
Abstract
Background:
The effects of medical comorbidities on clinical outcomes in patients with rotator cuff tears (RCTs) have not been fully elucidated. This study investigates the association between medical comorbidities, as measured by the Functional Comorbidity Index (FCI), and clinical outcomes in patients treated surgically or nonsurgically for symptomatic, full-thickness RCTs.
Hypothesis:
Patients with RCTs who have more comorbidities will have worse outcome scores.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We collected the following outcome measures at baseline and at regular intervals up to 64 weeks in all patients: FCI, the Western Ontario Rotator Cuff Index (WORC), and the American Shoulder and Elbow Surgeons (ASES) score. Changes in outcomes were compared separately for surgical and nonsurgical patients using paired t tests. The relationship of the FCI and all outcomes of interest at baseline, at 64-week follow-up, and for changes from baseline was explored using linear regression modeling.
Results:
Of the 222 study patients (133 males; mean age, 60.0 ± 9.6 years), 140 completed the 64-week WORC and 120 completed the 64-week ASES. Overall, 128 patients underwent RCT repair, and 94 patients were treated nonsurgically. Both treatment groups improved compared with baseline at 64 weeks on the ASES score and WORC. At 64 weeks, patients with higher baseline FCI scores had worse WORC score (by 74.5 points; P = .025) and ASES score (by 3.8 points; P < .01). A higher FCI score showed a trend toward predicting changes in the WORC and ASES scores at 64 weeks compared with baseline, but this did not reach statistical significance (WORC change, P = .15; ASES change, P = .07).
Conclusion:
Patients with higher FCI scores at baseline reported worse baseline functional scores and demonstrated less improvement with time. The magnitude of this change may not be clinically significant for single comorbidities.
Keywords
The prevalence of rotator cuff disease in the United States is significant, and the cost to society is substantial. 22,32 Numerous previous studies using cadavers and advanced imaging have demonstrated the increased prevalence of full-thickness rotator cuff tears (RCTs) with advanced age. 14,16,31 Nearly 30% of individuals aged 65 years and older will have a full-thickness RCT. With the baby-boomer generation now in this age demographic, the prevalence of rotator cuff disorders is expected to increase significantly over the next 2 decades. This highlights the importance of health care providers’ understanding of factors that may influence the success of treatment. A thorough understanding of how concurrent medical comorbidities may influence rotator cuff disease outcomes is key to effectively treating this common disorder.
A 2014 report from the Agency for Healthcare Research and Quality states that 3 out of 4 Americans aged 65 years and older have multiple chronic conditions. 11 There is some evidence that comorbidities are related to and can influence outcomes in patients with shoulder pathologies. 27,28,33 Wylie et al 33 found that baseline University of Pennsylvania (PENN) scores were associated with the number of chest comorbidities but did not find an association with total number of comorbidities. The PENN score is a validated measure of shoulder-specific outcomes that includes 24 questions representing pain, satisfaction, and function. In a multicenter study, 4 investigators attempted to assess functional and health status outcomes in patients following a physical therapy program after rotator cuff repair and to determine the impact of selected patient medical comorbidities on rehabilitation outcomes. They found that a higher number of comorbidities had a negative effect on general health status outcomes, but they included only a limited number of specific comorbidities (asthma, depression, degenerative osteoarthritis, headache, hypertension, kidney disease, pneumonia, and sinus infection). Another study evaluated the relationship between the number of medical comorbidities and the preoperative performance on outcome assessment tools in patients with a chronic RCT. 29 The authors found that medical comorbidities have a negative impact on patient-reported preoperative baseline pain, function, and general health status associated with chronic RCTs, but that study did not report on postoperative outcomes. In 2006, Tashjian et al 28 reported a baseline difference in shoulder outcomes in those patients with greater comorbidities but also noted that the higher comorbidity group improved more than did the lower comorbidity group, such that there was no difference in final outcome scores between the 2 groups. However, there are few studies assessing the interplay between full-thickness RCTs and medical comorbidities that affect patient function (obesity, chronic obstructive pulmonary disease, osteoporosis, diabetes, congestive heart failure, stroke, myocardial infarction). Also, little evidence explores this interaction separately in operative versus nonoperative patients.
The objective of this study was to evaluate the influence of functional comorbidities in patients with full-thickness RCTs. We hypothesized that patients with more comorbidities would report worse function and increased pain when compared to healthier patients both at baseline and across time. This elucidation of the effects of comorbidities on outcomes in patients with rotator cuff disease may allow surgeons to better inform patients of their expected outcomes in relation to their individual comorbidities.
Methods
Study Design
This study was a secondary interim analysis of data collected in a prospective pragmatic cohort study. Treatment allocation to surgical or nonsurgical management was determined by the treating physician and patient. Approval to conduct this study was obtained through the University of Michigan Institutional Review Board.
Inclusion and Exclusion Criteria
All patients presenting with full-thickness RCTs were enrolled into this cohort after providing informed consent. The inclusion criteria were age 18 years or older and the presence of a full-thickness RCT confirmed by either magnetic resonance imaging or diagnostic ultrasound. Exclusion criteria were a history of previous surgery or infection of the affected shoulder or postpresentation follow-up of less than 1 year. Participants were mailed a $50 incentive on completion of their final follow-up.
Data Collection and Management
All data were collected through paper-based forms within the clinic at baseline, and all follow-up forms were mailed to patients. All demographic data and patient-reported outcome measures were collected at baseline and at 4, 8, 16, 32, 48, and 64 weeks. Comorbidity data were collected at baseline only. All completed patient forms were entered into a clinical research software database (Socrates; http://www.socratesortho.com), and all outcome measures were scored using standard methods for the measures listed below. All data were kept on a secure server backed up on password-protected external hard drives.
Outcome Measures
The following demographic data were collected at baseline: age, sex, smoking status, body mass index (BMI), tear size (determined by an experienced diagnostic radiologist), tear chronicity (ie, self-reported length of time with shoulder pain), and comorbidities (Table 1). Comorbidity data were used to score patients on the Functional Comorbidity Index (FCI). 12 In addition, all patients completed the Western Ontario Rotator Cuff Index (WORC) and the American Shoulder and Elbow Surgeons (ASES) Shoulder Outcome Score at baseline and all follow-up points.
Baseline Characteristics of Study Participants a
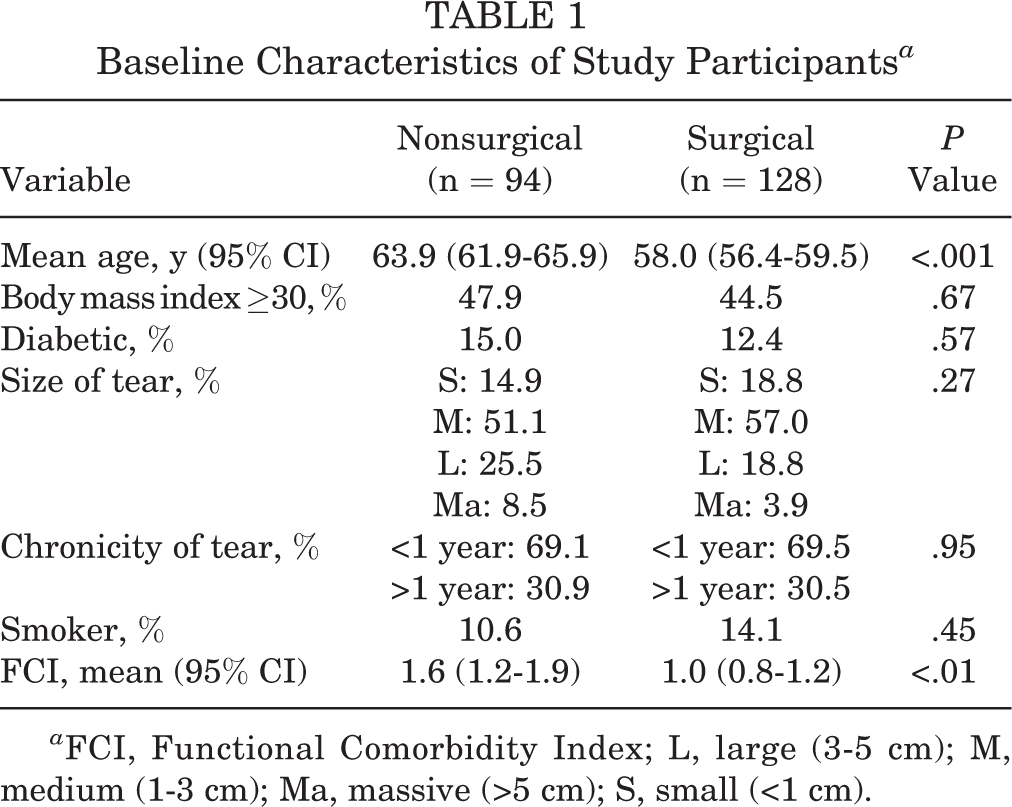
a FCI, Functional Comorbidity Index; L, large (3-5 cm); M, medium (1-3 cm); Ma, massive (>5 cm); S, small (<1 cm).
The FCI was developed by Groll et al 12 for use in general populations. The FCI is derived from self-reported diagnoses of 18 chronic conditions ranging from arthritis to congestive heart failure. The selected conditions predict the physical function subscale (10 items) of the Short Form–36. The FCI includes 7 conditions from the Charlson Comorbidity Index, plus arthritis, osteoporosis, angina, neurologic disease, depression, anxiety or panic disorders, visual impairment, hearing impairment, degenerative disc disease, and obesity. Two methods exist for scoring the FCI: (1) a simple count of the number of conditions reported by each subject and (2) a weighted count, where the weights come from standardized regression coefficients in a model predicting the physical function score. The FCI includes an important functional assessment that is appropriate in this population. In this study, the weighted scoring of the FCI was used.
The WORC includes 5 domains consisting of 21 questions and a 100-mm visual analog scale (VAS) response. The domains include pain and physical symptoms (6 questions), sports and recreation (4 questions), work function (4 questions), social function (4 questions), and emotional function (3 questions). The total possible raw WORC score is 2100, with higher scores indicating worse symptoms and function. The WORC has been proven to be valid, reliable, and responsive. 17,20
The ASES Shoulder Outcome Score is divided into 3 domains: pain, which includes several yes/no questions and a VAS; instability, which includes 1 yes/no question and a VAS; and activities of daily living. A 4-point ordinal scale rates 10 questions. The maximum score for the self-assessment portion is 30. This score is converted to a 100-point scale (100 being the highest score), with higher scores indicating better function. Construct validity, internal consistency, and reliability have been shown to be good. 1,3,5,15,19,21 Measurement of pain is via a 100-point VAS.
Statistical Analysis
Age and FCI scores were treated as continuous variables, and the following categorical variables were coded dichotomously: BMI (>30 or <30 kg/m2) and diabetes (yes or no). Baseline and demographic variables were summarized with means, proportions, SDs, and 95% confidence intervals (CIs) where appropriate. We used t tests to compare baseline values for continuous variables and chi-square tests for categorical variables.
Linear regression modeling, controlling for age, sex, and BMI, was used to explore the relationship of the FCI and all outcomes of interest at baseline, at 64-week follow-up, and for changes from baseline. Statistical significance was set at P < .05 for all analyses, and Stata/MP 14 (StataCorp) was used for all analyses.
The cohort study that the present analysis was conducted on was powered to detect the minimally important difference of the WORC. Given that this study was explorative and thus hypothesis-generating only, no sample size calculation was required. We sought to detect an 11.7% difference in the WORC (245.26 points) from baseline, with common SD of 500 points (alpha = 0.05, with 80% power), resulting in a sample of n = 132.
Results
A total of 140 patients were included in this interim analysis of this ongoing cohort study, which recruited 222 patients between May 2012 and October 2015. More than 85% of patients had complete follow-up on all outcomes for which they were eligible to complete. At baseline, there were 133 males and 89 females, with a mean age of 60 years (range, 36-76 years). Overall, 128 patients (57.7%, 83 males and 45 females; mean age, 58.0 ± 8.8 years) underwent rotator cuff repair, and 94 patients (42.3%, 50 males and 44 females; mean age, 63.9 ± 9.7 years) were treated nonsurgically. Sixty-two (27.9%) patients experienced symptoms for at least 12 months, and 54 (24.3%) had a tear exceeding 3 cm in the largest dimension. Thirty (13.5%) patients self-reported a diagnosis of diabetes, and 102 (45.9%) patients had a BMI ≥ 30. Patient demographics and baseline comorbidities are outlined in Table 1. Of note, the nonsurgical group was slightly older than was the surgical group (63.8 vs 58.0 years, P < .001).
At baseline, the patients who were treated without surgery had a better WORC (1089.4) when compared with those treated surgically (1241.5; P = .01) (Table 2). Those patients treated nonoperatively had a better baseline ASES score (57.3) compared to those of the surgically treated patients (51.2; P = .05). While patients in both surgical and nonsurgical groups improved from baseline to follow-up, patients in the surgical group improved more on all outcomes (Table 2).
Outcome Scores at Baseline and 64 Weeks

Across the entire sample, regression analysis revealed that an increased FCI score was associated with worse baseline WORC score (by 62.0 points; n = 218, P = .02) and ASES score (by 1.99 points; n = 192, P = .01). A higher FCI score showed a trend toward predicting improved changes in the WORC and ASES scores at 64 weeks compared to baseline, but this did not reach statistical significance (WORC change, P = .15; ASES change, P = .07) (Tables 3 and 4, respectively). In these same models, those who were older improved less when compared to baseline. At 64-week follow-up, a lower FCI significantly predicted better total WORC scores (by 74.5 points, P = .03) and ASES scores (by 3.8 points, P = .01) (Tables 5 and 6, respectively). Also, female patients tended to have better ASES scores at 64 weeks (by 9.3 points). When the surgical and nonsurgical patients were analyzed separately with linear regression, the FCI was not predictive of the WORC (surgical, P = .53; nonsurgical, P = .46) or ASES (surgical, P = .76; nonsurgical, P = .13) at 64 weeks or changes from baseline (surgical, WORC P = .96, ASES P = .78; nonsurgical, WORC P = .93, ASES P = .45).
Regression Analysis of Change in Western Ontario Rotator Cuff Index: Baseline to 64 Weeks (n = 138)

Regression Analysis of Change in American Shoulder and Elbow Surgeons Score: Baseline to 64 Weeks (n = 115)

a Sex coded as 0 = female, 1 = male.
Regression Analysis of Western Ontario Rotator Cuff Index at 64 Weeks (n = 138)
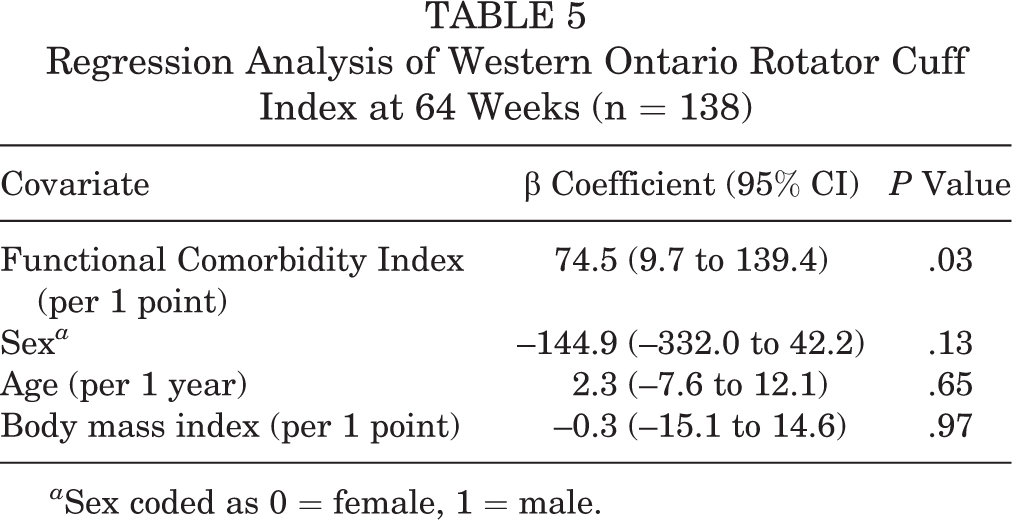
a Sex coded as 0 = female, 1 = male.
Regression Analysis of American Shoulder and Elbow Surgeons Score at 64 Weeks (n = 119)
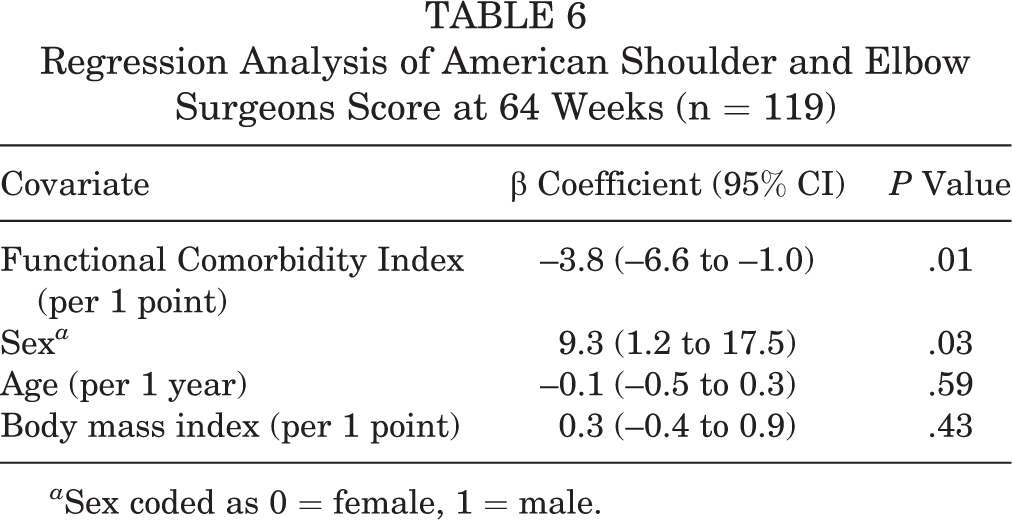
a Sex coded as 0 = female, 1 = male.
Discussion
In this study, while patients in both the surgical and nonsurgical groups improved from baseline, scores on all outcome measures improved more for the surgical group compared to those of the nonsurgical group. When looking across the entire sample, those with increased comorbidities, as measured by the FCI, had worse baseline and 64-week outcomes but greater improvement across time. Although Tashjian et al 28 used different outcome scores (Disabilities of the Arm, Shoulder and Hand; Simple Shoulder Test) than were used in this study, they too found that patients with more comorbidities had a greater improvement in outcomes compared to those with less comorbidities. Our study demonstrated that a higher FCI score in patients sustaining RCTs was a significant predictor of worse scores at baseline and at the final follow-up point but of greater change from baseline. However, when looking separately at surgical and nonsurgical patients, the FCI did not predict the 64-week ASES score or WORC, or changes from baseline for the ASES or WORC.
This finding is not surprising given that the FCI includes comorbidities that are relevant to the types of participant pathologies included in this study. That is, the FCI was developed to measure comorbidities that affect function. It was specifically developed and tested for use in patients with musculoskeletal impairments and injuries. Similar findings have also been reported across other orthopaedic conditions. For example, 2 previous studies evaluated adverse events and complications following orthopaedic procedures across many musculoskeletal conditions and found the FCI to be a reliable predictor of outcome. 10,25 SooHoo et al 25 found that increasing the comorbidity index by 1 point in patients undergoing total knee replacement increased mortality by 170%.
There are several limitations to our study. First, this is a cohort study and, thus, there is the potential to have differences between the treatment groups due to variables not controlled for or described in our analyses (eg, whether the tear was traumatic or not). Next, the change in outcome measure scores did not reach statistical significance when the surgical and nonsurgical groups were analyzed separately. This could be due to the relatively small sample sizes in these separate subgroup analyses, resulting in a lack of power to detect these effects. Future research with larger sample sizes could test this hypothesis.
Also, at first glance, the magnitude of change we found could be considered small. According to our findings in this cohort, a patient reporting a single comorbidity might be expected to do worse on the WORC at 64 weeks by 74 points (3.5%) when compared to a patient with no comorbidities, after controlling for sex, age, and BMI (Table 5). That is, a change of 74.5 points on the WORC for a 1-point change in the FCI is likely not clinically significant. That change does not reach the minimal important difference (MID) for this measure (245.26 points). 17 However, a patient with 3 comorbidities will do worse by 222 points on the WORC, after controlling for sex, age, and BMI, which approaches the MID and thus is likely clinically important. The same line of reasoning applies to ASES scores at 64 weeks (Table 6) and the change in WORC and ASES scores from baseline (Tables 3 and 4). For example, the findings in this cohort also showed a 3.8-point effect in ASES score for every 1 point on the FCI. Tashjian et al 27 showed an MID for the ASES score of between 12 and 17. Therefore, a patient would need to have 3 to 5 comorbidities for this to reach a clinically important effect. The idea here is that those with multiple comorbidities have worse scores at 64 weeks and change more from baseline, even after controlling for several other important variables. However, future research needs to confirm the MID for the WORC and ASES in patients with RCTs. 18,27 Many RCT patients have multiple comorbidities 11 since they tend to be older; therefore, our findings are highly relevant and clinically important in this group. Furthermore, most of the comorbidities collected in this study were self-reported; therefore, the actual number of comorbidities was possibly underestimated, especially for certain conditions, 24,26,30 suggesting that the “true” relationship between functional comorbidities and patient outcomes may be more pronounced than the data from this study suggest. But more work needs to be done to explore the breadth and impact of such underreporting in patients with rotator cuff disease. Overall, our findings suggest that patients with multiple comorbidities have worse outcomes.
Numerous studies have shown an increased risk of complications, decreased healing rates, and worse outcomes following rotator cuff repair in patients with diabetes, 5,6,8 hypercholesterolemia, 2 and osteoporosis. 7 These studies have all looked at specific medical comorbidities, but none have used a validated comorbidity index to evaluate the interplay between comorbidities and functional outcome following rotator cuff repair. Tashjian et al 28 examined the relationship between a select list of comorbid medical conditions and shoulder outcomes following RCT. They found that patients with more medical comorbidities had a worse general health status after rotator cuff repair, but these patients had greater improvement in overall shoulder pain, function, and quality-of-life scores compared with preoperative scores. Wylie et al 33 showed that PENN scores decreased with an increase in the number of chest comorbidities but not the total number of comorbidities. Another study looked at the prevalence of RCTs and correlation with comorbidities 9 but did not report on the relationship between medical comorbidities and patient-reported outcomes. The inverse relationship between comorbidity and shoulder function that we observed in patients with RCTs is similar to that reported by Harryman et al 13 and Rozencwaig et al 23 in their studies of patients with degenerative glenohumeral joint disease. It stands to reason that patients with more medical comorbidities are more likely to feel less healthy and report worse function than are patients who enjoy better overall health. It also makes sense that patients with more comorbidities at baseline improve more over time because they have lower shoulder scores at baseline and thus have greater room for improvement.
Our study evaluated the overall health of patients and how it affects outcomes following RCTs, which is of value to practicing orthopaedic surgeons. Taking into account the comorbidity status and overall health of each patient allows surgeons to discuss realistic outcome expectations for patients after an RCT. That is not to say that surgeons should treat only patients without any comorbid conditions, but it is our hope that this study will provide some data that orthopaedic surgeons can share with less healthy patients about their expected outcomes when compared with healthier patients sustaining RCTs.
The objective of this study was to investigate the relationship between health status, using a validated comorbidity index, and functional outcome following treatment of full-thickness RCTs. Our primary hypothesis was that patients with more comorbidities at baseline would report diminished baseline functional scores and diminished functional gains after treatment. In our study cohort, patients with full-thickness RCTs and more medical comorbidities (higher FCI score) had lower functional scores (WORC and ASES) at baseline and over time than did patients with fewer comorbidities (lower FCI score), but they also tended to improve more compared to baseline. The FCI has proven to be a reliable predictor of outcomes across populations with orthopaedic conditions in this and other studies. As our institution continues to enroll patients and the cohort grows, we will continue to evaluate our data. With larger patient numbers, we may learn if the FCI is predictive of functional outcomes scores when analyzing patient groups separately based on surgical or nonsurgical treatment.
Conclusion
Patients with higher scores on the FCI are worse at baseline, as measured by patient-reported outcomes (WORC, ASES), and have greater improvement when followed for 64 weeks. However, the magnitude of this change may not be clinically significant and may reach measurable significance only when a patient presents with multiple comorbidities.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the Francis and Kenneth Eisenberg Research Fund.
Ethical approval for this study was obtained from the University of Michigan Medical School Institutional Review Board.