
Abstract
Background:
Patients and clinicians often struggle to choose the optimal management strategy for posttraumatic knee osteoarthritis (OA) after an anterior cruciate ligament (ACL) injury. An evaluation of radiographic outcomes after a decision-making and treatment algorithm applicable in clinical practice can help to inform future recommendations and treatment choices.
Purpose:
To describe and compare 5-year radiographic outcomes and knee pain in individuals who had gone through our decision-making and treatment algorithm and chosen (1) early (<6 months) ACL reconstruction (ACLR) with pre- and postoperative rehabilitation, (2) delayed (>6 months) ACLR with pre- and postoperative rehabilitation, or (3) progressive rehabilitation alone.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
We included 276 patients with unilateral ACL injury from a prospective cohort study. Patients chose management using a shared decision-making process and treatment algorithm, and 5-year postoperative radiographs of the index and contralateral knees were assessed using the Kellgren and Lawrence (K&L) classification and minimum joint space width measurements. We defined radiographic tibiofemoral OA as K&L grade ≥2 and knee pain as a Knee injury and Osteoarthritis Outcome Score for Pain ≤72. To further explore early radiographic changes, we included alternative cutoffs for radiographic knee OA using K&L grade ≥2/osteophyte (definite osteophyte without joint space narrowing) and K&L grade ≥1.
Results:
At 5 years, 64% had undergone early ACLR; 11%, delayed ACLR; and 25%, progressive rehabilitation alone. Radiographic examination was attended by 187 patients (68%). Six percent of the cohort had radiographic tibiofemoral OA (K&L grade ≥2) in the index knee; 4%, in the contralateral knee. Using the alternative cutoffs at K&L grade ≥2/osteophyte and K&L grade ≥1, the corresponding numbers were 20% and 33% in the index knee and 18% and 29% in the contralateral knee. Six percent had a painful index knee. There were no statistically significant differences in any radiographic outcomes or knee pain among the 3 management groups.
Conclusion:
There were no statistically significant differences in any 5-year radiographic outcomes or knee pain among the 3 management groups. Very few of the patients who participated in our decision-making and treatment algorithm had knee OA or knee pain at 5 years.
Many patients experience the devastating consequences of posttraumatic knee osteoarthritis (OA) after an anterior cruciate ligament (ACL) injury. 1,3,30,45 Patients and clinicians often struggle to choose the optimal management strategy. A randomized controlled trial (the KANON trial) found no difference in 5-year radiographic tibiofemoral OA or cartilage thickness between patients who underwent early ACL reconstruction (ACLR) plus rehabilitation versus rehabilitation alone (plus the option of delayed ACLR). 16,58 In clinical practice, however, shared decision-making tends to result in different patients choosing different management strategies. 4,39,47 Recent research has also discovered that certain patients do better with certain mangements. 15,19 We therefore need to evaluate both clinical and radiographic outcomes after decision-making and treatment algorithms applicable in clinical practice. Such studies hold high external validity and can help to inform future recommendations and management choices.
The Delaware-Oslo ACL Cohort Study is a longitudinal cohort study of patients with acute ACL injury. The patients underwent a 5-week preoperative rehabilitation program before they chose rehabilitation only or ACLR as part of an informed shared decision-making process with their treating clinicians. Several elements of our decision-making and treatment algorithm are included in evidence-based recommendations for the management of ACL injuries, 14 and our results are therefore highly relevant for patients and clinicians outside our cohort. We have previously reported no statistically significant differences in the 5-year clinical, functional, and physical activity outcomes between patients treated with early ACLR, delayed ACLR, or progressive rehabilitation alone. 43
As the processes leading to knee OA start long before radiographic changes are evident, 12,38 measures of established OA do not sufficiently detect early OA development. Different criteria for defining early knee OA with and without radiological findings have been proposed without reaching a consensus, but knee pain is frequently included in previous definition proposals 33 –35,49 and is often the first sign of knee OA. 12,50 Different radiographic outcomes also contribute with different constructs of joint disease. 25,26,32 It is therefore of great interest to report a range of radiographic features and knee pain in addition to the more established radiographic knee OA cutoff of Kellgren and Lawrence (K&L) grade ≥2.
This study aimed to describe and compare 5-year radiographic outcomes and knee pain in individuals who had gone through our decision-making and treatment algorithm and chosen (1) early (within 6 months) ACLR with pre- and postoperative rehabilitation, (2) delayed (later than 6 months) ACLR with pre- and postoperative rehabilitation, or (3) progressive rehabilitation alone.
Methods
Patients
Between 2006 and 2012, we consecutively included 300 athletes at the Norwegian Sports Medicine Clinic in Oslo, Norway, or at the University of Delaware in Newark, Delaware. At inclusion, complete ACL injury and concomitant injuries were verified using magnetic resonance imaging (MRI) and increased anterior knee joint laxity (measured via a KT-1000 arthrometer; MED Metric). Of these 300, 24 had a graft rupture after a previous ACLR; hence, 276 patients with a first-time ACL injury (142 from Oslo and 134 from Delaware) were included in the analysis for this paper. Patients had to participate in level 1 (jumping, cutting, and pivoting sports such as soccer, football, handball, basketball, and floorball) or level 2 (lateral movements with less pivoting such as racket sports, alpine skiing, snowboarding, gymnastics, baseball, and softball) sports 22 ≥2 times per week preinjury and be between 13 and 60 years of age. They had to have resolved acute impairments (have no or minimal pain or effusion during or after plyometric activities) before inclusion (within 3 months after ACL injury in Norway and within 7 months in Delaware). We excluded patients with previous knee injuries or surgeries to either knee, bilateral injuries, other grade 3 ligament injuries, full-thickness articular cartilage damage, or fracture and patients who were unable to attend preoperative rehabilitation or had obviously repairable menisci on MRI.
We obtained written informed consent or assent with parental consent from all patients and approvals from the Regional Committee for Medical and Health Research Ethics of Norway and the University of Delaware Institutional Review Board before inclusion.
Treatment Algorithm
After inclusion (mean, 59 days after injury), all patients were educated on different management strategies and participated in a 5-week (10-session) preoperative rehabilitation program using progressive neuromuscular and strength training exercises. 9 Thereafter, they underwent functional testing and chose their management in dialogue with their physical therapists and orthopaedic surgeons. We were more likely to recommend ACLR to patients who wished to return to level 1 sports and to those who experienced dynamic knee instability. The most frequent patient-reported reason for choosing progressive rehabilitation alone was the achievement of good knee function after rehabilitation. 17 Delayed ACLR was indicated if patients subsequently experienced dynamic knee instability or changed their minds.
Graft choice was a shared decision with the orthopaedic surgeon. Bone–patellar tendon–bone autografts (21.5%), single-bundle or double-bundle hamstring autografts (51.5%), and allografts (27%) were used. Several experienced sports orthopaedic surgeons (in the United States, subspecialty certified) performed the ACLRs. Postoperative rehabilitation was individually adjusted depending on concomitant injuries, graft type, and knee function and consisted of 3 phases. The goal of the acute postoperative phase (phase 1) was to reduce swelling and atrophy and restore range of motion. The goal of the rehabilitation phase (phase 2) was to attain muscle strength and hop performance limb symmetry index ≥80% and to regain neuromuscular control. In the return-to-sports phase (phase 3), patients aimed to attain strength and hop performance limb symmetry index ≥90% and gradually increased participation in sports-specific training. The progressive rehabilitation alone group typically continued progressive rehabilitation for 3 to 4 months after the completion of the formal rehabilitation program and underwent the same testing as the ACLR groups.
Data Collection and Outcome Measurements
Information regarding patient characteristics, the injury, and surgical procedures was collected at inclusion or at the time of ACLR. New injuries to the index and contralateral knee were reported at follow-up. Follow-up was 5 years after completion of preoperative rehabilitation or ACLR. Clinical, functional, and physical activity outcomes at 2 years 11,17,18 and 5 years 43 have been reported previously.
Radiographic Outcomes
We used standardized weightbearing radiographs taken bilaterally from a posteroanterior view. In Norway, a fixed flexion protocol using a SynaFlexer Positioning Frame (Synarc, Inc) and 10° caudal beam angulation was used to ensure consistent and reproducible knee angulation and alignment. 23,27 In Delaware, the Lyon Schuss protocol was used. 28 The patients were positioned with 30° of knee flexion with the pelvis, thighs, and patella flush against the film cassette and coplanar with the tips of the great toes. The radiographic beam was adjusted for each image to align with the medial tibial plateau.
An experienced radiologist (R.G.) with high intrarater reliability (kappa = 0.77) 41 graded all the radiographs from both study sites according to the K&L classification for the tibiofemoral joint. 26 The K&L classification is well recognized for assessing radiographic knee OA based on osteophyte and joint space narrowing severity (grade 0, normal, to grade 4, severe). 1,26,29 We used the modified K&L definition proposed by Felson et al, 13 which distinguishes between knees with both definite osteophyte and possible joint space narrowing (K&L grade 2) and knees with definite osteophyte without joint space narrowing (K&L grade 2/osteophyte). We defined K&L grade ≥2 as radiographic OA and included K&L grade ≥2/osteophyte as an alternative cutoff for early radiographic changes in the tibiofemoral joint. 13,42 K&L grade 1 (doubtful joint space narrowing and possible osteophytic lipping) has been associated with progression of radiographic features, 21 and some have argued that K&L grade 1 should be treated as early-phase joint disease. 48,51 We therefore included K&L grade ≥1 as another alternative cutoff for early radiographic changes.
Since the K&L classification is highly osteophyte-centric, measurements of tibiofemoral minimum joint space width (mJSW) can contribute another aspect of joint degeneration. mJSW is a quantitative measure reflecting thickness of articular cartilage and meniscal pathology. 25,32 Substantial tibiofemoral mJSW changes are common early after ACLR and are associated with pain and worse quality of life. 52,53 The radiologist measured the mJSW manually at the narrowest point in each compartment using the most apparent cortical strip (interpreted as the anterior rim) of the femur and the tibia. Manual mJSW measurements have previously shown high reproducibility. 44 For 26 patients, ≥1 mJSW measures were impossible to perform because of poor projection or overexposure. Because variation in radiograph quality and protocols affects mJSW measures, 28,36,55 we expressed medial and lateral mJSW as the difference between the index and contralateral knees (mJSWdiff) in our statistical analysis.
Knee Pain
Pain was evaluated using the Knee injury and Osteoarthritis Outcome Score (KOOS) Pain subscale, which ranges from 0 to 100 points (100 indicates no impairment). 46 Patients with scores ≤72 were classified as having knee pain. This cutoff (2 standard deviations below the reported normal mean value in an athletic population) has previously been used to identify patients with a painful knee and patients with early symptomatic knee OA after ACLR. 56,57
Data Management and Statistical Analysis
A negative mJSWdiff indicates a narrower joint space in the index knee than the contralateral knee, while a positive mJSWdiff indicates a wider joint space in the index knee. The mJSWdiff variables were skewed according to the Kolmogorov-Smirnov test, but by inspecting histograms and skewness, we considered them close enough to a normal distribution to use parametric tests. 10
We report descriptive statistics for all outcomes for each treatment group, including separate statistics for those with and without new/concomitant injuries to the index or contralateral knee. We assessed group differences in nominal outcome variables using the chi-square test and group differences in mJSWdiff using 1-way analysis of variance.
Results
At 5 years, 187 patients (68%; 80% in Oslo and 55% in Delaware) attended radiographic examination, with similar attendance in the management groups (P = .055) (Figure 1). Loss to follow-up caused an inability to ascertain the treatment status for 14 patients who had been nonsurgically managed at the last follow-up (5% of the cohort). Patients who attended the follow-up were significantly older (mean difference, 3.8 years) and had lower body mass index (BMI) at inclusion (mean difference, 1.3) than did those who did not (n = 89). KOOS Pain scores were available for 220 patients (80%).
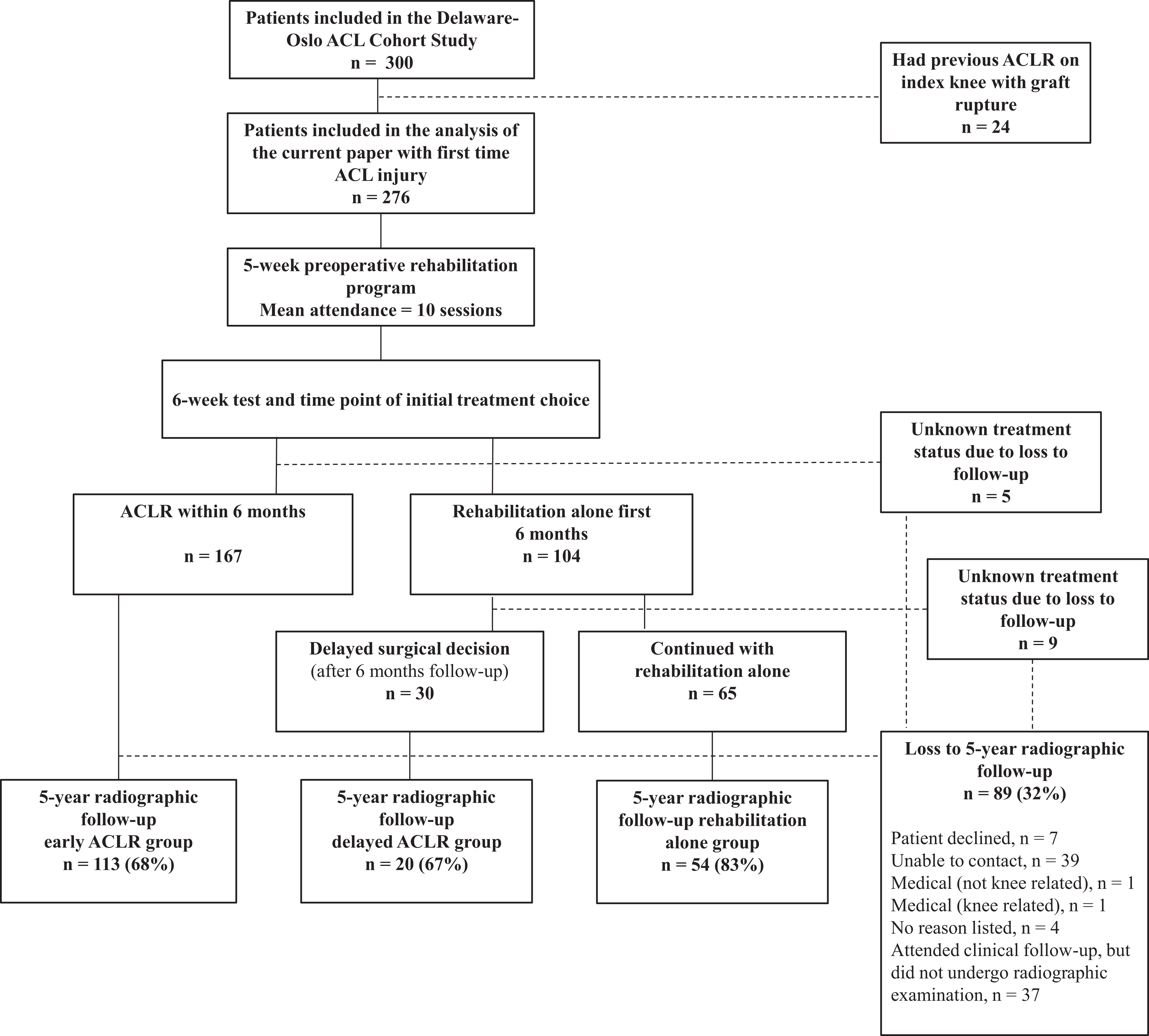
Study flowchart. ACL, anterior cruciate ligament; ACLR, ACL reconstruction.
Of the 262 patients with ascertained treatment status, 167 (64%) had undergone early ACLR, 30 (11%) delayed ACLR, and 65 (25%) progressive rehabilitation alone. Most patients who crossed over from the rehabilitation alone group to delayed ACLR did so early: 19 patients crossed over between 6 and 12 months after inclusion; 7 patients, between 12 and 24 months; and only 4 patients, at >24 months. The 2 ACLR groups were significantly younger, were more likely to participate in level 1 sports preinjury, and had more concomitant injuries to the medial meniscus at inclusion compared with the progressive rehabilitation alone group (Table 1). During ACLR, 41% and 40% in the early and delayed ACLR groups, respectively, had meniscal surgeries, of which 26% were excisions, 56% were repairs, and 18% were trephination/rasping.
Characteristics at Inclusion: Group Comparisons a
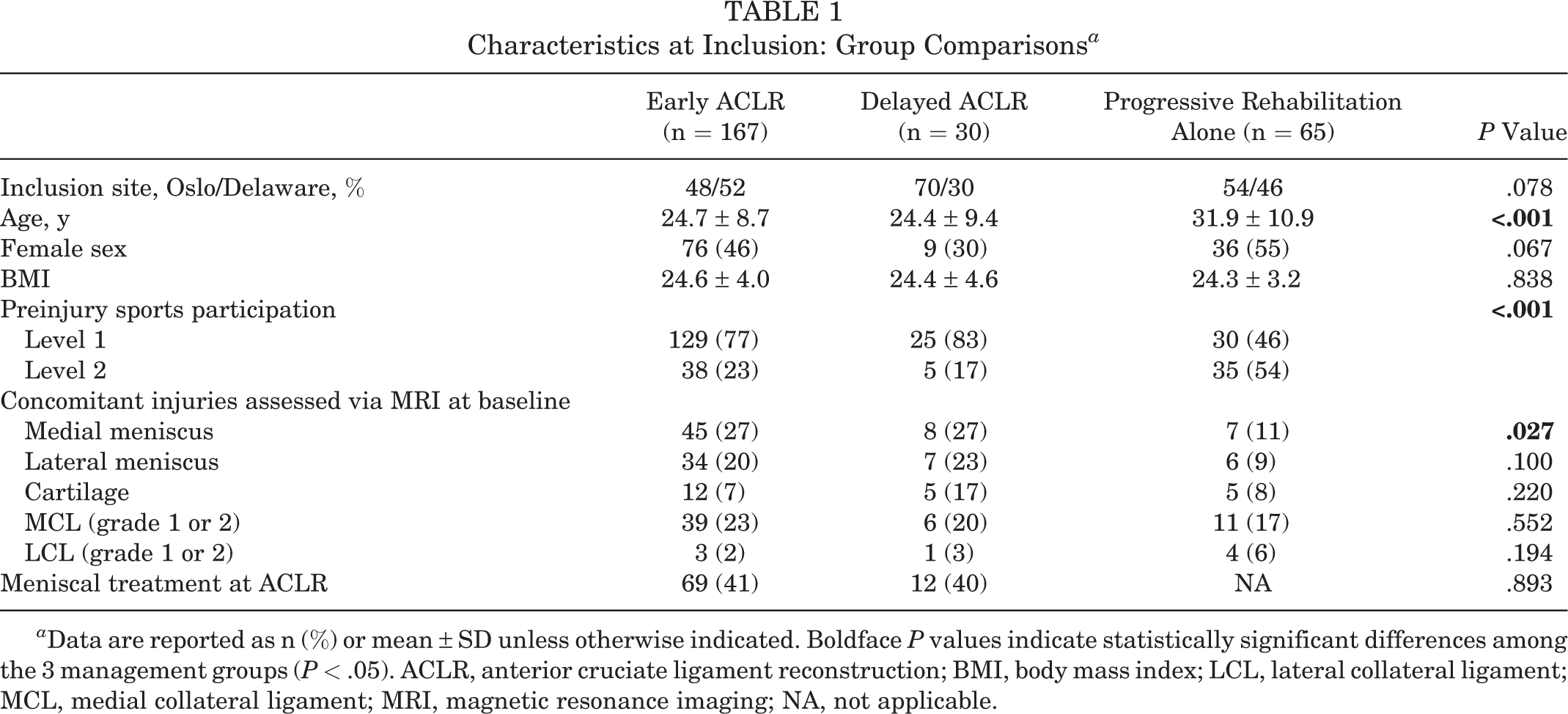
a Data are reported as n (%) or mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant differences among the 3 management groups (P < .05). ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; LCL, lateral collateral ligament; MCL, medial collateral ligament; MRI, magnetic resonance imaging; NA, not applicable.
Five-year tibiofemoral K&L grades in the index and contralateral knees are presented in Figure 2. Using the cutoff at K&L grade ≥2, 6% (95% confidence interval [CI], 3-11) of the cohort had radiographic tibiofemoral OA in the index knee; 4% (95% CI, 2-8), in the contralateral knee (Table 2). Using the alternative cutoffs at K&L grade ≥2/osteophyte and K&L grade ≥1, the corresponding numbers were 20% (95% CI, 15-27) and 33% (95% CI, 27-40) in the index knee and 18% (95% CI, 13-25) and 29% (95% CI, 22-36) in the contralateral knee. Regardless of K&L cutoff used, there were no statistically significant differences in the prevalence of radiographic tibiofemoral OA in either the index (P = .110-.919) or contralateral (P = .291-.869) knee among the 3 management groups (Table 2). Six percent (95% CI, 2.8-9.3) of the cohort had a painful index knee, and there were no statistically significant differences among the 3 management groups (P = .184).

Kellgren & Lawrence (K&L) grades for all index and contralateral knees in percentage for each management group (n = 187). 2/o, 2/osteophyte. ACLR, anterior cruciate ligament reconstruction.
Five-Year Outcomes: Group Comparisons a

a Data are reported as n/N (%) or mean ± SD unless otherwise indicated. Dashes illustrate that there were no patients in these subgroups to perform calculations on. ACLR, anterior cruciate ligament reconstruction; K&L, Kellgren and Lawrence; mJSW, minimum joint space width; OA, osteoarthritis.
b Graft ruptures or concomitant/new injuries to meniscus or cartilage of the index knee.
c Knee injury and Osteoarthritis Outcome Score Pain of 72.
d Contralateral injuries to the anterior cruciate ligament, meniscus, or cartilage.
e A negative joint space difference indicates a narrower joint space in the index knee compared with the contralateral knee, while a positive joint space difference indicates a wider joint space in the index knee.
Five-year mJSW measurements in both compartments of the index and contralateral knees are described in Figure 3, while mJSWdiff is expressed in Table 2. The mJSWdiff was similar across the 3 management groups in both the medial (P = .053) and lateral (P = .305) compartments.
We did not assess prognostic factors for knee OA or knee pain, as it was beyond the aim of this paper and because we had few observed cases.

Mean medial and lateral minimum joint space width (mJSW) measurements for all index and contralateral knees (n = 164-176) in millimeters and 95% CI for each management group. ACLR, anterior cruciate ligament reconstruction.
Discussion
We found no statistically significant differences in any radiographic outcomes or knee pain among the 3 management groups. More importantly, few patients who participated in our decision-making and treatment algorithm had radiographic tibiofemoral OA (K&L grade ≥2): 7% of the index and 4% of the contralateral knees in the early ACLR group, 15% and 5% in the delayed ACLR group, and 2% and 6% in the progressive rehabilitation alone group. K&L grades ≥2/osteophyte and ≥1, which may represent early-phase joint disease, were found in 19% to 21% and 25% to 35% of the index knees, respectively, and 16% to 20% and 20% to 32% of the contralateral knees, respectively. Only 6% of the cohort had a painful index knee.
Following our decision-making and treatment algorithm, we have previously reported excellent 5-year clinical, functional, and physical activity outcomes with no statistically significant differences among the management groups. 43 To our knowledge, this is the first study to compare 5-year radiographic outcomes following a specific treatment algorithm where management was chosen based on shared decision-making. As in clinical practice, different patients choose and are recommended different managements, which increases the external validity of our study. Because this study was not an effect study and because we aimed to describe and compare outcomes in the 3 management groups following our decision-making and treatment algorithm, we performed unadjusted analyses. Differences among management groups at inclusion (age, preinjury activity level, and concomitant meniscal injuries) may therefore have affected outcomes: for example, older age may have increased the risk of OA 20 in the rehabilitation alone group, while fewer concomitant meniscal injuries may have acted in the opposite direction. 1,41 There were also small but statistically significant differences in age and BMI between those who did and those who did not attend the 5-year radiographic follow-up, which may have affected our results.
The previously mentioned KANON trial also reported on the incidence of 5-year radiographic knee OA after early ACLR (plus rehabilitation) and after rehabilitation alone (plus the option of delayed ACLR). 16 Similar to our results, they found no statistically significant differences among the treatment groups. 16 According to the Osteoarthritis Research International (OARSI) atlas, 12% of the patients in the KANON trial had radiographic tibiofemoral OA in the index knee at 5 years. As the OA rates are reported to be almost twice as high when using the OARSI atlas compared with using K&L grade ≥2, 6 their rate corresponds well with ours. In contrast to our study—and longer term after ACL injury or reconstruction—a recent systematic review found a higher risk of radiographic knee OA >10 years after ACLR (range, 24%-80%) than after rehabilitation alone (range, 11%-68%), but because of low quality of included studies, the results should be interpreted with caution. 31 Early cartilage degeneration assessed using MRI has also been shown to be more pronounced after ACLR than after rehabilitation alone in some studies, 54 while no differences have been found in others. 58 Our study, along with studies with longer-term follow-ups 2,31,40 and animal studies, 7 reinforces the conclusion that reconstruction does not protect the ACL-injured knee from OA. Hence, rehabilitation alone does not provide inferior long-term outcomes compared with ACLR and is a viable solution for some patients.
The KOOS Pain cutoff at ≤72 points applied in this study has previously been used to define significant knee pain and OA after primary unilateral ACLR. 56,57 The prevalence rates in these previous studies were 9% at 6 years postoperatively 57 and 10% at 7 years postoperatively. 56 These numbers correspond well with those of our cohort, where the 5-year prevalence rates of knee pain were 13% in the early ACLR group, 6% in the delayed ACLR group, and 4% in the progressive rehabilitation alone group. Importantly, different definitions of knee pain result in different prevalence rates. In the study of Wasserstein et al, 57 the KOOS Pain cutoff at ≤72 points was 1 of 3 models used to explore prevalence of knee pain using the KOOS subscales. The prevalence rates were 39% and 12% when the other 2 models were used. 57 The reported threshold for a Patient Acceptable Symptom State (PASS) for the KOOS Pain subscale of 88.9 points 37 is also considerably higher than the cutoff used in our study, and hence we might have diagnosed more patients with knee pain if we had used a cutoff similar to the the PASS threshold. The recent work of Luyten et al 33 suggested more comprehensive classification criteria for early knee OA, which included clinical examination of joint line tenderness or crepitus in addition to KOOS subscales. Such a clinical examination was unfortunately not performed in our study.
Future research could apply more comprehensive definitions of symptomatic knee OA and early joint disease. In our study, using the alternative OA cutoffs at K&L grades ≥2/osteophyte and ≥1, we diagnosed 3 to 7 times more patients with knee OA than using the acknowledged cutoff at K&L grade ≥2. As very few patients in our cohort had knee pain and the OA rates were similar in the contralateral knees, we do not know how clinically relevant these radiographic findings are. Longer follow-ups of our cohort can explore whether K&L grades 1/- and 2/osteophyte at 5 years predict development or progression of the disease and contribute to the discussion of whether these radiographic findings should be considered early-phase joint disease. Other imaging techniques such as MRI are also valuable in the assessment of early knee OA. 23,24 We also need more studies with high quality and power to compare rates of radiographic and symptomatic knee OA after different management processes and decision-making algorithms. Such studies can provide more robust estimates and conclusions to guide clinical practice and thereby improve outcomes for patients with ACL-injured knees.
Limitations
Even though it was similar across management groups, the loss to follow-up for radiographic outcomes of 32% was a limitation of our study. Furthermore, the radiograph quality was in some cases (n = 26) unsuitable for the assessment of mJSW. Although the study design and treatment algorithm increase the external validity of our study, we can only generalize our results to patients who are active in jumping, pivoting, or cutting sports preinjury; do not have significant concomitant injuries; manage to resolve acute impairments within 3 to 7 months after injury; and are able and willing to attend rehabilitation and follow-ups. We also emphasize that 5-year radiographic outcomes represent early degenerative changes and differences in end-stage joint disease must be assessed at later follow-ups of the cohort.
Power may be another limitation of this study: the 95% CIs for our estimates of OA rates were quite wide, especially in the small delayed ACLR group. Therefore, we might have been unable to detect clinically relevant group differences for all outcomes. Even though not statistically significant (P = .053), the early ACLR group had a more positive medial mJSWdiff than did the delayed ACLR group (mean difference, 0.4 mm; 95% CI, –0.1 to 0.9), and this group difference exceeded the previously reported smallest detectable difference between 2 measurements for mJSW of 0.26 to 0.28 mm. 5,8
Conclusion
Following our decision-making and treatment algorithm, there were no statistically significant differences in any 5-year tibiofemoral radiographic outcomes or knee pain among the 3 management groups: early ACLR, delayed ACLR, and progressive rehabilitation alone. Few patients in our cohort had radiographic tibiofemoral OA (K&L grade ≥2) in the index (6%) or contralateral (4%) knee. Only 6% of the cohort had knee pain.
Footnotes
Acknowledgment
The authors thank all the participating patients in the study cohort, as well as the Norwegian Sports Medicine Clinic (NIMI) and University of Delaware Physical Therapy Clinic for providing facilities for clinical testing, and those who assisted with data collection: Martha Callahan, Håvard Moksnes, Ingrid Eitzen, Annika Storevold, Ida Svege, Espen Selboskar, Ben Clarsen, Karin Rydevik, Marte Lund, Andrew Lynch, David Logerstedt, Airelle Giordano, Angela Smith, Kristin Bølstad, Matthew Failla, and Elizabeth Wellsandt. The authors also thank James Alesi for organizing the database and Morten W. Fagerland for statistical advice.
Final revision submitted February 9, 2021; accepted February 28, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the National Institutes of Health (grant R37HD37985). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Regional Committee for Medical and Health Research Ethics of Norway.