
Abstract
Background:
The Simple Shoulder Test (SST) is a widely used patient-reported outcome measure for shoulder function. However, there is currently no version of the SST for the Thai population.
Purpose:
To cross-culturally adapt and evaluate the reliability and validity of a Thai version of the SST (Thai SST) for patients with shoulder pathologies, using the Thai version of the American Shoulder and Elbow Surgeons (ASES) score as a comparison tool.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
The Thai SST was developed using a standard translation and cross-cultural adaptation process. A total of 75 Thai patients, comprising 73 with rotator cuff tears, 3 with combined rotator cuff tear and secondary stiff shoulder, 2 with combined rotator cuff tear and biceps tendinitis, 1 with isolated adhesive capsulitis, and 1 with isolated long head biceps tendinopathy, completed the Thai SST and the Thai ASES score. The internal consistency, test-retest reliability, and construct validity of the Thai SST were assessed.
Results:
The 75 participants consisted of 19 men and 56 women with a mean age of 63.16 ± 7.66 years. The Thai SST demonstrated a strong positive correlation with the Thai ASES (r = 0.714). The test-retest reliability for the Thai SST was good (intraclass correlation coefficient, 0.895). The Cronbach alpha of the Thai SST was 0.85, indicating good and acceptable internal consistency.
Conclusion:
Our study demonstrated that the Thai SST had acceptable reliability and validity, making it a suitable patient-reported outcome measure for assessing shoulder function in Thai patients with shoulder problems. The Thai SST can be used to assess the effectiveness of interventions for these shoulder pathologies in Thai patients.
Keywords
Shoulder pain is a common orthopaedic condition in the general population. The prevalence of symptoms ranges from 7% to 27% in those <70 years and 13.2 to 26% in those aged 70 years or older. 14 The primary goal of treating shoulder pain patients is to relieve pain, improve range of motion, and restore normal function. As a result, a method for assessing pain and shoulder function is necessary. The patient-reported outcome score is essential for clinical practice as well as research. There are several patient-reported outcome scores available for clinical usage to measure shoulder function. 1
The Simple Shoulder Test (SST) is a self-administered questionnaire that evaluates a patient's ability to perform activities of daily living related to the shoulder.9,13,16 It has since been translated and validated in several languages, including Arabic, 25 Brazilian, 19 Persian, 17 Dutch, 11 Italian, 15 and Japanese. 24 The SST is a reliable and valid tool for assessing shoulder function in patients with different shoulder pathologies, such as rotator cuff tears, adhesive capsulitis, and shoulder instability.7,9,23 Another commonly used patient-reported outcome score to assess shoulder function is the American Shoulder and Elbow Surgeons (ASES) score, introduced by Richards et al 22 in 1994. The ASES score has been proven to be a reliable and valid tool for assessing shoulder function in patients with various shoulder pathologies. 23 The Thai version of the ASES score has been translated, and its validity and reliability have been tested. 20
Currently, the SST has not been translated into Thai and validated for use in that language. Therefore, it is necessary to undergo a cross-cultural adaptation process to ensure that the SST is suitable for use in a different culture or language. This process involves translating the original version of the questionnaire into the target language and adapting it to the cultural context of the target population. 2
The purpose of this study was to cross-culturally adapt and evaluate the reliability and validity of the Thai version of the SST (Thai SST). Additionally, we compared the Thai SST with the Thai ASES score to determine their correlation. We hypothesized that the Thai SST would be a valid and reliable tool for assessing the functional status of Thai patients with shoulder-related problems.
Methods
Participants
This study was approved by the institutional review board of our affiliated institution, and all patients provided written informed consent. The study recruited a total of 75 Thai patients who were evaluated for shoulder pathology at the outpatient orthopaedic sports medicine clinic of the King Chulalongkorn Memorial Hospital in Bangkok, Thailand. To develop this study, we followed the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) reporting guideline for studies on measurement properties. 21 The inclusion criteria for this study were patients with shoulder pain or disability, such as rotator cuff tears, shoulder instability, long head biceps tendinopathy, and adhesive capsulitis. The diagnosis of these conditions was confirmed through clinical examination and radiographic studies. Patients who were Thai speaking, literate, and <70 years were included in the study. Exclusion criteria were patients <18 years; those who received interventions during the test-retest period; those with cognitive impairment, infections, and inflammatory arthritis; and those who were unable to understand Thai. All 75 participants with shoulder problems who met the inclusion criteria were able to complete the questionnaires, with no loss to follow-up.
The SST and ASES Score
The SST (available separately as Supplemental Material) is a questionnaire that is commonly used to assess the function of the shoulder. It was designed to evaluate the ability of an individual to perform various tasks and activities that require shoulder function, such as reaching, lifting, and carrying objects. The SST is a straightforward and simple patient-reported outcome measure that can be completed by patients at home within a short time frame; this feature is particularly advantageous for surgeons with busy schedules. It consists of 12 dichotomous questions, each of which is scored on a 1-point scale (yes = 1, no = 0). The total score ranges from 0 to 12, with higher scores indicating better shoulder function.9,13,16
The ASES score is a patient-reported outcome measure used to assess shoulder function and pain. It is composed of 2 parts: pain and activities of daily living. The pain element is graded on a visual analog scale ranging from 0 (no pain) to 10 (most severe pain imaginable). The activities of daily living section contains 10 items, with each item accompanied by 4 answer options ranging from 0 to 3. An answer of 0 indicates the inability to perform the task, while an answer of 3 signifies the ability to perform the task with no difficulty. The pain and activities of daily living subscores are then combined to produce a percentage score, where each part accounts for 50% of the final score, with a maximum total score of 100. A higher score suggests better shoulder function.22,23
Translation and Cross-Cultural Adaptation of the SST
The translation and cross-cultural adaptation of the SST were conducted using the guidelines recommended by Beaton et al. 2 The forward translation was performed by 2 skilled experts in Thai and English, both of whom came from different backgrounds. The first forward translator (N.T.), an orthopaedic surgeon specializing in sports medicine, was knowledgeable about diseases, disease progression, and the purposes of the SST, in conjunction with the clinical perspectives of a specialist. The other translator was a linguistic expert with no medical background. The 2 translators independently translated the original version of the SST into Thai (Figure 1). This translation did not contain any clinical prejudice and used more accessible language appropriate for the general Thai-speaking population. A consensus version was then created by the 2 forward translators, and this version was back-translated into English by another bilingual translator with no medical background who, to avoid any potential bias, had not read it before, as well as by a fellowship-trained orthopaedic sport medicine surgeon (A.W.). A review committee consisting of the translators, the research team, and another orthopaedic surgeon (T.I.) reviewed the translated and back-translated versions and created a prefinal version of the Thai SST. The prefinal version was then pilot-tested on 10 Thai patients with shoulder pathology to identify any cultural or linguistic problems. The final version of the Thai SST was created after the pilot testing; this version (see Supplemental Material) was used for the subsequent study.

Diagram showing the translation and cross-cultural adaptation process.
Data Collection
Demographic data were also collected, including age, sex, diagnosis, body mass index, level of education, the affected shoulder, and the amount of time between symptom onset and when the questionnaire was completed. To avoid any order bias, the Thai SST and Thai ASES were administered to the study participants in random order. When patients visited our hospital's outpatient clinic, they were given the questionnaires via a Google Form in the waiting areas. The research assistant kept track of each patient's questionnaire completion time as well as any difficulties they faced. All patients were requested to complete a second round of the Thai SST the day after consulting their health care provider in order to assess reliability, and patients were asked to complete a third round of the Thai SST 14 days later in order to assess overall test-retest reliability. When assessing the miss rate for each item, we defined an acceptability problem as a miss rate of >5%. Figure 2 describes the procedure in detail.
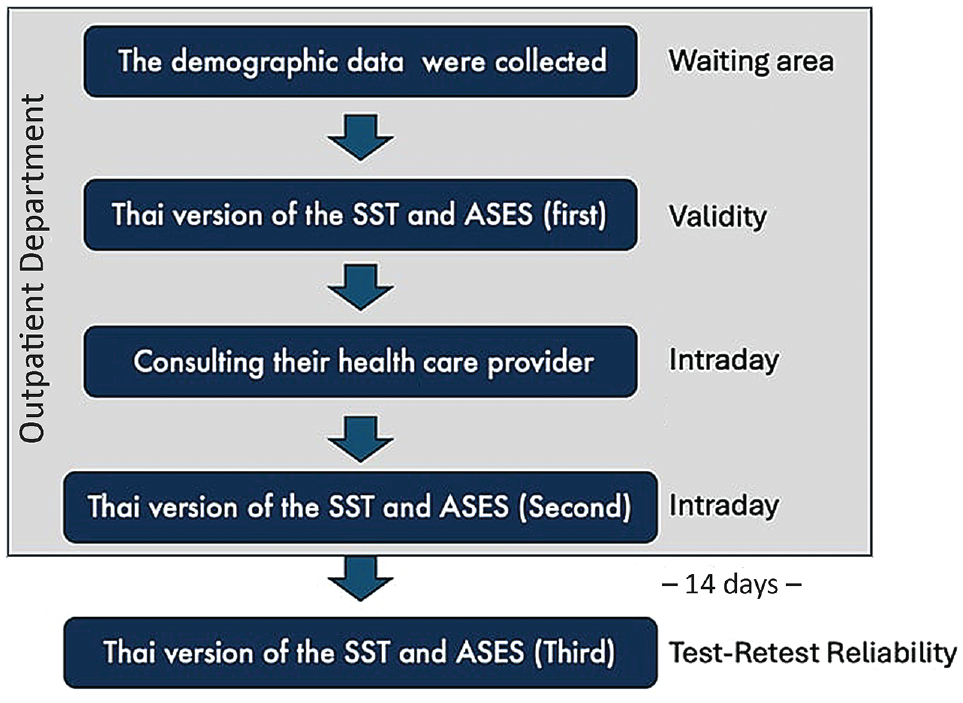
Diagram showing the data collection process. ASES, American Shoulder and Elbow Surgeons; SST, Simple Shoulder Test.
Patients were also asked to assess their improvement or deterioration between the test-retest reliability and the follow-up episode (14 days after) using a global rating of change (GRC) scale, with a global perceived effect of −1 (deterioration), 0 (no change), or +1 (improvement). 12
Statistical Analysis
Statistical analysis was conducted using Jamovi Version 2.4.14 for macOS. The intraclass correlation coefficient (ICC) was used to assess test-retest reliability, with ICC values interpreted as excellent (>0.9), good (0.76-0.9), or moderate (0.5-0.75). The validity of the Thai SST was assessed by the strength of its association with the ASES score according to the Spearman correlation coefficient (r), with a P value of <.05 and an r value of >0.60 indicating a strong correlation,6,27 while an r value between 0.40 and 0.59 was considered a moderate correlation.3,6 The internal consistency of the Thai SST was assessed using Cronbach alpha, with values between .70 and .95 considered acceptable reliability, values <.70 indicating poor correlation between items, and values >.95 indicating redundancy of the questionnaire based on Terwee et al. 27 By calculating the percentage of scores clustered at the bottom and top of the questionnaire range, the floor or ceiling effects were examined for the total scores of the Thai SST and the ASES; floor or ceiling effects that were >15% were considered significant. 27
An a priori power analysis was conducted. The formula
Results
Cross-Cultural Adaptation and Translation Process
The Thai version of the SST was established following translation and backward translation procedures. 2 No inconsistencies were found between the forward and backward translation processes. The questionnaire was not revised because misinterpretation occurred in <15% of cases. Nevertheless, the expert committee meticulously refined the simplest Thai language explanations as much as possible.
In the initial pilot study, which included 10 patients, all participants comprehended the instructions, and there were only minor mistakes in the questionnaires. Overall, no obstacles were encountered in translating the original questionnaire into the Thai-adapted version based on routine activity lists. In the Thai language, metric units are more commonly used, so questionnaire items originally in pounds and yards were subsequently converted to kilograms and meters. Thus, some items were adjusted, such as replacing a full pint container with a half-liter bottle or a full gallon container with a 4-L bottle.
Patient Characteristics
The 75 Thai participants enrolled to answer the questionnaires comprised 73 with rotator cuff tears, 3 with combined rotator cuff tear and secondary stiff shoulder, 2 with combined rotator cuff tear and biceps tendinitis, 1 with isolated adhesive capsulitis, and 1 with isolated long head biceps tendinopathy. The overall mean age of the patients was 63.16 years (range, 30-70 years). Most of the patients reported engaging in low-demand activities, despite 22.62% participating in recreational sports. The characteristics of the patients are shown in Table 1.
Patient Characteristics a

Data are presented as n (%) unless otherwise indicated. BMI, body mass index.
Feasibility
Ten patients participated in the pilot study after providing informed consent. The finalized Thai SST was initially used to assess feasibility before conducting the test-retest reliability process. No significant missing responses or misunderstandings were noted in the questions. The duration between starting and completing the questionnaire was <10 minutes (range, 3-6 minutes). The Thai SST was completed in <1 minute for all 12 of the dichotomous questions.
Validity and Floor/Ceiling Effects
The Thai SST exhibited a strong positive correlation with the Thai ASES (r = 0.714). Both the Thai ASES and the Thai SST exhibited acceptable floor and ceiling effects, each being <15%, at each time point. However, individual items in the Thai SST could not demonstrate floor and ceiling effects due to the binary questionnaire format. The visual analog scale component of the ASES score showed a ceiling effect exceeding acceptable levels, which is commonly observed in self-administered rating scales. The distribution of floor and ceiling effects for the Thai ASES and Thai SST is presented in Table 2.
Floor/Ceiling Effects of the Thai ASES and Thai SST a

ASES, American Shoulder and Elbow Surgeons; SST, Simple Shoulder Test; VAS, visual analog scale.
Reliability and Internal Consistency
All participants were reassessed after completing the first test on the same day and 14 days after the initial examination. Before reassessing the test-retest reliability, all 75 participants completed the GRC scale, and no treatment effects were observed among the included participants.
The ICC values for intrarater and test-retest reliability measures were good and excellent for the Thai SST (ICC = 0.943 and 0.883, respectively) (Table 3). The test-retest reliability across all time points showed good reliability (ICC = 0.895). The Cronbach alpha of the Thai SST was .852, indicating it exhibited good and acceptable internal consistency. The standard error of measurement and minimal detectable change were 1.22 and 3.38, respectively, for the total SST (Table 4). This means that the Thai version of the SST would have to be altered by ≥3.38 points (on a scale of 0-12) before the observed change could be considered an actual change in a patient rather than a measurement error. 5
Reliability of the Thai SST Score a

ICC, intraclass correlation coefficient; SST, Simple Shoulder Test.
SE Measurement and MDC of the Thai SST a

MDC, minimal detectable change; SEM, standard error of measurement; SST, Simple Shoulder Test.
Discussion
The Thai SST was found to be strongly and positively correlated with the Thai ASES (r = 0.714). It demonstrated good test-retest reliability (ICC = 0.895) and acceptable internal consistency (Cronbach alpha, .852).
Patient-reported outcome measurements for shoulder function vary across cultures and are tailored to daily life activities. Widely utilized patient-reported outcome measures for shoulder problems include the ASES, Constant, and Disabilities of the Arm, Shoulder and Hand (DASH), which serve both research and clinical purposes. 18 In 1995, Matsen et al 16 developed the SST instrument to reflect clinical outcomes across various settings. The SST offers the benefits of simplicity and brevity, allowing for functional outcome measurement within 3 minutes, making it practical for outpatient assessments.
The Thai SST underwent cross-cultural adaptation due to differences in culture and daily activities compared with other Southeast Asian countries. The adaptation process involved translation and back-translation, with adjustments made to certain objects in each item to align with recognized elements in Thai culture. The original imperial units, such as pounds, were converted to the metric system, which is widely used in Thailand.
We assessed intrarater reliability in accordance with previous literature, 10 which differs from other studies. Porramatikul 20 aimed to establish the cross-cultural validity and reliability of the Thai ASES, achieving excellent reliability (ICC = 0.98), which was used for comparison in this study. To evaluate criterion validity, the Thai SST and Thai ASES were compared using the Spearman correlation coefficient. In other studies, the Arabic version of the SST showed a strong correlation with the Shoulder Pain and Disability Index (r = 0.77), with separate assessments for pain and disability. 25 The Persian version of the SST reported a strong correlation with the Persian Oxford Shoulder Score (r = 0.68). 17 The Japanese version of the SST was strongly and positively correlated with the DASH (r = 0.717; P < .001). 24 Thus, the SST is a concise instrument capable of assessing various shoulder pathologies such as rotator cuff tears, instability, and adhesive capsulitis, similar to various other instruments.7,9,13,16
We assessed content validity by examining floor and ceiling effects. 27 A ceiling effect was observed in the visual analog scale component of the Thai ASES score (32%). This ceiling effect may be attributed to the limited detail provided by the visual analog scale, leading to potential misinterpretation among participants with lower literacy levels. Nonetheless, another advantage of the SST is its suitability for assessment across all educational backgrounds due to its simplicity.
The test-retest reliability of the Thai SST across all time points demonstrated good reliability (ICC = 0.895). Similarly, Japanese, Arabic, Persian, and Brazilian versions of the SST also exhibited good to excellent reliability, consistent with this study of the Thai version, with ICC values of 0.859, 0.95, 0.61, and 0.84, respectively.17,19,24,25 Before reassessing the test-retest reliability, the GRC scale was completed for all patients, and no treatment effects were observed among the 75 participants included in this study. Overall, the SST demonstrated reproducibility across various shoulder pathologies, consistent with findings from other studies of each respective version.
The Cronbach alpha of the Thai SST was .852, indicating acceptable internal consistency, consistent with other studies. Similar levels of acceptable internal consistency were reported in the Japanese, Arabic, Persian, and Brazilian versions (Cronbach alpha = .83, .97, .84, and .82, respectively).17,19,24,25 The high value of internal consistency reflects the low heterogeneity of the questionnaire items in the test. All items in the SST could be interpreted in terms of pain and disability of the shoulder in the same direction.
Both the SST and the ASES provide a similar construct consisting of pain and disability scores. Resting shoulder pain, daily life activities, and lifting of objects are included in both instruments to assess disturbance. Overhead throwing and sport participation are higher functional assessments in both SST and ASES, representing the ultimate performance of the shoulder. One limitation of the instruments is the lack of questions about occupational participation, which is a primary functional requirement for Thai laborers, workers, and military recruits. 4 Only 1 item in the SST assesses disability affecting full-time occupation.
Limitations
There are some limitations to this study stemming from participant demographics and feasibility. First, the main population group consisted of middle-aged female patients with the primary diagnosis of rotator cuff pathology. Diagnoses were obtained from the hospital's Health Information System records and International Classification of Diseases–9 codes; however, some participants lacked physical examinations and shoulder range of motion assessments, potentially resulting in underdiagnosis of stiff shoulder and long head biceps pathology. Cases of shoulder instability and osteoarthritis were minor populations within the research protocol's duration. On the other hand, the SST could be applied to all shoulder pathologies and is not specific to shoulder instability, unlike the Oxford Shoulder Instability Score and the Western Ontario Shoulder Instability Index. 8 Despite the floor and ceiling effects exceeding acceptable values, the consistency and responsiveness of the instrument remain applicable to various shoulder pathologies. Further studies should investigate sensitivity of change after treatment to address this gap.
Conclusion
Our study demonstrated that the Thai version of the SST has acceptable reliability and validity, making it a suitable patient-reported outcome measure for assessing shoulder function in Thai patients with shoulder problems. The Thai SST can be used to assess the effectiveness of interventions for these shoulder pathologies in Thai patients.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241308281 – Supplemental material for Cross-Cultural Validity and Reliability of the Thai Version of the Simple Shoulder Test
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241308281 for Cross-Cultural Validity and Reliability of the Thai Version of the Simple Shoulder Test by Napatpong Thamrongskulsiri, Arnan Wiwatboworn, Thun Itthipanichpong, Thanathep Tanpowpong, Somsak Kuptniratsaikul and Danaithep Limskul in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors thank Professor Frederick A. Matsen III for granting permission to translate the SST into Thai. This permission enabled them to conduct this study.
Final revision submitted July 2, 2024; accepted July 23, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research project was supported by grants for development of new faculty staff, Ratchadaphiseksomphot Fund, Chulalongkorn University (DNS_66_100_3000_013). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chulalongkorn University (reference No. 1270/2023).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.