
Abstract
Background:
Patient-reported outcomes and return-to-play (RTP) rates are inferior after revision anterior cruciate ligament reconstruction (ACLR) compared with primary ACLR. Physical properties such as maximal, explosive, and reactive strength influence reinjury and RTP rates after ACLR. No study has compared these outcomes between revision and primary ACLR.
Purpose:
To compare maximal, explosive, and reactive strength of the ACLR limb, as well as patient-reported outcomes and RTP rates between primary and revision ACLR at 9 months after surgery.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A comparative study was performed at 9 months after surgery for 344 male athletes who had undergone ACLR (298 primary, 46 revision). Maximal strength of the ACLR limb was measured by means of isokinetic dynamometry. Explosive strength was measured by use of single-leg countermovement jump height, and reactive strength was measured by single-leg drop jump. Patient-reported outcomes and responses to RTP questionnaires were recorded for both groups.
Results:
The primary ACLR group had higher scores than the revision ACLR group for single-leg countermovement jump height (P = .02) and single-leg drop jump reactive strength index (P = .01) on the ACLR limb. No significant difference was observed between groups on maximal strength of the quadriceps or hamstring, and no significant difference in limb symmetry index was observed between groups on any strength or jump test. The primary ACLR group demonstrated higher scores on the Marx Activity Rating Scale (P = .03) and the Anterior Cruciate Ligament–Return to Sport after Injury scale (P < .001). Athletes in the primary ACLR group were more likely to have returned to sport (P < .001).
Conclusion:
At 9 months after surgery, athletes who had undergone revision ACLR achieved maximal strength similar to that of athletes who had undergone primary ACLR. However, athletes who had revision ACLR demonstrated lower scores on explosive and reactive strength tests. Athletes who underwent revision ACLR had lower RTP rates at 9 months after surgery, potentially due to explosive and reactive strength deficits and lower perceived readiness for RTP.
Anterior cruciate ligament (ACL) injury is a common knee injury, with an incidence of 68.6 per 100,000 person-years. 32 ACL injuries are commonly seen during landing and cutting movements in field and court sports. 20,30 The incidence of ACL rupture has been reported to be as high as 0.32 tears per 1000 exposures in athletes who play sports such as soccer, rugby, and basketball. 31 ACL reconstruction (ACLR) is often performed to restore structural stability to the knee and facilitate return to sport. Approximately 75% of ACL ruptures will have ACLR, with this figure even higher in young athletes targeting return to sport. 32
Despite the volume of ACLR carried out annually, outcomes after ACLR can be mixed. Ardern et al 3 found that only 55% of athletes managed successful return to competitive sport after primary ACLR (P-ACLR). Reinjury is also a significant concern after ACLR, with reinjury rates shown to be as high as 23% in younger athletes. 34,36 In athletes who are reinjured and wish to return to sport, a revision ACLR (R-ACLR) is commonly performed. Athletes who undergo R-ACLR have poorer patient-reported outcomes at 1 and 5 years after surgery 1,22 and are significantly less likely to return to their previous level of participation in sport compared with P-ACLR. 22 Previous research comparing the 2 groups has focused on scoring of patient-reported outcome measures but has not explored whether the 2 groups perform differently on sport-specific functional tests. 22 Deficits in these physical properties may account for the poorer outcomes and the poorer return-to-play (RTP) rates.
Physical properties such as maximum strength, explosive strength, and reactive strength have also been shown to influence reinjury outcomes after ACLR, 11,21 and it is recommended that objective physical testing be carried out before athletes are cleared for RTP. 4,26 Isokinetic dynamometry is commonly used to assess quadriceps (QT) and hamstring (HS) strength and to assess strength imbalances between limbs after ACLR. 14 Explosive strength (speed strength) refers to the ability to rapidly change from eccentric to concentric muscle action on jumping tasks (duration >250 ms). 37 The countermovement jump has been shown to be a valid and reliable measure of lower limb explosive strength in male athletes. 24 Reactive strength refers to the ability to rapidly change from eccentric to concentric muscle action on plyometric tasks of shorter duration (100-250 ms). 37 The drop jump has been shown to be a valid and reliable measure of reactive strength. 24 Asymmetries and deficits on the drop jump have been shown to predict dysfunction 2 years after ACLR. 17 A 2018 study by King et al 18 demonstrated the relevance of assessing reactive strength using a single-leg drop jump (SLDJ) to identify deficits after ACLR. Reactive strength capabilities are typically expressed as a reactive strength index (RSI), which involves dividing jump height by ground contact time on a plyometric task. 37 RSI has been shown to give a reliable measurement of an athlete’s explosive capabilities in plyometric activities. 9 Despite the importance of physical recovery after ACLR, deficits in maximum strength, explosive strength, and reactive strength have been observed in the operated limb after ACLR when athletes RTP. 12,18 The current literature does not provide insight as to whether these qualities are worse after R-ACLR, and given that these are trainable qualities, this knowledge could be used to enhance rehabilitation after R-ACLR to result in greater RTP rates and improvements in performance.
Psychological factors and subjective knee function as measured by patient-reported outcomes have also been shown to influence outcomes after ACLR. 2,27 Instruments such as the International Knee Documentation Committee (IKDC) subjective knee form, 15,16 the Anterior Cruciate Ligament–Return to Sport after Injury (ACL-RSI) scale, 2,35 the Cincinnati Knee Score, 5 and the Marx Activity Rating Scale 25 have been shown to be valid and reliable measures of subjective knee function, perceived readiness to return to sport, and activity levels after ACLR. It is has been reported that patient-reported outcomes and RTP rates are lower after R-ACLR. 1,22 However, to our knowledge, no previous studies have compared physical outcomes relating to maximum strength, explosive strength, and reactive strength between R-ACLR and P-ACLR, which may play some role in the difference in subjective and perceived function between the groups.
The aim of this study was to compare maximum muscular strength and jump performance (explosive and reactive strength) of the ACL-reconstructed limb (ACLR limb) as well as evaluate limb symmetry, patient-reported outcomes, and RTP rates in P-ACLR versus R-ACLR male, field-sport athletes at 9 months after surgery. The 9-month follow-up assessment was selected for this study because this was when participants were most commonly cleared for RTP by their surgeon. It was hypothesized that the R-ACLR group would demonstrate inferior performance of the ACLR limb on objective maximum strength, explosive strength, and reactive strength tests. It was also hypothesized that the R-ACLR group would demonstrate inferior outcomes on patient-reported outcome measures, RTP rates, and level of RTP at 9 months from surgery.
Methods
Study Design
Participants for this study were recruited from a caseload of 2 specialist orthopaedic surgeons (R.M., M.J.) from January 2014 to December 2016. Individuals who were scheduled to undergo ACLR were invited to participate in the study and were included after informed consent was provided. Ethical approval was granted through the institution's ethics board.
To maintain a homogeneous sample, we defined the study inclusion criteria as male athletes between the ages of 18 and 35 years who played multidirectional field sports, had undergone P-ACLR or R-ACLR, intended to return to the same or higher level of sport than before injury, and returned for their 9-month follow-up assessment after discharge from their surgeon. Exclusion criteria included patients who experienced a contralateral second injury, those who underwent multiligament reconstructive surgery, those who did not intend to return to a similar level of sport compared with before their injury, and those who did not complete their 9-month follow-up assessment. In total, 344 male field-sport athletes who had undergone ACLR were included in the analysis (298 P-ACLR and 46 R-ACLR) (Figure 1). Descriptive data for the cohort are reported in Table 1.

Distribution of groups. ACL, anterior cruciate ligament; ACLR, ACL reconstruction.
Descriptive Data for the Cohort a
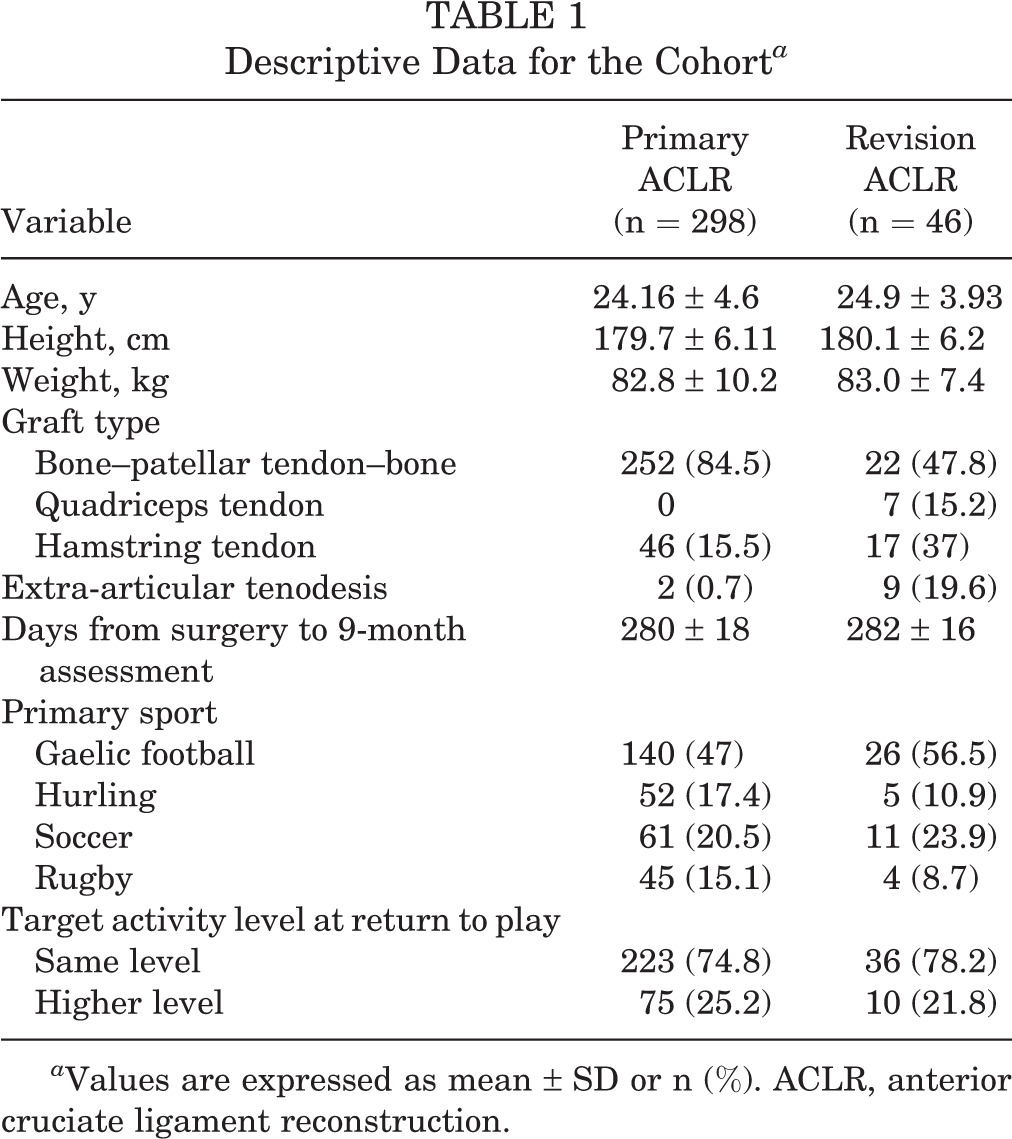
a Values are expressed as mean ± SD or n (%). ACLR, anterior cruciate ligament reconstruction.
After recruitment into the study, all participants completed a preoperative questionnaire providing details on their mechanism of injury, sports played, and the level of sport to which they planned to return. Arthroscopic ACLR was performed in all cases in a standardized fashion with grafts placed within the remnant footprints. All R-ACLR procedures were performed as a 1-stage procedure. Graft choice varied between bone–patellar tendon–bone (BPTB) and HS (gracilis/semitendinosus double bundle) in the P-ACLR group (252 BPTB, 46 HS) and BPTB, HS, and QT in the R-ACLR group (22 BPTB, 17 HS, 7 QT). An extra-articular tenodesis using the iliotibial band was performed where deemed appropriate by the operating surgeon, in a total of 11 cases (2 P-ACLR and 9 R-ACLR) (Table 1).
Owing to geographical limitations and sample size, athletes were rehabilitated by their own physiotherapist locally. They were advised to see their physiotherapist approximately every 2 to 3 weeks over the duration of their rehabilitation, and a rehabilitation protocol was provided to all participating physiotherapists. Participants presented to the facility for follow-up functional testing at 3, 6, and 9 months after surgery, at which time progress was assessed subjectively through patient-reported outcomes and objectively through maximum strength, explosive strength, and reactive strength tests. Patient-reported outcome measures and information on RTP status were also collected at this assessment.
Testing Procedure
Athletes performed a standardized 5-minute dynamic warm-up before testing. The non–ACL reconstructed (non-ACLR) limb was always tested first. Isokinetic dynamometry was conducted by use of the Humac Norm Isokinetic Extremity System (Computer Sports Medicine) to measure QT and HS strength. Following the guidelines published in a recent systematic review, 33 we used a protocol of 5 repetitions of concentric knee extension and flexion at an angular velocity of 60 deg/s, at a set range of motion of 0° to 100° using gravity correction. Athletes were given a practice set to familiarize themselves with the machine and the procedure before completing 2 test sets. Of these 2 sets, the set with the lowest interrepetition coefficient of variance was selected as an athlete’s maximum strength score to ensure optimum accuracy. Strength measures of the QT and HS were recorded in terms of peak torque (N·m) as a percentage of the participant’s bodyweight in kilograms [(Peak Torque ÷ Bodyweight) × 100] per O’Malley et al. 29 Limb symmetry index (LSI) was then calculated for both QT and HS strength by dividing the ACLR limb score by that of the non-ACLR limb and multiplying the outcome by 100.
Lower limb explosive strength was evaluated by analyzing jump height on the single-leg countermovement jump (SLCMJ). Reactive strength was evaluated through analysis of the SLDJ. Testing was conducted in a 3-dimensional (3D) motion capture laboratory using an 8-camera 3D motion analysis system (Bonita B10; Vicon), synchronized with two 40 × 60–cm force platforms (BP400600; AMTI). Vicon Nexus software (Version 1.8.2; Vicon) simultaneously collected and analyzed the force data at 1000 Hz. Kinetic and kinematic data were collected, but only the kinetic data were reported in this study. Jump height on the countermovement jump was calculated through use of the momentum impulse relationship. 23 Athletes executed 3 practice repetitions before performing 3 recorded maximal efforts on each leg, starting with the non-ACLR limb. Athletes kept their hands on their hips in all cases for consistency. The best jump height from the recorded valid trials was used in the analysis. A similar testing protocol was used for evaluation of reactive strength on the SLDJ, which was carried out from a 20-cm box. 18 Athletes were instructed to “spend as little time as possible on the ground” and “jump as high as possible.” Jump height and ground contact time were recorded. RSI for the drop jump was calculated by dividing jump height by ground contact time. 37 The LSI was calculated for both the SLCMJ and SLDJ to report any interlimb differences in explosive and reactive strength.
Statistical Analysis
A Shapiro-Wilk test was used to test for normal distribution of the data. The P-ACLR and R-ACLR groups were compared on each variable. An independent-samples Student t test was used to analyze parametric variables, whereas a Mann-Whitney U test was used to analyze nonparametric variables. A chi-square test was used to analyze distribution of the RTP rates between the 2 groups. All statistical analysis was conducted through JASP statistical analysis (Version 0.8.6). Where appropriate, effect sizes were reported; an effect size threshold of d ≥ 0.2 was categorized as small, d ≥ 0.5 was categorized as medium, and d ≥ 0.8 was categorized as large. 6
Results
No significant difference was seen on the ACLR limb between groups in QT or HS peak torque relative to bodyweight (Table 2), and no significant difference was found between groups in relation to QT or HS LSI. A significant difference between the R-ACLR and P-ACLR groups was noted in SLDJ performance on the ACLR limb, although the effect size was small, with the R-ACLR group demonstrating a lower RSI on the ACLR limb (P = .01). A small effect size difference was also seen between the 2 groups in relation to SLCMJ height on the ACLR limb, with the R-ACLR group producing lower jump heights than the P-ACLR group (P = .02). No significant difference was observed between groups in relation to LSI of SLCMJ and SLDJ height or RSI of SLDJ.
Descriptive Data for Outcome Variables a

a Bolded P values indicate statistically significant differences between the primary and revision ACLR groups (P < .05). ACL, anterior cruciate ligament; ACLR, ACL reconstruction; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury scale; IKDC, International Knee Documentation Committee; LSI, limb symmetry index; RSI, reactive strength index. Peak torque % bodyweight was calculated as follows: [Peak Torque (N·m) ÷ Bodyweight (kg)] × 100. LSI was calculated as follows: (Operated Limb ÷ Nonoperated Limb) × 100.
b Values are expressed as n/N (%).
In relation to patient-reported outcomes, a significant difference was noted, with medium effect size, between the 2 groups on the ACL-RSI questionnaire (P < .001), with the R-ACLR group demonstrating lower scores than the P-ACLR group. As well, a significant difference was found between groups, with small effect size, in the Marx Activity Rating Scale (P = .03), with the R-ACLR group reporting lower scores. No significant difference between the 2 groups was noted on the Cincinnati Knee Score or the IKDC at 9 months after surgery. A significant difference was found between groups relating to return to sports (Table 2), with the R-ACLR group reporting lower RTP rates (P < .001). In the P-ACLR group, 55% of athletes had returned to play by 9 months after surgery, whereas only 26% of the R-ACLR athletes reported doing so.
Discussion
This study demonstrated that athletes who underwent R-ACLR performed significantly worse than those who underwent P-ACLR on jump tests measuring explosive strength and reactive strength of their ACLR limb, despite there being no difference between the 2 groups in relation to QT or HS strength of the ACLR limb. Patient-reported outcomes were also significantly different between the 2 groups for the Marx Activity Rating Scale (small effect size) and the ACL-RSI (medium effect size), with lower scores in the R-ACLR group for both despite no between-group difference on the IKDC and Cincinnati questionnaires. This combination of reduced explosive and reactive strength alongside lower perceived readiness to RTP may contribute to the lower RTP rates and activity levels in the R-ACLR group at 9 months after surgery, and additional targeting of these qualities during rehabilitation may improve outcomes.
Dauty et al 7 also demonstrated that strength deficits in the ACLR limb after R-ACLR were similar to those observed after P-ACLR. However, our findings differ from those of Gifstad et al, 10 who reported lower isokinetic QT and HS strength on the ACLR limb in R-ACLR compared with P-ACLR. No studies have previously compared explosive and reactive strength between R-ACLR and P-ACLR groups. Prior research has shown that single-leg explosive strength and reactive strength qualities are related to running speed and change of direction performance 8 and form a key component of ACL injury prevention programs. 13,28 The current study demonstrated lower scores for single-leg explosive strength (SLCMJ height) and single-leg reactive strength (SLDJ) on the ACLR limb after R-ACLR despite there being no difference in LSI between groups. Neither group achieved >90% LSI on SLCMJ, SLDJ, or QT maximal strength tests, indicating that neither group achieved RTP criteria identified in previous research. As well, no significant difference was seen in LSI between the 2 groups on any of the tests, despite the R-ACLR group demonstrating significantly smaller absolute scores on jumping tasks. This raises a possibility that R-ACLR athletes may experience a chronic deconditioning effect in not only their ACLR limb but also their non-ACLR limb. In summary, although R-ACLR participants regained similar levels of QT and HS strength at 9 months after surgery, they had yet to regain similar explosive and reactive strength qualities relative to their P-ACLR counterparts. This suggests that R-ACLR athletes place a greater emphasis on development of these qualities throughout their end-stage rehabilitation.
This study also reported differences between groups in relation to the ACL-RSI questionnaire, with the R-ACLR group scoring lower than the P-ACLR on this scale. The ACL-RSI is a patient-reported outcome measure that focuses on analyzing the athlete’s perceived readiness to return to sport. The lower score seen in the R-ACLR group highlights the potential additional psychological impact that a second ACL injury can have on an athlete’s perceived readiness to RTP at the same stage after surgery as P-ACLR. Given the high physical, psychological, and financial cost of ACLR, these differences are understandable. Previous studies have demonstrated that psychological readiness to return to sport (as measured by the ACL-RSI) is the variable most associated with returning to preinjury level of participation in sport. 2 Ardern et al 2 reported that the 3 most common reasons athletes do not RTP after ACLR are lack of trust in the knee, fear of reinjury, and poor knee function. Our findings are in agreement with a 2017 study by Lefevre et al, 22 who also related poorer outcomes on the ACL-RSI along with poorer RTP rates in their R-ACLR group compared with their P-ACLR group (49.1% vs 63.6% RTP) at 1 year after surgery. We observed a significantly lower RTP rate at 9 months after surgery in the R-ACLR group compared with the P-ACLR group, in keeping with the lower scores reported on the ACL-RSI scale and the Marx Activity Rating Scale. This occurred despite no difference between groups on self-reported knee function in the IKDC and Cincinnati questionnaires. In our cohort, 55% of the P-ACLR group had succeeded in returning to their sport at 9 months compared with 26% of the R-ACLR group. Both the reduced perceived readiness to RTP and deficits in explosive and reactive strength may have contributed to this lower RTP rate and activity levels at 9 months after R-ACLR.
These findings suggest that clinicians treating R-ACLR athletes who intend to return to sport may need to inform athletes that their recovery may take longer than after their primary reconstruction. There is also the possibility that clinicians, surgeons, and athletes are more cautious about returning to sport after the second injury, and this could account for the delayed RTP times in this group. Clinicians should direct end-stage rehabilitation toward targeted strategies to improve jump performance through specific jump and plyometric training to address deficits in explosive and reactive strength in this cohort. These R-ACLR athletes may also need more exposure to sport-specific and match-specific practice before they RTP to address their fears about reinjury.
Limitations
Cohort size differed between the P-ACLR and R-ACLR groups. This was due to the lower incidence of R-ACLR surgery, and future studies should look to obtain larger numbers of R-ACLR athletes. Objective knee laxity was not measured using a device such as the KT-1000 arthrometer. There is a possibility that knee laxity could be more evident in the R-ACLR group, thereby affecting performance on dynamic tasks. Although the relatively homogeneous participant group (male field-sport athletes between the ages of 18 and 35 years) is undoubtedly a strength of this study, we cannot transpose our results to different participant groups such as female or adolescent athletes. In addition, the study examined only the performance qualities of maximum, explosive, and reactive strength, without examining the movement patterns with which these tests were executed. Previous research has suggested that biomechanical deficits can be evident in the absence of jump performance deficits, and biomechanical analysis may demonstrate physical differences between the 2 groups not highlighted by the performance measures used. 19 Future research should examine biomechanical differences between groups and the influence of interventions specifically targeting explosive and reactive strength after R-ACLR on RTP, activity levels, and self-perceived readiness for RTP.
Conclusion
This study demonstrated deficits in explosive and reactive strength in the ACLR limb of patients in the R-ACLR group compared with the P-ACLR group at 9 months after surgery. Participants who had undergone R-ACLR had lower RTP rates, lower self-perceived readiness to RTP (ACL-RSI scores), and lower activity levels (Marx Activity Rating Scale scores), despite there being no between-group difference in QT and HS strength. This study suggests that R-ACLR athletes target additional explosive and reactive strength exercises during rehabilitation as well as strategies to improve perceived readiness to RTP, which may improve activity levels and RTP rates, compared with P-ACLR groups. These findings may influence the management strategies of the clinician aiming to return an athlete to multidirectional field sport after R-ACLR.
Footnotes
Final revision submitted April 5, 2020; accepted April 24, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by Sports Surgery Clinic, Dublin, Ireland. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Sports Surgery Clinic Research Ethics Committee (ref No. 25-AFM-010).