
Abstract
Background:
The accurate identification of the anterior cruciate ligament (ACL) tear location is important for preoperative planning, as it influences the choice between reconstruction or repair procedures, particularly for proximal tears. Therefore, there is a need for a reliable preoperative tool that yields findings consistent with diagnostic arthroscopy.
Purpose:
To evaluate the reliability of preoperative magnetic resonance imaging (MRI) for determination of the ACL tear location.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
Patients diagnosed with a full-thickness ACL tear between January 2022 and January 2024 were included in this study. The modified Sherman classification was used to categorize the ACL tear location into 5 types: I (proximal avulsion tear), II (proximal tear), III (midsubstance tear), IV (distal tear), and V (distal avulsion tear). There were 2 musculoskeletal radiologists who reviewed preoperative MRI scans, whereas diagnostic arthroscopic video recordings were retrospectively reviewed by 2 orthopaedic surgeons. The MRI findings were then compared with the arthroscopic findings, with diagnostic arthroscopy serving as the reference standard for the exact tear location. The Fleiss kappa (κ) was used to assess the reliability of the MRI findings.
Results:
A total of 41 patients were included in this study. The rate of agreement between radiologists regarding the tear location based on preoperative MRI scans was 61.0% (25/41), while the rate of agreement between surgeons based on diagnostic arthroscopic video recordings was 87.8% (36/41). The interrater agreement between radiologists was moderate (κ = 0.460), whereas the interrater agreement between surgeons was excellent (κ = 0.833). The rate of agreement between radiologist 1 and surgeon 1 was 70.7% (29/41), and that between radiologist 1 and surgeon 2 was 75.6% (31/41). For radiologist 2, the rate of agreement was 75.6% (31/41) with both surgeon 1 and surgeon 2. The overall reliability analysis indicated good agreement (κ = 0.648) between the MRI and arthroscopic findings.
Conclusion:
Preoperative MRI reliably identified the tear location, with a good strength of agreement between preoperative MRI and diagnostic arthroscopy. Nevertheless, despite its reliability, the interrater agreement between radiologists in interpreting preoperative MRI scans was only moderate, whereas surgeons achieved excellent agreement based on diagnostic arthroscopic video recordings.
Keywords
Primary arthroscopic anterior cruciate ligament (ACL) repair has regained attention in recent years largely because of the advancements in modern surgical techniques and growing knowledge in regenerative medicine.13,16,28 Evidence has suggested that when performed on patients with proximal tears, this procedure resulted in superior outcomes compared with ACL reconstruction.5,27 Hence, it is crucial to reliably distinguish proximal tears. Precise identification would assist the surgeon in determining the potential reparability of the ACL and thus facilitate surgical planning.8,29
Magnetic resonance imaging (MRI) has been demonstrated to be reliable in distinguishing between partial-thickness tears and full-thickness tears.15,32 However, the reliability of MRI in identifying the exact tear location compared with diagnostic arthroscopy has not yet been established. To date, only 2 studies have evaluated the concordance between preoperative MRI and diagnostic arthroscopy, with both yielding conflicting results.17,22 The limited number of studies on this issue is primarily caused by the relatively recent emergence of evidence supporting arthroscopic ACL repair as a viable option for select proximal tears.
Given that only proximal tears are amenable to ACL repair, accurate MRI that reflects findings observed through diagnostic arthroscopy is essential. Therefore, this study aimed to investigate the reliability of preoperative MRI in determining the ACL tear location. Additionally, we aimed to evaluate the strength of agreement between radiologists and surgeons. We hypothesized that (1) MRI findings would be comparable with arthroscopic findings and (2) radiologists would demonstrate good interobserver agreement on tear location as assessed by preoperative MRI, whereas surgeons would demonstrate good interobserver agreement on tear location as assessed by diagnostic arthroscopy.
Methods
Study Design and Patient Selection
Study approval was obtained from the research ethics committee of our local hospital (No. 027/KEPK/IX/2024). This is a retrospective cohort study that included all patients diagnosed with a full-thickness ACL tear who underwent ACL reconstruction between January 2022 and January 2024. Patients aged <18 years, those with involvement of the posterior cruciate ligament, those with a duration from MRI to arthroscopy >3 months, and those with unavailable MRI scans were excluded from the study.
MRI Evaluation
All MRI scans were obtained with a 3.0-T scanner according to our hospital's standardized protocol. The sequences obtained consisted of T1-weighted, T2-weighted, and proton density–weighted images, with a slice thickness of 3, 3, and 1 mm, respectively. The MRI scans for each patient were reviewed by 2 musculoskeletal radiologists, with each possessing over 5 years of experience in musculoskeletal imaging. Both radiologists determined the tear location from sagittal proton density–weighted images and categorized the tear location according to the modified Sherman classification 4 (Figure 1). The classification system consists of 5 types of tears: type I, proximal avulsion tear (>90% remaining distal remnant length); type II, proximal tear (75%-90% remaining distal remnant length); type III, midsubstance tear (25%-75% remaining distal remnant length); type IV, distal tear (10%-25% remaining distal remnant length); and type V, distal avulsion tear (<10% remaining distal remnant length).
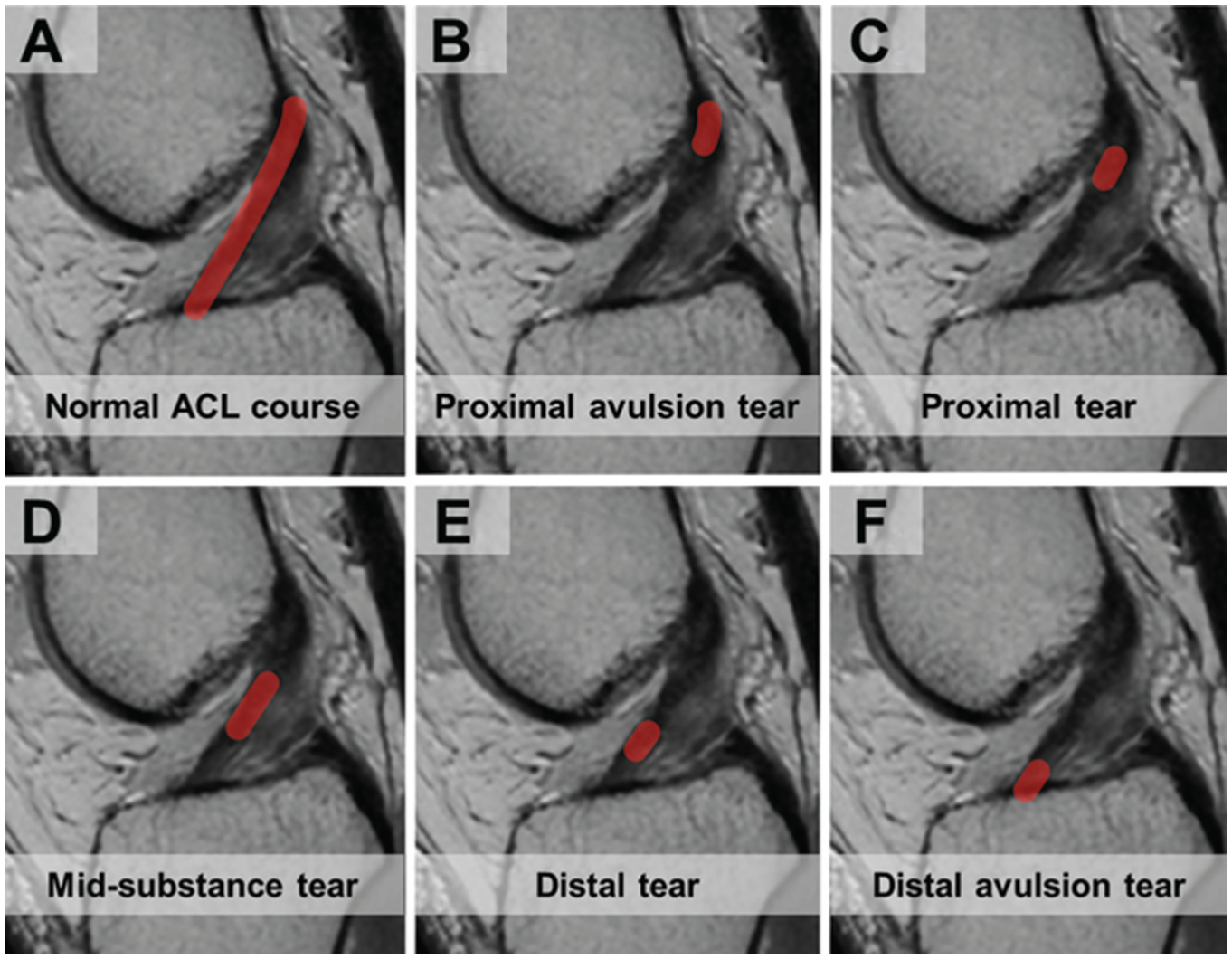
Anterior cruciate ligament (ACL) tear location according to the modified Sherman classification system. (A) Healthy ACL seen on a sagittal proton density–weighted image. (B) Type I: proximal avulsion tear. (C) Type II: proximal tear. (D) Type III: midsubstance tear. (E) Type IV: distal tear. (F) Type V: distal avulsion tear.
Arthroscopic Assessment
Diagnostic arthroscopy was used as the reference standard for identifying the exact tear location. There were 2 orthopaedic surgeons who retrospectively reviewed the intraoperative arthroscopic videos in a blinded manner. Tear location was determined based on the amount of remaining femoral and tibial remnants, with tears subsequently categorized according to the modified Sherman classification. The surgeons’ assessments of the tear location were then compared with the radiologists’ interpretation of the preoperative MRI scans.
Statistical Analysis
Data were analyzed using SPSS Statistics for Windows (Version 26.0; IBM). Numerical data were presented as mean ± standard deviation. Categorical data were presented as number and percentage. Interrater agreement between radiologists, between surgeons, and between radiologists and surgeons was assessed using the Fleiss kappa (κ). The strength of agreement was interpreted according to the guidelines of Landis and Koch 14 : poor (κ < 0.00), slight (κ = 0.00-0.20), fair (κ = 0.21-0.40), moderate (κ = 0.41-0.60), good (κ = 0.61-0.80), and excellent (κ = 0.81-1.00).
Results
Patient Characteristics
Between January 2022 and January 2024, a total of 56 patients diagnosed with full-thickness ACL tears underwent ACL reconstruction at our institution. However, 2 patients were excluded because of posterior cruciate ligament involvement, 3 were aged <18 years, 6 had an interval from MRI to arthroscopy >3 months, and 4 had an unavailability of MRI scans. Overall, 41 patients were included in the final analysis (Figure 2). The mean age of the patients was 30.2 ± 9.9 years, with 33 being male (80.5%). Regarding the cause of the injuries, 28 were sports-related injuries (68.3%), 12 were recreational injuries (29.3%), and 1 was a motor vehicle accident–related injury (2.4%). The mean interval from injury to MRI was 36.0 ± 53.3 days, while the mean interval from MRI to reconstruction was 15.7 ± 15.5 days.

Characteristics of patients included in this study.
Distribution of Tear Location
Details regarding the distribution of ACL tear locations based on preoperative MRI and diagnostic arthroscopy can be seen in Table 1. The rate of agreement between the radiologists was 61.0% (25/41), while the rate of agreement between the surgeons was 87.8% (36/41).
Distribution of Tear Location a
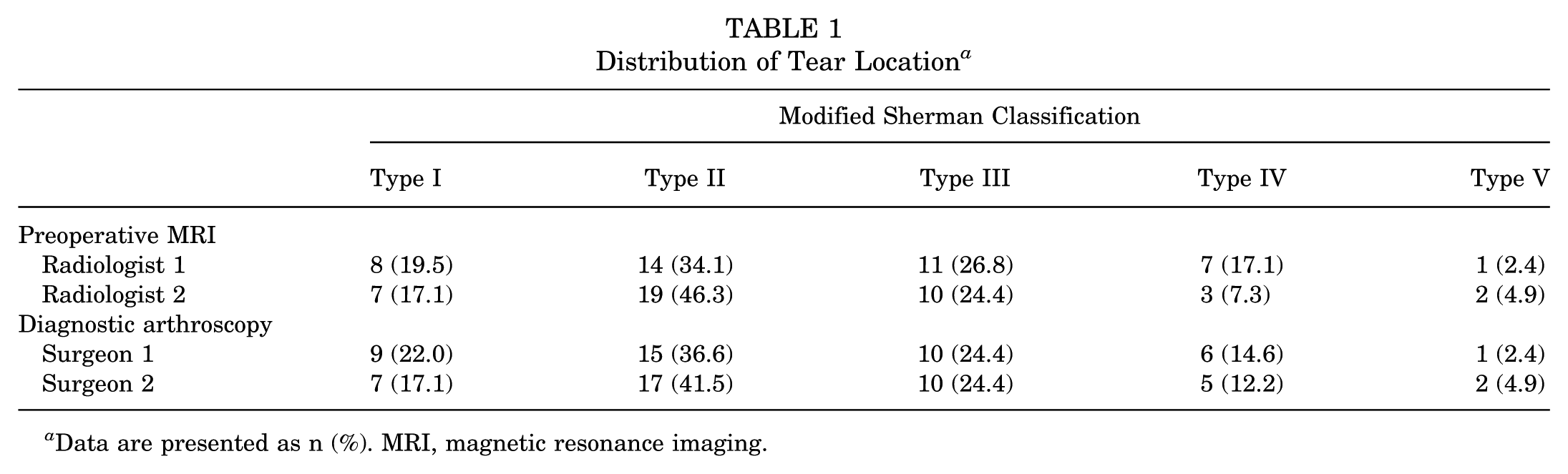
Data are presented as n (%). MRI, magnetic resonance imaging.
Agreement on Tear Location Between Raters
Details regarding agreement on the tear location between radiologists, between surgeons, and between radiologists and surgeons can be seen in Table 2. Based on preoperative MRI scans, radiologists exhibited moderate agreement (κ = 0.460) in the tear location. Meanwhile, based on diagnostic arthroscopic video recordings, surgeons exhibited excellent agreement (κ = 0.833). The rate of agreement between radiologist 1 and surgeon 1 was 70.7% (29/41), while that between radiologist 1 and surgeon 2 was 75.6% (31/41). In comparison, the rate of agreement between radiologist 2 and surgeon 1 was 75.6% (31/41), while that between radiologist 2 and surgeon 2 was 75.6% (31/41). The overall reliability analysis demonstrated good agreement (κ = 0.648) in the tear location between the preoperative MRI scans assessed by radiologists and the diagnostic arthroscopic video recordings assessed by surgeons.
Agreement on Tear Location Between Raters a

MRI, magnetic resonance imaging.
Agreement on Tear Location According to Modified Sherman Classification
The reliability analysis of preoperative MRI in identifying the tear location based on the modified Sherman classification is detailed in Table 3. The strength of agreement was found to be good for type I through type V tears.
Agreement on Tear Location According to Modified Sherman Classification (Preoperative MRI) a

MRI, magnetic resonance imaging.
Discussion
The main finding of this study was that there was good agreement between preoperative MRI and diagnostic arthroscopy. For interrater agreement, the radiologists shared moderate agreement on the tear location as assessed from preoperative MRI scans, whereas the surgeons shared excellent agreement on the tear location as assessed from diagnostic arthroscopic video recordings.
Sherman et al 21 were the first to introduce a classification system for ACL tear location, which was originally developed to categorize intraoperative findings on tear location during open ACL repair. However, midterm follow-up studies have revealed a high rate of reruptures associated with the open repair procedure.7,9 Consequently, open ACL repair and the original classification system have since been abandoned. In recent years, advances in surgical techniques, along with several reports of successful proximal repair6,8,31 and the healing augmentation potential offered by biological agents,11,23,30 have renewed interest in arthroscopic repair for proximal tears. The proximal region's abundant vascular supply has been described as a key factor in facilitating the intrinsic healing process after ACL repair.2,28 This has been demonstrated in a histological study by Nguyen et al, 19 which revealed that repaired proximal remnants exhibited signs of healing, including increased collagen fiber density, neovascularization, myofibroblast activity, type III collagen deposition, and metabolic activity.
To improve the previous intraoperative classification system consisting of 4 tear types, van der List et al 26 introduced the modified Sherman classification, which consists of 5 tear types and was designed to facilitate the preoperative identification of the tear location. This 5-type classification has been shown to produce good intraobserver (κ = 0.781) and interobserver (κ = 0.671) agreement among radiologists. Using this modified system, Mehier et al 17 evaluated the agreement between preoperative MRI and diagnostic arthroscopy. Their study demonstrated that MRI reliably determines the tear location, with an accuracy of 70%. The strength of agreement between preoperative MRI and diagnostic arthroscopy was revealed to be good. Additionally, the interrater reliability of MRI findings by radiologists was also found to be good. The results in the present study are mostly consistent with their reported results, except that we observed only moderate interrater agreement (κ = 0.460) between the radiologists based on preoperative MRI. We documented that the radiologists exhibited a lower agreement rate (61.0%) from preoperative MRI while surgeons demonstrated a higher agreement rate (87.8%) from diagnostic arthroscopy. The inconsistency observed in the present study highlights the observer-dependent nature of MRI interpretation, which could be influenced by individual experience or judgment. In addition, the presence of sagging remnants or spiral tear patterns could hinder the tear location assessment. 26 Therefore, because of the subjective variability in MRI interpretation, the final confirmation of the tear location should ultimately be established through diagnostic arthroscopy.
Interestingly, although our findings and those of Mehier et al 17 revealed good agreement between preoperative MRI and diagnostic arthroscopy, Shu et al 22 reported contradictory results. Their study demonstrated poor agreement between MRI and intraoperative arthroscopic findings, with the rate of agreement on the tear location as low as 2.9%. However, upon observation of their study methodology, we hypothesize that this low agreement is likely attributable to the study's inclusion criteria in which partial rupture cases were included, as 20 of 34 patients had a partial-thickness tear. Generally, the modified Sherman classification is supposed to be strictly used to categorize full-thickness tears.4,26 Hence, an attempt to determine the tear location in partial-thickness tear cases may lead to inaccurate findings. This reasoning also applies to ACL repair, as this procedure is only performed among patients with a full-thickness tear.12,18
In addition to tear location, the quality of the remnant has also emerged as a crucial factor in determining the reparability of the ACL. 1 A poor-quality remnant that has undergone hypoplastic changes and has an insufficient length is often difficult to reattach to its original footprint, making it unsuitable for repair. Therefore, repair procedures should only be considered in cases of proximal tears with a sufficient distal remnant length and adequate remnant quality. 24 Remnant quality may be affected by several factors, including age, sex, tear chronicity, and associated intra-articular abnormalities such as meniscal or chondral lesions.3,20 Among these, the chronicity of the tear is the most critical one. The longer the interval between the initial injury and surgical repair, the greater the likelihood that retraction and shortening of the remnant will occur. Therefore, repair is generally advocated only during the acute and subacute phases (within 1 week to 3 months after the initial injury).5,10,25
Several limitations of the current study need to be noted. First, the retrospective design of this study could introduce selection bias. Second, as it is a single-center study, the sample size was relatively small. Third, there may have been bias in MRI interpretation by the observers, as the findings strongly depended on their level of experience. Fourth, the determination of the tear location by the surgeons was conducted retrospectively from patients’ arthroscopic video recordings, which may have resulted in less accurate findings compared with direct intraoperative evaluations. Lastly, reliability tests for ACL tissue quality were not performed. The reliability of MRI in assessing tissue quality should ideally be validated against cases that undergo actual repair. However, because of the limited number of repair procedures performed at our institution, this analysis could not be carried out. Therefore, further prospective studies are needed to evaluate the accuracy of MRI in identifying both tear location and remnant tissue quality.
Conclusion
The present study demonstrated that preoperative MRI was reliable in determining the tear location, showing good agreement with findings from diagnostic arthroscopy. However, although appearing to be reliable, the interrater agreement between radiologists in interpreting preoperative MRI scans was only moderate, while surgeons demonstrated excellent agreement in evaluating diagnostic arthroscopic video recordings. For this reason, the final determination of the tear location should be confirmed directly during diagnostic arthroscopy.
Footnotes
Final revision submitted June 29, 2025; accepted July 16, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from St Borromeus Hospital (No. 027/KEPK/IX/2024).