characteristics
Patient characteristics are listed in Table 1. On analysis, there were 73,914 French patients identified by anterior shoulder stabilization procedural codes from 2010 to 2018. The mean age was 28.8 years (SD, 5.4 years), and male patients were predominant with a 4.38:1 ratio to female patients. In the United States, there was an estimated 391,521 patients who underwent anterior shoulder stabilization procedures during the same time period. The mean age was 30.2 years (SD, 6.2 years), and the male-to-female sex ratio was 2.82:1. American patients were significantly older than French ones (P = .001). The per capita caseloads stratified by sex are illustrated in Figure 1. In both France and the United States, there were more men than women undergoing both procedures. However, about twice as many women underwent surgery in the United States compared with in France. This translates into a male-to-female sex ratio that is higher in France than in the United States (Table 1).
10-Year Demographic Comparison of Patients Undergoing Anterior Shoulder Stability Procedures a

F, female; M, male.
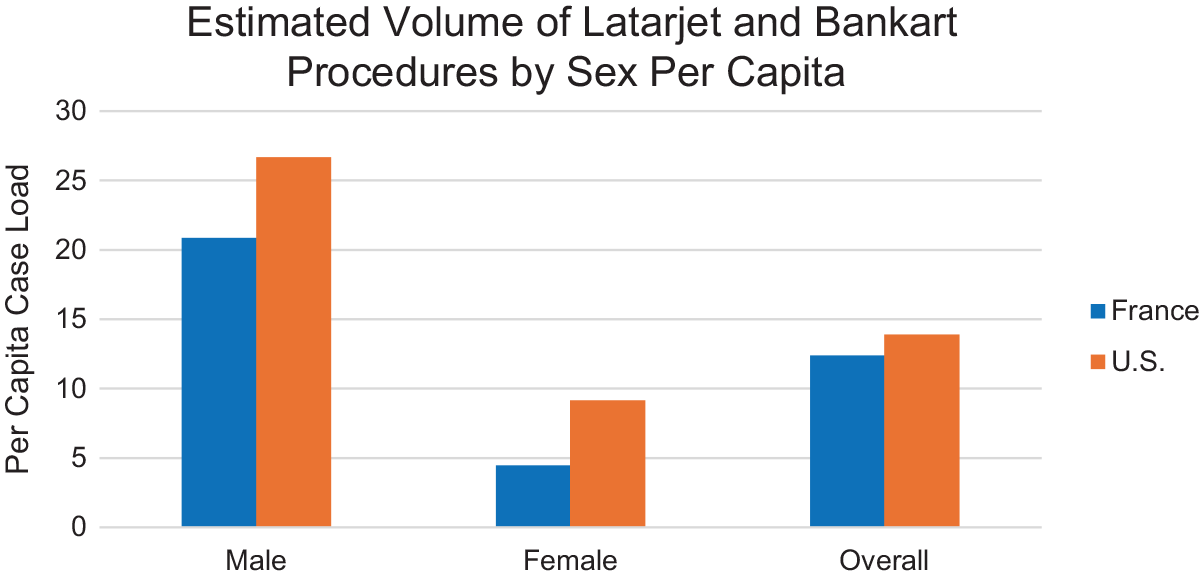
Per capita adjusted volume of Latarjet and Bankart procedures by sex.
Comparison in Surgical Procedures
When comparing the 2 countries, the Bankart procedure was performed at a much higher rate in the United States, while the Latarjet procedure was performed at a much higher rate in France. Overall, for the French cohort, there were 55,402 Latarjet procedures compared with 18,522 Bankart procedures in our date range. Alternatively, in the United States, there were 383,299 Bankart procedures, compared with 8221 Latarjet procedures during the same time (Figure 2). Overall, the Bankart-to-Latarjet ratio was 46.6:1 in the United States versus 0.33:1 in France.

Comparison of Latarjet versus Bankart procedural volume: France versus United States.
Trends in the United States
Over the 9-year study period, the total number of instability procedures per capita has remained fairly stable in the United States (Table 2). Alternatively, the Latarjet procedure became slightly more common, increasing by 154% between 2009 and 2018. Although it is still a small portion of stabilization procedures utilized, the number of Latarjet procedures in 2018 was more than twice that in 2009 (Figure 3). Across all age groups, there were more Bankart procedures performed than Latarjet procedures.
Annual Per Capita Adjusted Shoulder Stabilization Cases


Yearly per capita trends in Latarjet and Bankart procedure volume.
Trends in France
In France during the same 9-year time period, the total number of procedures per 100,000 people increased from 11.2 to 13.4 people (Table 2). The number of Bankart procedures remained relatively stable, while the number of Latarjet procedures increased continuously during the period for all age groups. In addition, Latarjet procedures were consistently the procedure of choice regardless of age (Figure 4).

Per capita adjusted volume of Latarjet and Bankart procedures by age group.
Discussion
In our study, we demonstrated that the number of anterior glenohumeral stabilization procedures increased from 2009 to 2018 in both France and the United States. This is likely in part because of the promising results achieved by both procedures and the move toward even more minimally invasive approaches. As we hypothesized, use of the Latarjet procedure has been increasing in both countries. However, it remains much more frequently performed in France than in the United States. Within the United States, a large percentage (97%-99%) of glenohumeral stabilization procedures performed are the Bankart procedure. The number of each procedure does not appear to be associated with age or sex, nor are the trends in each country.
The treatment of anterior shoulder instability remains controversial, with many factors impacting the surgeon's ultimate preferred option for each patient. Radiographic, patient, and clinical considerations impact this decision, including glenoid and humerus bone loss, chronicity, age, activity level, and prior procedures. 2 Additionally, treatment choices have been shown to be based on many other factors, including age, 25 urban versus rural population, 39 emerging surgical trends in locations with 1 predominant technique, 1 sport type,12,43 and insurance. 45 Other important factors likely include the rate of complications and overall success after each procedure. When considering the Latarjet procedure, it is important to take into account the risk of complications such as nerve injury (1.8%-20.6%).11,38,46,47,50 When considering the Bankart procedure, it is important to consider the long-term re-dislocation rates (up to 20%-30%) and associated revision surgery rates.9,26,28,36,51 There may be historical considerations, due to France being the birthplace of the Latarjet procedure,13,24,30 whereas the Bankart 4 procedure was first described in England and is chosen more frequently outside France. 3 The learning curve and associated comfort level of surgeons trained in the different health care systems also likely play an important role. Given these considerations, we performed a review of the incidences and trends of each procedure within both the United States and France.
Although the number of Latarjet procedures performed in the United States remains low, the numbers have increased by 154% between 2009 and 2018. Similarly, in France, the numbers of Latarjet procedures have increased by 40% from 2009 to 2018. This is likely due to the very promising results published on the Latarjet procedure and the comfort level of shoulder surgeons in each country as they gain experience.7,8,26,31,37,47,51 Alternatively, both in France and in the United States, the number of Bankart repairs has remained stable during the past 10 years except in the <20-year age group. Given the spread of the arthroscopic Bankart procedure over the open technique, 6 this has likely contributed to the continued high number of Bankart procedures performed in the United States, as many young surgeons trained in arthroscopic-heavy fellowships become very well trained in this technique. Furthermore, younger patients may have aesthetic concerns, electing for arthroscopic Bankart repairs in the United States. Although arthroscopic Bankart repairs have been previously reported as the procedure of choice for American surgeons, 1 we anticipate seeing a rise in Latarjet procedures for this population as more studies, like the one by Waltenspül et al, 44 find lower rates of failure after this procedure in adolescents.
There were also subtle differences in demographics between the 2 countries’ cohorts. Although the mean age of American patients is significantly higher than that of French patients, it reflects a difference of <2 years between the 2 countries. Furthermore, the mean age of French patients undergoing stabilization surgery increased steadily over the course of our study, approaching that of the American cohort. There were many more men in proportion to women in the French cohort compared with the American cohort, but over the 10-year period, the number of women undergoing stabilization procedures increased in both countries. In the United States, this rise may be partially explained by a large increase in female participation in sports such as tennis (30%), lacrosse (370%), volleyball (111%), and softball (174%) from the 1981-1982 season to the 2018-2019 season.19,48 These are interesting considerations, as other studies have shown that many nonpathological factors have had an impact on the decision to undergo surgery and the types of surgery, including age, 25 urban versus rural population, 39 emerging surgical trends in locations with 1 predominant technique, 1 sport type,12,43 and insurance. 45 The impact of all of these factors on the treatment algorithm in anterior shoulder instability demonstrates the complexity of the treatment decisions and lack of a standardized algorithm.
Our data confirmed our hypothesis that use of the Latarjet procedure has increased in both the United States and France, despite Bankart repair still being the intervention of choice for American surgeons. Although there are many factors to consider regarding why this difference remains so divergent, one is potentially traced to the origin and historical development of the Bankart 4 and Latarjet13,24,30 procedures. We have observed that in recent years, in the treatment of anterior shoulder instability, the Latarjet procedure remains French surgeons’ preferred choice, while in the United States it is mostly reserved for cases of failed prior surgery or in cases of large glenoid bone loss. We speculate that this might be due to the learning curves of the surgeons. When one is more familiar with a certain technique, their own skill and comfort level will potentially bias their treatment algorithm to prefer this technique. This is likely partially the explanation for these differences.
This study also has several advantages. It allows us to describe surgical practices in countries historically linked to a particular glenohumeral instability surgery, over a very large cohort. If the international comparison is generally understood, few previous studies have quantified the difference of the current practice as we do the current study. The observation period of our cohorts is important and covers a decade that has seen the development of progress in the surgical techniques described, notably thanks to the development of arthroscopy.22,29 The age groups evaluated in this study allow us to observe the impact that work such as the Instability Severity Index Score has had on the evolution of practices, suggesting low scores on the non-age prognostic factors seeing that many Bankart procedures are performed on younger patients in the United States.
Limitations
This study has limitations: it is a cross-sectional epidemiological study, without any outcome data limiting our conclusions to those of case volume, incidence, and associated trends. When comparing procedure rates between countries, we are assuming that the multiple factors affecting surgical decision-making are equivalent between countries. This database review does not allow us to know whether the intervention is carried out as a first intention or as a secondary treatment, nor does it have information on bone loss on the glenoid or humerus. Data on prior stabilization procedures were not recorded. It should be noted that the data are 6 years out of date; however, the direct comparison between case volumes using 2 nationwide databases provides nuanced information in the discussion on these stabilization procedures. Additionally, these nationwide databases rely on accurate coding; therefore, any coding errors will result in inaccurate data. Finally, it might be interesting to know the effect of the center on the choice of practices, from a purely geographic point of view and also to compare the so-called expert centers with centers performing surgical stabilization of the glenohumeral joint on a more occasional basis, as volume is known to be related to outcome for other shoulder surgeries.14,27
Conclusion
Our study demonstrated that, overall, use of the Latarjet procedure has been increasing over the last decade in both the United States and France. However, there remains a divergence in the treatment of anterior shoulder instability between the 2 countries. The Latarjet procedure remains the preferred treatment option in France for anterior shoulder instability (75% Latarjet vs 25% Bankart), whereas the Bankart procedure is dominant within the United States (98% Bankart vs 2% Latarjet). When breaking data down by age groups, more Bankart procedures are being performed on younger patients, and in both countries, the incidences of women requiring these surgeries are increasing. We hope this study will serve as a foundation for future prospective studies establishing evidence-based algorithms to guide the treatment of anterior instability and provide a root cause analysis on why different surgeons choose a specific procedure to treat this problem.
Footnotes
Final revision submitted August 31, 2024; accepted October 15, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.R.W. has received consulting fees from Stryker Corporation, Zimmer Biomet, Acumed, and Osteoremedies; institutional research support from Konica Minolta; and hospitality fees from Arthrex, Wright, Stryker, Integra, and Acumed. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.