
Abstract
Background:
The intricate relationship between anterolateral ligament (ALL) and Kaplan fibers (KF) injuries in acute traumatic anterior cruciate ligament (ACL) tears presents a diagnostic challenge. Understanding these associations is crucial for enhancing therapeutic strategies and patient outcomes.
Purpose:
To elucidate the prevalence of ALL and KF injuries among patients with acute ACL tears and examine their correlations with other imaging findings.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A retrospective review of magnetic resonance imaging (MRI) was performed for patients with knee pain or instability, leading to an MRI evaluation between April and August 2022. The inclusion criteria were primary ACL tears diagnosed via MRI within 6 weeks after injury, excluding cases with concurrent posterior cruciate ligament, medial collateral ligament, or lateral collateral ligament injuries. Out of the initial cohort, 51 patients met the inclusion criteria, all with recent trauma and timely imaging.
Results:
Our results highlighted that 21.6% of these patients had ALL injuries, whereas a notably higher proportion (33.3%) exhibited KF injuries. We observed bone contusions on the medial and lateral femoral condyles in 3.9% and 41.2% of patients, respectively. Similarly, the medial and lateral tibial condyles presented contusions in 31.4% and 49% of the cases, respectively, with a subset of 29.4% demonstrating both tibial condyle involvement.
Contusions on the lateral femoral and tibial condyles were used as indicators of pivot-shift injuries, identified in 41.2% of cases (n = 21). Subgroup analysis revealed a significant association between these injuries and KF damage, present in 71.4% of cases (odds ratio, 33.8 [95% CI, 6.04-188.53; P < .001), compared with a lower incidence of ALL injuries at 28.6% (P = .31). This suggests a stronger link between KF injuries and pivot-shift mechanisms, emphasizing the role of KF in knee trauma. In addition, KF injuries were more common in patients with lateral meniscal injuries, although this finding was not statistically significant (P = .10).
Conclusion:
Surgeons should focus more on detecting KF injuries than ALL injuries when ACL tears are accompanied by lateral femoral and tibial condyle contusions, as these may play a crucial role in the injury mechanism.
Keywords
The anterior cruciate ligament (ACL) is a frequently injured ligament within the knee joint, playing a crucial role in stabilizing this intricate structure. 16 Most ACL ruptures are observed in athletes and typically result from noncontact mechanisms. Specifically, these injuries often arise during a noncontact pivoting event, characterized by anterior translation of the tibia relative to the femur when the knee is in a state of slight flexion and subjected to a valgus force with external or internal rotation of the tibia or the femur, respectively.18,24 ACL injuries are notably prevalent, impacting 6.2% of high school athletes and 6.9% of adolescent athletes, with a higher occurrence rate of 8.4% among women compared with 6% in men. 11
The anterolateral complex (ALC) of the knee is instrumental in maintaining the knee’s rotational stability and composed of 2 distinct layers—a superficial layer and a deeper layer. These layers become strained during the internal rotation of the tibia relative to the femur, aiding in the stabilization of the ALC. The superficial layer includes the iliotibial band (ITB) and Kaplan fibers (KF), while the deeper layer contains the anterolateral knee capsule and the anterolateral ligament (ALL).5,10,15 These structures work in coordination with the ACL to mitigate excessive anterior translation and internal rotation of the tibia, playing a pivotal role in the knee's biomechanical function. Simultaneous injury to one or both of these ligaments, along with the ACL, can exacerbate anterolateral rotatory instability (Figure 1). 15
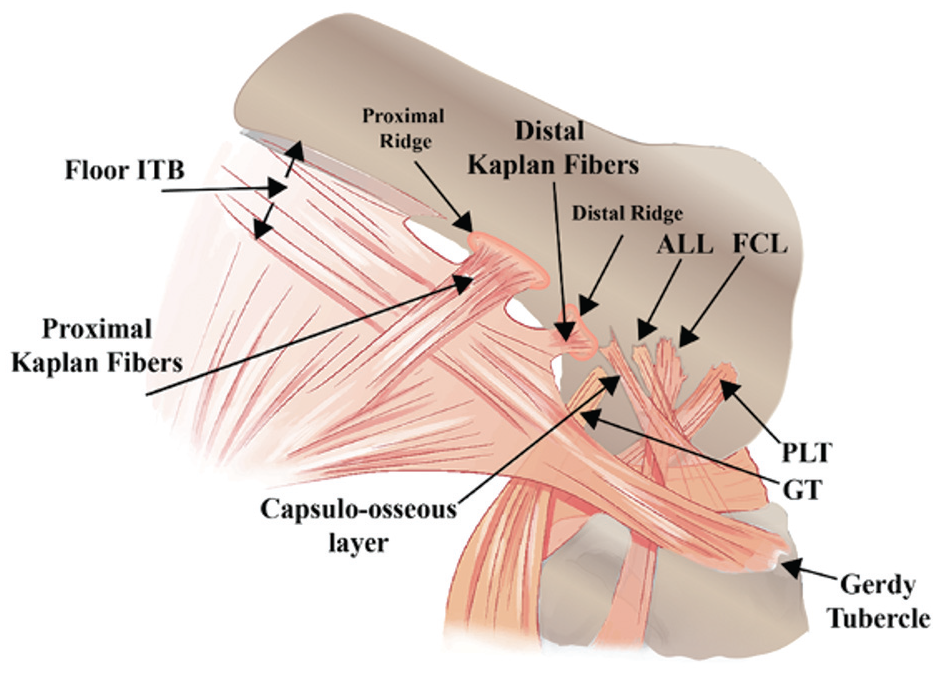
Anatomic diagram of the ALC of the knee. The KF are part of the ITB complex and play a role in stabilizing the lateral aspect of the knee. The proximal fibers arise 5-7cm proximal to lateral femoral epicondyle, while the distal fibers 2-4 cm proximal to it. The ALL is a distinct ligamentous structure that has gained recognition for its role in controlling the rotational stability of the knee. The FCL, also known as the LCL, is a band of tissue connecting the femur to the fibula. The ITB is a longitudinal fibrous reinforcement of the fascia lata, which extends down the outside of the thigh from the pelvis to the tibia. The Capsulo-osseous layer refers to the ITB’s deep layer that has fibrous attachments to the distal femur. Gerdy tubercle is a bony prominence on the lateral aspect of the tibia where the ITB inserts, providing an anchor point for the ITB. The PLT originates from the lateral femoral condyle and travels to the posterior aspect of the tibia. It is essential for initiating knee flexion and unlocking the knee from its fully extended position. The GT is a small tubercle found on the femur that serves as the origin for part of the gastrocnemius muscle. ALC, anterolateral corner; ALL, anterolateral ligament; FCL, fibular collateral ligament; GT, gastrocnemius tubercle; ITB, iliotibial band; KF, Kaplan fibers; LCL, lateral collateral ligament; PLT, popliteus tendon.
In the context of ACL deficiency, the escalation of anterior tibial translation and internal tibial rotation exacerbates rotatory instability, particularly when the ALC is impaired.6,19 The ITB, especially through the KF’s deep attachments to the distal femur, is critical in mitigating internal tibial rotation, pivot shifts, and anterior tibial conversion, highlighting the necessity of intact cruciate ligaments for knee stability. 23
The role of extra-articular anterolateral structures in maintaining anterolateral stability in post-ACL reconstruction (ACLR) has been reexamined in recent years to evaluate whether it optimizes the outcome of ACLR.9,13 In cases of simultaneous ACL and anterolateral corner injuries, performing an ACLR without addressing the ALC may result in persistent anterolateral rotatory instability, increasing the risk of ACLR failure. Therefore, recognizing these injuries is essential for planning an appropriate surgical approach to ensure anterolateral rotatory stability. Concomitant lateral extra-articular tenodesis is beneficial, as it protects the intra-articular ACL graft during healing and acts as a secondary stabilizer, helping to control anterolateral rotatory instability during subsequent sports activities.1,2,5,8
The importance of detecting fiber injuries in preoperative imaging is highlighted by the challenges in visualizing extra-articular fibers during arthroscopic ACLR. This detection is crucial for planning an extra-articular approach. In addition, accurate reconstruction of both the KF and the ALL is essential, given their differing roles in anterolateral rotatory stability at various degrees of knee flexion. The KF provide anterolateral rotatory stability at >30° of knee flexion, while the ALL provides this stability at <30° of knee flexion. 15
Identifying KF injury in preoperative magnetic resonance imaging (MRI) helps to schedule extra-articular reconstruction of these fibers after the initial ACLR in the presence of anterolateral laxity. Considering their role in preventing anterolateral rotatory laxity, the reconstruction of these fibers is very important in reducing future ACLR failure.
Despite advancements in MRI for evaluating the ALL and the KF, there is still a lack of comprehensive understanding regarding the frequency and characteristics of injuries to these structures in patients with ACL tears. Recent perspectives and studies have emerged to assess the KF and the ALL in patients with ACL injuries.12,14 Similarly, we aimed to evaluate these structures and speculate on the injury mechanisms and secondary imaging findings related to these structures in the context of ACL injuries. This study aimed to fill this knowledge gap by investigating the incidence of ALL and KF injuries in patients with acute ACL tears using MRI. By assessing the association between injuries to the ALL and the KF, this research seeks to shed light on their implications for ACLR strategies, potentially guiding improvements in surgical practices and patient outcomes.
Methods
Study Design and Patient Selection
This cross-sectional retrospective study received approval from the institutional ethics committee. We examined MRI scans of 420 consecutive patients experiencing knee pain who were directed to our orthopaedic clinics and underwent knee MRI scans at our institution from April to August 2022.
The study focused on patients who experienced primary complete or high-grade partial tears in ACL without significant tears in the posterior cruciate ligament (PCL), medial collateral ligament (MCL), or lateral collateral ligament (LCL) and underwent MRI assessments within 6 weeks after injury. Out of 420 knee MRI reviews, 65 patients were identified with ACL injuries linked to recent traumatic events. To minimize the effect of such conditions on the evaluation of ligamentous or capsular components, 11 of these patients were excluded because of knee deformities or signs of degenerative changes in the knee joint. Consequently, 54 patients with ACL tears were initially selected. However, 3 patients were later excluded because >6 weeks had elapsed from the time of the injury to their MRI scan. Ultimately, 51 patients were included in the study, all of whom had a history of recent trauma, with MRI images acquired within 6 weeks of the injury.
MRI Procedure
Patients underwent MRI scans using either 1.5- or 3-T MRI systems (specifically, the Discovery MR350 and Discovery MR750 models; GE Healthcare). These scans were performed with a dedicated knee coil designed for phased array use. The imaging protocol adhered to our institution’s standard guidelines, which include multiple-plane imaging—axial, coronal, and sagittal.
The imaging parameters in the axial, coronal, and sagittal planes are as follows:
Proton density fat–suppressed (PD FS) images were acquired with a repetition time (TR) of 2800 ms and an echo time (TE) of 44 ms. The matrix size was set to 320 × 192 for axial images and 288 × 192 for coronal and sagittal images. The field of view (FOV) was maintained at 16 cm with a slice thickness of 4 mm.
Coronal T1-weighted images were obtained with a TR of 490 ms, a TE of 9 ms, a matrix size of 288 × 192, a FOV of 16 cm, and a slice thickness of 4 mm.
Sagittal T2-weighted images had a TR of 3500 ms, a TE of 99 ms, a matrix size of 288 × 192, a FOV of 16 cm, and a slice thickness of 4 mm.
Image Review
All MRI sequences underwent a thorough review by a musculoskeletal radiologist (S.K.) specializing in the intricate anatomy and imaging characteristics of the knee, with a particular focus on the KF and the ALL. To evaluate intrarater reliability, a radiologist (S.K.) examined 26 patients twice over 4 weeks. The review aimed to identify the integrity of these fibers across axial, coronal, and sagittal views, categorizing them as either intact, injured, or not visualized. This evaluation extended to both the proximal and distal aspects of the KF.
The KFs are identified through the detection of low signal structures in PD/T2 sequences, observable across 2 consecutive slices, with the superior lateral geniculate artery serving as a landmark for delineation of the KF, as well as the insertion site of the lateral head of the gastrocnemius muscle (Figure 2). The ALL was recognized as a band of low signal intensity, originating from the lateral femoral epicondyle and inserted distally into the lateral meniscus and the lateral tibial plateau. 14
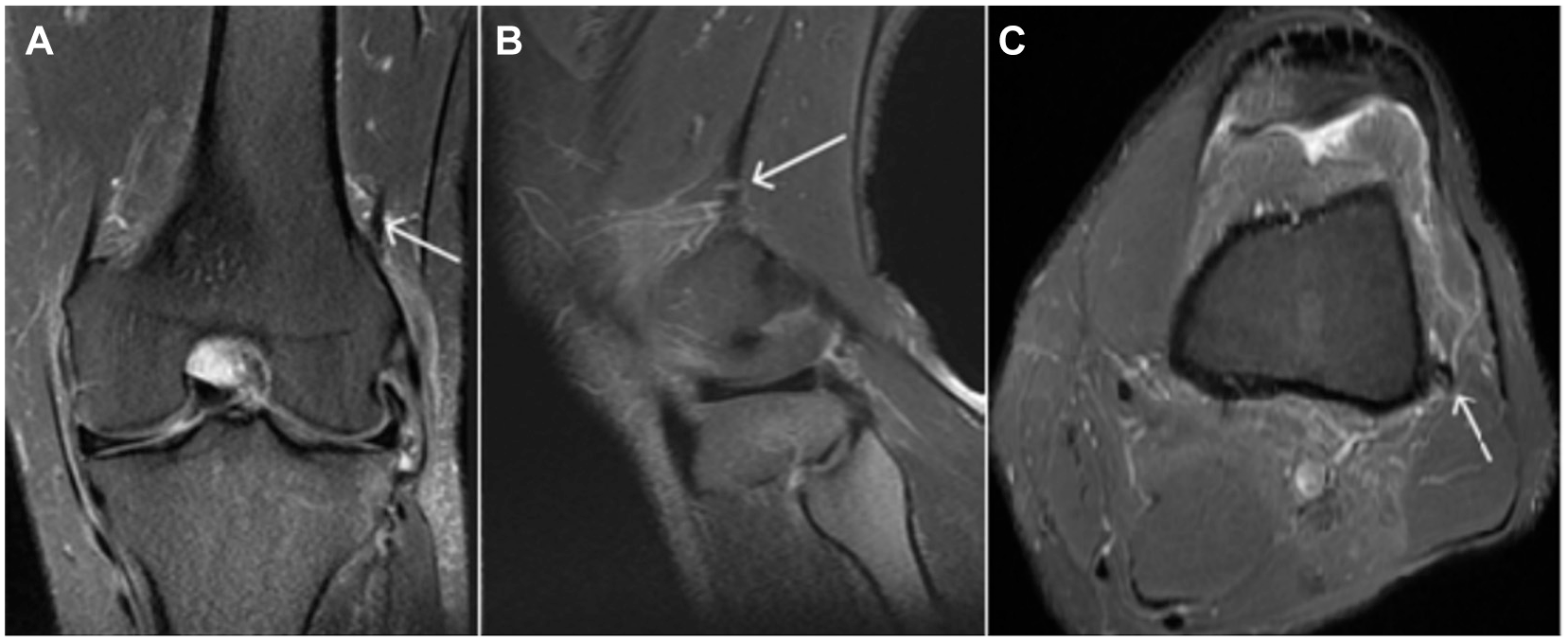
Normal Kaplan fibers. (A) Coronal, (B) sagittal, and (C) axial views of the knee. The PD FS MRI sequence shows normal Kaplan fibers. White arrows show intact Kaplan fibers. MRI, magnetic resonance imaging; PD FS, proton density fat–suppressed.
The KF and the ALL are classified as injured when discontinuities are detected or when there is an abnormal increase in the PD/T2 signal intensity along the extent of the fibers (Figure 3).
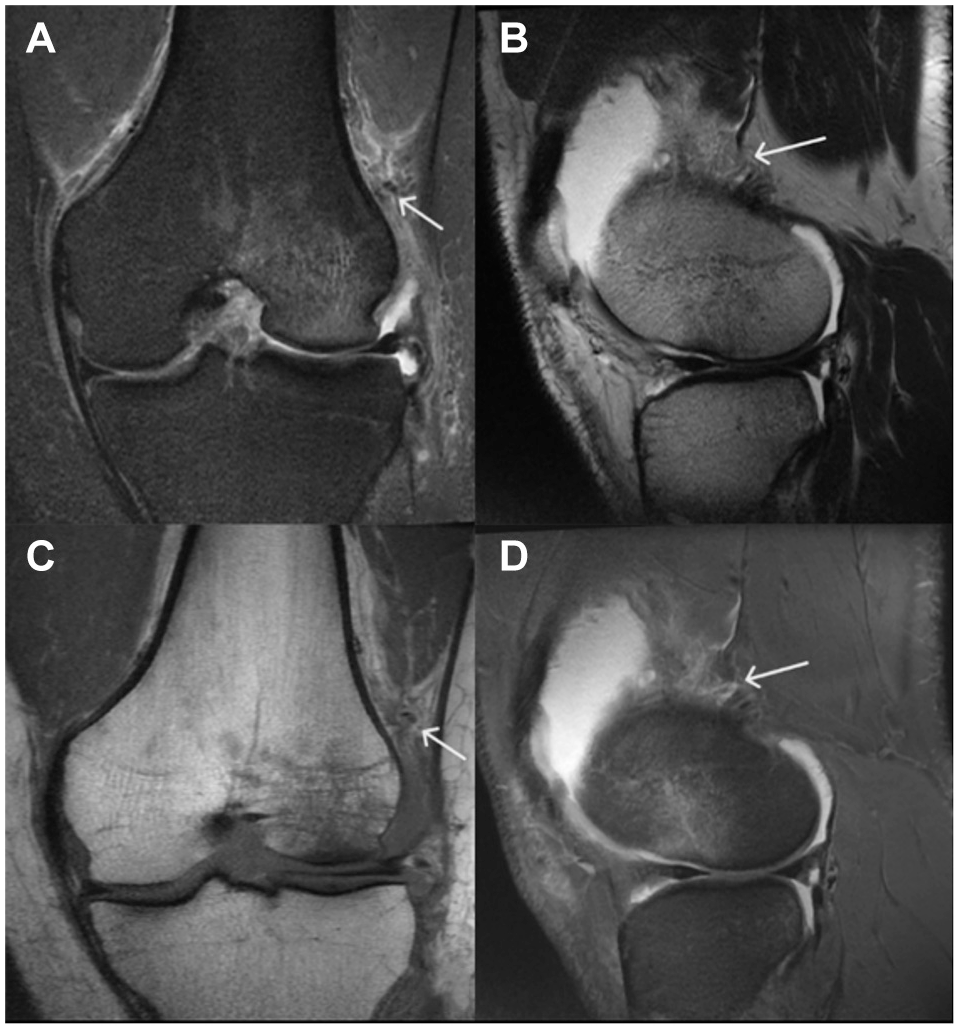
Kaplan fiber injury. (A) A PD FS coronal image. (B) A T2-weighted sagittal image. (C) A T1-weighted coronal image. (D) A PD FS sagittal image. White arrows show injured Kaplan fibers in a patient with an ACL tear. ACL, anterior cruciate ligament; PD FS, proton density fat–suppressed.
In addition, the assessment included the examination of bone marrow edema or contusion in the medial and lateral condyles of both the femur and the tibia, showing an increase in bone marrow signal intensity in PD FS sequences. Injuries to the ALL and other associated findings were also examined and documented.
Statistical Analysis
We conducted the analysis using SPSS Version 26 (IBM Corp) and applied both descriptive and inferential statistical methods. Descriptive statistics included calculating the mean and standard deviation for continuous variables. For categorical variables, frequencies were computed to understand their distribution. Inferential statistics involved the use of t tests for comparing means of continuous variables between the 2 groups, and the chi-square test or the Fischer exact test (when appropriate) for comparing proportions in categorical variables. Odds ratios (OR) were calculated when we encountered statistically significant associations between categorical variables yielded in 2*2 cross tables. In addition, 95% CIs of these ORs were calculated. The Kolmogorov-Smirnov test was utilized to assess the normality of data distribution. P < .05 was considered statistically significant.
Results
Patient Characteristics and ACL Injury Profile
In total, 51 patients were enrolled in the study. The mean age of patients was 31.8 ± 7.8 years (range, 18-49 years), and 44 participants (86.3%) were male. Among these patients, 41 participants (80%) had a noncontact mechanism of injury. Every participant was diagnosed with an ACL tear, and 13 participants (25%) also exhibited a low-grade sprain in the proximal LCL. Furthermore, 6 participants (11%) had a sprain in the MCL, with 2 of them experiencing a high-grade sprain and the remaining 4 exhibiting only a low-grade sprain in either the deep or superficial fibers.
Femoral and Tibial Condyle Involvement
Involvement rates for the femoral condyle were recorded at 4% (2 patients) medially and 41.2% (21 patients) laterally, with a single case showing involvement of both the medial and lateral femoral condyles. Moreover, medial and lateral tibial condyle involvement rates stood at 31.4% (16 patients) and 49% (25 patients), respectively. Notably, 15 patients (29.4%) demonstrated involvement in both the medial and lateral tibial condyles.
Pivot Injury Analysis
Considering the combined lateral involvement of the tibial and femoral condyles as an indicator of pivot injury, a total of 21 patients (41.2%) with such injuries were identified, and all of these patients also had noncontact mechanisms of injury. Among these 21 cases of pivot injury, there was 1 instance of medial femoral condyle involvement. Furthermore, 15 out of the 21 patients with pivot injuries also sustained injuries to the medial tibial condyle. In addition, there was 1 case (2%) of medial retinaculum involvement, whereas no cases of lateral retinaculum involvement were observed. Involvement of the ALL was noted in 11 patients, accounting for 21.6% of the cases, and 10 participants (91%) had a history of noncontact injury mechanisms.
KF Involvement
We evaluated the involvement of the KF in both proximal and distal sections, utilizing axial, sagittal, and coronal views for comprehensive assessment. By classifying any injury to the proximal or distal sections of the KF as indicative of KF involvement, we identified that 17 patients (33.3%) exhibited KF injuries. Among the imaging views, the sagittal view proved most effective for visualizing distal KF injuries, with a 96.1% visualization rate, while the axial view was preferable for observing proximal KF injuries, achieving a 53% visualization rate. The MRI findings related to the assessment of the KF in various views are detailed in Table 1.
Assessment of Proximal and Distal Kaplan Fiber Injuries Using Axial, Sagittal, and Coronal MRI in Patients With ACL Tears a

Data are presented as n (%). ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
In patients with KF injury, 14 participants (82%) had a history of noncontact injury mechanisms. To assess intrarater reliability, a radiologist (S.K.) assessed 26 patients twice in 4 weeks. When we considered KF involvement in the case of positive MRI in at least 1 of the mentioned views—integrating data of axial, sagittal, and coronal views—the Kappa coefficient was 0.92 and 0.62 for distal and proximal parts of the KF, respectively (P < .001 for both). This coefficient was 0.84 (P < .001) when assessing the distal KF in the sagittal view. The Kappa coefficient was 0.6 (P < .001) when assessing the proximal KF in the axial view. The Kappa coefficient of agreement was 1 when assessing the ALL (P < .001).
Popliteofibular Ligament and Meniscus Findings
A sprain of the popliteofibular ligament was observed in 10 patients, accounting for 19.6% of the cases. In terms of the popliteomeniscal fascicles, involvement of the superior and inferior fascicles was noted in 2 (3.9%) and 12 (23.5%) patients, respectively.
The details regarding the medial and lateral meniscus findings are provided in Table 2. Among 8 patients with lateral meniscal injury, 5 patients showed KF injuries (62.5%), while in 42 patients with intact lateral meniscus, 12 (28.6%) showed KF injuries (P = .10).
MRI Analysis of Medial and Lateral Meniscus in Patients With ACL Tears a

Data are presented as n (%). ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
Association of Different Injuries
We evaluated the association of pivot injury (determined by contusions of the lateral femoral and tibial condyles) with injuries to the proximal and distal sections of the KF.
In the presence of pivot injuries, 61.9% (13/21) of patients exhibited involvement of the distal KF, which was in stark contrast to patients without pivot injury that showed no distal KF involvement (0/29) (OR, 2.63 [95% CI, 1.52-4.53]; P < .001).
Furthermore, among those with pivot injuries, 68.8% (11/16) showed proximal KF involvement, compared with just 12.5% (2/16) among those without pivot injuries (OR, 15.4 [95% CI, 2.50-95.05]; P = .004).
Age and sex were found to have no significant association with KF involvement (P > .45 for both). Analyzing the involvement of both proximal and distal parts of the KF together, there were 17 instances (33.3%) of at least 1 compartment of the KF being affected. Of these, 9 patients had both proximal and distal compartments involved. In 4 cases, only the distal compartment showed involvement while the proximal compartment remained unaffected. Another 4 patients had proximal compartment involvement, but the distal part was not evaluated. A total of 33 patients exhibited no KF involvement (64.7%), and the ligament’s condition could not be assessed in 1 case.
In the context of pivot injuries, 15 out of 21 patients (71.4%) exhibited involvement of the KF, in contrast to only 2 out of 29 patients (6.9%) without pivot injuries, demonstrating a highly significant difference (OR, 33.8 [95% CI, 6.04-188.53]; P < .001).
Furthermore, the association between ALL involvement and pivot injuries was not statistically significant, with 28.6% (6/21) of patients with pivot injuries showing ALL involvement compared with 16.7% (5/30) of patients without pivot injuries (P = .31), indicating that ALL involvement does not significantly correlate with pivot injuries in this sample.
When analyzing the combined involvement of ALL and KF, 23 patients (45.1%) exhibited involvement in either or both structures. Specifically, 5 patients had involvement in both ALL and KF, 12 had involvement solely in KF, and 6 had involvement only in ALL (Table 3).
Incidence and Co-occurrence of Anterolateral Ligament and Kaplan Fiber Injuries During ACL Tears a

Data are presented as n (%). ACL, anterior cruciate ligament; ALL, anterolateral ligament; KF, Kaplan fiber.
In the 21 patients with pivot injuries, 16 (76.2%) showed involvement of either KF or ALL, in contrast to just 7 out of 30 patients (23.3%) without pivot injuries, indicating a significant association (OR, 10.5 [95% CI, 2.8-38.5]; P < .001).
Discussion
In patients experiencing ACL tears, the ALL and KF play crucial roles in maintaining the anterolateral rotational stability of the knee, making imaging insights into these structures essential. 22 Regarding our observations, the MRI approach is better suited for evaluating distal KF, as they were unassessable in only 1 case, in contrast to the proximal KF, which could not be assessed in 37.3% of cases.
In our research, one-third (33.3%) of the patients with ACL injuries also exhibited injuries to the proximal or distal KF. This percentage is lower compared with the findings of the study by Marom et al, 15 which reported KF injuries in 50% to 58% of patients undergoing evaluation for primary acute ACL injuries. Also, in their recent study, Leao et al 14 reported KF and ALL injuries in 50% and 71% of their patients, respectively.
Our reported KF injuries percentage is higher than the study by Guruprasad et al, 12 in which KF injuries were reported in 17% of patients, which could be attributed to a lack of time threshold in their exclusion criteria compared with our 6-week post-trauma threshold.
In a 2020 study conducted by Batty et al, 3 MRI evaluations of patients with ACL ruptures indicated an enhanced probability of KF lesions when assessments were performed within 90 days after injury. Their findings revealed that KF injuries were present in 18.6% of cases with ACL disruptions, a prevalence significantly lower than that reported in our study. This difference may be attributed to the distinct methodological approaches adopted—our study set the exclusion threshold at 6 weeks after trauma—compared with their 90-day benchmark. Moreover, the study by Batty et al, 3 also established an association between KF ruptures and concurrent injuries to the lateral ligament, lateral meniscus, and bone bruising on the posteromedial aspect of the tibia, findings that were congruent with those reported in our research.
Berthold et al 4 study revealed that injuries to the KF and ACL were co-occurring in about 53% and 56% of cases examined, demonstrating that most patients with ACL ruptures also had concurrent injuries to the KF.
In our study, one-third (34%) of participants with noncontact injury mechanisms exhibited injuries to the proximal or distal KF, and among patients with KF injuries, 82% had a noncontact mechanism of injury. These findings may be attributed to rotational forces involved in noncontact injuries, such as the pivot-shift mechanism, which affect the KF and the ALL as part of the anterolateral rotatory stabilizer more than contact injuries do. In our research, injuries to the KF were observed more frequently than injuries to the ALL in cases of ACL rupture, a finding that contrasts with the results from Runer et al, 17 Leao et al, 14 and Guruprasad et al, 12 where ALL injuries were reported to occur at a higher frequency than KF injuries in patients with ACL tears.
In light of the varying results from the studies mentioned, including our own, there is a discrepancy in the reported incidence of KF injuries associated with ACL tears. This variation may stem from differences in study designs and patient selection criteria. The clinical relevance of these findings, and whether they align with one another, introduces a growing concern regarding the preoperative identification of KF injuries to inform the appropriate surgical strategy.
In our research, we assessed the pattern of bone contusion in each subject, identifying a statistically significant correlation between KF injuries and the presence of contusions on the lateral femoral and tibial condyles. This correlation serves as a radiological indicator of the trauma mechanism involved. Numerous studies suggest that the co-occurrence of ACL tears and lateral femoral and tibial condyle contusions is indicative of a pivot-shift injury mechanism. Based on these findings, we propose that the presence of both ACL tear and KF injury is significantly linked to the pivot-shift injury mechanism.
However, our study did not find a significant statistical relationship between the pattern of condylar contusion—indicative of a pivot injury—and injuries to the ALL. We infer that in traumatic scenarios involving a pivot-shift mechanism where the ACL is compromised, an associated injury to the KF is statistically significant. Given the crucial role of these fibers in anterolateral rotatory stability, we suggest that in cases of ACL tears with radiological signs of a pivot-shift injury mechanism—such as lateral femoral and tibial condyle contusion—surgeons should meticulously evaluate anterolateral rotatory stability. This evaluation is essential for devising an effective surgical plan that addresses all aspects of the injury.
In the context of acute ACL injuries, the study by Devitt et al 7 highlighted that KF injuries were relatively uncommon, occurring in only 17.6% of cases—a contrast to our findings where approximately one-third of ACL tear cases involved KF injuries. In addition, their research confirmed a correlation between KF injuries and lateral meniscal tears detected during ACLR.
Our research presents findings that align closely with those reported by Van Dyck et al 20 regarding the co-occurrence of KF injuries in conjunction with ACL tears. However, while their study noted an association between ALL injuries and ACL tears in 57% of cases, our data indicate that concomitant injuries to the ALL and ACL were present in only 21.6% of instances.
Our research indicates a 45.1% coincidence of injuries to the ALL or KF in association with ACL tears. Given the crucial function of these structures in preserving anterolateral rotatory stability after ACLR, recognizing the prevalence of such concurrent injuries is essential for planning effective surgical interventions to mitigate future rotatory instability. In addition, our findings reveal that 9.8% of patients with acute ACL tears also had simultaneous injuries to both the KF and the ALL. This incidence aligns closely with the 12.7% rate of combined injury reported by Runer et al. 17 Collectively, these results suggest a relatively low frequency of simultaneous ALL and KF damage in acute ACL injury scenarios.
In our analysis of patients with ACL tears exhibiting a pivot-shift contusion pattern, we observed that 71.4% had associated injuries to the KF, whereas only 28.6% demonstrated injuries to the ALL.
In our study, we excluded complete tears of the MCL, LCL, and PCL to minimize the complexity of injury mechanisms. This approach allowed us to focus on ACL injuries and their associated injuries without the confounding effects of severe multiligamentous damage, which involves more complex mechanisms. Furthermore, our research indicates a higher incidence of medial meniscal injuries (31.4%) compared with lateral meniscal injuries (15.7%) among patients with ACL tears, diverging from previous studies such as those by Venkataraman et al, 21 which reported a higher prevalence rates for lateral meniscal tears in the context of acute ACL ruptures. Notably, within the subset of patients with lateral meniscal injuries, 62.5% exhibited concurrent KF injuries, in contrast to 28.6% among those with intact lateral menisci.
Limitations
Incorporating 3-dimensional PD-weighted sequences into the standard knee MRI protocol can enhance the visualization of the ALL and KF, as demonstrated by Guruprasad et al. 12 Despite this limitation in our protocol, we aimed to assess these structures using the standard knee MRI in routine clinical practice, guiding radiologists and clinicians to be more vigilant and consider additional assessments when needed.
This study is also limited by its retrospective design, relying on existing MRI in a single center data that may not encompass all relevant clinical details or comprehensive patient outcomes. The pronounced overrepresentation of men in our study cohort reflects cultural norms of sports engagement in our country. This demographic skew could potentially limit the broader applicability of our findings to more diverse populations. In addition, while the exclusion criteria for significant concurrent ligament injuries were necessary to focus on ACL-related outcomes, they may have inadvertently excluded cases with complex knee injuries that could affect the observed associations between ALL and KF injuries and other imaging findings. Therefore, it is recommended that future research continue to explore these relationships—particularly the predictive factors linking KF injuries with ACL tears—to refine surgical and diagnostic approaches.
Conclusion
Our study shows that in cases of ACL rupture, the presence of bone contusions on the lateral femoral and tibial condyles, indicative of a pivot mechanism of injury, should alert surgeons to a higher likelihood of KF injury relative to ALL injury. Although both KF and the ALL are critical for anterolateral rotatory stability, they necessitate distinct surgical approaches—particularly in terms of tenodesis. Therefore, identifying these specific injury patterns can assist in preoperative planning by enabling surgeons to tailor their approach to the individual structural damage observed. This strategic focus could enhance the efficacy of surgical interventions aimed at restoring knee stability.
Footnotes
Final revision submitted July 20, 2024; accepted September 5, 2024.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tehran University of Medical Sciences (ref No. IR.TUMS.MEDICINE.REC.1400.1462).