
Abstract
Background:
Partial anterior cruciate ligament (ACL) tears, particularly injuries detected with magnetic resonance imaging (MRI) but stable on ligamentous examination, appear to be recognized more frequently; however, there remains no consensus management for this complex pathology.
Purpose:
To present the results of a survey of a group of international ACL experts on the management of partial ACL injuries.
Study Design:
Survey study; Level of evidence, 5.
Methods:
The ACL Study Group is an international group of orthopaedic surgeons with a special interest in the ACL. There are 169 members overall, with 135 clinically active surgeons. A branching logic survey was developed and circulated to members of the ACL Study Group via electronic mail. Categories included member demographics as well as recommended management strategies of partial ACL injuries, including recommendations on return to play.
Results:
Of the 135 clinically active surgeon members, 113 responded to the survey (84%). Nonoperative management of partial ACL injuries was selected by 92% of respondents. Of those who managed nonoperatively, 75% indicated they would not restrict weightbearing and 59% would not recommend a knee brace. When those who managed the patient nonoperatively determined criteria for return to sports (RTS), 33% would use differential knee laxity, 87% would assess functional testing, 26% would utilize imaging, and 40% selected time from injury. When using time as a guide for RTS, 13% chose RTS between 7 and 11 weeks postinjury, 56% selected no sport before 3 months, and 22% favored waiting 4 to 6 months before allowing an athlete with a partial ACL injury to RTS. With regard to function as a tool to determine RTS, painless Lachman, strength, swelling, and functional performance tests were all chosen by a majority of respondents.
Conclusion:
This study presented the results of a survey on partial ACL injury management administered to ACL Study Group active surgical members. The majority favored nonoperative management for partial ACL injuries (stable ligament examination but MRI changes in the ligament). Nonoperative treatment and RTS protocols varied and must be customized to the patient.
Partial tears of the anterior cruciate ligament (ACL) are a relatively common cause of sports injury. Although there exists no standardized definition or diagnostic procedure, partial ACL tears are estimated to make up 10% to 27% of isolated ACL injuries.5,14,24 Diagnostic modalities often include ≥1 of the following: clinical signs, intraoperative, magnetic resonance imaging (MRI), and/or arthrometry. Multiple definitions based upon these diagnostic tools have been proposed. Historically, partial ACL tears were diagnosed when there was a “significant portion” of 1 or both bundles remaining in continuity, <5 mm of laxity on testing, and a trace or negative pivot shift.2,4 However, this is changing with advances in imaging technology, including MRI. Further, advances in understanding of the pathology and how it is related to functional stability as opposed to structure alone is also altering the landscape of definition and management of these injuries.
Considering this diagnostic ambiguity, along with a lack of basic science foundation to understand healing of partial ACL injuries, it follows that there is no concrete treatment algorithm. Fundamentally, treatment should be customized to the patient based upon symptomatology, demand, concomitant injury, and particularly risk of progression to complete ACL tear. Nonoperative management typically consists of progressive physical therapy with or without initial restrictions or immobilization.1,7,14,15,17 This method of management may be best utilized in those with reasonably low risk of progression. Results in the appropriate patient have had reasonable success.9,16,21 Surgical management may be indicated in patients with a high likelihood of failure. 23 However, it is still not determined which method of treatment is best. Further, there is a dearth of data on the healing potential and timing of healing of partial ACL tears with overall maintained integrity (no laxity). Although many patients may be treated nonoperatively, there are no accepted guidelines due to lack of basic science to guide recommendations for rehabilitation protocol or return to sports (RTS). 23
In lieu of this, expert consensus may offer valuable insight into, or at least serve as a starting point to better understand, the optimal management of this injury. The ACL Study Group is an international group of orthopaedic surgeons and scientists that was founded with the goal to “advance the art and science of knee soft tissue surgery, rehabilitation, and injury prevention.” Given this focus, a survey of members’ opinions may be of use for those encountering partial ACL injuries in practice. The goal of this study was to present the results of an ACL Study Group survey on the management of partial ACL injuries.
Methods
The ACL Study Group is an international group of orthopaedic surgeons with a special interest in the ACL. It is a society of international knee surgeon “experts” who are voted in as members by their peers. There are 169 members overall, with 135 clinically active surgeons (119 active members, 16 associate members, 4 scientists, and 30 emeritus members). The survey, described below, was sent to all members of the ACL Study Group using the membership roster, which includes electronic mail addresses of each member.
In the fall of 2023, a survey was created consisting of a case presentation of a typical young patient with a partial ACL injury (a patient of the senior author, M.R.S.) followed by a questionnaire (Supplemental Figure S1 and Supplemental Table S1, available separately). The case scenario involved a high school athlete with an acute knee injury sustained during sports, but unclear mechanism of injury, an MRI demonstrating edema within the ACL and physical examination including full knee motion, negative Lachman maneuver, and negative pivot shift. A brief description of the image and 2 sagittal cuts from the MRI were provided, as well as status of menisci and bone bruising. The questions were developed internally with input from the 4 authors who are experienced ACL surgeons (G.D.A., S.L.S., T.S., and M.R.S.). It was developed with a branching logic format to follow responses with appropriate follow-up questions based upon management choices. For example, those who selected nonoperative management were subsequently asked if and how they would limit weightbearing. The last component was member demographics questions. After approval from the institutional review board, the questionnaire was distributed to all surgeon members of the ACL Study Group using an online survey software (Qualtrics).
Surveys were sent out on September 5, 2023. There were 2 separate reminders sent to the ACL Study Group, during the weeks of October 14 and November 6. Personal correspondence from the senior author with those who did not perform the survey occurred November 21. There were no other clarifications or other correspondences concerning the questions between participants and research team or principal investigator (M.R.S.) during the survey period. No surveys were accepted after December 1. After the collection period, the data from active surgeon members were aggregated and used for primary analysis. Some of the questions were designed to allow for choosing multiple answers. In cases where responses are reported as a percentage of total (“yes” or “no” in binary), the total percentage may sum to over 100%. Analysis was performed in Microsoft Excel.
Results
Demographics
A total of 113 members (84% of active associate and surgeon members)correctly filled out the survey and were included. Approximately 27% of members were from North America, 9% from Asia, 45% from Europe, 12% from Oceana, 0.9% from Africa, 5.3% from Latin America, and 1.8% from the Middle East. Under 2% were <5 years in practice, 11% were 6 to 10 years into practice, 23% were 11 to 20 years into practice, and 64% were >20 years into practice. Of participants, 4% were female. Of respondents, 30% worked in an academic setting, 54% mixed setting, and 13% private or nonacademic.
Operative Treatment
Only 6 (5.4%) active surgical members chose primary surgical treatment for the management of the presented case of partial ACL injury. Of those who opted for surgical management, 1 (17%) chose ACL reconstruction, 1 (17%) chose ACL augmentation, 3 (50%) chose single-bundle reconstruction, and 1 (17%) chose repair. All complete ACL reconstruction and augmentation procedures were chosen by North American surgeons while international surgeons comprised all partial (single-bundle) reconstruction and repair responses.
Nonoperative Treatment
The overwhelming majority (92%) of active surgeon members opted to treat the case scenario patient nonoperatively. Of respondents, 25% indicated they initially would limit weightbearing. Of these respondents, 42% opted for 1 to 3 weeks of limited weightbearing using crutches, 39% chose 4 to 6 weeks of crutch assistance, and 19% selected ambulatory-assist devices only if the patient were limping.
Of those who chose to manage nonoperatively, 41% indicated they would use a knee brace. For those who selected bracing, the respondents had the opportunity to select the type of brace they would prescribe: 57.1% would have chosen a rigid double upright functional ACL brace while 35.7% would have chosen a long-hinged postoperative type of brace. Most would use the brace for 4 to 6 weeks (69%); 19% would use a brace for less time, and 12% would brace for longer or “other”. When comparing across demographics, North American respondents braced significantly longer than international surgeons, and academicians significantly longer than mixed or private practice (P < .5).
When queried about whether they would recommend a brace for return to play, fewer respondents selected they would recommend a brace to return to play, with only 20% choosing “yes.”
Members who selected nonoperative management of these injuries were asked whether they would use biologics in their treatment algorithm. Active surgical members utilizing nonoperative management tended not to utilize biologics (10% would use biologics).
There were several options for determining RTS for those who selected nonoperative management; >1 answer was allowed. The most common was function, at 87%, followed by time from injury at 40%. Next was differential laxity with 33%, and last was imaging, with only 26% relying on imaging to determine when an athlete was able to RTS (Figure 1).

Bar graph depicting determination of return to sports.
For those who selected functional assessment as criteria to RTS, many chose >1 option. The most commonly identified response was a functional performance test with 87.8%. Next was extremity strength, with 77%, followed closely by knee joint swelling, with 76%. Last was painless Lachman maneuver with 52% (Figure 2).

Bar graph depicting return to sports by function.
The majority (56%) of respondents choosing time from injury to determine RTS indicated waiting 3 months from injury before allowing the athlete to return. Another 22% picked 4 to 6 months, while 13% chose 7 to 11 weeks. Few chose outside the time range of 6 weeks to 9 months (Figure 3).
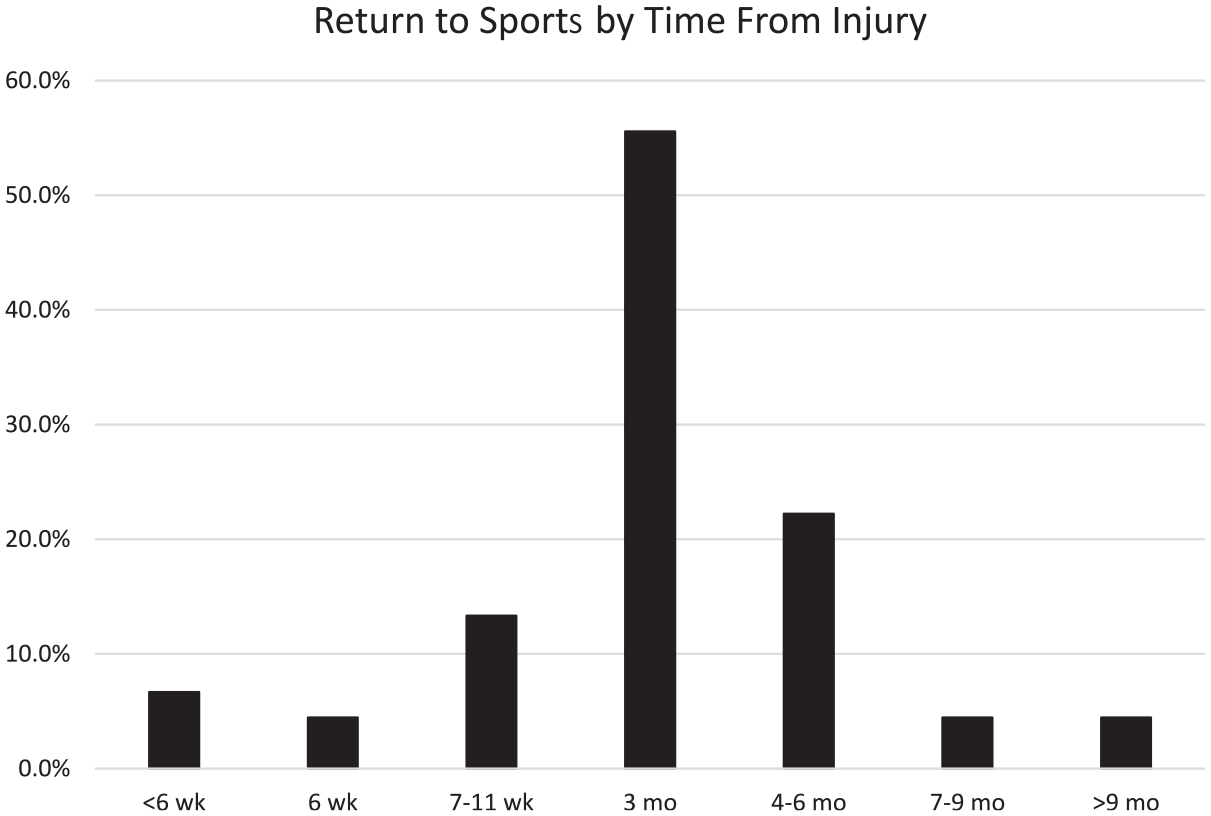
Bar graph depicting return to sports by time from injury.
If a patient were to demonstrate any laxity, all else being equal, some members recommended differential laxity as a determinant for RTS. Various options were presented to assess laxity, including KT-1000 arthrometer, Lachman maneuver, or both. A total of 22% chose KT-1000 arthrometer, 33% selected Lachman, and 44% recommended a combination.
Although imaging was chosen by fewer members, all respondents who selected imaging as a factor to determine readiness to RTS opted for MRI.
Discussion
Due to a relative dearth of scientific or consensus information to guide management of patients with partial ACL tears, we attempted to distill the opinions of the active surgical members of the ACL Study Group on the management of partial ACL injuries. Although fairly common, these injuries are complex in nature with a heterogeneous definition and unclear guidelines on management. 23 Thus, these patients require a nuanced and individualized approach. 6 The goal of the survey was to assess the opinion of an international cohort of world experts to provide some clarity on this treatment. It was found that most members would opt for nonsurgical management of partial ACL injuries. When managing nonoperatively, the majority did not brace or restrict weightbearing. Many respondents used multiple parameters to determine RTS, with functional performance testing being the most popular, and the majority not allowing the athlete to RTS for ≥3 months postinjury.
Few respondents primarily managed stable partial ACL injuries with surgery. A total of 5.4% of current surgical members indicated surgery as their leading treatment. This is in line with how the literature on nonoperative management of partial ACL injuries which have shown generally good outcomes.1,2,4,9,16,17,20,21 There are some studies that imply partial ACL tears are at high risk of progressing to complete tears, especially in young active populations. 7 Fayard et al 7 reported a 39% progression rate at a mean 43 months in those with “delayed but firm endpoint” with Lachman. Similarly, there are reports of RTS as low as 30%. 1 It must be noted that there are great methodological differences in these studies. For instance, Bak et al defined the diagnosis as “macroscopically incomplete tear[s] involving up to 75% of the ligament with the remaining fibers sustaining tension on probe testing.” 1 It may be that the respondents’ criteria for partial ACL diagnoses involved more strict parameters such as stable Lachman, negative pivot shift, and relatedly, no bony bruising on MRI to select proper cases to manage nonoperatively. It is important to weigh all data available when deciding if patients are at an acceptably low risk of progression to full tear such that the benefits of rehabilitation and quicker return to play outweigh the expected risk of failure requiring surgery and lengthy postoperative recovery. There is a lack of basic science research or clinical studies to determine the true risk of progression to a complete tear. In scenarios when risk is considered greater than in our presented case, especially with regard to laxity on examination, some surgeons may have opted for more aggressive management with surgery. Ultimately, in the appropriate patients, the overwhelming majority of ACL Study Group active surgeon respondents indicated they would manage partial ACL tears nonoperatively.
The majority (75%) of respondents indicated they would not limit weightbearing when managed nonoperatively. Similarly, 59% of those surveyed would opt not to use a knee brace when managing nonoperatively. Once again, there is no consensus on the proper rehabilitation protocol for nonoperative management. Many of the historical studies even initially immobilized the knee in a splint or cast.1,8,9,12,13,15,17,21 When compared with studies using more liberal protocols, retear rates and RTS are similar.2,7,14,18 This is similar to how postoperative bracing and restricted weightbearing does not appear to offer improved benefits in patients after isolated ACL reconstruction. 10 There do not seem to be convincing data implying weightbearing limitations or restrictive bracing as a requirement to optimize outcomes, and this is reflected in the survey outcomes.
There were several different modalities chosen to determine RTS. Most respondents selected functional (87%); however, time from injury (40%), differential laxity (33%), and MRI (26%) were also utilized. This is similar to proposed rehabilitation protocols that rely on multiple metrics. For example, Sonnery-Cottet and Colombet 22 followed a protocol in patients with differential laxity that involved waiting 3 months and assessing knee laxity at that time. In this study, a majority of ACL Study Group active members (56%) selected RTS timelines of 3 months and 22% selected 4-6 months. Only 6.7% selected <6 weeks. Once again, this is similar to the timelines reported in literature, with many studies waiting for ≥3 months before allowing return to play.7,12,14,15,17 Fritchy et al 8 employed one of the more aggressive nonoperative protocols, with splinting until weeks 4 to 6 and RTS at 2 months and experienced one of the highest persistent instability rates at nearly 42%. It should be noted, however, that 15 of the 18 knees that eventually suffered a complete rupture had an estimated 50% to 75% ACL rupture. Of the 25% to 50% tear group, only 3 of 17 (18%) were found to have converted to complete rupture. Considering this, 3 months may be on the more conservative end of the spectrum for functional partial ACL injuries; however, there are otherwise no comparative studies to guide the timeline. Reliance on functional testing to determine RTS is consistent with the literature on RTS after ACL reconstruction, showing improved RTS and lower reinjury in those who passed functional performance testing. 10
Limitations
There are some limitations to the study. First, the survey exclusively polls the opinions of the ACL Study Group. This may not be representative of the orthopaedic surgery community as a whole. For example, only 4 surgeons were female and the majority were from North America or Europe. However, when comparing responses between demographic location and type of institution, the primary differences were duration of bracing and type of operative intervention. Thought processes on partial ACL tears without instability seemed fairly similar overall. Considering the scholarly rigor by which these individuals were elected members of this exclusive society, who by all accounts are considered experts in ACL injuries, this should be deemed an appropriate cohort to provide expert opinion. Second, while the survey was designed to be clear and unbiased, it may not perfectly extract respondent opinions. While web-based branching logic questionnaires have been validated, this particular survey has not yet been validated. 11 These questions were developed in an iterative process by multiple surgeons to help reduce the interpretive variability that may occur with nonvalidated questionnaires. To address this, questions were made to be closed-ended and unambiguous. Perhaps an open face-to-face discussion would better facilitate member opinions, but this would not be as logistically feasible. Additionally, an online survey has the benefit of blinding participants to the responses of others. There is also the possibility of nonresponse bias, which is inherent in disseminated survey studies. However, it should be noted that the 84% response rate of active surgical members was well within various accepted rates for published survey results, with participation ranging from 60% to 80%. 19 Moreover, the typical impact of socioeconomic status may be lessened in this cohort of physicians. 3
Conclusion
This study presented the results of a survey on partial ACL injury management administered to ACL Study Group active surgical members. These findings offer aggregated expert opinion on this difficult pathology. Multiple management plans and RTS algorithms were endorsed. Treatment should be customized to the patient. Insights from this study may provide guidance for practitioners encountering partial ACL tears in clinical practice and contribute to the international discourse regarding partial ACL injuries.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241311603 – Supplemental material for Management of Isolated Partial ACL Tears: A Survey of International ACL Surgeons
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241311603 for Management of Isolated Partial ACL Tears: A Survey of International ACL Surgeons by Christopher S. Frey, Kinsley J. Pierre, Nicole S. Pham, Geoffrey D. Abrams, Seth L. Sherman, Tim Spalding and Marc R. Safran in The Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted July 25, 2024; accepted August 30, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.F. has received education payments from Evolution Surgical. G.A. has received hospitality payments from Evolution Surgical, consulting fees from Evolution Surgical and Bioventus, and education payments from Evolution Surgical. S.L.S. has received nonconsulting fees from Arthrex, Smith & Nephew, Synthes GmbH, and Vericel; consulting fees from Flexion Therapeutics, Olympus America, LifeNet Health, Medical Device Business Services, Bioventus, DJO, Kinamed, Linvatec, Smith & Nephew, Vericel, Biorez, JRF Ortho, DePuy Synthes Products, and Pacira Pharmaceuticals; royalties from Linvatec and CONMED Corporation; hospitality payments from OSSIO and Aesculap Biologics; education payments from Evolution Surgical; and honoraria from Pacira Pharmaceuticals, Flexion Therapeutics, JRF Ortho, and Vericel. M.R.S. has received royalties from Medacta USA and Smith & Nephew, consulting fees from Smith & Nephew, and nonconsulting fees from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.