
Abstract
Background:
Information derived from functional return-to-sport (RTS) tests after primary anterior cruciate ligament (ACL) reconstruction (ACLR) can have a significant impact on the risk reduction of ACL reruptures. However, due to space, time, and financial limitations, few clinicians utilize objective data to assess their patients’ functional abilities after ACLR.
Purpose:
To identify validated and feasible RTS tests that could reliably estimate the risk of reinjury after ACLR in everyday clinical practice beyond the highly sophisticated laboratory setting.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A focused review was performed by experts of the committees for Ligament Injuries and Prevention/Rehabilitation of the German Knee Society. RTS functional tests, their reinjury prognostic values (if known), their reliabilities, and their implementation capacities were extracted from the original studies on the described RTS test setup, as well as from studies on potential test alternatives. These alternatives were required to be less resource-consuming yet still validated and thus able to be implemented into everyday practice. All tests were categorized according to their relevant target objective: isokinetic or isometric strength, functional (hopping and jumping) ability, or self-reported readiness.
Results:
In the final analysis, 19 studies involving 7513 patients were included. From these, a total of 21 RTS tests were retrieved, and 13 tests were included. For strength testing, 2 dynamic tests and 1 static test were found to be eligible. Functional ability was represented by 8 different jump, hop, and agility tests. Tests for self-reported readiness included the ACL–Return to Sport after Injury scale and the Knee injury and Osteoarthritis Outcome Score Sport and Recreation subscore. Alternative tests included the 8–repetition maximum test, handheld/portable dynamometer, single-leg vertical (countermovement) hop with inertial sensor or smartphone app, and the drop jump with knee displacement or normalized knee distance measurement.
Conclusion:
For most of the strength and functional abilities assessed by RTS tests, validated and less resource-consuming alternatives do exist. Therapists and clinicians working in nonlaboratory settings may find it helpful to select from a menu of established RTS tests and test alternatives for each relevant target objective, depending on their individual requirements.
With an annual incidence of 0.9% to 1.7%62,72 within an athletic population, an anterior cruciate ligament (ACL) rupture is one of the most common ligament injuries of the knee. The incidence is particularly high among athletes involved in pivoting and cutting sports. 8 In order to restore knee joint function and stability, 6 including return to pivoting and cutting sports, most athletes are advised to undergo ACL reconstruction (ACLR) followed by functional rehabilitation. 54 However, the risk of reinjury is high even for athletes who successfully complete rehabilitation and are able to return to sport (RTS)9,85; the overall risk of subsequent ACL rerupture after ACLR is reported to be 6% to 15%.72,92 Therefore, an important goal before RTS must be to assess the individual's risk of reinjury.
Comprehensive rehabilitation with test criteria–based progression during RTS, combined with key discharge criteria for RTS release, may reduce the likelihood of subsequent ACL failure or reinjury after ACLR.9,34,48 RTS testing is an important tool to estimate this risk and thus determine the readiness for RTS on an individual level,9,83,93 but only if the tests are validated for assessing the risk of rerupture and/or reinjury. 48 Although controversy exists in the current literature,11,21,53,89,92 meeting corresponding test criteria appears to reduce the risk of a rerupture and/or reinjury.22,23,34,48,82
However, there is great variability in the definition, assessment, and reporting of RTS after ACLR, and several studies have been conducted on RTS test batteries, their variability, and their validity.53,87,88 Multiple measurements should be performed to achieve the desired goal of monitoring the continuum of RTS,17,22 which can be a significant resource burden in everyday clinical practice. Given these facts, it would be useful for clinicians to know if there are simpler alternative but still valid tests that assess the same variables. Importantly, a greater number of therapists, clinicians, and physicians should be able to validly use objective RTS tests and data to assess the functional capacity of their patients recovering from ACLR in real-time clinical settings.
With this in mind, the purpose of the current review was to analyze the literature to objectify the RTS tests that have been validated to estimate the risk of recurrent ACL rupture, with the aim of assessing their applicability in daily clinical practice beyond the sophisticated laboratory setting.
Methods
Study Design
The study was designed as an umbrella review, concentrating on the current literature (up to July 2023) on RTS testing and the associated risk of ACL rerupture. The umbrella review used is a relatively new concept. 13 It refers specifically to a review that synthesizes evidence from multiple reviews into a single accessible and usable document. It focuses on broad conditions or problems for which there are competing interventions and highlights reviews that address these interventions and their outcomes. Umbrella reviews are not required to follow PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, although we tried to follow them as closely as possible.
A review of the literature and best-practice guidelines was performed by an expert multidisciplinary working group mostly consisting of members of the committees for Ligament-Injury and Prevention/Rehabilitation of the German Knee Society (DKG), each having 10 to almost 30 years of experience in the treatment of ACL injuries.
Overview of the Review Process
Considering Past Review Studies for Inclusion
To gain an initial overview of the current literature, we first sought previously published reviews that explicitly evaluated tests or test batteries for the ACL rerupture risk or reinjury risk. For that purpose, PubMed, Web of Knowledge, the Cochrane Library, and Google Scholar databases were screened for original articles regarding “ACL” AND (“re-injury” OR “re-rupture” OR “second”) AND (“RTS” OR “return to sport” OR “return-to-sport” OR “test” OR “test batterie” OR “testing” OR “criteria”). Subsequently, 4 reviews framing the current knowledge on the topic were identified.4,11,52,88 These studies were considered the latest systematic review–based scientific perspectives; 2 studies were systematic reviews with meta-analyses on the validity of RTS testing after ACLR 88 and on the association between passing RTS criteria and second ACL injury risk 52 ; 1 study was a systematic review on evidence level 2 studies regarding the reinjury risk and prognostic value of RTS testing 4 ; and 1 study was a critical reanalysis 11 of the first review on the validity of RTS testing after ACLR. 88
To determine the test pool, we reviewed all original studies included in the four selected reviews.4,11,52,88 We extracted the RTS tests used in these studies and evaluated their ability to predict reinjury risk after ACLR, their reliability, and how easily they could be implemented. Additionally, we manually searched the reference lists of these articles to find further relevant studies and tests. Each study was then reviewed in full text to ensure it was relevant to our research purpose.
Exclusion Criteria
Case reports, letters to the editor, expert opinions, editorials, abstracts, technical reports, and protocols, as well as studies not reporting tangible pass/cutoff criteria, studies with a cohort of minors (patients <18 years) as the study population, and duplicate studies were excluded.
Data Extraction: Valid Reinjury-Predictive RTS Testing
It is possible that some tests that are easier to perform in a clinical setting were not included in the test batteries of the original studies, as the focus of the included studies was mainly on the aspect of passing the RTS test and returning to the sport, as well as the risk of reinjury. Therefore, the literature was reviewed again specifically with this question in mind. The aim was to identify those RTS tests that would be easier to perform in everyday clinical practice, while still maintaining good validity and reliability. For this purpose, PubMed, Web of Knowledge, the Cochrane Library, and Google Scholar databases were screened for original articles regarding the specific RTS test (eg, isokinetic testing = XX) “XX” AND (“anterior cruciate ligament”) AND (test OR testing) AND (“alternative” OR “test criteria” OR “valid” OR “quality criteria”). The inclusion criteria for these alternative tests were those that (1) had been validated against a previously identified, standardized, and established test procedure and (2) were reliable for their predictive values regarding the risk of ACL rerupture, reporting intraclass correlation coefficients (ICCs) or correlation coefficients (r values) of ≥0.9 to be rated “approved” and recommended.
Results
Study Selection and Characteristics
A total of 27 studies, including 8689 patients, were extracted. After the application of the exclusion criteria, 19 studies ‖ ‖ (N = 7513 patients) using 21 reinjury-predictive functional and self-reported RTS tests were included in this review.
Within the framework of this umbrella review, the different studies and the respective RTS tests are summarized in Table 1. The studies varied in terms of the activity level of the participants (from amateur to professional athletes) and also in terms of the types of sport investigated. This was an advantage for our research question, as a wide range of sports and patient groups could then be covered. A detailed discussion of the strengths and weaknesses of the included studies is available in the Appendix, and a table summarizing the characteristics of the population within each included study is shown in Appendix Table A1.
Studies Included in the Final Review and Their Respective RTS Tests a


ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; Ext, extension; Flex, flexion; GRS-PF, global rating scale for perceived function; HT, hamstrings; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LESS, Landing Error Scoring System; Quad, quadriceps; SEBT, Star Excursion Balance Test; Sport/Rec, Sport and Recreation; TSK, Tampa scale of kinesiophobia.
Test validated (either isolated or as part of a test battery) regarding its prognostic value for the risk of anterior cruciate ligament rerupture.
Characteristics of the Included RTS Tests
Of the 21 RTS tests, 13 tests were considered in the final analysis. Further information on 7 alternative tests with more practical but still valid and reliable test quality for estimating the risk of ACL reinjury were retrieved from 11 additional studies ¶¶ with 292 patients. All tests were categorized according to their respective target objective: isokinetic or isometric strength, functional ability (hopping and jumping), or self-reported readiness. For each test, reinjury prognostic values, reliabilities, and performance capacities were assessed, and where available, cutoff values and reference values from healthy individuals were obtained for each target objective. This information is summarized in Tables 2 (strength testing), 3 (functional ability), and 4 (self-reported readiness). Each of these tables is divided into 3 different sections, highlighted with a gold, silver, and bronze frame. The gold-framed tests are mostly complex and labor-intensive to perform. They are costly, space- and time-consuming, and therefore not feasible in most clinical settings. To address this issue, validated test alternatives have been compiled in the silver and bronze frameworks. These alternatives allow RTS testing with significantly less financial, time, and space expenditure. Nonetheless, it should be noted that the amount of information (ie, validity, reliability, or objectivity) usually decreases, and the uncertainty increases when descending from the established extensive test batteries to the test alternatives. In addition, each test characteristic was graded according to quality, indicated by different-colored shadings (green, yellow, or red)
RTS Tests Recommended After Final Analysis: Strength Testing a

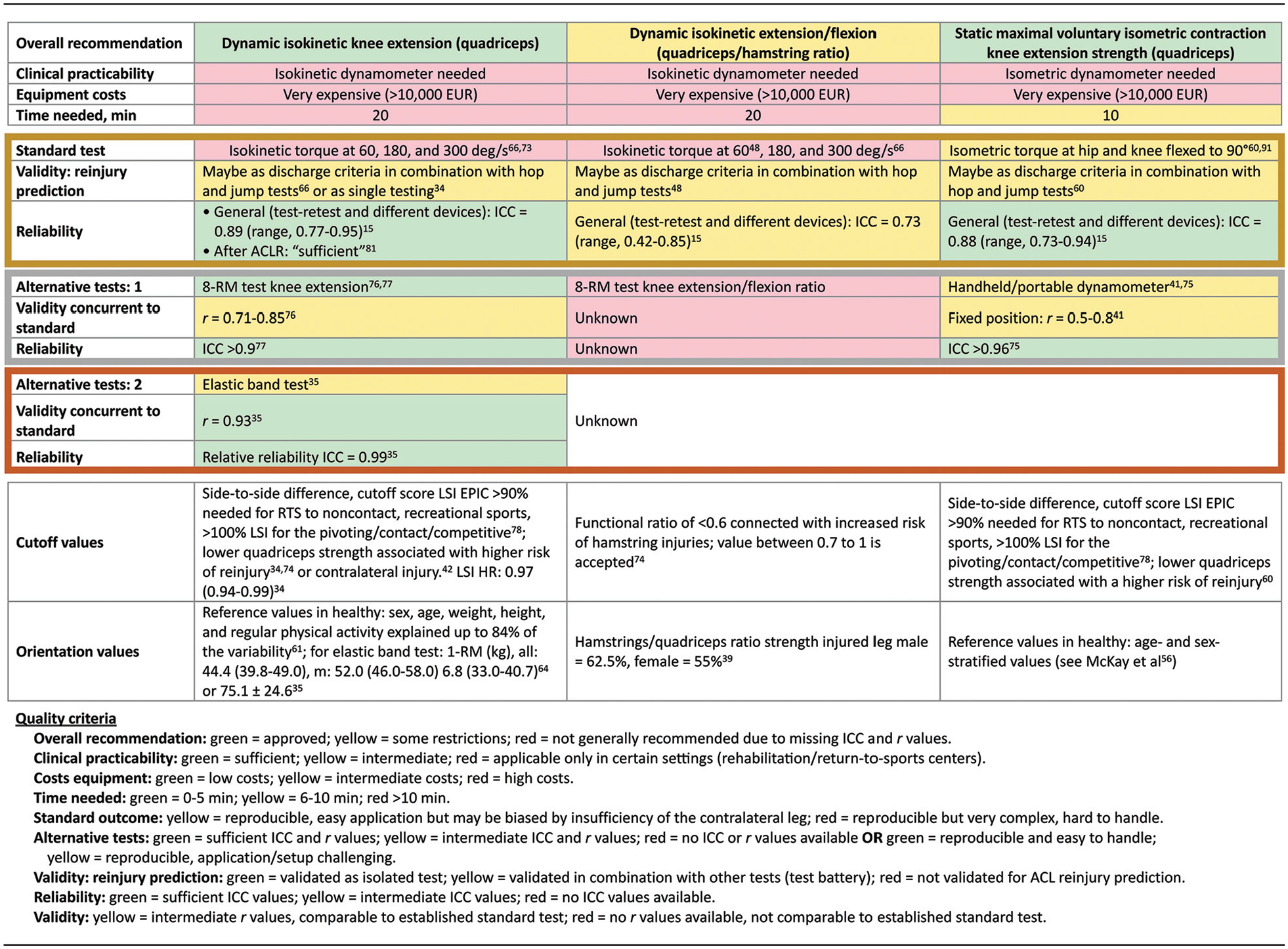
ACLR, anterior cruciate ligament reconstruction; EPIC, estimated preinjury capacity; HR, hazard ratio; ICC, intraclass correlation coefficient; LSI, limb symmetry index; RM, repetition maximum; RTS, return to sport.
RTS Tests Recommended After Final Analysis: Functional Ability Testing a


ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; EPIC, estimated preinjury capacity; F, female; ICC, intraclass correlation coefficient; LSI, limb symmetry index; M, male; OR, odds ratio; sec, second.
RTS Tests Recommended After Final Analysis: Self-Reported Readiness a


ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; ACLR, anterior cruciate ligament reconstruction; ICC, intraclass correlation coefficient; KOOS, Knee injury and Osteoarthritis Outcome Score; Sport/Rec, Sport and Recreation.
Values shown are mean scores for patients with rehabilitation and early ACL reconstruction. The “Return to same activity” are the ACL-RSI scores in patients who returned to same activity or activity level.
Strength Testing
Three established strength tests were found to be eligible: the dynamic test for isokinetic knee extension torque, the dynamic test for isokinetic extension/flexion or quadriceps/hamstring torque ratio, and the static test for maximal voluntary isometric contraction knee extension strength. To carry out these tests according to their standard requirements, an isokinetic dynamometer was mandatory. The supplied software simultaneously provided the age- and sex-specific standard strength values to be aimed for, which was a great advantage. However, a disadvantage of this approach was the high cost related to the purchase of an isokinetic dynamometer, which led us to search for more applicable and cost-saving alternatives. The 8–repetition maximum (RM) knee extension test, 82 a handheld/portable dynamometer, 45 or the elastic band test, 39 being a 1-RM test for dynamic knee extension, were alternatives for strength testing that were found within the studies included in this review. Several studies have shown that lower quadriceps strength is associated with a higher risk of reinjury34,60,74 or contralateral injury. 42 A functional hamstrings/quadriceps ratio of <0.6 has been connected with increased risk of hamstring injuries; values between 0.7 to 1 are to be accepted. 74
Functional Ability Testing
In terms of the hop and jump tests, 8 tests were found to be eligible. The drop jump has shown excellent reliability in measuring the knee valgus moment using 2 cameras26,67 and is a time- and space-saving established standard test, whereas purchasing 2 camera systems cannot be considered a cost saving. As an alternative to measuring the valgus moment using cameras, medial knee displacement or normalized knee distance could be assessed, which may be easier to measure using either an inertial sensor24,69 or a smartphone app. 29 Side-to-side differences (asymmetry) in the sagittal plane of the knee valgus moment at the point of initial contact of >2.81 × 10−2 N·m/kg (odds ratio = 3.3 [95% CI, 1.2-8.8]) 67 do have a positive predictive validity in predicting reinjury. The cutoff values given in current literature lie within a side-to-side difference <2.8 × 10−2 N·m/kg; a knee separation distance of >60% at initial contact and >40% at lowest point. 6 Due to the well-researched results of this test in the current literature and with valuable test alternatives in terms of cost, the drop jump should be considered for each individualized test battery in combination with a test involving horizontal movement patterns.
Horizontal movement tests such as the single-leg distance-, triple-, triple crossover-, and 6-m timed hop have been validated in combination in terms of their predictive values for the risk of ACL rerupture.16,19,34,50,60,66,80 These tests are time- and cost-effective but require a large open area (≥8 × 2 m) to perform.Due to the low resource requirements of the test methods, there was no need for test alternatives if the appropriate space capacity was available. The same applied to the running t test, although in this case, the space requirement was even greater, with a minimum test area of 6 × 6 m.
The single-leg vertical countermovement hop test may provide an RTS discharge criterion in combination with the isokinetic strength testing of knee extension, triple hop, and triple crossover hop tests. 73 For the established standard test, a contact time mat is required, which could easily estimate the jumping height. Since contact time mats can be costly, a more economical alternative could be an indirectly calculated jumping height with inertial sensor or insoles. 84 Sufficient ICC and r values have also been demonstrated by the smartphone app, 29 which can, therefore, be a good financial alternative.
Hop testing appears to possess fair association to subjective tests of knee function, as measured by the Knee injury and Osteoarthritis Outcome Score (KOOS) and a patient's ability to RTS after ACLR. 51 However, as mentioned above, an isolated assessment using a horizontal hop should be avoided.43,44
Self-Reported Readiness
Two self-reported tests were recommended. The ACL–Return to Sport after Injury (ACL-RSI) is a scale that was developed by Webster et al 86 in 2008 to measure the psychological impact of RTS after ACLR.2,3 It has since been used to assess the reinjury risk in various studies and RTS testing1,31,90 and is an established evaluation criterion. According to Sadeqi et al, 71 the optimal ACL-RSI score threshold to return to the same sport at 2-year follow-up is >65. To return to a professional or competitive level of play, an ACL-RSI score >60 at 6-month follow-up should be reached.
In this context, the KOOS is also an established and validated scale to measure self-reported knee function. It can be divided and evaluated in subscales and has been validated for its predictive value regarding the risk of ACL reinjury on its own 28 or in combination with other tests. ## The Sport and Recreation subscale of the KOOS (KOOS Sport/Rec) is a quick and easily assessed outcome measure that shows significant differences between patients with and without a later revision surgery 33 and was therefore relevant for this study. Both the ACL-RSI and the KOOS Sport/Rec are easy to assess and take little time to complete. Therefore, they are eligible to be used in all setups and should be implemented in every RTS test compilation.
The Tampa scale of kinesiophobia may be a bit more elaborate and time-consuming, but it has been evaluated for the risk of second ACL injuries, and although it was not included as a recommended test, it is also valuable in assessing psychological readiness with regard to RTS after ACLR.46,65
Applications
Depending on the resources available (money, time, personnel, and equipment) and the accuracy required (validity and reliability), tests that reflect the target objective can be administered using either the established test version (marked with a gold outline in Tables 2 and 3) or alternative test versions (marked with a silver or bronze outline in Tables 2 and 3). This may be applied as follows:
For strength testing:
● Dynamic isokinetic knee extension torque
● Dynamic isokinetic extension/flexion
● Static maximal voluntary isometric contraction knee extension strength
Alternatives:
● 8-RM knee extension test
● elastic band test
For functional ability testing:
● Distance hop
● Triple hop
● Triple crossover hop
● 6-m timed hop
● Speedy hop
Alternative 1:
● Single-leg vertical (countermovement) hop with inertial sensor
● Drop jump: medial knee displacement in degrees
Alternative 2:
● Single-leg vertical (countermovement) hop with smartphone app
● Drop jump: normalized knee distance in centimeters or as a limb symmetry index (%)
Starting from the established strength and functional ability tests at the top of Tables 2 and 3 going downward to their test alternatives, the time, money, and space resources required usually decrease as the uncertainty increases.
Tailoring the Individual Tests According to Resources
In the flowchart in Figure 1, different test selections depending on quality criteria (approved, some restrictions, or not generally recommended) and resources (time, money, and space) are depicted. Starting with only 1 resource (time or money or space) in the upper horizontal row, the respective tests reflecting the 3 relevant test abilities (strength, functional ability, and self-reported readiness) are listed underneath. In the second row, the resources (money and space, money and time, space and time) are combined, and the respective tests regarding the target objective are listed underneath once more. If the established most standardized test setup is applicable, the arrows point directly to the standardized tests.

Flowchart for test selection regarding the different resources of time, money, and space
and space  The development from the most time-, money- and space-efficient test alternatives to the most standardized tests is indicated with the arrows. The different colors of the text boxes correspond to the quality criteria outlined in Tables 2–4. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; KOOS, Knee injury and Osteoarthritis Outcome Score; RM, repetition maximum; Sport/Rec, Sport and Recreation.
The development from the most time-, money- and space-efficient test alternatives to the most standardized tests is indicated with the arrows. The different colors of the text boxes correspond to the quality criteria outlined in Tables 2–4. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; KOOS, Knee injury and Osteoarthritis Outcome Score; RM, repetition maximum; Sport/Rec, Sport and Recreation.
For strength testing, if time is critical but space and cost are not an issue, then the static maximal voluntary isometric contraction knee extension strength may be used from the test compilation (Table 2). As a more time- and space-efficient test alternative, the 8-RM knee extension test may be applied, while if costs need to be saved, the elastic band test or the handheld/portable dynamometer tests can be effective alternatives (Figure 1).
A selection of appropriate functional tests ideally combines measures for speed, agility and dynamic knee valgus moments to monitor the improvement of neuromuscular control in athletes. 10 However, an isolated assessment using a horizontal hop should be avoided, since the knee contributes about one-third to vertical hop height but only about one-eighth to horizontal hop distance.43,44 Distance hop, triple hop, triple crossover hop, and 6-m timed hop are time-saving tests, each taking <5 minutes for their execution. A combination of single-leg vertical/countermovement hop and the drop jump, which are able to assess explosive strength with a contact time mat (vertical/countermovement hop) or knee valgus moments via cameras (drop jump), could be adopted. However, both assessments are costly. A more economical and faster test alternative would be to assess both tests and test qualities (jumping height, medial knee displacement) with an inertial sensor (Figure 1).
To create an RTS test battery tailored to the individual needs of clinicians and patients, established tests for the 3 main categories can be combined with test alternatives and vice versa (Figure 2).
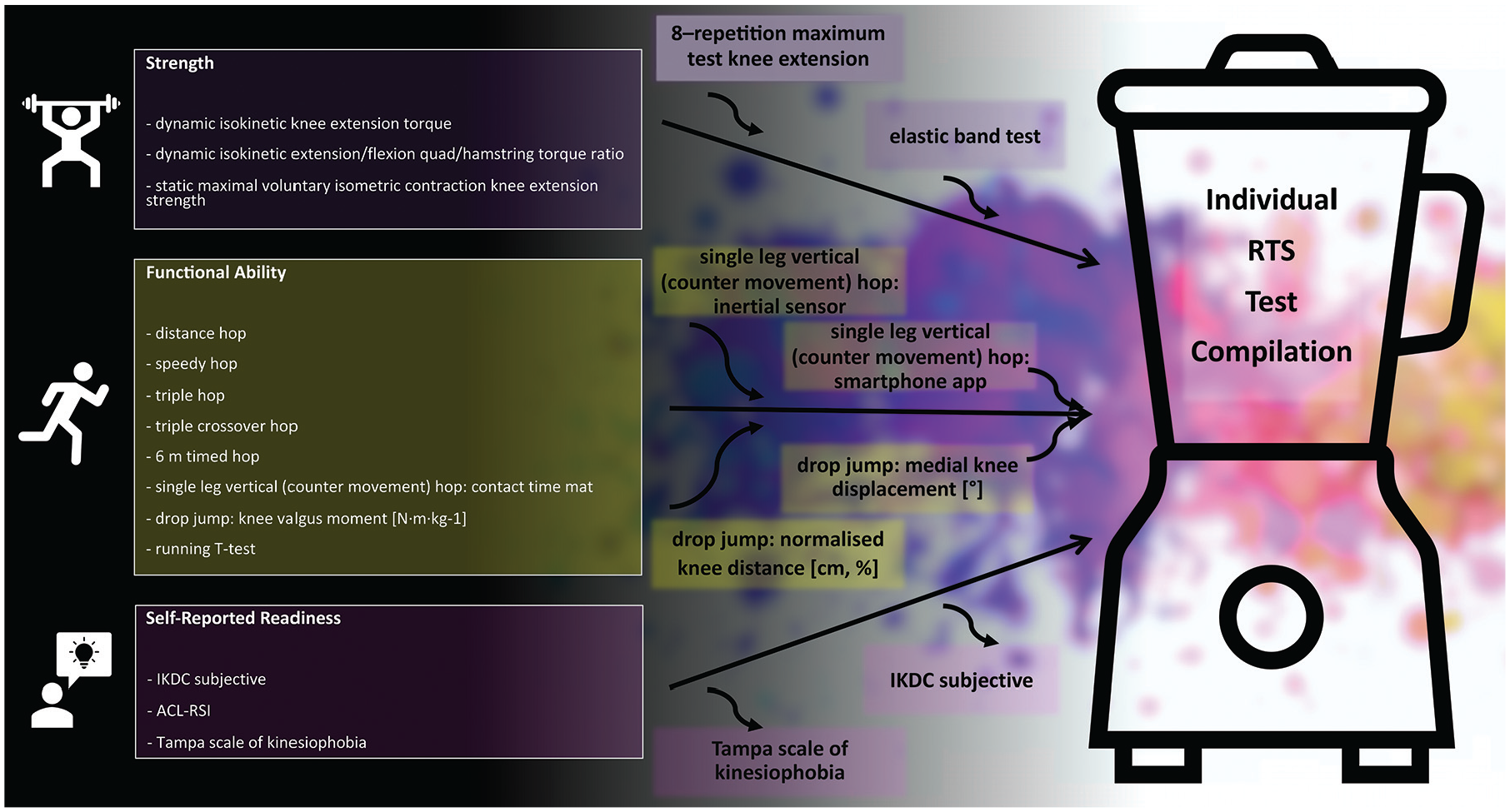
Flowchart to create a return-to-sport test battery tailored to the individual needs of clinicians and patients. ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; IKDC, International Knee Documentation Committee; RTS, return to sport.
Discussion
Many systematic reviews evaluating measurements of functional performance after ACLR have come to the same conclusion: studies lack the objective physiological criteria concerning at what time RTS after ACLR should be allowed.5,6,14,20,37,59,83 There are only a few objective measurement criteria, such as the isokinetic strength measurement, that are adapted to standardized age, sex, height, and weight values when estimating normal knee function; these are very helpful but are also very expensive and time-consuming. This review was intended to assist clinicians in selecting validated RTS tests for each relevant target objective (strength, functional ability, self-reported readiness) and offer guidance on how to conduct RTS assessments within the time, space, and budget available in their clinical setting (see Tables 2–4).
A difficulty in our daily practice has been the interpretation of the test results. Without cutoff and/or reference values, it is not possible to provide sustained support to athletes during RTS testing. For this reason, cutoff and reference values are described in the included studies in Tables 2 through 4, to give a rough orientation regarding the athletes’ performance.
Each individual test compilation should include the primary selection of the relevant abilities to be tested 27 in view of estimating a “safe” RTS.22,34,48,65,66,91 Different movement patterns in the horizontal or vertical planes, while focusing on the medial knee displacement, should be taken into consideration for functional assessment and RTS testing after ACLR.10,12,18 We recommend starting with the self-reported questionnaires, which may be completed before the consultation in the waiting area. Contrary to the test battery described by Gokeler et al, 31 we believe it to be important and more time-efficient to perform testing as follows: (1) self-reported questionnaires, (2) strength testing, and (3) functional ability testing. We believe that if the tests are performed in this order, neuromuscular deficits, which are essential to identify in order to prevent reinjury, may be easier to detect due to the fatigued muscle strength following the RTS strength test. In addition, the strength test is intended to measure peak torque, which may be reduced by previous functional testing.
The evidence that single RTS tests are predictive for reinjuries and, therefore, can reduce the risk of ACL rerupture is sparse and generally refers to test batteries. Despite this knowledge, ongoing monitoring of the progress after ACLR using a combination of strength tests, hop tests, and self-reported outcome scores can support the athlete to a safe RTS. It is important that the athlete's and clinician's expectations are in line with the capabilities and predictive power of an RTS test battery, as it is not a green card for a lifelong injury-free sporting career but rather a guideline and helpful tool in the RTS process.
Limitations
One limitation of the current review was that data regarding age, sex, rehabilitation protocol, follow-up time, RTS criteria, functional tests, graft type, and surgical techniques were not standardized across the selected studies. These factors are known to play a role in ACL reinjury; however, we found them beyond the scope of this review. In addition, for most of the RTS tests included, it was not possible to make an individual risk assessment for reinjury. This was due to the combination of RTS tests in many of the studies. Therefore, the validity of the reinjury prediction for a single test had to be rated as intermediate (yellow-shaded text in Tables 2–4) in many cases.
There is a lack of RTS testing concentrating on the different sporting patterns (eg, gymnastics, soccer) that have to be evolved and reestablished for each sport after ACLR. Most studies focus on professional soccer players and athletes of pivoting sports, which, on the one hand, are at the highest risk of suffering reinjury but, on the other hand, are the most popular and one of the best paid worldwide, with considerable interest in early RTS. Another problem within the current literature is that we hardly know what happens after the RTS testing. The exposure to high-risk activities is an essential point when evaluating the validity of RTS tests. Indeed, a player failing RTS tests but returning to sports with very low exposure to high-risk activities might still be at a relatively lower injury risk compared with another player passing RTS tests with very high exposure to high-risk activities. However, this exposure is not reported in current studies. 30
Irrespective of these methodological variations, we believe that the findings add valid, evidence-based information in terms of RTS testing regarding the risk of ACL reinjury and RTS advice in clinical settings due to the high level of the included studies. Nevertheless, we believe that further work to validate new, more precise outcome measures and to determine their true predictive values regarding ACL reinjury is required.
Conclusion
This study enables physicians and therapists to offer RTS testing in their practice according to their individual resources and gives them the freedom to accompany the process of RTS. With the provided outcome measures and cutoff values from multiple studies, this focused review contains an appropriate assessment basis for the overall orientation of the rehabilitation status and RTS skills of patients, bridging the gap between science and everyday practice.
A practical tip: With the findings of this article, the authors developed 3 test manuals, which are freely available for download on the homepage of the DKG (https://deutsche-kniegesellschaft.de/downloads).
Footnotes
Appendix
Final revision submitted June 17, 2024; accepted June 24, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.