
Abstract
Background:
After arthroscopic Bankart repair (ABR) for anterior glenohumeral instability (GHI), adolescent athletes have higher rates of subsequent recurrent GHI than any other subpopulation. Elucidating which adolescents are at highest risk of postoperative recurrent GHI may optimize surgical decision-making.
Purpose:
To identify prognostic factors associated with subsequent recurrent GHI requiring revision stabilization surgery (RSS) after ABR.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
The study included patients 12 to 21 years old who had undergone ABR for anterior GHI at a pediatric tertiary care hospital by 1 of 5 sports medicine fellowship–trained surgeons between 2000 and 2020. A multivariate Cox proportional hazards model, with percentage of patients with recurrent GHI undergoing subsequent RSS, was used with a time-to-event outcome analysis. The Cox model effects were expressed as the hazard ratio (HR). All tests were 2-sided, with an alpha of .05.
Results:
Records of 488 adolescent patients with ABR (78% male; mean age, 16.9 ± 1.98 years) were analyzed. Of these, 86 patients (17.6%) underwent subsequent RSS for recurrent GHI, yielding a cumulative risk of 8.8% at 2 years, 16.5% at 5 years, and 20% at 15 years. RSS occurred at a mean of 2.6 ± 2.1 years after ABR. Risk factors for RSS included >1 preoperative dislocation (2 dislocations: HR = 7.4, P = .0003; ≥3 dislocations: HR = 10.9, P < .0001), presence of a Hill-Sachs lesion (small: HR = 2.5, P = .0114; medium-large: HR = 4.2, P = .0004), younger age (1-year decrease: HR = 1.2, P = .0015), and participation in contact sports (HR = 1.8, P = .01). Adolescents with only 1 preoperative dislocation had a cumulative incidence of RSS (3.2%), which was significantly lower than those with 2 (24.2%) or ≥3 preoperative dislocations (33.5%).
Conclusion:
The number of dislocations before index ABR was the strongest risk factor for recurrent GHI requiring RSS in adolescents with anterior GHI, with 2 dislocations conferring >7-fold increased risk compared with a single preoperative dislocation. Other significant risk factors included the presence of a Hill-Sachs lesion, younger age, and participation in contact sports.
Keywords
Anterior shoulder dislocation, or glenohumeral instability (GHI), is common in adolescents 12 and has increased in recent years in association with athletic participation.17,42 The incidence of anterior GHI in this age group is reported to be upward of 164 per 100,000 person years.27,49 Adolescents have been shown to have a high incidence of recurrent GHI after nonsurgical management of a primary anterior glenohumeral dislocation, with several natural history studies reporting rates of recurrent GHI of 75% to 96% in those 12 to 18 years of age.14,24,35,37 Evolving evidence has led to increasing rates of stabilization procedures, most commonly in the form of arthroscopic Bankart repair (ABR). 41
The timing and role of ABR after a single dislocation episode are controversial topics in orthopaedics. Given the high rates of recurrent GHI after nonsurgical management, along with concerns about the long-term sequelae of repeat dislocation episodes on the long-term health of the shoulder, some authors have advocated for ABR for adolescent patients with first-time shoulder dislocations.6,7,34 Furthermore, studies to date have shown significantly lower rates of recurrent instability at both short- and long-term follow-up after a first-time shoulder dislocation treated with surgical stabilization compared with nonoperative management.2,45 Conversely, some authors contend that the incidence of recurrent GHI after ABR remains high in adolescents,11,23,44 and some patients with recurrent GHI may opt against surgical management. 38
Although ABR yields good short-term results and is effective in allowing return to play,10,13,18,39 adolescents have higher rates of subsequent recurrent GHI than any other age group.11,33,40,44,46 Identifying patients at highest risk of such events postoperatively may facilitate optimized surgical decision-making in this population. Factors that have previously been shown to be associated with recurrent GHI after ABR in adults include patient age, number of dislocation episodes, type of sports participation,3,47 and the presence and degree of humeral bone loss, or Hill-Sachs lesion.8,29 To date, adolescent-focused studies have included a relatively small number of patients.16,23,44 The purpose of the current study was to identify prognostic factors associated with recurrent GHI requiring reoperation after ABR in a primarily adolescent patient population. It was hypothesized that a greater number of dislocations, a longer time from first dislocation to surgery, younger age, increased glenoid and humeral bone loss, and participation in contact sports would be associated with an increased risk of recurrent GHI requiring reoperation.
Methods
Study Design
The institutional review board approved the current study protocol. No consent was needed as per retrospective review protocol. Consecutive patients 12 to 21 years of age were included in this retrospective, case-control study. Demographic data, including age, height, and weight, were obtained from a review of the patient’s electronic medical records. The event of interest in this study was recurrent GHI requiring subsequent revision stabilization surgery (RSS) of the ipsilateral shoulder. The date and frequency of RSS, which included both arthroscopic and open procedures, with or without glenoid augmentation, were recorded, whether performed at the study institution or an outside institution.
Patient Selection
Study inclusion criteria consisted of patients 12 to 21 years of age with documented anterior GHI who underwent primary ABR between 2000 and 2020 by 1 of 5 sports medicine fellowship–trained surgeons at a pediatric tertiary care hospital. Exclusion criteria were patients who presented initially for revision surgery, those who underwent primary open procedures, those who underwent ABR <2 years before the search date, those who underwent concomitant stabilization procedures in addition to ABR (eg, a remplissage procedure) or concomitant posterior stabilization procedures, and those with multidirectional instability. Patients with off-track bone loss based on magnetic resonance imaging (MRI) measurement were excluded, 48 as these patients are not typically managed with ABR alone at the study institution.
Variables for Assessment
The independent variables analyzed were based on clinical rationale and previous similar studies, including age, skeletal maturity, sex, shoulder dominance, participation in contact or overhead sports, number of dislocation episodes before index ABR (categorized as 1 dislocation, 2 dislocations, or ≥3 dislocations), time from first dislocation to index ABR, presence of a Hill-Sachs lesion on MRI before the index procedure (categorized as no lesion, small lesion [<20% of humeral head articular surface], or medium-large lesion [≥20% of humeral head articular surface]),4,22 presence of glenoid bone loss on MRI and confirmed intraoperatively (categorized as none, mild [<10%], or moderate-large [10%-20%]), presence of an anterior labral periosteal sleeve avulsion lesion, presence of a glenolabral articular disruption lesion, and number of anchors used in the ABR procedure.
Statistical Analysis
Analyses were conducted using SAS, Version 9.3 (SAS Institute). Descriptive statistics were calculated, including counts, frequencies, and percentages for categorical variables; means and standard deviations for normally distributed variables; and medians and ranges for nonnormally distributed data. The nth-year cumulative incidence was calculated as the number of patients with recurrent GHI requiring RSS before the nth-year, divided by the number of patients with follow-up data at the nth-year.
Kaplan-Meier curves were constructed to depict the time to RSS. The primary analysis was conducted using a proportional-hazards model, where the percentage of patients with recurrent GHI requiring RSS were analyzed in a time-to-event analysis as the outcome. It was anticipated that a total of approximately 85 to 90 events (RSS procedures) would be recorded, and therefore it was decided a priori that no more than 8 independent variables could be included in the model to prevent an overfitted, unstable model. The selection of possible independent variables for inclusion in the final models was guided by clinical judgment, univariate analyses, the change-in-estimate criterion, and the Akaike information criterion. 1 Cox proportional hazard regression modeling was used to estimate the effect of the selected independent variables on the time to RSS. Tests for nonproportional hazards included cumulative sums of Martingale residuals over time, 28 a Kolmogorov-type supremum test, and plots assessing Schoenfeld residuals of each included variable over time. 43 If the proportionality assumption was not met, the results would be stratified, if appropriate. The selected independent variables were included in the final model only if their inclusion in the model changed the effect size of the treatment group by a cut-off of >10%, as per the change-in-estimate criterion. 30 The effects from the Cox model were expressed as a hazard ratio (HR), the corresponding 95% CI, and the associated P value. All tests were 2-sided with an alpha level of .05. A post hoc power analysis was conducted using the formula proposed by Hsieh and Lavori 19 within the SAS Power procedure. Based on the results of this study, the probability of an event (recurrent instability requiring RSS) was taken as 0.20. The standard deviations of each of the assessed variables were estimated based on their distribution in the present study. A 2-sided test was used to assess the power of our analysis to detect a 2- or 2.5-fold increase (HR = 2 or 2.5) in the incidence of RSS given our sample size of 488 total patients included.
Results
A total of 488 adolescent patients were included in the analysis (Figure 1), with a mean age at the time of surgery of 16.9 ± 1.98 years, including 107 (22%) female patients. The most common primary sports played included American football (n = 141; 29%), hockey (n = 47; 10%), basketball (n = 40; 8%), baseball (n = 33; 7%), lacrosse (n = 30; 6%), soccer (n = 25; 5%), wrestling (n = 18; 4%), and volleyball (n = 18; 4%) (Figure 2). A total of 270 (55%) athletes participated in contact sports, whereas 95 (20%) were overhead athletes. There were 23 patients (5%) who did not report participation in any sport.
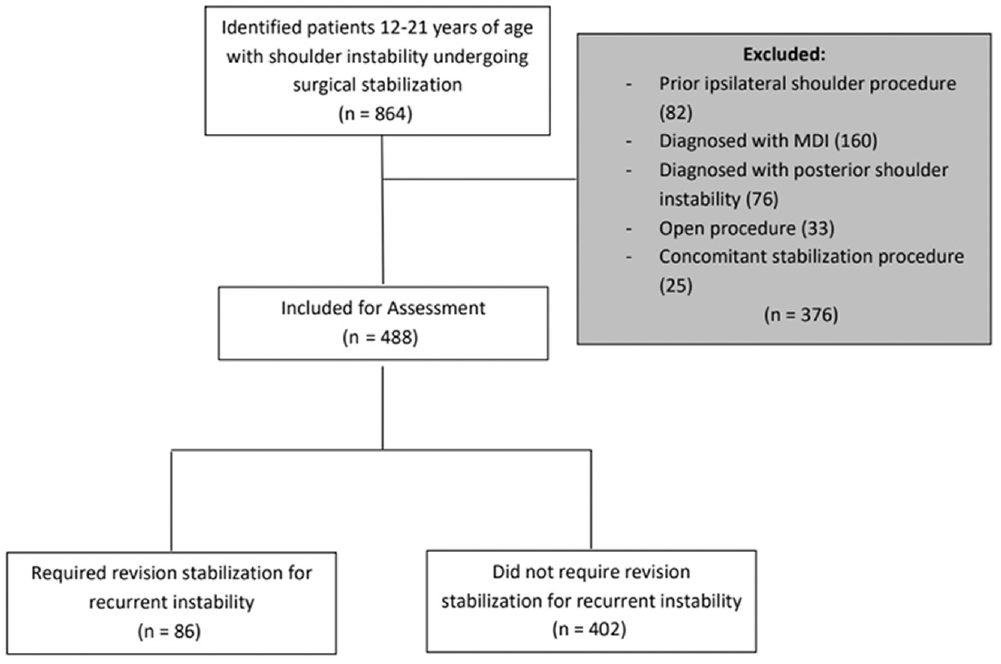
Flow diagram depicting the number of patients included/excluded and reasons for exclusion. MDI, multidirectional instability.
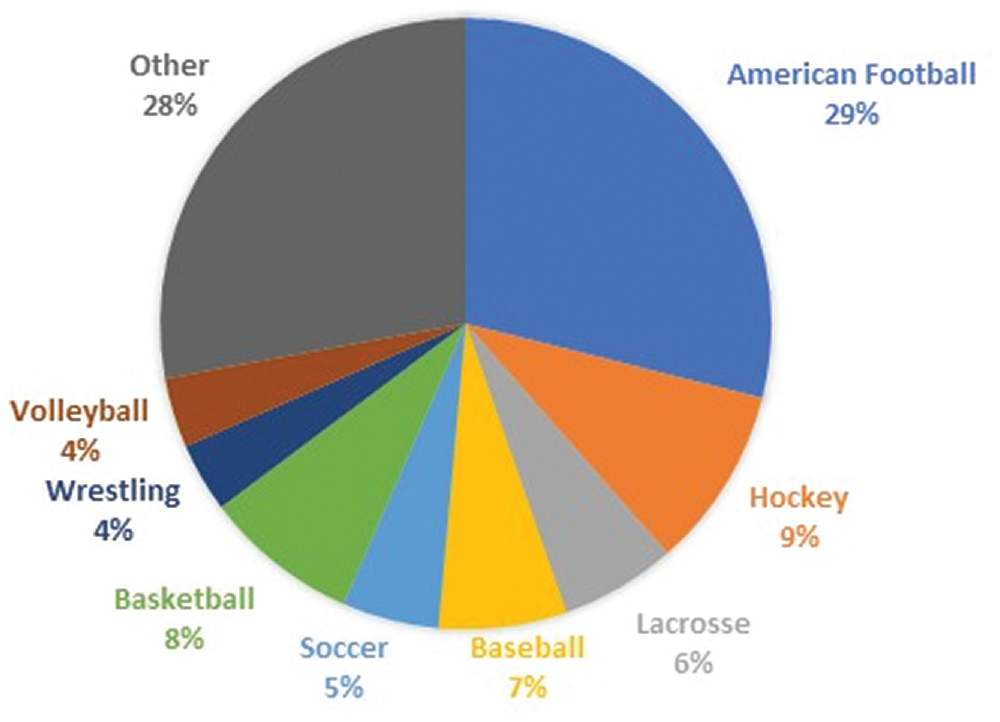
Primary sports participation among patients who underwent arthroscopic anterior Bankart repair.
In total, 86 patients (17.6%) developed recurrent GHI that required RSS. The RSS procedures occurred at a mean of 2.6 ± 2.1 years from the index procedure. The cumulative risk of recurrent GHI requiring RSS was 8.8% (95% CI, 6.3%-11.3%) at 2 years, 12.6% (95% CI, 9.6%-15.6%) at 3 years, 16.5% (95% CI, 13.1-19.9%) at 5 years, 19.2% (95% CI, 15.4%-23%) at 10 years, and 20% (95% CI, 15.9%-24.1%) at 15 years after index stabilization procedure (Figure 3). The most common RSS procedure was open Latarjet (n = 42; 49%), followed by revision ABR (n = 24; 28%) and open capsulorrhaphy/Bankart repair (n = 20; 23%). No significant change was noted in the type of RSS procedure performed over time.
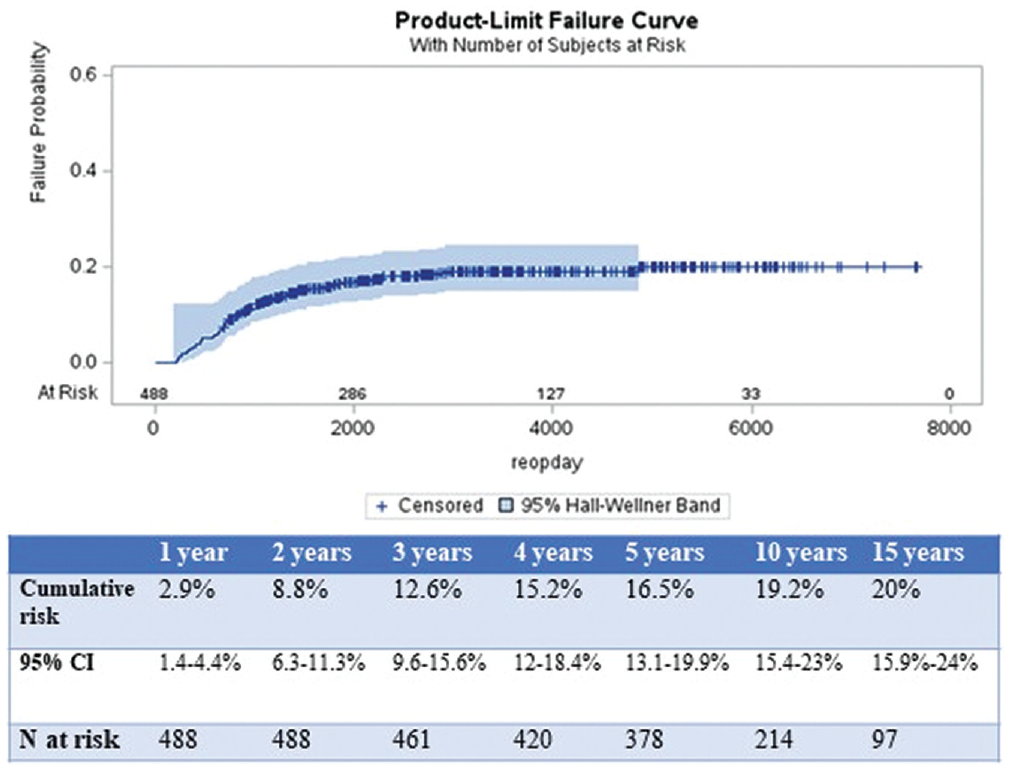
Cumulative risk of recurrent instability as measured by requiring revision stabilization by number of years from index procedure.
Patient characteristics for those with and without recurrent GHI requiring RSS are presented in Table 1. Univariate Cox proportional hazards analyses found no significant effect of sex, shoulder dominance, glenoid bone loss, presence of anterior labral periosteal sleeve avulsion lesions, presence of glenolabral articular disruption lesions, participation in overhead sports, or number of anchors used in the index ABR on the time to recurrent GHI requiring RSS (Table 1).
Patient Characteristics for Those With and Without Recurrent Instability Requiring Revision Stabilization a
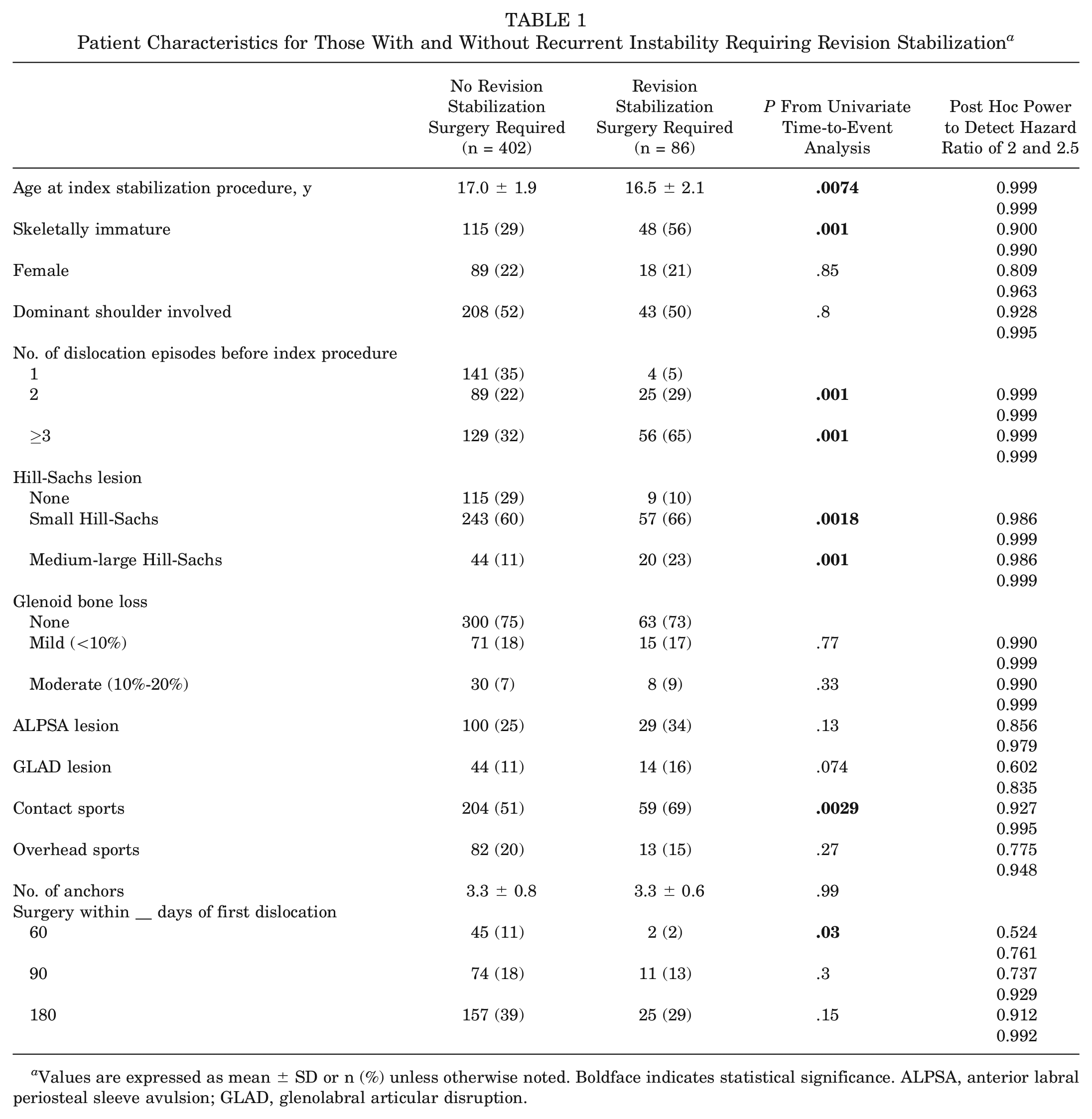
Values are expressed as mean ± SD or n (%) unless otherwise noted. Boldface indicates statistical significance. ALPSA, anterior labral periosteal sleeve avulsion; GLAD, glenolabral articular disruption.
Based on the multivariate Cox proportional hazards model, significant risk factors for recurrent GHI requiring RSS included >1 dislocation before index ABR (2 dislocations: HR = 7.4 [95% CI, 2.5-21.6], P = .0003); ≥3 dislocations: HR = 10.9 [95% CI, 3.9-30.5], P < .0001), presence of a Hill-Sachs lesion (small Hill-Sachs: HR = 2.5 [95% CI, 1.2-5.1], P = .0114; medium-large Hill-Sachs: HR = 4.2 [95% CI, 1.9-9.3], P = .0004), age at the time of the index ABR (1-year decrease in age: HR = 1.2 [95% CI, 1.1-1.4], P = .0015), and participation in contact sports (HR = 1.8 [95% CI, 1.1-2.9], P = .01) (Table 2).
Multivariate Cox Model of Risk Factors for Recurrent Instability Measured by Revision Stabilization Surgery a
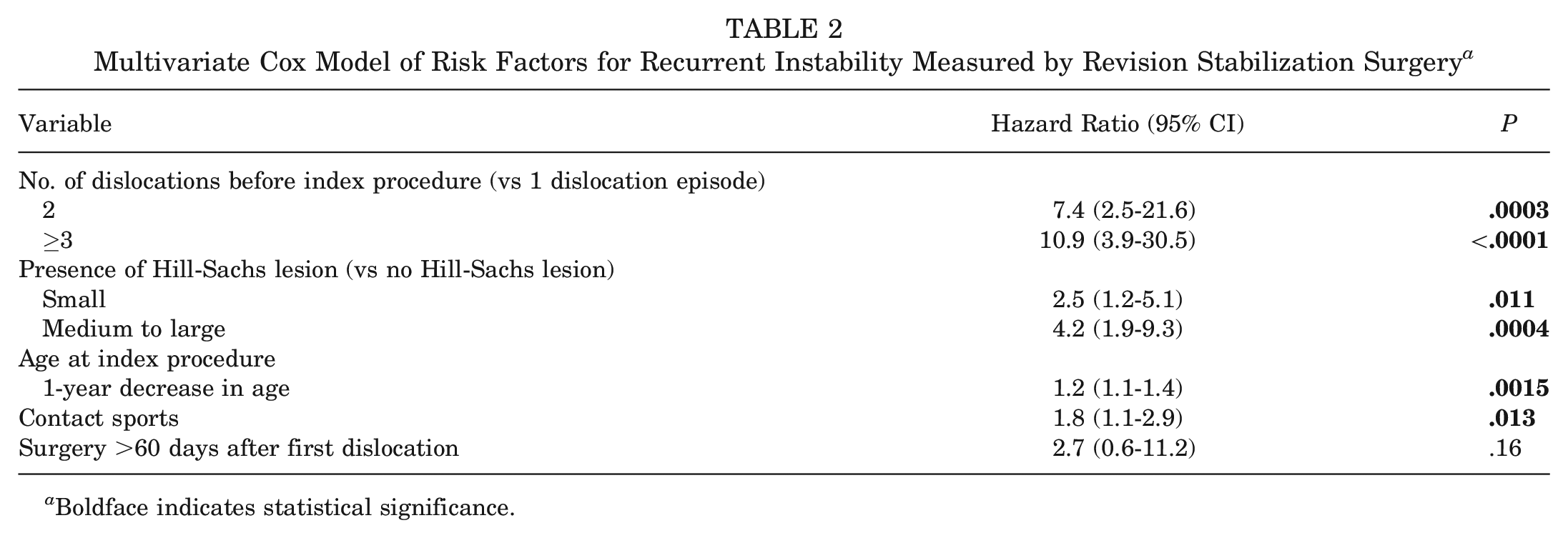
Boldface indicates statistical significance.
The cumulative risk of recurrent GHI requiring RSS for those with 1 dislocation before the index ABR was 3.2% (95% CI, 0.1%-6.3%), compared with 24.2% (95% CI, 15.6%-32.8%) for those with 2 dislocations and 33.5% (95% CI, 26%-41%) for those with ≥3 dislocations. For patients with no Hill-Sachs lesion identified, the cumulative risk of recurrent GHI requiring RSS was 8.8% (95% CI, 3%-14.6%), compared with 21.8% (95% CI, 16.5%-27.3%) in those with small Hill-Sachs lesions and 32.6% (95% CI, 20.7%-44.5%) in those with moderate-large Hill-Sachs lesions. Skeletally mature patients had a cumulative risk of recurrent GHI of 13.8% (95% CI, 9.3%-18.3%), whereas skeletally immature patients had a risk of 32.1% (95% CI, 24.3%-39.9%). Last, patients who did not participate in contact sports had a cumulative risk of recurrent GHI of 14.2% (95% CI, 8.5%-19.9%), compared with 25% (95% CI, 19.3%-30.7%) in those who did participate in contact sports (Table 3).
Cumulative Risk of Recurrent Instability as Measured by Revision Stabilization for Patients With Various Risk Factors a
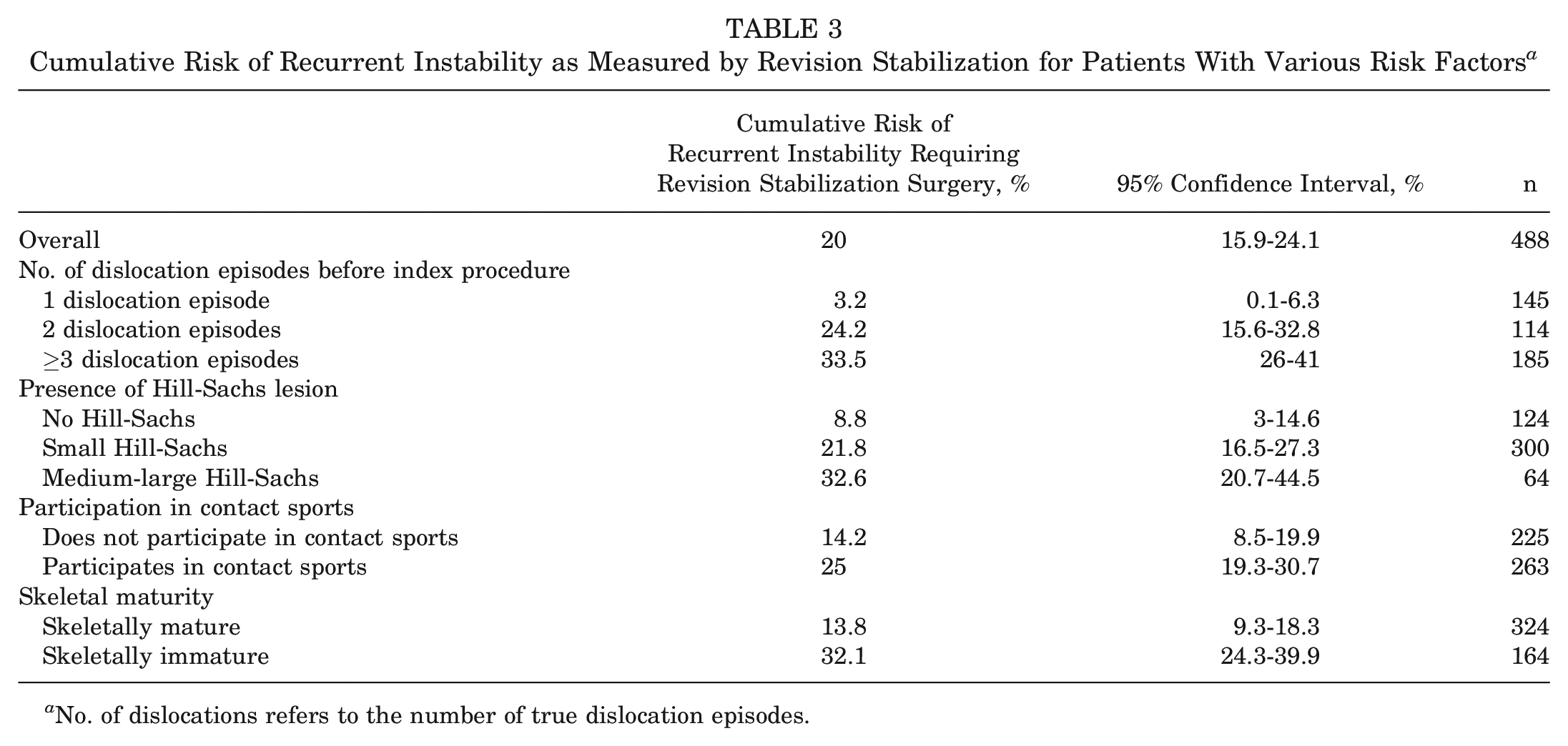
No. of dislocations refers to the number of true dislocation episodes.
Discussion
The most important finding of the current study is that adolescent patients with anterior GHI who sustained only a single dislocation before ABR had a cumulative rate of recurrent GHI requiring RSS that was >7 times lower than those who sustained 2 dislocations and >10 times lower than those who sustained ≥3 dislocations. Furthermore, the presence of a Hill-Sachs lesion was a significant risk factor for recurrent GHI requiring RSS with small and medium-large Hill-Sachs lesions, conferring a 2.5-fold and 4-fold increased risk, respectively, compared with those with no Hill-Sachs lesions. Younger age and participation in contact sports were additional predictors of recurrent GHI requiring RSS. We noted no significant effect of sex, shoulder dominance, glenoid bone loss, presence of anterior labral periosteal sleeve avulsion lesions, presence of glenolabral articular disruption lesions, participation in overhead sports, or number of anchors used, on the incidence of recurrent GHI.
The cumulative incidence of RSS for recurrent GHI in the present study was 20% at 15 years. Several studies that investigated smaller cohorts of adolescent patients similarly reported relatively high rates of recurrent GHI after ABR for treatment of anterior GHI. In a study of 67 adolescent patients <18 years old, all of whom participated in contact sports and had undergone ABR, Torrance et al 44 reported that 34 (51%) developed recurrent GHI at a mean 33 months after surgery. Kramer et al 23 assessed 39 adolescent patients with a mean age of 16 years who had undergone ABR for anterior GHI; those investigators reported 9 (23%) cases of recurrent GHI at a mean of 20.7 months of follow-up. Similarly, Cheng et al 11 studied 171 adolescents after ABR and found that 35 (20%) developed recurrent GHI. Egger et al 16 recently studied 59 adolescent patients 12 to 18 years of age and reported that 10 (17%) had recurrent GHI that required RSS. It is important to consider the follow-up for rates of recurrent GHI after ABR in adolescents, as <50% of the instability events in this study occurred within the first 2 years postoperatively. However, by 5 years postoperatively, >80% of the recurrent GHI events had occurred, and by 10 years >95% of the recurrent GHI events were identified.
Management of adolescents with first-time anterior glenohumeral dislocations has been one of the more controversial topics in recent years. One concern with recurrent GHI is that repeated dislocations can lead to fractures and/or attritional bone loss of the glenoid and Hill-Sachs lesions,5,15 which may cause higher rates of failure after ABR.9,11,23 Lau et al 25 assessed patients with anterior GHI and found that almost one-quarter of the adolescent patients had off-track bone loss, compared with <4% in adults, with multiple dislocations being the only other independent risk factor for bone loss. Cheng et al 11 assessed 171 adolescents who had undergone ABR and found that those who had >1 dislocation before ABR were >7 times more likely to have recurrent GHI postoperatively (odds ratio = 7.7; P = .01). Although the aforementioned study did not differentiate between 2 dislocations and ≥3 dislocations, the findings are similar to the current study, which found that the number of dislocations before ABR was the most important predictor of recurrent GHI requiring RSS after ABR. Adolescents who sustained 2 dislocations before index ABR were >7 times more likely to experience recurrent GHI requiring RSS. Moreover, those with ≥3 dislocations were >10 times more likely to experience recurrent GHI that required RSS. We believe that the reason why the number of dislocations is such an important factor is likely multifactorial, relating both to increasing humeral and glenoid bone loss with each dislocation episode. Moreover, recurrent dislocation episodes cause damage and stripping to the adolescent capsulolabral complex that become more difficult to repair with ABR alone after >1 dislocation. Although recurrent GHI has traditionally been an indication for RSS, the findings of the present study support consideration for primary ABR after a single, first-time dislocation, particularly in younger teenagers, in contact athletes, or when a Hill-Sachs lesion is present, to prevent recurrent GHI requiring further, often more invasive, and less successful stabilization procedures.
The presence and size of a Hill-Sachs lesion were important predictors of recurrent GHI requiring RSS, with medium to large Hill-Sachs lesions leading to the most significantly increased risk compared with those with no Hill-Sachs lesion. However, even small Hill-Sachs lesions led to an increased risk compared with those with no Hill-Sachs lesion. An adjuvant surgical technique to address the Hill-Sachs lesion arthroscopically is the remplissage procedure, 36 which is typically indicated for a Hill-Sachs lesion that is found to be large and engaging, when the glenoid bone loss is not substantial enough in size to warrant an open procedure.21,26 A Hill-Sachs lesion is considered engaging if, during arthroscopic examination, the size and orientation of the lesion is such that it engages the glenoid at 90° of abduction and external rotation of the shoulder. 8 The present study included only those who had isolated arthroscopic Bankart repair and excluded patients who had a remplissage procedure performed due to an engaging Hill-Sachs lesion. Hughes et al 20 retrospectively compared 21 adolescents who underwent an arthroscopic remplissage in addition to ABR versus 20 matched controls who had undergone ABR alone and found that those in the remplissage group had a significantly lower rate of recurrent GHI (13%) compared with those in the isolated ABR group (47%). The findings of the current study, that even small Hill-Sachs lesions pose a significant risk for recurrent GHI in the adolescent population, suggest that there may be a role to consider expanding the indications for the remplissage procedure to smaller Hill-Sachs lesions, particularly in those at highest risk for recurrent GHI. Although studies to date demonstrate encouraging outcomes on the use of the remplissage procedure, adolescent-focused studies have been limited by their study design and sample size. Further research would be useful to determine the benefits and drawbacks of remplissage and broader indications for the remplissage procedure in adolescents.
Other risk factors for recurrent GHI in the present study included the presence of Hill-Sachs lesions, younger age, and participation in contact sports. The sex of the patient was not found to be a significant risk factor for recurrent GHI. Previous studies that have assessed the effect of sex on recurrent instability in adolescent patients have reported no significant effect.11,16,31,32 In their series of 67 adolescent patients, Torrance et al 44 reported that age was the most important predictor of recurrent GHI after ABR, with those <16 years of age 2.2 times more likely to develop recurrent GHI than the older adolescent patients in the cohort. Kramer et al 23 reported a higher incidence of Hill-Sachs lesions on MRI in patients who developed recurrent GHI (89%) compared with those who did not develop recurrent GHI (52%; P = 048). In a study of 171 adolescents, Cheng et al 11 reported that in addition to the number of dislocations, risk factors for postoperative recurrent GHI included skeletally immaturity and glenoid retroversion <6°. In a study of 59 adolescents, Egger et al 16 found that those with recurrent GHI requiring RSS had larger Hill-Sachs lesions (P = .04) than those who did not require RSS. Interestingly, the aforementioned study also found that glenoid bone loss was not statistically different between the groups that did or did not require RSS. 16 In the present study, glenoid bone loss was similarly not significantly associated with recurrent instability requiring RSS, contrary to our hypothesis. We believe that one explanation for this finding is that participants who had a large degree of glenoid bone loss or off-track bipolar bone loss were often treated with procedures other than arthroscopic soft tissue stabilization alone and were excluded from this study. The findings of this study may suggest that within the population of patients with on-track bone loss, the presence of small or even moderate glenoid bone loss in and of itself may not be a risk factor for recurrent GHI requiring RSS. However, a Hill-Sachs lesion may have the potential to dynamically engage in an adolescent patient, despite the shoulder being classified as “on-track,” due to greater scapulothoracic motion than in adults. 16
The primary limitation of the present study is its retrospective nature; therefore, it is subject to known and unknown confounders as well as bias, including selection bias. We attempted to control for known confounders by considering a wide range of demographic, patient, and surgical factors. Furthermore, a multivariate model was used to obtain the final hazard ratios. However, it is not possible to control for all confounding factors in a nonrandomized study design, and therefore it is possible that some of the associations identified in this study were explained, in part, by other variables that differed between patients who did and did not develop recurrent GHI. To mitigate the risk of selection bias, we included a large number (n = 488) of adolescents investigated in a continuous fashion over a wide time period, and the presence or absence of recurrent GHI was determined only after their inclusion in the study. However, the retrospective nature of the study also precluded an a priori power analysis to ensure that sufficient patients were included to detect differences in each of the variables assessed.
Only recurrent GHI that required RSS was considered, and therefore we may have excluded patients who sustained recurrent GHI who did not undergo RSS for a variety of reasons (eg, patient preference, cessation/change in activity, geographic mobility). Due to the retrospective nature of the study, we concluded that a focus on recurrent GHI that required RSS would provide the most reliable clinical outcome measure, as the incidence of subluxation and subjective instability was not uniformly recorded for all included patients. The population included in this study was predominantly male (78%); however, this proportion is in line with the proportion of male patients in previous studies assessing anterior shoulder instability in adolescent patients—68% to 98%.10,11,16,39,44 Another limitation is the inclusion of patients from a wide time period (2002-2021) during which surgical techniques and implants used in ABR have changed. Moreover, 5 different surgeons were involved, and therefore, by the nature of ABR, slightly different techniques may have been used across the patients included in the study, such as amount of release, position of the anchors, and types of anchors and knots. Although this nonhomogeneous population in terms of surgical technique allows for more generalizable results, the effects of these possible differences in technique could not be controlled within the study.
Conclusion
The number of dislocations before index ABR was the strongest risk factor for recurrent GHI requiring RSS in adolescents with anterior GHI, with 2 dislocations conferring >7-fold increased risk compared with a single preoperative dislocation. Other significant risk factors included the presence of a Hill-Sachs lesion, younger age, and participation in contact sports.
Footnotes
Submitted December 5, 2023; accepted April 16, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: B.E.H. has received consulting fees from and owns stock in Imagen Technologies and is an educational consultant for Arthrex and Kairos Surgical. M.S.K. has received royalties from OrthoPediatrics and Ossur and support for education from Kairos Surgical. D.E.K. has received support for education from Kairos Surgical and consulting fees from Miach, Smith + Nephew, and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.