
Abstract
Background:
It remains unknown whether anterior cruciate ligament (ACL) reconstruction (ACLR) alters the natural history of degenerative changes or prevents further injury compared with nonoperative treatment.
Purpose/Hypothesis:
The purpose of this study was to evaluate the midterm risk of knee surgery in patients who sustained an ACL tear treated with initial nonoperative management. It was hypothesized that the majority of patients who pursue initial nonoperative treatment after ACL rupture will not undergo further surgery within 5 years.
Study Design:
Case series; Level of evidence, 4.
Methods:
An electronic health record search was performed for all patients aged 12 to 65 years from 2011 to 2012 with magnetic resonance imaging–confirmed ACL tear. Patients who did not undergo ACLR within 6 months after diagnosis comprised our initial cohort. Patients were longitudinally followed until August 31, 2017. The primary outcome was an occurrence of ipsilateral knee surgery, including ACLR and non-ACLR procedures.
Results:
A total of 932 patients with a mean age of 36.2 ± 13.6 years were included. The mean follow-up time was 57.9 ± 7.4 months. During the follow-up period, 365 patients (39.2%) had ipsilateral knee surgery, with a mean time from ACL tear diagnosis to the first procedure of 11.9 ± 13.0 months. Overall, 67% of surgeries occurred within 12 months of diagnosis. ACLR was performed in 211 patients (22.6%); 284 patients had non-ACLR knee procedures, with 130 undergoing ACLR and non-ACLR surgery and 154 patients undergoing non-ACLR procedures alone. After adjusting for demographic and clinical factors, younger age remained a significant risk factor for undergoing ACLR: patients aged 12 to 18 years and those aged 19 to 30 years had similar adjusted hazard ratios compared with patients aged 51 to 65 years (5.49 [95% CI, 2.78-10.88] and 5.48 [95% CI, 2.85-10.53], respectively; P < .001 for both).
Conclusion:
In this universally insured, contained patient cohort, 39.2% of the patients underwent a subsequent surgical procedure on the ipsilateral knee within 5 years of ACL injury, with 22.6% of patients opting to undergo delayed ACLR. Younger age was an independent risk factor for undergoing ACLR.
There has been a rise in the diagnosis of anterior cruciate ligament (ACL) injury and treatment with ACL reconstruction (ACLR) in both adult and pediatric populations over the past 2 decades.27,43 Biomechanical studies have shown the ACL to be the primary stabilizer to anterior translation of the tibia relative to the femur along with its role in resisting internal/external rotation.21,44 The natural history of the ACL-deficient knee is not well understood. The common consensus is that without a functional ACL, the knee joint is subjected to functional instability that may lead to long-term complications such as meniscal injuries,1,44 failure of secondary stabilizers, and early-onset osteoarthritis. 25
With current knowledge, it is unclear whether all ACL-deficient patients require reconstruction. Noyes and McGinniss 30 postulated that ACL-deficient patients fall into 3 categories: (1) copers, (2) adapters, and (3) noncopers. One-third of patients were copers who could function without an ACL; one-third were adapters who adjusted their sports to more straight-line activities; and one-third were noncopers who continued to experience instability even after appropriate rehabilitation. The rationale for surgical treatment assumes that the ACL is crucial for knee function and that surgical reconstruction prevents further intra-articular damage. The rationale for nonsurgical treatment assumes that the ACL-deficient knee may function reasonably well under certain circumstances and that reconstructions do not preclude further damage. Additionally, it is not clear if surgery provides superior outcomes in certain patient populations.
There are inherent challenges to the study of nonoperative management of ACL tears. Small, nonrandomized studies have shown good outcomes in athletes following nonoperative treatment,12,15 equivalent short- to midterm outcomes between patients who selected nonoperative treatment to those who selected reconstruction,6,20 and satisfactory long-term subjective outcomes despite radiographic degenerative changes. 19 Randomized trials comparing nonoperative versus operative treatments face challenges in randomization and recruitment.9,24,28 The most recent Cochrane review article in 2016 28 only identified 1 randomized trial 10 with low-quality evidence. In that trial, patients were randomized into early ACLR or optional delayed ACLR: 51% of optional delayed ACLR patients eventually had an ACLR with no significant differences in outcome at 5 years in the intention-to-treat analysis.
While primary ACLR provides increased stability to the knee and helps patients return to sports and activity, 26 studies have not demonstrated a benefit with regard to the development of arthritis.4,39,40 Subsequent meniscal damage 17 and subsequent surgery 16 are common after ACLR in prospective studies. Additionally, longitudinal studies examining return to sport following ACLR have shown that one-third to one-half of patients are not able to return to preinjury level of participation.2,23 While ACLR is typically recommended in the younger patient population and initial nonoperative treatment is recommended in older patients, a dilemma occurs with ACL tears in middle-aged patients.37,45
The purpose of this study was to evaluate the midterm risk of ipsilateral knee surgery of patients who sustained an ACL tear treated with initial nonoperative management. We hypothesized that the majority of patients who pursue initial nonoperative treatment after ACL rupture will not undergo further surgery within 5 years.
Methods
The protocol for this observational data–only study received institutional review board approval, with a waiver of consent. We performed an electronic health record (EHR) search for all patients aged 12 to 65 years with a new diagnosis of magnetic resonance imaging (MRI)–confirmed ACL tear (identified using International Classification of Diseases, Ninth Revision, Clinical Modification diagnosis code 844.2) in the Kaiser Permanente Northern California health care system from 2007 to 2012. Patients whose initial diagnosis was prior to 2011 were then excluded, to eliminate patients who tore their ACL prior to the study period. The final population included patients with initial diagnosis of ACL tear in 2011 or 2012. The population included is part of an integrated community health care system with a universally insured patient population, which reflects the demographics of the general population in the region. A visual illustration of the study cohort selection is shown in Figure 1. To ensure cohort identification accuracy, the principal study investigator (D.Y.D.) conducted a structured EHR review on a random sample of 5% of the patients. Patients were identified who had a listed diagnosis of ACL rupture. The EHR was then searched for an MRI of the knee from 60 days before to 60 days after the coded diagnosis to confirm the ACL rupture diagnosis and laterality. Using the date of ACL tear diagnosis, patients who did not elect to undergo ACLR in ≤6 months comprised our initial cohort. We chose 6 months as an arbitrary cutoff, as 90.5% of patients in our system who underwent ACLR in ≤2 years after diagnosis did so in ≤6 months (Figure 2). Nonoperative treatment consisted of offering the patients physical therapy. Patients were excluded if they were not within the health care system for ≥1 year leading up to and 2 years after the diagnosis date. Patients were longitudinally followed through our health system until August 31, 2017, with censoring at death or health care membership disenrollment.
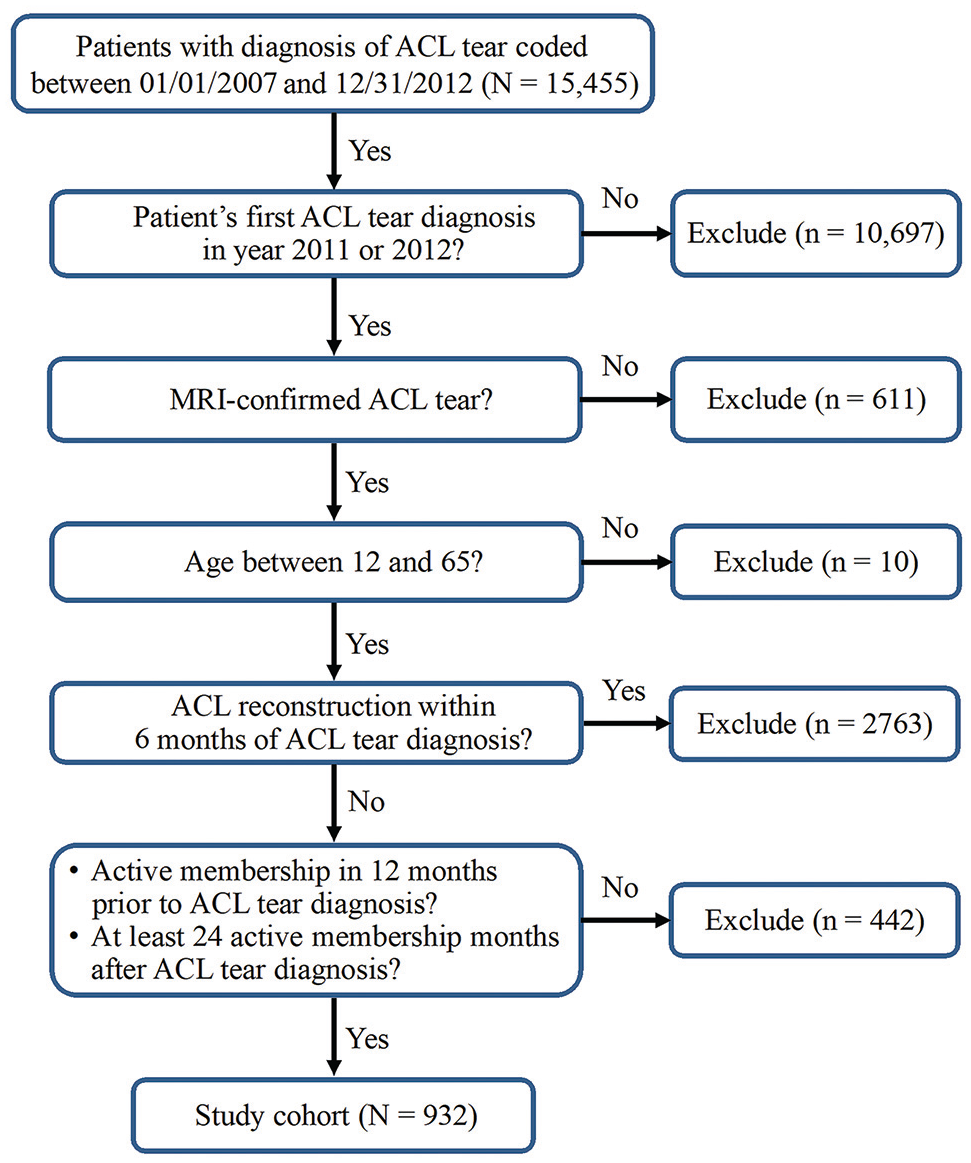
Diagram showing enrollment procedure of the study cohort. ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.

Percentage of patients with magnetic resonance imaging–confirmed anterior cruciate ligament (ACL) tear who underwent ACL reconstruction within 2 years according to time from initial ACL tear diagnosis.
Other patient demographics included sex and race/ethnicity (Asian, Black, Hispanic, White, other), and clinical characteristics consisted of body mass index (BMI), Charlson Comorbidity Index score, and smoking status (current smoker or not). BMI value and smoking status closest to the ACL tear diagnosis and up to 1 year prior were utilized. Operative procedures of the same and opposite knee during follow-up (hereafter termed “subsequent knee surgery”) up to 5 years were the primary and secondary outcomes of interest, respectively. The Concurrent Procedural Terminology (CPT) codes were used to identify these knee surgeries including ACLR (CPT 29888), meniscal repair (CPT 27403, 29882, 29883), meniscal transplant (CPT 29868), meniscectomy or meniscal debridement (CPT 27332, 27347, 29880, 29881), microfracture or chondroplasty (CPT 29879, 29877), cartilage transplant (CPT 29866, 29867), and other (CPT 27447). All variables were abstracted from the Kaiser Permanente Northern California EHR, and time from index ACL tear diagnosis to each outcome was calculated.
Statistical analyses were performed using SAS software Version 9.4 (SAS) with significance threshold set at 2-sided P < .05. The rate of each outcome was calculated for (1) the overall cohort, (2) those with any ipsilateral knee surgery, and (3) those who subsequently underwent ACLR. Time from ACL tear diagnosis to the first primary outcome, as well as total follow-up time, was calculated for each patient. Descriptive statistics of patient characteristics were calculated and expressed as frequencies with proportions or means with standard deviations. Kaplan-Meier survival analyses were performed for cumulative risk of undergoing ipsilateral ACLR during follow-up period. These analyses were stratified by age and BMI groups and compared using the log-rank method. Before fitting the multivariable regression analysis (Cox proportional hazards modeling), we performed unadjusted analyses to evaluate the association of each risk factor of interest with outcomes of interest (any ACLR and any ipsilateral knee surgery). Risk factors of interest included age at diagnosis, sex, race/ethnicity, BMI, Charlson Comorbidity Index, smoking status, and prior ipsilateral non-ACLR surgery (only applicable to ACLR patients). None of the risk factors showed significant results in the unadjusted analyses for non-ACLR surgery; therefore, the multivariable regression analysis was limited to ipsilateral ACLR.
Results
Patient Characteristics
A total of 932 patients with nonoperatively managed ACL tears diagnosed between 2011 and 2012 met the study inclusion criteria. The mean age of the cohort was 36.2 ± 13.6 years, with 41% of patients >40 years (Table 1). Most patients were male (63.3%) and identified as White (50%). The most common BMI cohorts were overweight (32.4%) and normal (25.1%); 32% of the patients had a BMI >30. Overall, 87.6% of patients had no comorbidity conditions, and 10.1% were current smokers. The mean follow-up time was 57.9 ± 7.4 months.
Characteristics of the Study Patients (N = 932) a

Data are presented as n (%) unless otherwise indicated. ACL, anterior cruciate ligament; BMI, body mass index.
Within 1 year before ACL tear diagnosis through diagnosis; if >1 entry was found in the electronic health record, the one closest to the ACL tear diagnosis was used.
Subsequent Knee Surgery
During the follow-up period, 365 patients (39.2%) underwent ipsilateral knee surgery (Table 2). Mean time from ACL injury diagnosis to the first knee surgery was 11.9 ± 13.0 months (Figure 3A). Two-thirds of ipsilateral surgeries were ≤12 months after diagnosis. Subsequent ipsilateral ACLR was performed in 211 patients (22.6%), and 55.9% (118/211) had concomitant surgeries including meniscal debridement (46%), meniscal repair (18.5%), and microfracture/chondroplasty (4.7%). In patients who had ACLR, 48.3% had reconstruction between 6 and 12 months from diagnosis (Figure 3B). Undergoing multiple ACLR of the same knee or ACLR of the opposite knee during the follow-up period were rare (0.5% and 1.6%, respectively) (Table 2).
Knee Surgeries in ≤5 Years in Patients Treated Nonoperatively for ≥6 Months After ACL Tear Diagnosis (N = 932) a

Data are presented as n (%). ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
Denominator is any ipsilateral ACLR.
Defined as undergoing any non-ACLR knee procedure before ACLR.
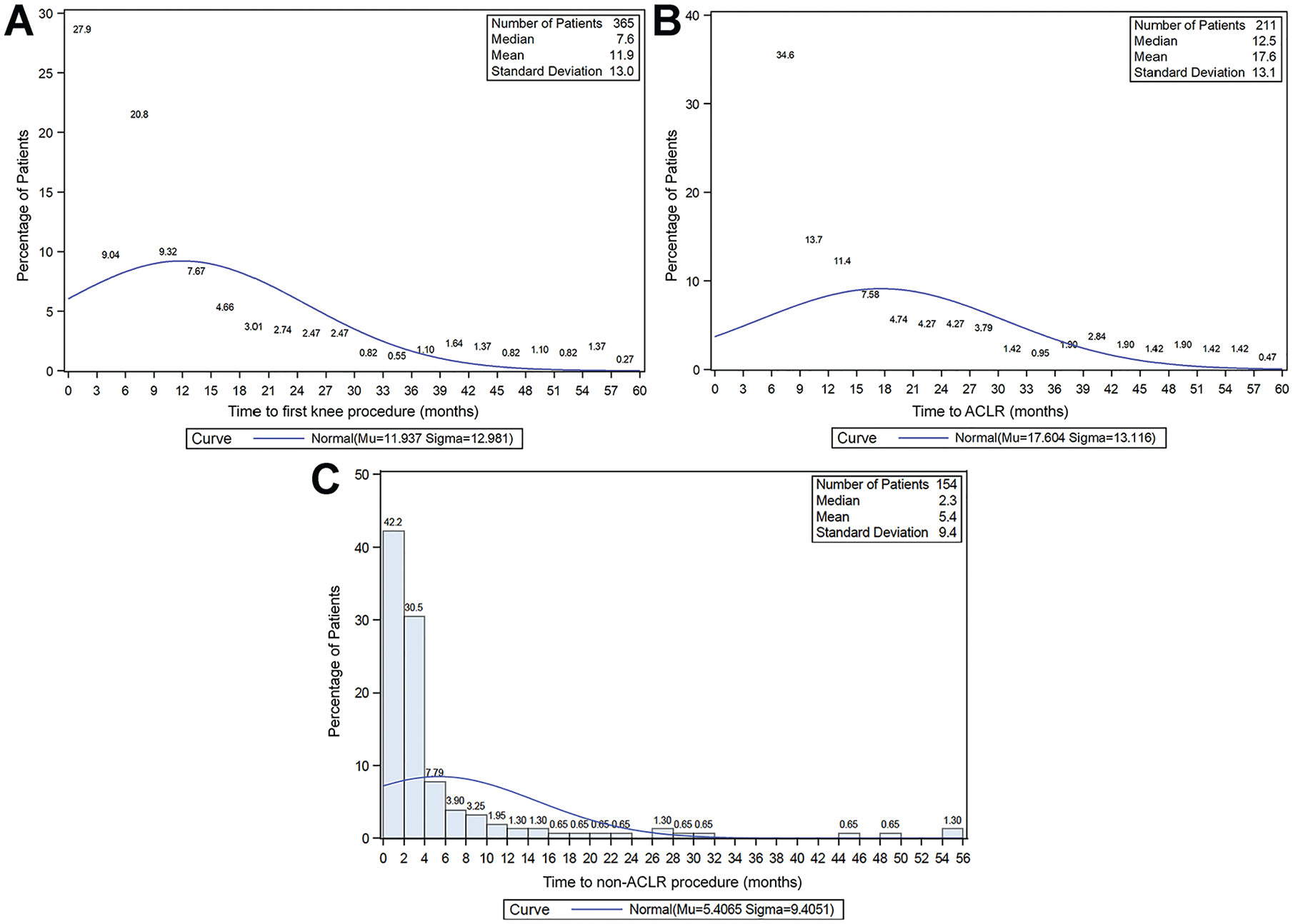
Percentage of study patients who underwent surgery on the ipsilateral knee according to time from initial anterior cruciate ligament (ACL) tear to (A) first knee procedure, (B) ACL reconstruction (ACLR), and (C) any non-ACLR knee procedure.
As shown in Table 2, 30.5% of patients (n = 284) received ipsilateral non-ACLR knee surgery, with a mean time from diagnosis to surgery of 10.7 ± 12.7 months. This included 130 patients who underwent ACLR at some point during the follow-up period and 154 patients who did not undergo ACLR during the follow-up period. Of these 284 patients, 47.5% (n = 135) had surgery ≤6 months following ACL tear diagnosis (Figure 3C) and 15 patients had ipsilateral knee surgery before ACLR (Table 2). The most common non-ACLR procedures performed were meniscectomy/meniscal debridement (n = 232; 24.9%), meniscal repair (n = 75; 8.0%), and microfracture/chondroplasty (n = 36; 3.9%). In patients who did not undergo ACLR (n = 154) the most common procedures were meniscectomy/meniscal debridement (n = 125) and meniscal repair (n = 29).
Risk Factors for ACLR
Figure 4 shows the cumulative risks of undergoing ACLR over the 5-year study period, stratified by age and BMI at diagnosis. In the unadjusted analysis (Table 3), compared with patients aged 51 to 65 years, younger age was predictive for undergoing ACLR; this was most pronounced for patients aged 19 to 30 years (hazard ratio [HR], 5.21; 95% CI, 2.74-9.88) and 12 to 18 years (HR, 4.66; 95% CI, 2.41-9.05). Normal or overweight BMI categories were significant risk factors for undergoing ACLR when compared with morbidly obese patients (normal: HR, 2.24 [95% CI, 1.30-3.86]; overweight: HR, 1.85 [95% CI, 1.08-3.18]). After adjusting for other risk factors, age group remained predictive of undergoing ACLR: patients aged 12 to 18 years and those aged 19 to 30 years had similar adjusted HRs compared with patients aged 51 to 65 years (5.49 [95% CI, 2.78-10.88] and 5.48 [95% CI, 2.85-10.53], respectively; P < .001 for both) (Table 3). However, BMI was no longer a significant risk factor for ACLR. Undergoing non-ACLR procedures before ACLR was a significant risk factor in both the unadjusted and the adjusted analyses (HR, 8.33 [95% CI, 4.91-14.14], adjusted HR, 7.56 [95% CI, 4.30-13.28]) (Table 3).

Cumulative risk of anterior cruciate ligament (ACL) reconstruction (ACLR) on the ipsilateral knee after ACL tear diagnosis in patients initially managed nonoperatively. (A) Risk stratified by age group (12-18, 19-30, 31-40, 41-50, 51-65 years). (B) Risk stratified by body mass index (BMI) group (18.5-24.9, 25-29.9, 30-34.9, ≥35.0).
Risk Factors Associated With Undergoing Ipsilateral ACL Reconstruction in Patients Treated Nonoperatively for ≥6 Months After ACL Tear Diagnosis a

Dashes indicate areas not applicable. Boldface P values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; HR, hazard ratio.
Adjustment estimated using Cox proportional hazard model for ACLR on the ipsilateral knee, controlling for all risk factors included in the table.
Defined as undergoing any non-ACLR knee procedures before ACLR.
Discussion
Though the yearly number of patients undergoing ACLR in the United States is on the rise,27,43 many patients choose nonoperative management after initial injury. A major challenge in assessing outcomes after ACL tear is the lack of follow-up of nonoperatively managed patients. By using a universally insured patient cohort with adequate follow-up, we were able to evaluate the effects of initial nonoperative management on acute ACL tears with regard to subsequent knee surgery. In this retrospective study, such patients who did not undergo ACLR within 6 months of MRI-confirmed diagnosis were followed for 5 years for the occurrence of surgical intervention on the ipsilateral and contralateral knees. Within the 5-year follow-up period, 39.2% of patients had ipsilateral knee surgery, including 22.6% who ultimately underwent ACLR. Additionally, we found that younger patients were most likely to undergo reconstruction.
The true incidence of operative and nonoperative treatment of ACL tears in the US population is unknown. A national study using Iceland's social insurance data from 2006 to 2012 found that only about half of patients with an identified ACL tear underwent ACLR, though their follow-up period was not reported. 29 In a geographic database study in the United States examining >500,000 patient records from 1991 to 2005, a total of 1398 patients with ACL tear were identified, and 16% were treated nonoperatively. 13 While the rate of ACLR in the US population is increasing,14,27 it is unknown whether the rate of nonoperative treatment is decreasing. Further population-based studies are needed to determine the true incidence of nonoperative treatment in the United States.
During the 5 years after initial nonoperative treatment in our study, 39.2% of patients underwent ipsilateral knee surgery. A systematic review pooling ≥10-year follow-up data on operatively and nonoperatively managed ACL tear patients found that nonoperatively managed patients were twice as likely to undergo ipsilateral knee surgery (24.9% vs 12.4%). 4 In comparing with an operatively managed cohort, a study from the Multicenter Orthopaedic Outcomes Network 16 demonstrated prospectively that 18.9% of ACLR patients undergo ipsilateral surgical intervention within 6 years. Frobell et al10,11 performed a randomized controlled trial of 121 adults in Sweden with ACL tears, comparing early ACLR to rehabilitation with optional delayed reconstruction. Of the initial nonoperative arm, 38% of patients underwent delayed reconstruction within 2 years and 51% underwent delayed reconstruction within 5 years. While patients treated in the optional delayed reconstruction group had greater knee laxity at 2 and 5 years, there were no differences in patient-reported outcomes or return to preinjury level of activity at 2 years 10 and no differences in meniscal surgery or radiographic osteoarthritis at 5 years. 11 In our study, of the 211 patients who elected for delayed reconstruction, about half underwent ACLR between 6 and 12 months from diagnosis and another quarter had surgery between 1 and 2 years. We conclude that patients who initially select nonoperative treatment yet then cross over to surgical management usually do so within 2 years of diagnosis.
The literature is mixed as to the effect on meniscal and cartilaginous health in the setting of early versus delayed ACLR. An increase in secondary meniscal tears has been shown in some retrospective studies3,13,32 whereas others have shown no difference.8,11 After an untreated ACL tear, Levy and Meier 22 showed that the incidence of meniscal tears is 40% at 1 year and 60% at 5 years after injury. In the current study, most non-ACLR procedures were performed ≤18 months after ACL tear diagnosis. The majority of surgeries addressed the meniscus, with a quarter of patients undergoing meniscal debridement and 8% undergoing repair. About half of patients who had delayed ACLR also had meniscal surgery, whereas over 80% of patients who had a non-ACL surgery were having surgery of the meniscus. The literature remains mixed with regard to the risks and benefits of meniscal surgery, particularly partial meniscectomy.5,18,31,34,35 Randomized clinical trials of surgery for degenerative tears have failed to show the benefit of arthroscopy over nonoperative treatments.5,18,34,35 At least 1 study has suggested that partial meniscectomy may increase the chance of osteoarthritis as early as 5 years postoperatively. 33 The true cost of nonoperative treatment of ACL injury may, therefore, be underestimated without considering the risks of partial meniscectomy without reconstruction. Cartilage procedures were substantially less common in this midterm follow-up period, performed in just 4% of patients. Therefore, the rates of surgical intervention were not as high as the rates of injury published by Levy and Meier, though they do affect a large subset of patients. One limitation of the current study is the inability to differentiate between primary meniscal injuries (occurring with the ACL injury) and secondary meniscal tears that occurred during the period of ACL deficiency.
In the unadjusted analysis, risk factors for undergoing surgery in the 5 years after ACL tear in this cohort included younger age, lower BMI, and non-ACLR surgery before ACLR. Younger patients are more likely to place higher demands on their knee,36,42 and return to sport may be hampered by continued instability. In an observational database study of 1398 patients undergoing early reconstruction, delayed reconstruction, and rehabilitation only for ACL tear, the age for patients undergoing nonoperative treatment was significantly higher than the mean ages for those undergoing early or delayed reconstruction. 13 With regard to BMI, a higher BMI has been associated with increased risk of subsequent knee surgery in the reconstruction population36,38 and increased risk of meniscal and chondral injury at the time of ACL injury.3,41 On the other hand, elevated BMI has been associated with lower physical activity levels.7,46 In this study, while unadjusted analysis showed lower BMI to be correlated with undergoing delayed ACLR, the adjusted analysis showed no statistical association. The initial correlation is likely explained by the age distribution of patients in the lower and higher BMI groups, with lower BMI patients more likely to be younger. There are no data in the literature that examine the role of BMI on subsequent surgery in nonoperatively treated patients, and these findings highlight the need for further study.
Of patients in this study who initially selected nonoperative treatment, 60.8% had no subsequent knee surgeries within 5 years following ACL tear. It is possible that these patients represent “copers” (those who function well with ACL deficiency) or “adapters” (those who change activities due to ACL deficiency and maintain a satisfactory lifestyle). Predicting which patients will have an acceptable outcome following nonoperative treatment is an attractive goal for orthopaedic surgeons hoping to accurately counsel patients. In this study, patients who were older (especially those >50 years) and had a higher BMI (especially the morbidly obese) were least likely to have subsequent surgery. There was no significant effect of sex, race, or Charlson Comorbidity Index with regard to undergoing subsequent ACLR. Consideration of the patient's individual circumstances is prudent, with attention to age and activity level.
Limitations
While this study represents the largest published cohort of nonoperatively treated patients with ACL tear, it has several limitations. The findings are generalizable to the patient population studied, which includes insured patients from 12 to 65 years old; bias exists regarding which patients were included in this study—namely, older patients who were likely lower demand. Being retrospective in nature, there was no opportunity for intervention. Furthermore, no patient-reported outcomes were collected. In this pragmatic design, it is unknown what percentage of patients attended physical therapy, and the physical therapy protocols were not standardized. While a key strength is that the health care system has high retention, there is theoretically a possibility of crossover to surgical intervention in a different health care system. Despite these limitations, this study aids physicians in counseling patients who are considering nonoperative treatment options for ACL tear as to the risk for conversion to surgical management.
Conclusion
In this retrospective observational study, 22.6% of patients who underwent nonoperative management for the first 6 months after a diagnosed ACL tear elected to have delayed ACLR within 5 years, with the majority occurring within 2 years of diagnosis. In all, 39.2% of patients underwent an ipsilateral knee procedure during the 5 years after ACL injury. Younger age was found to be an independent risk factor for crossing over to reconstruction, which is likely related to increased activity demands. Given the mixed literature on nonoperatively treated patients with ACL deficiency, future studies should focus on comparing these patients with operatively managed patients for subsequent injury and patient-reported outcomes.
Footnotes
Final revision submitted July 29, 2024; accepted August 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a grant from the Kaiser Permanente Community Benefit Program (grant No. RNG209454). C.M.R. has received grant support from Arthrex and education payments from Arthrex and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kaiser Permanente Northern California (reference No. 00001045).