
Abstract
Background:
Reduced quadriceps strength influences knee function and increases the risk of knee osteoarthritis. Thus, it is of significant clinical relevance to precisely quantify strength deficits in patients with knee injuries.
Purpose:
To evaluate isokinetic concentric quadriceps muscle strength torque values, assessed both from peak torque and at specific knee flexion joint angles, in patients with anterior cruciate ligament (ACL) injury, focal cartilage lesions, and degenerative meniscus tears.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were synthesized from patients included in 3 previously conducted research projects: 2 prospective cohort studies and 1 randomized controlled trial. At the time of inclusion, all patients were candidates for surgery. Isokinetic concentric quadriceps muscle strength measurements (60 deg/s) were performed at baseline (preoperative status) and after a period of progressive supervised exercise therapy (length of rehabilitation period: 5 weeks for ACL injury, 12 weeks for cartilage lesions and degenerative meniscus). Outcome measures were peak torque and torque at specific knee flexion joint angles from 20° to 70°. All patients had unilateral injuries, and side-to-side deficits were calculated. For comparisons between and within groups, we utilized 1-way analysis of variance and paired t tests, respectively.
Results:
In total, 250 patients were included. At baseline, cartilage patients had the most severe deficit (39.7% ± 24.3%; P < .001). Corresponding numbers for ACL and degenerative meniscus subjects were 21.7% (±13.2%) and 20.7% (±16.3%), respectively. At retest, there was significant improvement in all groups (P < .001), with remaining deficits of 24.7% (±18.5%) for cartilage, 16.8% (±13.9%) for ACL, and 3.3% (±17.8%) for degenerative meniscus. Peak torque was consistently measured at 60° of knee flexion, whereas the largest mean deficits were measured at 30° at baseline and 70° at retest for the ACL group, at 70° at baseline and retest for the degenerative meniscus group, and at 60° at baseline and at 50° at retest for the cartilage group.
Conclusion:
This study underlines the importance of including torque at specific knee flexion joint angles from isokinetic assessments to identify the most severe quadriceps muscle strength deficits. Furthermore, it confirms the importance of progressive exercise therapy interventions before potential surgery in patients with knee injuries.
Quadriceps muscle strength deficits are common both after acute knee injury and in degenerative knee joint diseases. 28 Loss of quadriceps muscle strength may contribute to reduced knee joint stability, fatigue, and a diminished ability to adequately dampen impact forces and evenly distribute load on the joint surface during different weightbearing activities. 22,24,36,37 These implications may prevent individuals from participating at their desired level of sports and leisure activities in the short term, 27 and in the long term, play a role in future development of knee osteoarthritis (OA). For patients with a reconstructed anterior cruciate ligament (ACL), quadriceps muscle strength deficits have been shown to negatively influence both self-reported function 7 and the ability to return to sport (RTS). 21 Furthermore, Grindem et al 15 found more symmetrical quadriceps strength prior to RTS to significantly reduce the knee reinjury rate the 2 first years after ACL reconstruction. A recent meta-analysis 26 identified decreased quadriceps muscle strength (assessed from peak torque [PT] in 4 and total work [TW] in 1 of the 5 studies included in the study) as a risk factor for later development of knee OA, both in the form of posttraumatic OA after an injury to the ACL and for primary knee OA. In older females, quadriceps muscle strength has even been shown to be significantly associated with independent living skills. 19 Monitoring of quadriceps muscle strength during exercise therapy and rehabilitation in patients with knee pain or knee injuries is therefore of utmost importance, both from a short- and a long-term perspective.
Quadriceps strength deficits in patients with knee injuries are usually quantified by comparing the strength of the injured leg to the uninjured. The gold standard for assessment of quadriceps muscle strength is isokinetic concentric dynamometry, with PT as the most established outcome measure. 6,13 PT is defined as the greatest observed force during the set movement cycle of the knee joint. Previous data from our research group have shown that PT occurs between 50° and 70° of knee flexion. 6 Thus, assessment of PT alone will provide information about the strength level only at the 1 point during the movement cycle where the greatest torque occurs. Deficits at other knee joint angles will not be identified. Consequently, it may be hypothesized that assessing PT alone may be insufficient to identify both the magnitude and localization of the most severe quadriceps deficit, unless we take for granted that the most severe deficits occur at PT.
In a previous study by our group, 6 we investigated angle-specific quadriceps muscle strength comparing differences between the injured and uninjured limbs in patients with a recent unilateral ACL injury. When plotting curves for strength values at specific knee joint flexion angles from 15° to 80°, we found that these patients exhibited the largest deficits at 20° rather than at PT. These findings suggested that assessment of PT alone concealed the largest deficits in this patient group. As interlimb muscular strength symmetry is often included in screening tools and RTS testing protocols, this may have interesting clinical implications both for patients with ACL injuries and other knee injuries. Muscle strength assessments are utilized to monitor progress during rehabilitation and may thus influence both treatment decisions (nonoperative management or surgery and timing of potential surgery) and the recommendations we give to our patients regarding activity and sports participation. For example, the established cutoff for passing RTS criteria is ≥90% strength on the injured side compared with the uninjured. 15 But, can we state that our patients have passed this criterion if the symmetry index is <90% elsewhere during the movement cycle?
A substantial amount of previous research on quadriceps muscle strength in patients with knee injuries has involved those with ACL injury and/or ACL reconstruction. However, we do know that quadriceps muscle strength deficits pose a challenge in patients with other types of knee injuries. Still, to our knowledge, no study has investigated angle-specific quadriceps muscle strength patterns in any other patient group than the ACL.
Over the past 10 years, the Norwegian Research Centre for Active Rehabilitation (NAR) has conducted 3 different prospective studies in collaboration with other international research centers 8,34,38 involving patients with acute ACL ruptures, focal cartilage lesions, and degenerative meniscal tears. In all 3 cohorts, isokinetic quadriceps muscle strength has been included as an outcome measure before and after accomplishment of a progressive exercise therapy program. The synthesized material from these 3 cohorts now enables us to compare the angle-specific quadriceps muscle strength curve patterns at baseline and after rehabilitation in all 3 patient groups. We do not know whether the largest deficits at baseline occur at PT or other knee angles in patients with focal cartilage lesions or degenerative meniscus injuries. Furthermore, we do not know whether potentially severe strength deficits manifesting elsewhere than at PT are persistent or to what extent they may be altered after a period of structured exercise therapy. This is also unknown for patients with an ACL injury. We believe identification of both angle-specific localization and magnitude of strength deficits bear clinical interest, as it may help us customize targeted rehabilitation programs and assist us in treatment decision making for all patient groups.
This study addresses the following research questions: (1) Are there differences in PT quadriceps muscle strength between patients with ACL rupture, focal cartilage lesions, and degenerative meniscal injuries? (2) Are there angle-specific differences in the isokinetic quadriceps muscle strength curve pattern between patients with ACL rupture, focal cartilage lesions, and degenerative meniscal injuries? (3) Can quadriceps muscle strength torque values and, consequently, muscle strength deficits both at PT and other specific knee joint angles throughout the curve change for each patient group after performing a progressive exercise therapy program? It should be emphasized that this study is not designed or intended to compare the efficacy of the 3 programs.
Methods
Subjects
The subjects included were originally recruited in 3 different studies: the Delaware-Oslo ACL study, 14 the Oslo Cartilage Active Rehabilitation and Education (CARE) study, 38 and the Odense Meniscus Exercise (OMEX) study. 34 Patients in all studies were included with unilateral injuries only. An overview of inclusion criteria and timeline for the 3 cohorts is given in Table 1. As shown, the time since injury for ACL patients and the duration of symptoms for the focal cartilage lesion and degenerative meniscus patients differ substantially. However, all subjects were recruited to their respective studies at a time point where they were referred to an orthopaedic surgeon and considered candidates for surgery.
Overview of Original Studies a

a ACL, anterior cruciate ligament; MRI, magnetic resonance imaging.
b The total number of patients included in the OMEX study was 150, but the patients randomized to surgery were not included in the present study.
c Reasons lost to follow-up: Delaware-Oslo ACL cohort study: unable to reach/did not respond, n = 2; swelling and unable to perform strength test, n = 2; loss of angle-specific data due to technical problems, n = 2. OMEX study: unable to reach/did not respond, n = 3; did not show at test day, n = 2; noncompliant to rehabilitation program n = 2. Oslo CARE study: withdrew from study, n = 3; did not show at test day, n = 1.
In our clinic, all patients with ACL injury, focal cartilage lesions, and degenerative meniscus tears are strongly encouraged to undergo structured rehabilitation before it is decided whether they should undergo surgery. All subjects were candidates for surgery (ACL reconstruction, cartilage repair, and arthroscopic partial meniscus resection surgery) at the time of inclusion; however, the final decision for surgery was different in the 3 cohorts. In the Delaware-Oslo ACL study, all included patients were obliged to complete a 5-week supervised exercise therapy program 8 prior to consideration of further surgical treatment (n = 150). In contrast to established practice in other countries, especially the United States, this was independent of whether they initially were classified as copers or noncopers. 30 The Oslo CARE study was analogous in that all included patients were committed to undergo a 12-week supervised exercise therapy program before the decision for surgery was made 38 (n = 48). Thus, the results presented for the ACL and cartilage patients reflect the quadriceps muscle strength status of the patients at baseline and after a period of structured rehabilitation, before the decision for surgery or continued nonoperative management was taken. The OMEX study was different as this was a randomized controlled trial where patients who were referred to an orthopaedic surgeon as candidates for surgery were allocated to either arthroscopic treatment or a nonoperative intervention in the form of a 12-week supervised exercise therapy program. 34 As the patients who were drawn to arthroscopic treatment underwent surgery immediately after randomization, only patients who were allocated to the 12-week supervised exercise therapy were included in this material (n = 69).
All data are based on preoperative assessments. However, within 2 years after the baseline test, 64.0% of included patients in the ACL cohort had undergone reconstruction. It is important to note that these patients did not necessarily have isolated ACL tears. At the time of surgery, 27.8% were diagnosed with either a meniscal or cartilage injury (19.2% medial meniscus, 8.0% lateral meniscus, 0.6% cartilage lesion).
In total, 267 patients from the 3 cohorts were eligible for inclusion in the present study (Table 1). All subjects provided written informed consent before inclusion. The studies were conducted in line with the Declaration of Helsinki and ethically approved by The National Committees for Research Ethics in Norway.
Exercise Therapy Interventions
All 3 supervised exercise programs utilized in the different cohorts have previously been presented in detail in 3 separate articles from our research group (Delaware-Oslo ACL, 8 Oslo CARE, 38 and OMEX 35 ). These articles provide descriptions of the included exercises, dosage, and repetition, as well as discussions of the feasibility of each program. We have therefore condensed the information on the programs to a general description of the overall content and purposes as well as highlighted differences between the programs that are of particular relevance for the present study.
All patients had undergone initial rehabilitation (acute phase rehabilitation for ACL patients) before inclusion in the study, implying that they had restored full range of motion and swelling was minimized. Common for all 3 exercise therapy programs was open- and closed-chain exercises to address knee and hip muscle strength and neuromuscular training in the form of balance and plyometric exercises. Furthermore, all patients received individual weekly supervision from a physical therapist who ensured continuous progression of load in strength exercises and level of difficulty in neuromuscular exercises. Adherence to the program as well as adverse events were registered in training diaries. There were no major differences in the specific strengthening exercises included. The most important difference was the duration of the programs. The patients in the Delaware-Oslo ACL study completed their program within 5 weeks. 8 In contrast, the exercise therapy programs for Oslo CARE and OMEX both lasted 12 weeks. 35,38 As all 3 programs required a minimum of 2 weekly sessions, the number of sessions was more than 2-fold for the OMEX and Oslo CARE patients. Finally, 10 sessions of specific perturbation training 12 were included in the Delaware-Oslo ACL study only, which means that this program had an additional component of neuromuscular training. The aim of this study, however, was not to compare the efficacy of the programs but rather to investigate whether quadriceps muscle strength deficits appeared with different characteristics between the 3 patient groups and to what extent the patients in each patient group responded to rehabilitation.
Quadriceps Muscle Strength Testing Procedure
Isokinetic strength was measured with an isokinetic dynamometer (Biodex 6000; Biodex Medical Systems Inc). The positioning of the patient was individually adjusted to ensure correct alignment of the anatomical axis of the knee joint with the axis of rotation of the lever arm during the movement. The trunk and thigh of the tested limb were fastened with straps to minimize body movements. Before the test, subjects performed a 10-minute warm-up on a stationary bike, followed by a trial session of 4 repetitions with submaximal effort to get familiarized with the dynamometer. To minimize chances of test errors, the strength curves from the trial session were visually inspected, and feedback was given to the subjects on the importance of maximum effort during the test. The test then consisted of 5 repetitions with maximum effort at an angular velocity of 60 deg/s, with the range of motion (ROM) set from 90° of knee flexion to full extension (0°). No visual feedback was provided to the subjects during the test. The reliability of assessments of quadriceps strength with the use of isokinetic dynamometers has previously been shown to be adequate, with high intraclass correlation coefficients both for healthy subjects and subjects with knee injuries and symptoms. 2,10,16,17,33 The chosen settings for ROM and velocity are the most commonly reported in present literature including patients with knee injuries. 4,16,29 The positioning of each patient at baseline was registered and replicated at the postintervention retest. To further standardize the test procedure and minimize interrater test variability, no verbal encouragement was given to the subjects during testing other than counting out loud from 1 to 5. Arms were kept crossed over the chest during the entire test.
Data Management and Statistical Analyses
Of the 5 repetitions included in the test, the one with the highest PT was identified for all patients and selected for analysis. In addition, angle-specific torque values from the same test were identified from the Biodex software program and extracted at 70°, 60°, 50°, 40°, 30°, and 20° of knee flexion. This range was chosen based on our previous work with angle-specific isokinetic strength curves 6 and after initial assessments of raw data to eliminate data noise in the acceleration and deceleration phases of the knee range of motion present at knee joint angles >70° and <20°. Side-to-side strength deficits were calculated as 100 – involved torque / uninvolved torque × 100. Strength values are reported as torque (N·m/kg).
All data were checked for outliers, normal distributions, and homogeneity of variance. Analyses of difference between the 3 patient groups were performed using 1-way between-group analysis of variance (ANOVA), and post hoc testing was assessed with the Fisher least significant difference test when a significant effect was found. Paired t tests were used to assess changes after the exercise therapy programs within the respective patient groups. Statistical Product and Service Solutions (SPSS) for Windows, V.20.0 (IBM Corp) was used to analyze the data. For all analyses, the significance level was set at P < .05.
Results
Patient Characteristics
Of 267 patients eligible at baseline, 250 completed the exercise therapy programs and retest and were included in the final material (Table 1). The demographics of the 3 patient groups are shown in Table 2.
Demographics of Patients With an ACL Injury, Degenerative Meniscus Tear, and Focal Cartilage Lesions a

a Data are presented as mean ± SD unless otherwise specified. ACL, anterior cruciate ligament; BMI, body mass index; Cart, patients with focal cartilage lesions; Men, patients with a degenerative meniscus tear.
Significant group differences were found for age, sex, body mass index (BMI), and time between test and retest (Table 2). The ACL-injury patients were significantly younger, had lower BMI, and included more women compared with patients with degenerative meniscus tears and focal cartilage lesions. As expected, due to the shorter duration of the exercise therapy program for the ACL-injury cohort, there were significant differences in time from baseline to retest. Specifically regarding the Oslo CARE study, the size of the articular chondral lesions was a mean ± SD of 2.9 ± 1.3 cm2, and the majority were located on the medial condyle (37/48).
Baseline PT Quadriceps Strength
Patients with ACL injuries had significantly higher PT strength in the involved leg at baseline than patients with degenerative meniscus tears (P = .041) and patients with focal cartilage lesions (P < .001). The involved leg for the meniscus and cartilage patients did not have significantly different PT quadriceps strength nor was there a difference between the 3 groups in PT for the uninvolved leg (all P > .050). When normalized to body weight (BW), the ACL-injury patients had significantly higher (PT/BW) quadriceps strength than did meniscus patients (P < .001), while both ACL-injury and meniscus patients had higher PT/BW quadriceps strength than cartilage patients (P < .001). No differences for the uninvolved leg were observed for PT/BW between meniscus and cartilage patients (P = .519), whereas the ACL-injury patients had significantly higher PT/BW for the uninvolved side than the 2 other groups (P < .001) (Table 3).
Peak Torque Quadriceps Strength for Both Legs at Baseline and Retest, Deficit at Peak Torque, and Largest Deficit During Movement a
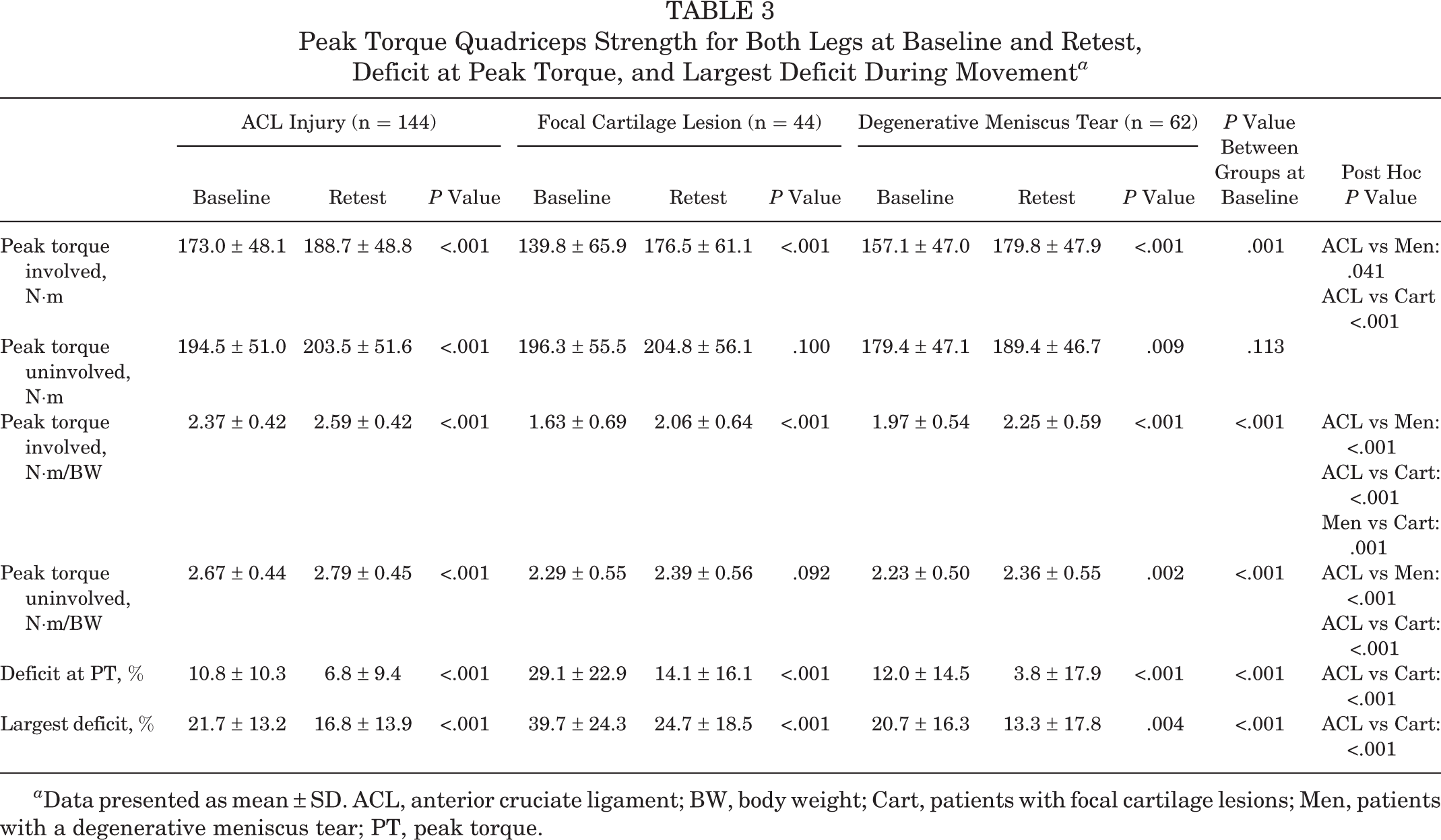
a Data presented as mean ± SD. ACL, anterior cruciate ligament; BW, body weight; Cart, patients with focal cartilage lesions; Men, patients with a degenerative meniscus tear; PT, peak torque.
Quadriceps Strength Deficits at Baseline and After Progressive Exercise Therapy
At baseline, the largest strength deficits (the highest percentage deficits between the involved and the uninvolved leg) were 21.7% (±13.2%) in patients with ACL injuries, 20.7% (±16.3%) in patients with a degenerative meniscus tear, and 39.7% (±24.3%) in patients with focal cartilage lesions (Table 3). The largest deficit was significantly higher in patients with focal cartilage lesions compared with patients with an ACL injury and patients with a degenerative meniscus tear (both P < .001). All 3 patient groups increased the absolute strength of their involved leg at retest (all P < .001), and both deficits at PT and the largest deficits observed during total ROM from 70° to 15° of knee flexion were significantly reduced in all 3 groups (all P < .001). At retest, the largest deficits were 16.8% (±13.9%) in patients with ACL injuries, 13.3% (±17.8%) in patients with a degenerative meniscus tear, and 24.7% (±18.5%) in patients with focal cartilage lesions (Table 3).
Angle-Specific Quadriceps Strength Curve Patterns at Baseline and After Progressive Exercise Therapy
Table 4 shows the angle-specific torques for involved and uninvolved legs at both time points for all 3 groups. The greatest values were consistently measured at 60° of knee flexion.
Angle-Specific Quadriceps Strength for Both Legs at Baseline and Retest a
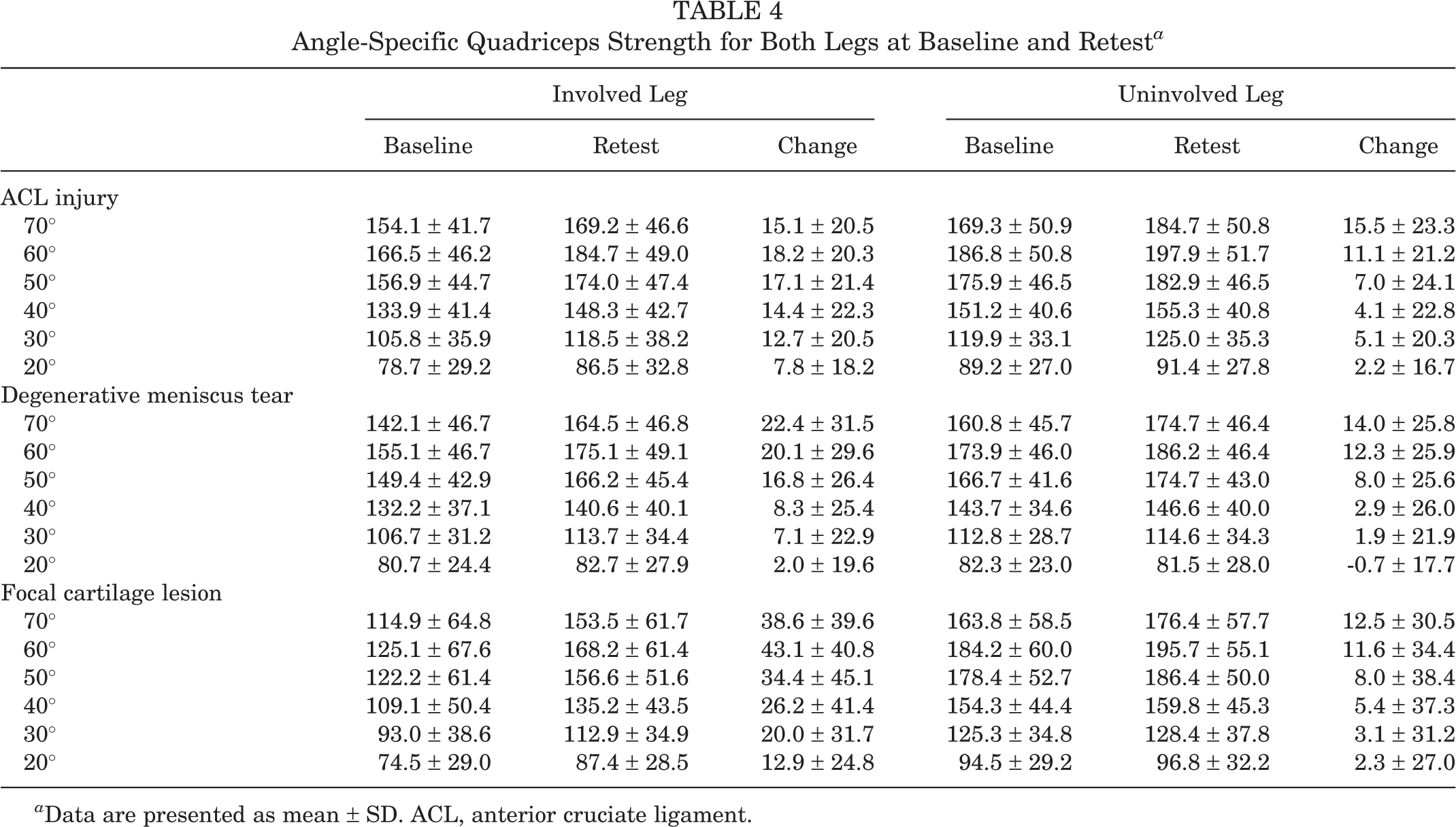
a Data are presented as mean ± SD. ACL, anterior cruciate ligament.
Figures 1 and 2 show the mean angle-specific side-to-side strength deficits at baseline and retest, respectively. The largest mean strength deficits in patients with ACL injuries were measured at 30° at baseline and at 70° at retest. In patients with a degenerative meniscus tear, the largest mean strength deficits were found at 70° both at baseline and retest. In patients with focal cartilage lesions, the largest mean strength deficits were found at 60° at baseline and 50° at retest.

Mean angle-specific deficits at baseline (anterior cruciate ligament [ACL], n = 144; meniscus, n = 62; cartilage, n = 42).

Mean angle-specific deficits at postintervention retest (anterior cruciate ligament [ACL], n = 144; meniscus, n = 62; cartilage, n = 42).
Discussion
This is the first study to quantify isokinetic quadriceps muscle strength in 3 different groups of knee-injured patients from both the gold standard of PT and angle-specific curve patterns. Furthermore, it is the first study to evaluate to what extent quadriceps muscle strength deficits both at PT and at different knee joint angles can be modified after a period of progressive exercise therapy. The patients included in this study were all recruited at a time point where they were regarded as candidates for surgical treatment but where the final treatment decision had not yet been made. Thus, our results should be interpreted in the context of preoperative assessments.
Our first research question regarded differences in PT quadriceps muscle strength between patients with ACL rupture, focal cartilage lesions, and degenerative meniscal injuries. We determined that PT (absolute value; N·m for both involved and uninvolved) was measured at 60° for all 3 groups (Table 4). However, the analyses revealed that patients with ACL injury had significantly smaller PT quadriceps muscle strength deficits at baseline compared with patients with focal cartilage lesions and degenerative meniscus tears. Furthermore, patients with focal cartilage lesions had significantly larger PT strength deficits than both patients with an ACL injury and patients with a degenerative meniscus tear (both P < .001). Concerning quadriceps muscle strength, it was not surprising that patients in the ACL cohort revealed the highest absolute values, as these patients were significantly younger and generally more athletic than patients included in the other 2 cohorts. Furthermore, due to differences in both age and activity level between the ACL cohort and the 2 other cohorts, it is likely that there were also differences in muscle morphology and absolute strength in favor of the ACL cohort. However, the finding that muscle strength deficits were more prominent for patients with focal cartilage lesions and degenerative meniscus tears should nevertheless be noted, as it may imply that muscle strength needs to be given particular focus during rehabilitation. Another important difference between the groups was the preinclusion patient history. The baseline testing of the ACL patients took place on average 8 weeks after acute injury, whereas meniscus and cartilage patients had experienced symptoms for more than 6 months and almost 4 years, respectively. Reduced quadriceps muscle strength after acute knee injury is believed to frequently be related to arthrogenic muscle inhibition (AMI), attributable to altered sensory information caused by pain, swelling, inflammation, and damage to mechanoreceptors. 1 Thus, it may be suggested that while AMI probably still played a part in patients with ACL injuries at the time of inclusion, deficits in the other groups, and in particular for cartilage patients, to a higher degree could be explained by inactivity and subsequent muscle atrophy. However, pain did not seem to play an important role in our study. All patients included in the final material were able to complete the muscle strength testing, and very few reported any pain or discomfort during testing. Our findings for the ACL cohort may further reflect findings from a recent study, 20 suggesting that the knee flexion test angle may influence whether peripheral or central factors underlie observed quadriceps muscle strength loss. The authors suggest that whereas peripheral changes could explain strength loss at 90° of knee flexion, weakness at 45° appeared to be strongly associated with limited voluntary activation in line with the presence of AMI.
Our second research question was related to quadriceps muscle strength deficits between the involved and uninvolved leg at specific knee flexion angles for the 3 patient groups. In the ACL cohort, the largest deficit was found at 30° of knee flexion rather than at the position of PT (approximately 60°). This pattern was not evident in patients with focal cartilage lesions or degenerative meniscus tears; these patients revealed the largest baseline deficit closer to or equivalent with their PT angle: at 60° for the patients with focal cartilage lesions and 70° of knee flexion for meniscus patients. Thus, our results suggest that there were differences in angle-specific assessments between the 3 patient groups. Furthermore, the largest side-to-side deficit was not disclosed for any patient group when looking at PT only. The deficits were 10.9, 10.6, and 8.7 percentage points higher than the deficits at PT for the ACL injury, cartilage lesion, and degenerative meniscus groups, respectively. These findings indicate the clinical value of including more variables than just PT in our assessments of these patient groups. If PT is not representative for the largest deficits, we may underestimate the strength loss severity. Subsequently, we may consequently also underestimate the effort needed to restore adequate muscle strength symmetry or clear patients with regard to RTS too early.
In our third and final research question, we wanted to investigate the potential for improvement of the quadriceps muscle absolute strength, and thus reduction in strength deficits, both at PT and at the angle-specific measured variables used in this study. We found significant improvements (reduced deficits) in quadriceps muscle strength at PT in all 3 groups (P < .001) (see Table 2). The deficits decreased with 4.0 percentage points for the ACL group, 15.0 percentage points for the cartilage lesion group, and 8.2 percentage points for the degenerative meniscus group. Significant improvement was established in absolute strength at the involved side in all 3 patient groups (P < .001). The strength increase was furthermore larger on the involved side than the uninvolved, which confirms the potential of strength gain on the involved side for all 3 patient groups. The smaller improvement in ACL patients may be explained both from the shorter duration of the exercise therapy program and the fact that they had the highest absolute strength values and the lowest deficits at baseline. The angle-specific deficits observed at baseline were also reduced throughout the movement cycle in all 3 groups. Importantly, the largest deficits were reduced to the same degree as the reductions at PT, with a reduction of 4.8 percentage points for the ACL group, 15.0 percentage points for the cartilage lesion group, and 7.4 percentage points for the degenerative meniscus group. Two findings postintervention were of particular clinical interest. First, the specific curve pattern with the largest deficits toward the extension portion of the ROM observed at baseline among the ACL patients did not persist at retest. Postintervention, ACL patients had their largest deficit closer to PT, at 70° of knee flexion, which means that their curve pattern was more or less equal to that for cartilage and meniscus patients. This seems reasonable from the hypothesis that the protective nature of AMI may play a part for these patients early after injury. It is also clinically important because improving strength deficits in angles close to an extended knee may contribute to reduce the risk of later reinjury. Second, the cartilage patients revealed not only the greatest deficits at baseline but also the largest reduction of the deficits. This shows the potential to significantly reduce even severe (39.7% at baseline) and long-standing deficits (mean duration of symptoms, 46 months) through a relatively short period (12 weeks) of progressive exercise therapy.
The patients included in this study were all candidates for surgical treatment. In addition to quadriceps muscle weakness after injury, previous studies have also documented long-standing postoperative deficits for patients in all categories included in this study. 3,7,9,23,31,37 Postoperative pain and swelling, as well as restriction to movement and exercise therapy during the first few months after surgery, will inevitably lead to at least some degree of nonuse atrophy. The total strength loss, and thus the level of strength that needs to be regained after surgery, will consequently be the result of aggregated pre- and postoperative muscle deficits. In this regard, delayed surgery has been argued to be a possible cause for increased muscular strength deficits. 11,25 However, this argument is only valid if the preoperative period is not utilized for adequate rehabilitation, and concurrent evidence therefore underlines the importance of targeted preoperative interventions before surgical interventions are considered. 18,32,38 The 3 exercise programs referred to in this study have all been shown to be feasible in separate studies and demonstrated clinically meaningful changes 5 with few adverse events. 8,35,38 As long as progressive rehabilitation programs introduced prior to potential surgery are conducted safely, there seems to be no reason to recommend early surgery for the 3 patient groups included in this study from the argument of strength loss.
Limitations
The study design of the 3 cohort studies did not include any control groups that did not receive progressive exercise therapy. Thus, we cannot account for improvements in muscle strength from baseline to the postintervention retest that might have occurred as a result of time only. It should also be emphasized that the study was not designed for or intended to compare the efficacy of the 3 programs. Assessments from isokinetic dynamometry are not necessarily representative for muscle performance in functional movements and activities, even though it is the established gold standard for isolated quantification of muscle strength in defined movements. Further studies are thus required to investigate to what extent our findings may be reflected in other performance-based outcome measures and self-reported measures.
Conclusion
This study provides new data on isokinetic quadriceps muscle strength throughout the ROM, including both the gold standard outcome measure of PT and angle-specific torque values in patients with ACL injury, focal cartilage lesions, and degenerative meniscus tears. Despite differences in patient characteristics and potentially different underlying mechanisms for strength loss, all patients revealed excellent potential for quadriceps strength improvements during progressive exercise therapy. However, analyses of angle-specific torque values suggest that assessment of PT alone may not reflect the maximal level of deficit in quadriceps strength assessment. It is therefore plausible to suggest more comprehensive testing protocols when evaluating quadriceps muscle strength in these patient groups to quantify evident deficits.
Footnotes
Acknowledgment
The material in this study has been synthesized from 3 different original studies, where a number of people have contributed. The authors acknowledge research coordinator Kristin Bølstad for the organization of the participants and physical therapists Karin Rydevik, Marte Lund, Emilie Jul-Larsen Aas, Annika Storevold, Espen Selboskar, and Ida Svege for assistance in data collection. We further acknowledge our international and national collaborators in the Delaware-Oslo cohort study (Professor Lynn Snyder-Mackler), the OMEX Study (Professor Ewa Roos), the Oslo CARE Study (Professor Asbjørn Årøen), as well as the PhD students collecting data in these 3 cohorts (Silje Stensrud, Nina Kise, Jan Harald Røtterud, and Barbara Wondrasch). Finally, we also acknowledge the Norwegian Sports Medicine Clinic (Nimi), Oslo, Norway, for supporting the Norwegian Research Center for Active Rehabilitation (NAR) with rehabilitation facilities as well as the Department of Orthopaedic Surgery, Oslo University Hospital; the Department of Orthopaedic Surgery, Martina Hansens Hospital, Bærum; and the Department of Orthopedic Surgery, Akershus University Hospital for accessibility to patients and clinical resources.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study is based on funding from the following grants: The Delaware-Oslo ACL Cohort (NIH Grant No. 5 R37 HD 037985 -11); the OMEX study: The South-Eastern Norway Regional Health Authority, Sophies Minde Ortopedi AS, the Swedish Rheumatism Association, the Swedish Scientific Council, Region of Southern Denmark, and the Danish Rheumatism Association; and the Oslo CARE study: South-Eastern Norway Regional Health Authority and the Norwegian Research Council. The OMEX study is registered on ![]() : NCT01002794.
: NCT01002794.