
Abstract
Background:
Anterior cruciate ligament reconstruction (ACLR) continues to be associated with a variable rate of return to sports and a concerning rate of further anterior cruciate ligament injury. Persistent functional deficits may explain these results and support the need to keep exploring lower limb functional indexes, especially during vertical jumping. This would help improve rehabilitation through the return-to-sports continuum and improve postoperative outcomes.
Hypothesis:
Vertical jumping performance indexes are impaired among patients 7 months after ACLR.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 202 patients who underwent ACLR and 50 healthy participants performed single-leg vertical jump (SLVJ) and single-leg drop jump (SLDJ) testing. Jump height (H) as well as reactive strength index (RSI) were assessed and the limb symmetry index (LSI) of each parameter was compared between both groups. Vertical jumping indexes were also compared between healthy participants and the injured and contralateral legs of ACLR patients. Frequency analysis (chi-square test) of participants exhibiting an LSI >90% for each parameter was calculated in both groups. The level of association between SLVJ-H, SLDJ-H, and SLDJ-RSI was evaluated using the Pearson coefficient (r).
Results:
At 6.6 ± 0.7 months (mean ± SD) postoperatively, participants after ACLR exhibited poorer LSI than the control group for all parameters (79.1 ± 14.8 vs 93.9 ± 4.5, 77.3 ± 14.6 vs 93.4 ± 5.2, and 71.9 ± 17.4 vs 93.4 ± 3.8; all P < .001; for the SLVJ-H, SLDJ-H, and SLDJ-RSI, respectively). Vertical jumping performance was lower on both injured and contralateral legs compared with healthy participants (all P < .001). Only 27%, 25%, and 16% of the ACLR patients exhibited an LSI >90% for the SLVJ-H, SLDJ-H, and SLDJ-RSI, respectively, in comparison with 80%, 72%, and 86% in the control group. Moderate correlations were observed between SLDJ-H and SLVJ-H (r = 0.494; P < .001) as well as between SLDJ-RSI and SLVJ-H (r = 0.488; P < .001) in the ACLR group.
Conclusion:
Vertical jumping indexes (both symmetry and absolute values) were highly impaired 7 months after ACLR. Deficits were more marked for reactive strength ability. Clinicians should focus on restoring vertical jumping abilities to improve functional performance after ACLR.
Current recommendations after anterior cruciate ligament (ACL) reconstruction (ACLR) encourage the use of a battery of isokinetic and functional tests to improve return to sports (RTS) and reduce the risk of reinjury.9,21,22,37 While clinicians agree on isokinetic assessment protocol, there remains a lack of consensus for functional and athletic assessments4,5,21,42,49 with a large disparity in protocols, therefore requiring data4,5,42,49 to determine the most meaningful tests regarding the constraints of sport activities.4,9,12,49,52
The functional test battery currently used is mostly based on horizontal and lateral jumps (eg, single-leg hop for distance) with a passing criterion for limb symmetry index (LSI) >90%.1,7,16 Vertical jumping is rarely performed even though it targets the capacity of lower limbs to produce power output during a functional task commonly encountered in sport activities.9,28,38,39,56,62 Overall lower limb vertical power is considered the primary contributor to vertical jumping performance.9,11,13,18 Moreover, Kotsifaki et al34-36 observed that the knee joint (and the associated muscle groups) was the most important joint contributor during vertical jumps. The percentage of total work contribution for the knee joint is higher during the propulsion phase of vertical jumping than horizontal jumping (34.1% vs 12.9%, respectively) justifying the implementation of vertical jumping in functional test batteries after ACLR.
External power capacity represents the ability to produce the greatest force at the highest velocity in the shortest time. 63 Lower limb power output generation can be assessed through 2 distinct types of vertical jumps: single-leg vertical jump (SLVJ) and single-leg drop jump (SLDJ). Performance during an SLVJ is mostly related to concentric power production associated with a slow stretch-shortening cycle.6,17,20,45,60 On the contrary, performance during an SLDJ is mainly related to plyometric power production associated with a fast stretch-shortening cycle (F-SSC), and thus the reactive strength, meaning the ability to effectively use the F-SSC.13,18,30,43,44,46,47
Vertical jumping performance can be assessed during the SLVJ by measuring the height of the jump (SLVJ-H)10,13,19,48 and during the SLDJ by measuring the height of the jump (SLDJ-H) or the reactive strength index (SLDJ-RSI), which is calculated by dividing the jump height by the ground contact time.8,20,24
Performance on vertical jumping tests after ACLR has already been evaluated, and previous studies consistently identified a deficit in performance on the injured leg.13,25,29,34,37,42,45,54 It is worth noting that some studies comparing jumping performance between ACLR and control participants also observed a poorer performance on the uninjured leg in ACLR patients.15,51 However, to the best of our knowledge, SLVJ and SLDJ variables (SLVJ-H, SLDJ-H, and SLDJ-RSI), which inform different jumping qualities, have never been explored concomitantly after ACLR with comparisons in their recovery and with healthy individuals.
The aim of this study was therefore to explore both SLVJ and SLDJ performance 7 months after ACLR by (1) comparing the symmetry of these indexes in ACLR patients and healthy participants, (2) comparing these indexes of the injured and contralateral legs of ACLR patients with that of healthy participants, and (3) evaluating the association between the 3 jumping indexes assessed during SLVJ and SLDJ (SLVJ-H, SLDJ-H, and SLDJ-RSI).
Our initial hypothesis was that the LSI for vertical jumping performance would be lower after ACLR compared with healthy participants. We also supposed that only a small proportion of patients after ACLR would be able to achieve an LSI >90% at 7 months postsurgery, particularly for SLDJ-RSI. Our third hypothesis was that the performance of the uninjured leg of the ACLR group would be lower than that of healthy participants.
Methods
Population
All ACLR patients who performed functional testing at our center between January 2019 and December 2021 were screened for eligibility. We obtained data on 202 patients. Inclusion criteria for the ACLR group were (1) participants between 16 and 40 years, (2) ACL rupture with or without associated meniscal injury, (3) patellar tendon or hamstring tendon graft, (4) preinjury Tegner score from 5 to 9, and (5) vertical jump tests performed between 6 and 8 months after ACLR. Patients were excluded from the study if they had associated grade 3 collateral ligament injury.
We obtained data on 50 healthy individuals (control group) matched to the ACLR group for mean age, height, mass, Tegner score, and sex. Inclusion criteria were (1) participants aged between 16 and 40 years and (2) Tegner score from 5 to 9. Exclusion criteria were (1) previous ACL injuries, (2) recent lower limb injury (<7 months; eg, ankle sprain), and (3) symptoms that limited lower limb testing, such as pain.
The characteristics of the 2 groups are shown in Table 1.
Characteristics of ACLR and Control Groups a

ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; BPTB, bone-patellar tendon-bone; H, hamstring tendon graft; N/A, not applicable.
Protocol
All assessments were performed by the same evaluator (T.C.), a senior physical therapist at our rehabilitation center. Both groups performed the same standardized protocol: (1) global warm-up: 15 minutes of cycling at an intensity of 150 watts; (2) specific warm-up: 4 SLVJs and 4 SLDJs on each lower limb; and (3) testing procedure with 3 SLVJs followed by 3 SLDJs performed on each lower limb (with shoes).
SLVJs were performed from a standing position with hands on the hips. The hands had to remain on the hips throughout the test. The instruction was to “spend as little time as possible on the ground and jump as high as possible.”
For SLDJs, patients stood on a 30 cm–high box. They dropped down on their lower limb and performed a maximal vertical jump. The final landing had to be stabilized on the same lower limb. The hands had to remain on the hips throughout the test. The instructions were “to react as quickly as possible on the ground and jump as high as possible during the vertical jump.”
Measurements and Data Processing
All measurements were collected and analyzed with the OPTOGAIT RX system (Microgate). The jump height (in meters) was calculated from the flight time measured during the SLVJ and SLDJ.
The SLDJ-RSI (m/s) was the ratio between the jump height during SLDJ and the contact time:
For each parameter, the LSI percentage was calculated from the following equation:

Statistical Analysis
The distribution normality of the data set was verified by Shapiro-Wilk tests. Two-way mixed analyses of variance (within group: SLVJ-H, SLDJ-H, SLDJ-RSI; between group: ACLR and control) were performed on LSI values. When an interaction or main effect was significant, post hoc tests (Holm) were performed.
For each parameter, a frequency analysis (χ2 test) was performed to determine the proportion of participants who obtained an LSI >90%.
Values of SLVJ-H, SLDJ-H, and SLDJ-RSI of both the injured and the contralateral legs of ACLR participants were compared with those of healthy participants (mean of both legs) with independent-samples t tests.
We assessed the linear correlations between all parameters with Pearson correlation tests to determine the associations between SLVJ-H, SLDJ-H, and SLDJ-RSI. The correlation magnitude (r) was defined according to the following guidelines: ≤0.20 = very weak; >0.20 to 0.40 = weak; >0.40 to 0.70 = moderate; >0.70 to 0.90 = strong; and >0.90 = very strong. 54
For all analyses, the significance level was set at .05. Statistical analyses were performed using JASP software (Version 0.14.1.0). Effect sizes (Cohen d or partial η2) were calculated and interpreted using the Hopkins scale.
Results
A significant interaction between the 3 parameters and the 2 groups was found (P = .003). Post hoc tests showed a lower value of LSI for all parameters in the ACLR group compared with the control group (SLVJ-H, SLDJ-H, and SLDJ-RSI; all P < .001). When focusing on the ACLR group, the LSI for SLDJ-RSI was lower than for SLVJ-H (P < .001) and SLDJ-H (P < .001). Conversely, no difference was found in the control group between the different parameters (all P > .05) (Figure 1).

LSI percentage for the SLVJ-H, SLDJ-H, and SLDJ-RSI for the ACLR and control groups (mean ± SD). LSI, limb symmetry index; ACLR, anterior cruciate ligament reconstruction; SLDJ-H, single-leg drop jump–height; SLDJ-RSI, single-leg drop jump–reactive strength index; SLVJ-H, single-leg vertical jump–height.
Frequency analysis (participants with an LSI >90%) showed significant differences between the ACLR and control groups for SLVJ-H, SLDJ-H, and SLDJ-RSI, respectively (all P < .001). In the ACLR group, only 27% of the participants exhibited an LSI >90% for the SLVJ-H, 25% for the SLDJ-H, and 16% for the SLDJ-RSI, respectively (Figure 2). In the control group, 80% of the participants had an LSI >90% for the SLVJ-H, 72% for the SLDJ-H, and 86% for the SLDJ-RSI, respectively (Figure 2).
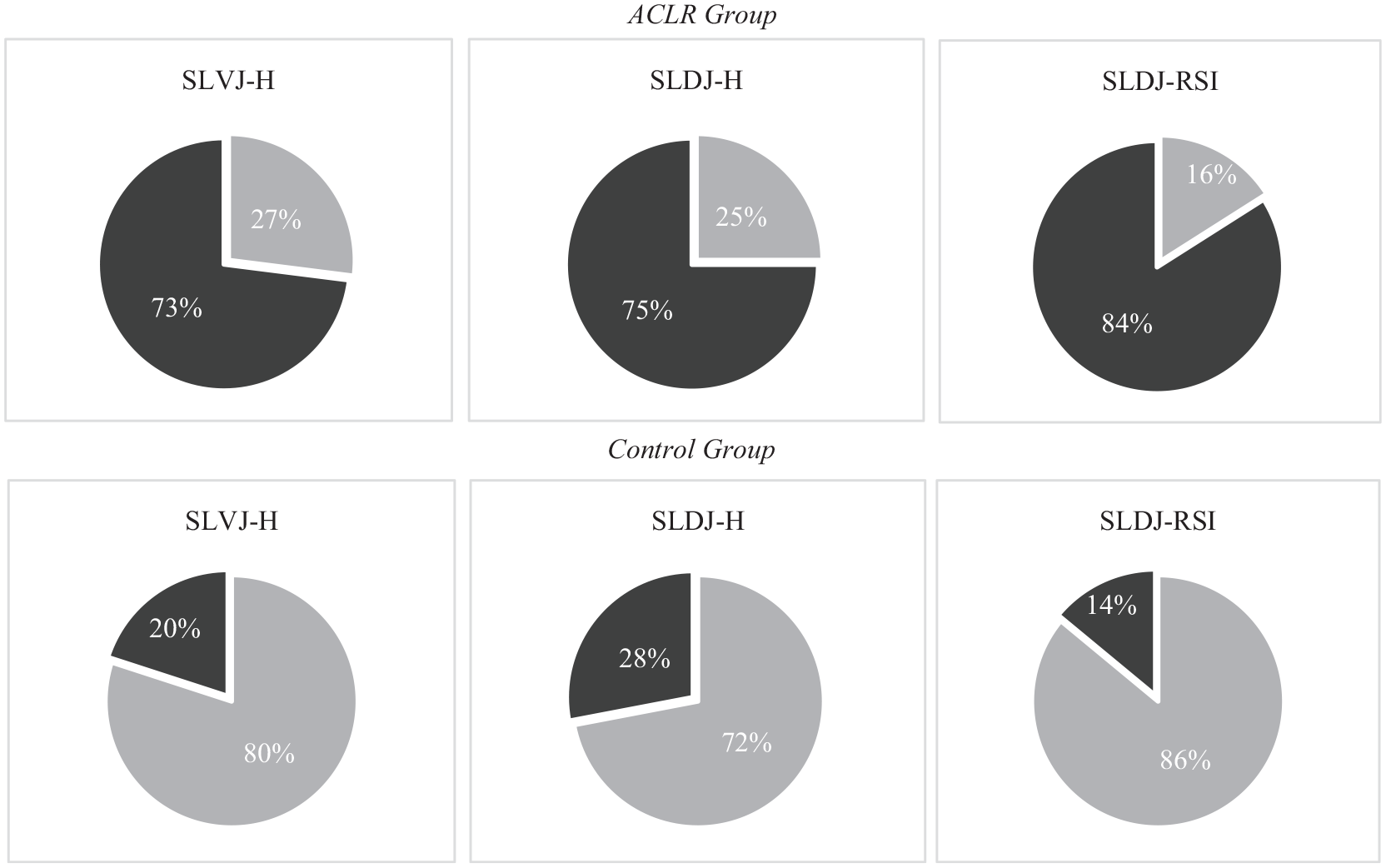
Percentage of participants with limb symmetry index above (gray) or below (black) 90% for SLVJ-H, SLDJ-H, and SLDJ-RSI in the ACLR group (top) and Control group (bottom). ACLR, anterior cruciate ligament reconstruction; SLDJ-H, single-leg drop jump–height; SLDJ-RSI, single-leg drop jump–reactive strength index; SLVJ-H, single-leg vertical jump–height.
There were significant differences between the control group and both the injured and the contralateral legs of the ACLR group for the SLVJ-H, the SLDJ-H, and the SLDJ-RSI (all P < .001) with lower values in the ACLR group (Table 2).
Values for Injured and Contralateral Legs of ACLR Group and Mean of Both Legs for Control Group a
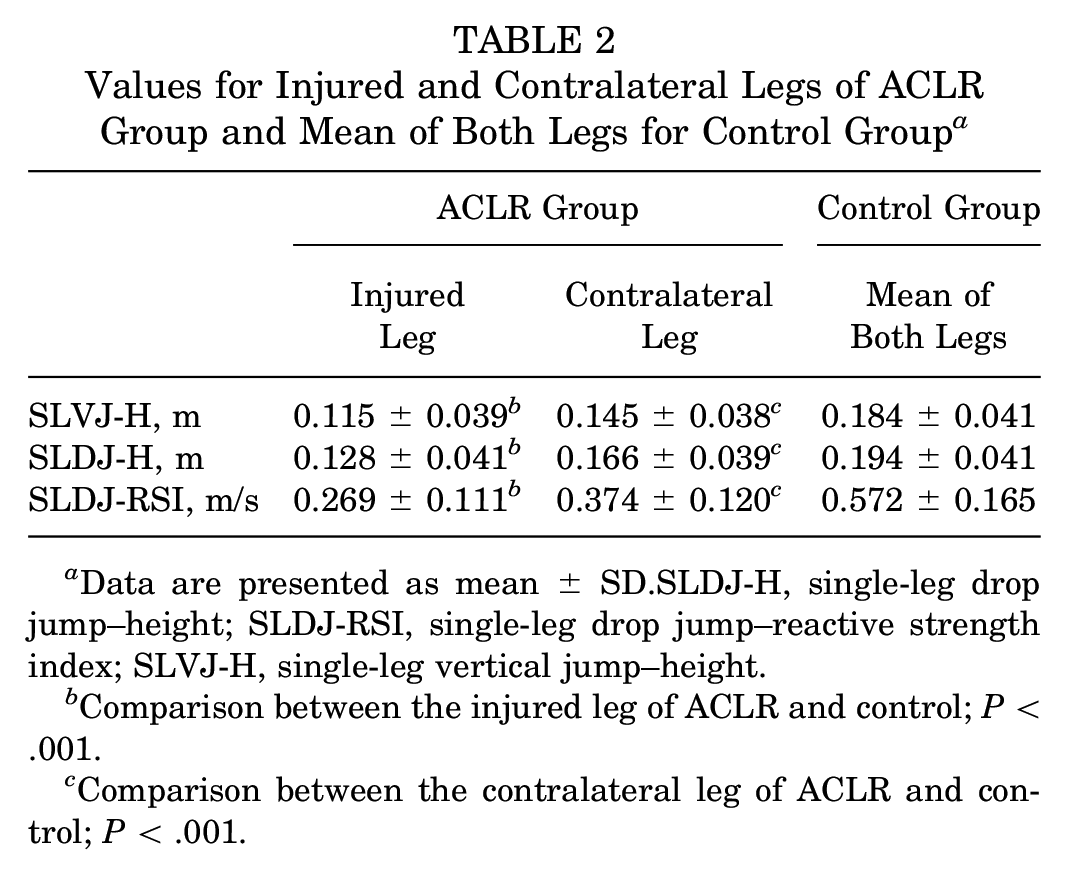
Data are presented as mean ± SD.SLDJ-H, single-leg drop jump–height; SLDJ-RSI, single-leg drop jump–reactive strength index; SLVJ-H, single-leg vertical jump–height.
Comparison between the injured leg of ACLR and control; P < .001.
Comparison between the contralateral leg of ACLR and control; P < .001.
In the ACLR group, the LSI of SLVJ-H was significantly but moderately correlated with LSI of both SLDJ-H and SLDJ-RSI. There was no significant correlation in the control group (Table 3).
Association Between LSIs of SLVJ-H, SLDJ-H, and SLDJ-RSI Within ACLR and Control Groups (Pearson Correlation Coefficient) a
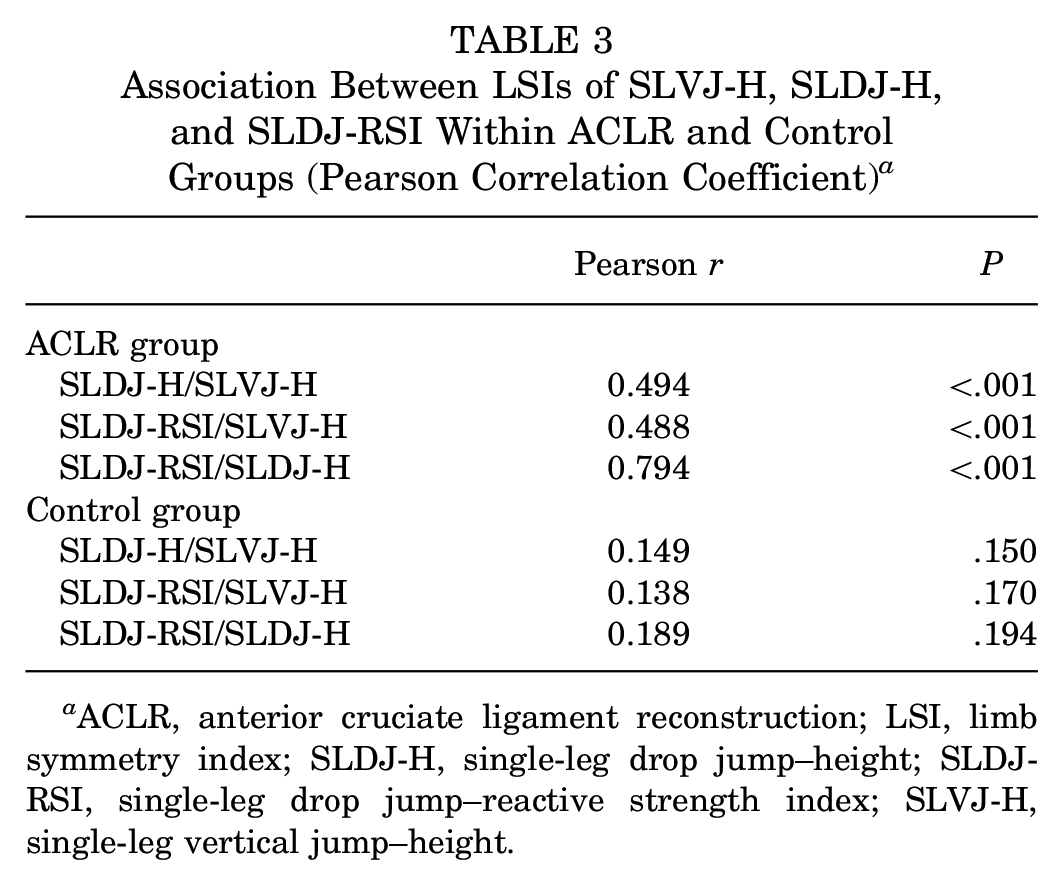
ACLR, anterior cruciate ligament reconstruction; LSI, limb symmetry index; SLDJ-H, single-leg drop jump–height; SLDJ-RSI, single-leg drop jump–reactive strength index; SLVJ-H, single-leg vertical jump–height.
Discussion
This study explored the vertical jumping performance in patients 7 months after ACLR in comparison with a group of healthy participants. Our results confirmed our first hypothesis, with lower LSI values in the ACLR group compared with the control group for all vertical jumping performance parameters. This demonstrated a deficit of vertical power generation on the injured leg, specifically during an F-SSC movement such as the SLDJ when returning to sport after ACLR.
Our results are consistent with previous studies reporting that the vertical jumping performance is highly altered after ACLR.8,13,25,29,34,36,40,41,43,53 The symmetry of performance during the SLDJ was the most altered, specifically the LSI of the SLDJ-RSI (reactive strength ability). This can be explained by a finer assessment with the inclusion of both ground contact time and jump height for the calculation of the RSI than only the measure of jump height.
The primary distinction between the SLVJ and the SLDJ lies in the duration of the stretch-shortening cycle, categorized as a slow and fast stretch-shortening cycle, respectively. Notably, in the SLDJ, there is a greater emphasis on the recruitment and stimulation of type 2 muscle fibers.2,3,31,50,58 It is conceivable that an altered neuromuscular activation pattern in motor units, particularly when producing rapid contractions28,31-33 that are inherent to athletic performance, 9 may persist. This alteration could potentially result in a reduced rate of force development among patients after ACLR, particularly evident during an F-SSC movement such as the SLDJ. Electromyography or inverse dynamic analyses are required to determine the underlying factors responsible for these deficits.
In functional testing after ACLR, an LSI value of 90% is commonly used as a threshold of success. In this study, the success rates for vertical jumping at the time of RTS were much lower than those found for horizontal jumping in the literature (>95%36,62). Our results confirm our hypothesis, with only 27%, 25%, and 16% of participants after ACLR displaying an LSI >90% for SLVJ-H, SLDJ-H, and SLDJ-RSI, respectively. The contribution from the knee joint is larger during vertical jumping than during horizontal jumping and may explain these discrepancies. 35 Vertical jumping seems therefore more discriminant to reveal persistent deficit of power output generation after knee injuries during functional task (notably at the knee joint) than horizontal jumping, which is currently used in the majority of current RTS evaluations.14,26,36,53,54,61,62 Our results support a combined use of vertical and horizontal jump testing for assessing the whole spectrum of functional knee joint recovery after ACLR.
Moreover, our results showed a high success rate in the control group, with a minimum LSI value of 80%, 72%, and 86% for the SLVJ-H, SLDJ-H, and SLDJ-RSI, respectively. A threshold LSI value of 85% (±2 SD) for the SLDJ-RSI seems to be meaningful in order to determine an appropriate symmetry recovery of reactive strength at the time of RTS.
Our findings also highlight a significant decrease in performance values in the uninjured leg of the ACLR group compared with the control group in all assessed parameters. These results are in accordance with the literature and suggest a deconditioning effect on the contralateral leg in ACLR patients.15,51 This observation confirms that relying solely on the LSI can potentially lead to an overestimation of the actual performance of the injured leg.23,27,57,59 While the use of the LSI has its merits in the context of RTS evaluation, it is crucial to bear in mind that after rehabilitation, the patient may still lack the necessary physical capabilities required for the resumption of high-intensity sports activities. Beyond the clinical and functional aspects, it becomes essential to assess the athletic performance of patients before permitting their RTS, and normative data are required to help in the decision-making process. A simplistic reliance on LSI readings after ACLR proves to be insufficient.
Finally, we found moderate associations between LSIs measured during SLVJ (SLVJ-H) and SLDJ (SLDJ-H or SLDJ-RSI). This confirmed that SLVJ and SLDJ are 2 specific jumping tasks assessing different strength capacities (ie, power output production during slow and F-SSC movements, respectively). Including both tests during a functional test battery seems therefore meaningful to evaluate the neuromuscular requirements related to sport participation. Our results suggest that clinicians should monitor vertical jumping abilities through the RTS continuum and implement specific training to restore functional performance.
This study presents certain limitations. We did not consider morphological specificities or preinjury athletic ability of the participants. It would have been meaningful to standardize the drop-jump height based on biomorphological attributes and preinjury jumping abilities. This may explain why 28% of the participants in the control group were not able to meet the RTS criteria (LSI >90%) on the SLDJ-H.
We also did not perform subgroup analysis by type and level of sport (Tegner score), and this could have influenced the results of our studies. However, at group level, there was no difference in Tegner scores.
Conclusion
Vertical jumping performance is still highly impaired 7 months after ACLR, specifically, reactive strength ability. Incomplete restoration of vertical jumping symmetry and altered performance on both injured and contralateral legs may compromise the ability to RTS after ACLR.
Footnotes
Acknowledgements
The authors thank all the participants involved in this study. The authors also acknowledge Pierre Samozino and Benoit Pairot de Fontenay as co-last authors in recognition of their significant contributions to this research.
Final revision submitted January 25, 2024; accepted February 12, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Conseil d’Orientation Scientifique Ramsay Santé (COS-RGDS-2023-01-004-PAIROT-DE-FONTENAY-B).