
Abstract
Background:
Subcritical bone has been shown to result in a higher rate of recurrent instability and inferior outcomes after an arthroscopic soft tissue Bankart procedure alone. The ideal surgery for patients with subcritical bone loss remains controversial, with options including arthroscopic Bankart alone, Bankart plus Remplissage (BRR), open Bankart, or a bone transfer procedure.
Purpose/Hypothesis:
The purpose of this study is to compare the outcomes between the arthroscopic BRR with an open Latarjet for the treatment of anterior shoulder instability in patients with glenoid bone loss (GBL) from 13.5% to 24% in an active-duty military population. It was hypothesized that there will be no difference in recurrence rate or patient-reported outcomes between the 2 procedures.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A retrospective matched-cohort comparison of patients who underwent anterior glenohumeral instability procedures with subcritical bone loss was performed. Inclusion criteria included symptomatic anterior shoulder instability, subcritical GBL (13.5% to 24%), recurrent instability with ≥2 instability episodes, surgical treatment with arthroscopic BRR or open Latarjet, and minimum follow-up of 2 years. Outcomes assessed included recurrent instability (defined as postoperative dislocation or subjective subluxation), military physical restrictions, Western Ontario Shoulder Instability Index (WOSI) score, and Single Assessment Numeric Evaluation (SANE) score.
Results:
In total, 50 patients were included, 25 of whom underwent an arthroscopic BRR and 25 patients who were treated with an open Latarjet. Mean bone loss was 16.1% and 19.3%, respectively. Five patients experienced recurrent instability, 3 in the arthroscopic BRR group and 2 in the open Latarjet group (P = .64). Mean postoperative SANE score for the arthroscopic BRR group was 81.6% and open Latarjet group was 84.2% (P = .42). Mean postoperative WOSI score for the arthroscopic BRR group was 64.6% and open Latarjet group was 67.9% (P = .44). There was no difference in the number of patients placed on permanent military physical restriction in the arthroscopic BRR group (n = 2) compared with open Latarjet (n = 3) (P = .64).
Conclusion:
In our small cohort of active-duty military patients with subcritical GBL, there was no difference in recurrent instability between arthroscopic BRR compared with open Latarjet. Additionally, there was no significant difference in postoperative SANE or WOSI scores, complications, or the number of patients placed on permanent military restriction.
Patients with recurrent anterior glenohumeral instability (GHI) with subcritical bone loss of the glenoid (commonly defined as between 13.5% and 24%) have many surgical options available to them.2,5,11 It is widely accepted within the field of orthopaedic surgery that arthroscopic Bankart repair in isolation is a poor option for patients with subcritical bone loss, with many studies demonstrating inferior outcomes and high rates of recurrent instability after this procedure in these patients.4,15,19
Several options exist beyond isolated arthroscopic Bankart repair to manage the problem of subcritical bone loss, with 2 common options being arthroscopic Bankart repair supplemented with Remplissage (BRR) and the open Latarjet procedure. There is little available literature directly comparing the outcomes of these 2 surgical techniques in patients with subcritical glenoid bone loss (GBL).13,14 BRR involves both repair of any Bankart lesion and “filling in” of any present Hill-Sachs lesion by the anchoring of both infraspinatus and posterior capsule into the defect. This effectively converts any present, off-track Hill-Sachs lesion into an extra-articular defect and reduces the risk of its engaging with the glenoid. Proponents of the procedure cite its relative lack of invasiveness and a reduced complication profile compared with the open Latarjet.14,18,21 The Latarjet procedure is commonly performed via an open, deltopectoral approach and involves detaching the coracoid process and reattaching it to the anteroinferior glenoid neck. Proponents of the procedure cite the additional stability provided via the dual advantages of bony augmentation and the sling effect as a result of rerouting the conjoint tendon.9,20
The purpose of this study was to compare the outcomes between arthroscopic BRR with the open Latarjet for the treatment of anterior shoulder instability in matched cohorts of patients with GBL in a subcritical zone from 13.5% to 24% in an active-duty military population with a high level of mandatory activity. We hypothesized that there would be no difference in recurrence rates or patient-reported outcomes between the 2 procedures.
Methods
This study is a retrospective cohort comparison of patients with anterior GHI who either underwent an arthroscopic BRR or an open Latarjet. All procedures performed were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. An institutional review board approved the study. All surgeries were performed by 1 of 2 fellowship-trained surgeons (K.S.M., N.P.) specialized in sports medicine surgery or shoulder and elbow surgery. This series consisted of a matched cohort of patients who underwent either an open Latarjet or a BRR from 2017 to 2022. During this time period, a total of 17 patients were unable to be matched in the study. The procedure performed was based on the discretion of the operative surgeons based on surgeon preference, patient preference, number of dislocations, and size of Hill-Sachs defects. Patients were matched based on age and GBL measurement between 13.5% and 24%. Inclusion criteria included anterior GHI, subcritical GBL (13.5%-24%), surgical treatment with an arthroscopic BRR or open Latarjet, and minimum follow-up of 2 years. Exclusion criteria included associated revision procedures and other coexisting glenohumeral pathology (superior labrum anterior-posterior tear, rotator cuff tear, fracture, acromioclavicular joint pathology, posterior labral tear, humeral avulsion of the glenohumeral ligament lesion, ALSPA lesion, and multidirectional instability). For all patients, the operative report was reviewed to verify the indications and procedure performed. Advanced imaging (computed tomography) was reviewed to measure GBL using the linear measurement percentage (LMP) method and glenoid track.6,17 Three fellowship-trained surgeons (K.S.M., J.P.S., C.A.C.) measured the bone loss of all patients who met the inclusion criteria. Demographic information included sex and age at first dislocation.
Patients meeting the inclusion criteria were contacted telephonically for final follow-up. Patients were queried whether they had sustained a recurrent shoulder dislocation or subluxation event after their instability procedure and if they were placed on any permanent physical restrictions because of their affected shoulder (permanent military profile). A dislocation was strictly defined as an injury requiring a manual reduction. A subluxation was defined as an injury that resulted in the shoulder's shifting/slipping or that subjectively caused a sense of instability. Recurrent instability was defined as either a recurrent dislocation or subluxation. Last, patients were asked to telephonically complete the Western Ontario Shoulder Instability Index (WOSI) and Single Assessment Numeric Evaluation (SANE).
Bone Loss Assessment
Measurements of humeral bone loss and GBL were determined using preoperative computed tomography. GBL was calculated using the LMP method. 13 Glenoid diameter (D), GBL (d), and the Hill-Sachs interval (HSI) were utilized to calculate the glenoid track (GT). The GT was calculated using the equation GT = 0.83 × D–d, and percentage GBL was calculated as percentage GBL = (d/D) × 100. HSI was measured as the largest distance from the medial-most edge of the Hill-Sachs lesion to the infraspinatus tendon insertion.
Surgical Technique
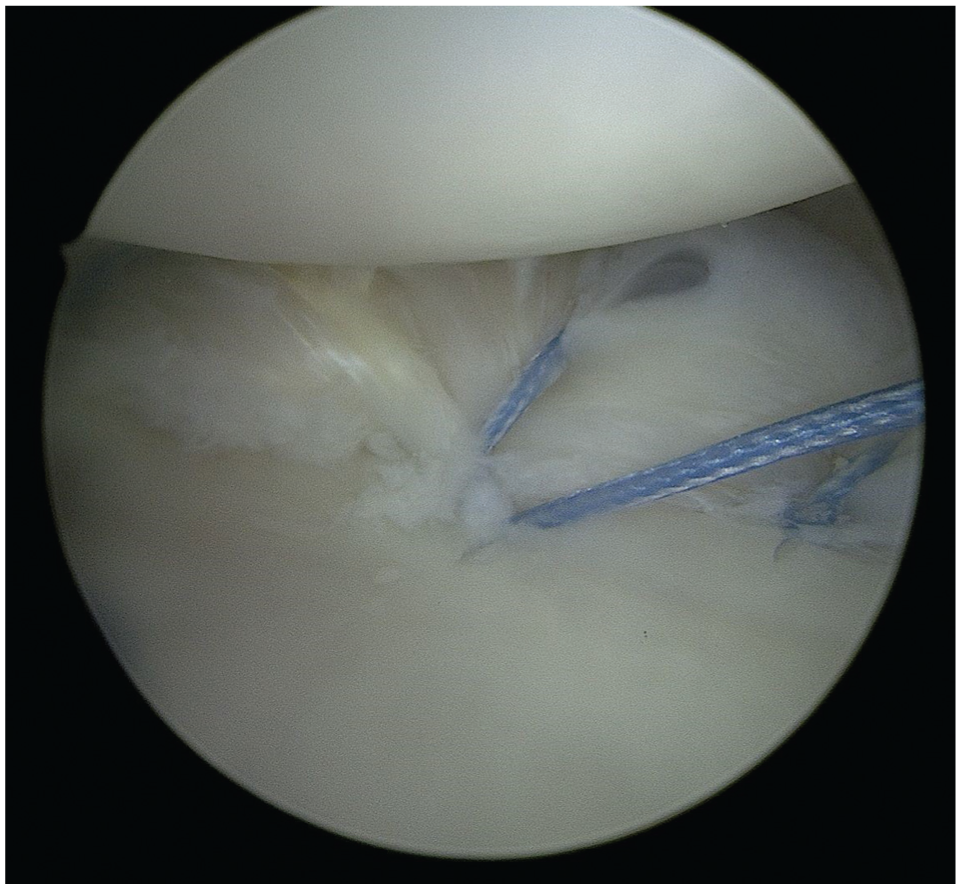
Surgeries were performed at 2 separate hospitals. All Latarjet procedures were performed via open technique with a European method of coracoid fixation. The European method refers to the orientation of the graft on the glenoid. In the European technique, the inferior portion of the harvested coracoid is placed against the anterior glenoid surface. All coracoid grafts were fixed with 2 fully threaded solid 4.0-mm screws (Arthrex). All grafts were made intra-articular with the capsule closed on top of the bone block. All Bankart repairs were performed in the lateral position with knotless suture anchors (SutureTak or 1.8-mm Fibertak; both Arthrex). All Bankart repairs had ≥3 knotless suture anchors. All suture anchors were passed around the labrum in a simple fashion and tensioned via a knotless mechanism. All Remplissage procedures were done via a suture staple technique. With the patients in the lateral position, two 1.8-mm Fibertak knotless anchors were inserted into the Hill-Sachs defect. The repair suture from one anchor was shuttled through the passing mechanism of the opposite anchor and vice versa. The repair sutures were then sequentially tensioned over the infraspinatus to create a knotless suture staple construct (Figures 1 -3).
Standard Bankart repair utilizing knotless anchor.

Arthroscopic view in the lateral decubitus position of a single knotless anchor placed in the Hill-Sachs defect.

Arthroscopic view in the lateral decubitus position of 2 knotless anchors placed in the Hill-Sachs defect for suture staple configuration.
Statistical Analysis
The primary outcome was recurrent instability after the index procedure. Recurrent instability was defined as a recurrent dislocation or subluxation episode. Secondary outcomes were permanent physical restrictions, WOSI score, and SANE score. Statistical analyses and tests were conducted with IBM SPSS Statistics (Version 18.0). Unpaired t tests were performed to compare cohorts with respect to recurrent instability rates, preoperative GBL, patient age at dislocation, permanent physical restrictions, SANE score, and WOSI score. Significance was assumed for P values <.05. Based on historical data, a power analysis was conducted with recurrent instability, SANE, and WOSI as the variables of interest.10,16 For recurrent instability, based on an alpha value of .05, 140 patients per group were required to achieve a power of 0.8. For both WOSI and SANE, based on an alpha value of .05, 14 patients per group were required to achieve a power of 0.8. The interrater reliability of GBL measurements was calculated using the intraclass correlation coefficient (ICC) with mixed 2-way measures and absolute agreement. Internal consistency of the glenoid measurements was determined using the Cronbach α.
Results
In the study period, there were 25 patients who underwent an arthroscopic BRR and 25 patients who underwent an open Latarjet. The mean follow-up was 51.3 months and 35.6 months, respectively. The mean GBL was 16.1% ± 3.2% for the arthroscopic BRR group and 19.3% ± 2.1% for the open Latarjet group (P = .002). There were no differences in the age at surgery (P = .77) or sex (P = .55) between the 2 groups (Table 1).
Demographic and Baseline Characteristics a

Data are presented as n or mean ± SD.
Overall, 5 patients experienced recurrent instability in the study groups (BRR, 3; Latarjet, 2; P = .64). In the BRR group, there were 2 recurrent dislocations and 1 recurrent subluxation. Two patients underwent revision surgery with a Latarjet. There was 1 recurrent dislocation and 1 recurrent subluxation in the Latarjet cohort. One patient underwent revision to a distal tibial allograft. The mean postoperative SANE score for the arthroscopic BRR group was 81.6% ± 12% and open Latarjet group was 84.2% ± 14% (P = .42); the WOSI score for the arthroscopic Bankart group was 64.6% ± 13.3% and open Latarjet group was 67.9% ± 9.1% (P = .44) (Table 2). Two patients who underwent an arthroscopic BRR were placed on permanent military restriction compared with three in the open Latarjet cohort (P = .64) (Table 2). All of these patients were on permanent military restriction due to their operative shoulder and inability to complete or perform military physical fitness test.
Postoperative Outcomes a

Data are presented as n or mean ± SD. SANE, Single Assessment Numeric Evaluation; WOSI, Western Ontario Shoulder Instability Index.
We identified 2 noninstability postoperative complications, both in the open Latarjet group compared with zero in the BRR cohort (P = .49) There was 1 ulnar neuritis and 1 axillary nerve neurapraxia. In both situations, the symptoms fully resolved within 2 years (Table 3).
Postoperative Complications a

Data are presented as n or n (%).
The mean difference in GBL measurements was 0.665° (95% CI, 0.569°-0.750°). The interrater reliability, as measured by the ICC for GBL, was 0.898 (95% CI, 0.859-0.928). The Cronbach α was .90.
Discussion
The primary finding of this study was that there was no difference in recurrent instability between matched cohorts of patients with subcritical GBL who underwent either arthroscopic BRR or open Latarjet. Furthermore, there was no difference in functional outcomes at 2 years postoperatively. Last, there was no difference in return-to-duty rates between the 2 groups.
There continues to be significant debate regarding the optimal treatment for patients with subcritical bone loss of the glenoid. Current available literature does not offer many direct comparisons between these 2 commonly utilized surgical techniques, with the handful of published studies offering no significant postoperative advantage of one technique over the other.1,3,8,14,21 One systematic review by Haroun et al 13 published in 2020 and another by Gouveia et al 12 published in 2021 identified only 4 comparative studies in the current literature examining BRR versus the Latarjet procedure. Pooled meta-analysis performed by Haroun et al of postoperative functional outcome metrics (visual analog scale pain score and Rowe score) determined no difference between the 2 surgical techniques. Similarly, the authors found no difference between either procedure with respect to postoperative range of motion and recurrent instability rates. Pooled analysis did demonstrate a significantly higher rate of other complications postoperatively for patients who underwent open Latarjet as compared with BRR (17 total vs 2, respectively), with the Latarjet complications involving either postoperative infection, hardware irritation, failure of bony healing, postoperative stiffness, and transient suprascapular nerve injury.8,13,21 It is important to note, however, that only 2 of the 4 examined studies reported the mean preoperative GBL of each cohort.8,21
A comparative study of the 2 techniques by Horinek et al 14 published in 2022 demonstrated similar results. These authors found no significant differences between groups with postoperative functional outcome metrics (including both WOSI and SANE scores), range of motion, instability recurrence, and return to sport. Notably, these authors demonstrated a lower rate of other complications within their Latarjet cohort, with the only complication in the referenced study being a single case of an infected postoperative hematoma requiring debridement. 14 The similar outcomes postoperatively are notable, particularly considering the mean preoperative bone loss in their Latarjet and BRR cohorts were 25.1% ± 9.0% and 25.8% ± 7.8%, respectively. This was significantly higher than the preoperative bone loss in 2 previous comparative studies that had documented that metric,8,21 although in this referenced study those means fell above the accepted upper threshold for subcritical bone loss (24%). 19
The most recent study comparing both surgical techniques was published in 2024 by Charles et al 7 and boasts one of the largest patient cohorts examined thus far with 108 patients total. The authors included 38 revision cases in their cohort and ultimately found no significant differences in outcome between the 2 procedures in both the primary and the revision situations. As with other published literature comparing the 2 techniques (except for Horinek et al’s 14 study), the mean preoperative GBL present in both the BRR and the Latarjet cohorts fell below the commonly accepted lower limit of subcritical bone loss of 13.5%.7,19 The results of the referenced study are also confounded by a statistically significant difference of the mean preoperative GBL between the BRR and Latarjet cohorts (8.3% and 13.2%, respectively). Nevertheless, the Charles et al study added information not previously documented in the literature with respect to their revision cases. Additionally, these authors documented a mean follow-up of 4.3 years, which is the longest documented in any comparative study of these 2 techniques to date.
Our study demonstrated similar results to these previous studies, with no apparent differences between our 2 age-matched cohorts with respect to postoperative functional outcome metrics and instability recurrence. Notably, all patients were active-duty military and were thus subjected to a high level of mandatory activity postoperatively. To our knowledge, aside from the study by Horinek et al, 14 there is no other comparative study of these operative techniques with a documented mean preoperative GBL >13.5%. Our findings affirm Horinek et al’s conclusion that BRR can be a viable intervention for patients with preoperative subcritical GBL approaching 24%.
It appears that in certain cases of GHI with significant GBL, BRR may be just as effective as the Latarjet procedure, without the risk of an increased postoperative complication profile. Although the current study and others published previously have demonstrated the parity of the 2 procedures in patients with subcritical bone loss, there is a dearth of prospective and highly powered studies. This question should continue to be addressed in the future, with prospective literature and with longer-term follow-up of large cohorts out to ≥5 years.
Limitations
This study is not without limitations. The main limitation of this study is that the cohort size was small. Our pre hoc power analysis demonstrates that this study is adequately powered with respect to the postoperative WOSI and SANE scores, but the study is underpowered with respect to postoperative instability. Treatment choice was not randomized and was left to shared patient/surgeon decision making. The potential bias because of this is evident with a significant difference in mean preoperative GBL between the 2 cohorts (P = .002), although both means fell within the subcritical zone. The 2 cohorts were largely homogeneous, although they were only matched by age and not by other variables. Postoperative range of motion was not measured. External rotation loss has been reported as a possible complication of Remplissage and this was not included in our study. Finally, our follow-up was ≥2 years, but longer follow-up will be needed to better determine the true instability recurrence rate in this patient population.
Conclusion
In our small cohort of active-duty military patients with subcritical GBL, there was no difference in recurrent instability between arthroscopic BRR compared with open Latarjet. Additionally, there was no significant difference in postoperative SANE or WOSI scores, complications, or the number of patients placed on permanent military restriction.
Footnotes
Final revision submitted August 10, 2025; accepted September 8, 2025.
Presented at the annual meeting of the AOSSM, Nashville, Tennessee, July 2025.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Madigan Army Medical Center Institutional Review Board (protocol No. 221092).